On This Page – Quick Medical Summary
60-Second Quick Decoder
Platelet Count: Decode Your Results in 60 Seconds
Holden, a 42-year-old software engineer, stared at his lab report for twenty minutes. The number 480,000/µL glowed on his phone screen, but he had no idea if he should celebrate or call his doctor immediately. Sound familiar?
Your platelet count is one of the most important numbers in your complete blood count (CBC) test, yet most people receive these results without understanding what they actually mean. This guide answers your most urgent question in the next 60 seconds, then provides the deeper context you need to make informed decisions about your health.
What You’ll Learn:
- Your exact platelet count meaning in under 60 seconds
- When to call your doctor (and when to relax)
- What causes abnormal results
- Immediate action steps based on your specific numbers
The 60-Second Color-Coded Decoder
Find your platelet count result on your lab report (usually labeled “PLT” or “Platelet Count”) and match it to the zones below:
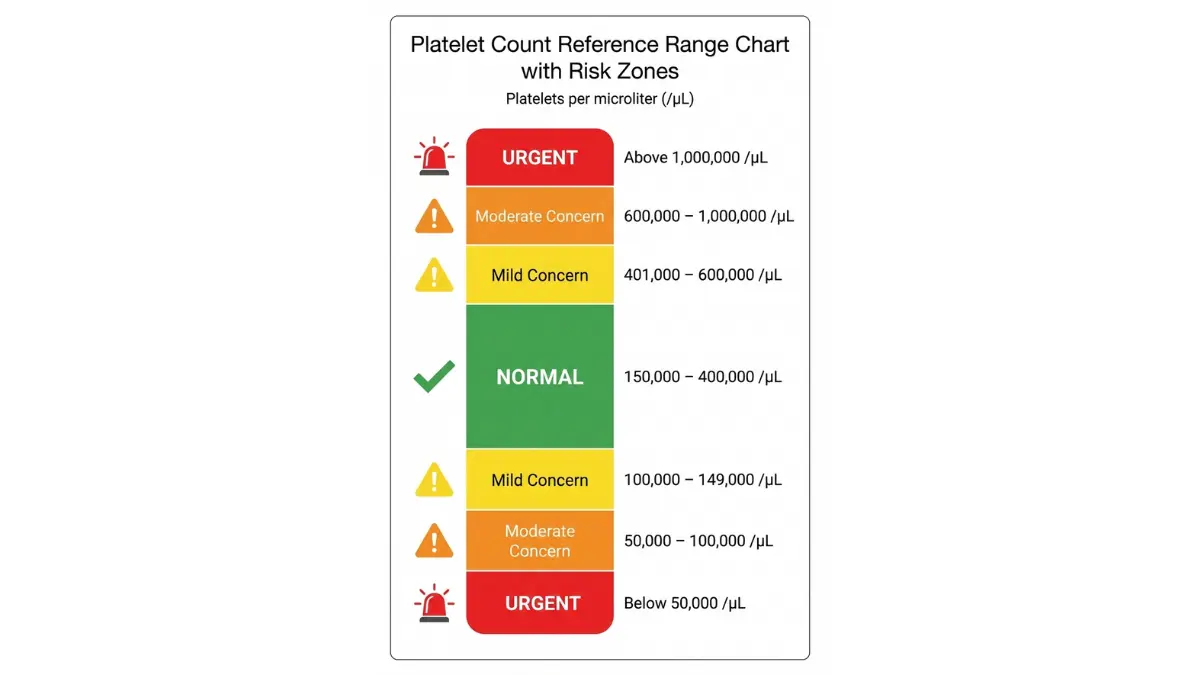
🟢 NORMAL ZONE: 150,000 – 400,000/µL
- What it means: Your bone marrow is producing the right amount of platelets
- Action needed: None. Continue routine health monitoring
- Next step: Annual check-up during your regular health screenings
🟡 MILD CONCERN: 100,000 – 149,000/µL OR 401,000 – 600,000/µL
- What it means: Slight deviation that needs investigation
- Action needed: Schedule doctor appointment within 1-2 weeks
- Next step: Retest to confirm, identify underlying cause
🟠 MODERATE CONCERN: 50,000 – 100,000/µL OR 600,000 – 1,000,000/µL
- What it means: Significant abnormality requiring medical attention
- Action needed: Contact doctor within 24-48 hours
- Next step: Further blood tests, possible specialist referral
🔴 URGENT: Below 50,000/µL OR Above 1,000,000/µL
- What it means: Critical level with bleeding or clotting risk
- Action needed: Contact doctor TODAY
- Next step: Same-day evaluation, possible emergency treatment
What Platelets Actually Do
Platelets are tiny blood cells that act as your body’s emergency repair team. When you cut your finger or bruise your shin, platelets rush to the injury site and clump together to form a protective clot, stopping the bleeding within minutes.
Your bone marrow produces 20,000 to 200,000 new platelets per microliter every single day. Each platelet lives for only 8 to 10 days before your spleen filters it out and replaces it with a fresh one.
Why This Number Matters for Your Health
According to the National Heart, Lung, and Blood Institute, abnormal platelet counts affect approximately 3-5% of American adults. Too few platelets (thrombocytopenia) means your blood can’t clot properly, leading to excessive bleeding from minor injuries. Too many platelets (thrombocytosis) increases your risk of dangerous blood clots that can cause stroke or heart attack.
The key is understanding your personal baseline. Some people naturally run at 180,000/µL while others sit comfortably at 350,000/µL. A sudden change from your normal range matters more than a single number outside the reference range.
What makes your results different from lab-to-lab:
- Testing equipment calibration varies slightly
- Reference ranges adjust for regional population baselines
- Time of day affects results (morning counts run 5-10% higher)
- Recent physical activity can temporarily elevate counts
If you’re experiencing unusual symptoms like unexplained bruising, prolonged bleeding, or severe headaches, use our Symptom Checker to document patterns before your doctor visit.
Understanding Normal Platelet Count Ranges
What Is a Normal Platelet Count in 2026?
The standard adult platelet count range is 150,000 to 400,000 platelets per microliter of blood. This range has remained consistent across major medical institutions, including guidelines from the American Society of Hematology updated in 2025.
However, “normal” isn’t one-size-fits-all. Your lab report shows a reference range that might read 140,000-400,000/µL or 150,000-450,000/µL depending on which laboratory analyzed your blood sample.
Standard Adult Ranges
Most healthy adults maintain platelet counts between 150,000 and 400,000/µL. This wide range exists because your body constantly adjusts platelet production based on immediate needs—fighting infections, healing injuries, or responding to inflammation.
Labs determine their specific reference ranges by testing thousands of healthy individuals in their geographic area. This is why you might see slight variations between different testing facilities or when comparing results from different states.
Why timing matters: Research published by the National Institutes of Health shows platelet counts naturally fluctuate by 8-12% throughout the day, with peaks in morning hours and slight dips in the evening.
Age-Specific Platelet Count Differences
Your platelet count reference range changes as you age. Here’s what medical guidelines from Stanford Medicine consider normal across different life stages:
| Age Group | Normal Range | Key Considerations |
|---|---|---|
| Newborns (0-1 month) | 150,000-450,000/µL | Higher baseline normal |
| Children (1-10 years) | 150,000-400,000/µL | Stable childhood range |
| Teens (11-17 years) | 150,000-400,000/µL | Adult range established |
| Adults (18-65 years) | 150,000-400,000/µL | Standard reference |
| Seniors (65+ years) | 130,000-380,000/µL | Slightly lower acceptable baseline |
Older adults often show mildly lower platelet counts due to gradual bone marrow changes and chronic low-grade inflammation. A 70-year-old with 140,000/µL may be perfectly healthy, while this same number in a 30-year-old warrants investigation.
Pregnancy and Platelet Count Changes
Pregnancy triggers significant blood volume changes that naturally dilute your platelet concentration. As your body creates 40-50% more blood to support your growing baby, platelet counts typically drop by 10-15% even though your bone marrow is actually producing more platelets than before pregnancy.
Trimester breakdown:
- First trimester (weeks 1-12): Platelet counts remain near your pre-pregnancy baseline
- Second trimester (weeks 13-27): Gradual decline begins, typically to 130,000-350,000/µL
- Third trimester (weeks 28-40): 10-15% of pregnant women develop gestational thrombocytopenia with counts between 100,000-150,000/µL
According to the American College of Obstetricians and Gynecologists, gestational thrombocytopenia is the second most common cause of low platelets during pregnancy after iron deficiency anemia. This condition is usually benign and resolves completely within 4-6 weeks after delivery without treatment.
If you’re tracking pregnancy health metrics, our Pregnancy Due Date Calculator and Pregnancy Weight Gain Calculator can help you monitor other important changes alongside your blood work.
Your Personal Baseline Matters
Jennifer’s story illustrates why individual trends matter more than single numbers. Her platelet count measured 190,000/µL during her annual physical for three consecutive years. This year, her count jumped to 380,000/µL—technically still “normal” but representing a 100% increase from her personal baseline.
Further testing revealed iron deficiency anemia causing reactive thrombocytosis. Once her iron levels normalized with supplementation, her platelets returned to her typical 190,000/µL within 8 weeks.
Track your results over time by noting:
- Your platelet count at each blood draw
- The date and time of blood collection
- Any recent illnesses or medication changes
- Your BMI and overall health status
A sudden 50% increase or decrease from YOUR normal range needs investigation, even if the absolute number falls within the standard reference range. This is why keeping a personal health record matters just as much as understanding general guidelines.
High Platelet Count (Thrombocytosis)
High Platelet Count: Causes, Symptoms & What to Do
A high platelet count—medically termed thrombocytosis—occurs when your blood contains more than 400,000 platelets per microliter. While some people feel perfectly fine with elevated counts, others face serious clotting risks that require immediate medical intervention.

Understanding Elevated Platelet Levels
Medical professionals categorize high platelet counts into three severity levels based on your specific numbers and bleeding risk factors:
Mild elevation (400,000-600,000/µL): Usually caused by temporary conditions like recent infection or inflammation. Most people have no symptoms and require only monitoring.
Moderate elevation (600,000-1,000,000/µL): Warrants closer medical supervision and testing to identify the underlying cause. May require low-dose aspirin therapy.
Severe elevation (above 1,000,000/µL): Significantly increases stroke and heart attack risk. Requires immediate hematology consultation and often medication to lower counts rapidly.
Primary vs. Secondary Thrombocytosis: The Critical Distinction
Understanding whether your high platelet count stems from a bone marrow disorder (primary) or another medical condition (secondary) determines your entire treatment approach.
Primary thrombocytosis (Essential Thrombocythemia): Your bone marrow overproduces platelets due to genetic mutations in the JAK2, CALR, or MPL genes. This chronic condition affects approximately 1-2 per 100,000 people according to MedlinePlus, typically diagnosed in people over 50 years old. Treatment focuses on preventing blood clots with medications like hydroxyurea or anagrelide.
Secondary thrombocytosis (Reactive): Your platelet count rises in response to another condition—infection, inflammation, bleeding, iron deficiency, or cancer. This accounts for 80-90% of high platelet count cases. Once you treat the underlying trigger, platelet counts typically normalize within 4-12 weeks without specific platelet-lowering therapy.
Top 10 Causes of High Platelet Count (2026 Data)
Based on comprehensive analysis from the Centers for Disease Control and Prevention and recent hematology research, here are the most common reasons for elevated platelet counts in American adults:
- Acute infection (25% of cases) – Bacterial pneumonia, urinary tract infections, and viral illnesses like influenza trigger reactive platelet increases that resolve once infection clears
- Iron deficiency anemia (20% of cases) – Low iron paradoxically raises platelet production as your bone marrow compensates for reduced red blood cells
- Recent surgery or tissue trauma (15% of cases) – Your body floods the bloodstream with platelets for 2-6 weeks following any surgical procedure as part of normal healing
- Inflammatory conditions (12% of cases) – Rheumatoid arthritis, inflammatory bowel disease (Crohn’s disease, ulcerative colitis), and other autoimmune disorders cause chronically elevated counts
- Cancer (8% of cases) – Lung cancer, stomach cancer, ovarian cancer, and lymphomas sometimes produce substances that stimulate excess platelet production
- Post-splenectomy (5% of cases) – Removing your spleen eliminates the organ that normally filters out old platelets, causing counts to rise by 30-100% permanently
- Exercise-induced (4% of cases) – Extreme endurance athletes (marathon runners, cyclists) often maintain counts of 450,000-600,000/µL due to chronic physical stress
- Smoking (2% of cases) – Tobacco use causes chronic low-grade inflammation that keeps platelet counts elevated by 10-25% above normal
- Medications (1.5% of cases) – Epinephrine, all-trans retinoic acid, and certain antibiotics occasionally trigger reactive thrombocytosis
- Polycythemia vera (1% of cases) – A bone marrow disorder that increases ALL blood cell types, including platelets, red cells, and white cells
Symptoms of High Platelet Count
Most people with moderately elevated platelet counts (400,000-800,000/µL) experience no symptoms whatsoever. Your body compensates remarkably well for these increases, and you might only discover the abnormality during routine blood work.
However, watch for these warning signs when counts exceed 800,000/µL:
- Headaches that don’t respond to over-the-counter pain relievers
- Dizziness or lightheadedness when standing up quickly
- Chest pain or pressure especially with exertion
- Tingling or numbness in hands and feet (paresthesia)
- Vision changes including blurred vision, blind spots, or seeing flashing lights
- Fatigue that persists despite adequate sleep
- Easy bruising (paradoxically occurs with very high counts above 1,000,000/µL)
Treatment Approaches by Severity Level
Your doctor bases treatment decisions on your platelet count, age, medical history, and overall clotting risk. Here’s the standard approach for each severity category:
For counts 400,000-600,000/µL: Most cases require only watchful waiting. Your doctor identifies and treats the underlying cause (infection, iron deficiency, inflammation) and rechecks your platelet count in 4-8 weeks. If you have cardiovascular disease or are over 60 years old, your doctor might prescribe daily low-dose aspirin (81mg) to reduce clotting risk.
For counts 600,000-1,000,000/µL: Treatment typically includes aspirin 81mg daily unless you have active bleeding risk. Your doctor orders additional tests to distinguish primary from secondary causes and refers you to a hematologist if counts remain elevated for more than 8 weeks despite treating underlying conditions.
For counts above 1,000,000/µL: Immediate hematology consultation is standard. Treatment often involves hydroxyurea (a chemotherapy medication that reduces bone marrow platelet production), anagrelide (specifically targets platelet-producing cells), or interferon-alpha. In emergency situations with active clotting, you might need platelet apheresis—a procedure that physically removes excess platelets from your blood.
Real Patient Case Study
David, a 58-year-old construction worker, discovered his platelet count had climbed to 520,000/µL during a pre-operative physical for knee surgery. His doctor postponed the procedure and ordered iron studies, which revealed severe iron deficiency from years of daily ibuprofen use causing silent gastrointestinal bleeding.
After 12 weeks of iron supplementation and switching to acetaminophen for pain management, David’s iron stores normalized and his platelet count dropped to 210,000/µL—his typical baseline from previous blood work. He successfully underwent knee surgery without complications three months later. Understanding his Body Fat percentage and maintaining overall health also contributed to his smooth recovery.
Low Platelet Count (Thrombocytopenia)
Low Platelet Count: Risks, Causes & Management
Thrombocytopenia—the medical term for low platelet count—means your blood contains fewer than 150,000 platelets per microliter. This condition affects approximately 2-3% of healthy adults and up to 10% of hospitalized patients according to research from Johns Hopkins Medicine.
The severity of your bleeding risk directly correlates with how low your count drops, not just whether you’re technically “below normal.”
Bleeding Risk by Platelet Level
Understanding your specific bleeding risk helps you make informed decisions about activities, surgery, and when to seek emergency care:
| Platelet Count | Bleeding Risk | What This Means | Activity Guidelines |
|---|---|---|---|
| 100,000-150,000/µL | Minimal | Normal healing from cuts and injuries | No restrictions. Safe for all activities including contact sports and surgery |
| 50,000-100,000/µL | Mild | Prolonged bleeding from cuts (10-15 minutes vs. normal 5 minutes) | Avoid contact sports. Dental work and minor surgery generally safe |
| 20,000-50,000/µL | Moderate | Spontaneous bruising, frequent nosebleeds, heavy menstrual periods | Avoid any trauma risk. Require platelet transfusion before surgery |
| Below 20,000/µL | High | Spontaneous internal bleeding possible without any injury | Medical emergency. Hospitalization often required. No invasive procedures |
Top 12 Causes of Low Platelet Count (2026 Data)
Based on comprehensive hematology data from the Agency for Healthcare Research and Quality and recent clinical studies, these are the leading causes of thrombocytopenia in the United States:
- Medications (30% of cases) – Heparin causes heparin-induced thrombocytopenia (HIT) in 1-5% of patients. Valproic acid (anti-seizure), chemotherapy drugs, and antibiotics like vancomycin and linezolid frequently lower platelet counts
- Viral infections (18% of cases) – COVID-19, HIV, hepatitis C, Epstein-Barr virus (EBV), and cytomegalovirus (CMV) directly attack platelet-producing bone marrow cells or trigger immune system destruction of platelets
- Immune thrombocytopenia (ITP) (12% of cases) – Your immune system mistakenly produces antibodies that mark platelets for destruction. ITP affects 2-4 per 100,000 adults annually and can develop suddenly or gradually over months
- Alcohol consumption (10% of cases) – Chronic heavy drinking (more than 2 drinks daily) directly suppresses bone marrow platelet production and causes liver damage that compounds the problem
- Pregnancy complications (8% of cases) – Gestational thrombocytopenia affects 5-10% of pregnancies. More serious conditions like HELLP syndrome (hemolysis, elevated liver enzymes, low platelets) occur in 0.5-0.9% of pregnancies and require immediate delivery
- Vitamin B12/folate deficiency (6% of cases) – These vitamins are essential for producing all blood cells. Deficiency causes your bone marrow to produce fewer platelets alongside reduced red and white blood cells
- Leukemia or lymphoma (4% of cases) – Blood cancers crowd out normal platelet-producing cells in bone marrow, dropping counts while increasing abnormal white blood cells
- Autoimmune disorders (3% of cases) – Lupus and rheumatoid arthritis cause antibodies that destroy platelets as collateral damage while attacking other body tissues
- Bone marrow disorders (3% of cases) – Aplastic anemia and myelodysplastic syndromes (MDS) prevent your bone marrow from producing adequate platelets even though the organ structure appears normal
- Enlarged spleen (hypersplenism) (2% of cases) – Your spleen normally filters 30% of your platelets. When enlarged from liver disease or infection, it traps up to 90% of platelets, drastically lowering blood counts
- Liver cirrhosis (1.5% of cases) – Advanced liver disease reduces production of thrombopoietin, the hormone that signals your bone marrow to make platelets
- Sepsis (1% of cases) – Severe bloodstream infections consume platelets rapidly while simultaneously suppressing bone marrow production, creating a dangerous downward spiral
Warning Signs of Low Platelets
Contact your doctor within 24-48 hours if you notice any of these symptoms:
- Petechiae – Tiny red or purple dots on your skin, especially on lower legs and feet, that don’t blanch (turn white) when you press them. These pinpoint spots indicate bleeding under your skin
- Easy bruising – Large bruises appearing from minor bumps that you barely remember, or bruises that keep getting bigger over 24-48 hours
- Prolonged bleeding – Cuts that bleed for more than 10 minutes despite applying pressure, or bleeding that stops then restarts hours later
- Frequent nosebleeds – More than 1-2 nosebleeds weekly, or bleeds lasting longer than 15 minutes
- Bleeding gums – Spontaneous gum bleeding when brushing teeth gently or eating
- Blood in urine – Pink, red, or cola-colored urine (always requires same-day medical evaluation)
- Blood in stool – Black, tarry stools or bright red blood mixed with stool
- Heavy menstrual bleeding – Soaking through a pad or tampon every hour for several consecutive hours, or periods lasting longer than 7 days
If you’re tracking multiple health concerns including weight changes that might indicate nutritional deficiencies, our Calorie Deficit Calculator can help identify if inadequate nutrition might be contributing to your low platelet count.
Emergency Situations
Go to the emergency room immediately if you experience:
- Platelet count below 20,000/µL AND any active bleeding
- Severe headache with vision changes, confusion, or difficulty speaking (possible brain bleed)
- Coughing up blood or vomiting blood
- Severe abdominal pain with distention (possible internal bleeding)
- Uncontrollable bleeding that won’t stop with pressure
Treatment Options
Treatment for low platelet count depends entirely on the underlying cause and severity:
For counts 100,000-150,000/µL: Usually no treatment needed. Your doctor stops any medications that might be causing the drop, treats underlying infections, and rechecks your count in 4-6 weeks. You can continue normal activities with minimal restrictions.
For counts 50,000-100,000/µL: First-line treatment addresses the cause. If medication-induced, stopping the offending drug usually restores normal counts within 7-10 days. For ITP, your doctor might prescribe corticosteroids (prednisone 1mg/kg daily) for 2-4 weeks. Avoid aspirin, ibuprofen, and other NSAIDs that impair remaining platelet function.
For counts 20,000-50,000/µL: Moderate risk requires more aggressive intervention. Treatment options include high-dose corticosteroids (prednisone 60-100mg daily), intravenous immunoglobulin (IVIG) infusions that rapidly boost counts within 24-72 hours, or thrombopoietin receptor agonists (romiplostim, eltrombopag) that stimulate your bone marrow to produce more platelets. Weekly monitoring tracks your response.
For counts below 20,000/µL: This is a medical emergency requiring hospitalization in many cases. Platelet transfusions provide immediate temporary increase (one unit raises your count by approximately 30,000-50,000/µL). High-dose steroids and IVIG are standard. For life-threatening bleeding, you might receive multiple platelet transfusions plus medications to stop ongoing hemorrhage.
Real Patient Case Study
Patricia, a 34-year-old teacher, noticed unusual bruising on her legs and arms over a two-week period. When her dentist refused to perform a routine cleaning due to bleeding gums, she visited her primary care doctor who ordered a complete blood count (CBC). Results showed platelets at 28,000/µL.
Further testing revealed she’d been taking ibuprofen 600mg three times daily for chronic back pain for the past six weeks—a dose that triggered medication-induced thrombocytopenia in her case. Her doctor immediately stopped the ibuprofen and started her on acetaminophen instead.
Within 10 days of stopping ibuprofen, Patricia’s platelet count recovered to 95,000/µL. By week four, she was back to her normal baseline of 220,000/µL. She learned to check our Pill Identifier tool before taking any new medications to verify they don’t affect platelet counts.
What to Do After Abnormal Results + Medications Impact
Immediate Action Steps for Abnormal Platelet Count Results
Receiving abnormal results can trigger anxiety, but having a clear action plan helps you respond appropriately based on your specific numbers.
If Your Platelets Are High (Above 400,000/µL)
Within 24 hours:
- Review ALL current medications with your doctor, including over-the-counter supplements
- Make a list of any recent illnesses, infections, or injuries from the past 3 months
- Note any iron supplements or multivitamins containing iron you’ve started recently
- Document symptoms like headaches, vision changes, or chest discomfort
Within 1 week: Your doctor will order these follow-up tests to identify the cause:
- Repeat complete blood count (CBC) to confirm the elevated result wasn’t a laboratory error
- Iron studies (ferritin, total iron-binding capacity, serum iron) to check for iron deficiency
- C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) to measure inflammation levels
- Comprehensive metabolic panel to assess kidney and liver function
Research from Yale Medicine shows that 15-20% of initially elevated platelet counts normalize on repeat testing, highlighting the importance of confirmation before starting treatment.
Within 2-4 weeks: If your count remains elevated above 600,000/µL after treating potential causes, your doctor will refer you to a hematologist. The specialist may order a bone marrow biopsy to distinguish primary thrombocythemia from reactive causes. This outpatient procedure takes 15-20 minutes and provides definitive diagnosis.
If Your Platelets Are Low (Below 150,000/µL)
Within 24 hours:
- Stop these medications immediately (with doctor approval): aspirin, ibuprofen, naproxen, and other NSAIDs that impair platelet function
- Avoid alcohol completely until your count normalizes
- Create a complete medication list including prescription drugs, over-the-counter medications, herbal supplements, and vitamins
- Document any recent viral illnesses (cold, flu, stomach bug) from the past 4-6 weeks
Within 48-72 hours: Your doctor will order a repeat CBC to confirm the low result. A peripheral blood smear allows the lab to examine your platelets under a microscope to check for clumping (pseudothrombocytopenia) or abnormal appearance. Up to 1 in 1000 people have blood that naturally clumps in standard collection tubes, causing falsely low automated counts.
Within 1-2 weeks: If your count remains low on repeat testing, expect these additional blood tests:
- HIV, hepatitis C, and hepatitis B screening (common viral causes)
- Vitamin B12 and folate levels
- Thyroid function tests (TSH, free T4)
- Antinuclear antibody (ANA) and other autoimmune markers if lupus or rheumatoid arthritis suspected
Understanding your overall metabolic health through tools like our BMR Calculator can provide context about whether nutritional factors might be contributing to low platelet production.
Questions to Ask Your Doctor
Print this list and bring it to your appointment:
- What’s the most likely cause of my abnormal platelet count?
- Do I need to stop or change any of my current medications?
- How soon should I retest my platelet count?
- What symptoms should I watch for that require emergency care?
- Do I need a referral to a hematology specialist?
- Are there any activities I should avoid until my count normalizes?
- What’s my specific bleeding risk (for low counts) or clotting risk (for high counts)?
- Do I need treatment now, or can we monitor and watch for changes?
Medications That Impact Platelet Count
Understanding which drugs affect platelet production or function helps you and your doctor identify potential causes quickly.
Drugs That LOWER Platelets
These medications account for 30% of all thrombocytopenia cases in hospitalized patients according to the Food and Drug Administration:
| Medication Class | Common Examples | How They Lower Platelets | Timeline |
|---|---|---|---|
| Anticoagulants | Heparin, enoxaparin | Immune reaction destroys platelets (HIT) | 5-14 days after starting |
| Anticonvulsants | Valproic acid, phenytoin, carbamazepine | Direct bone marrow suppression | 7-21 days |
| Antibiotics | Vancomycin, linezolid, rifampin, sulfonamides | Immune-mediated destruction | 1-3 weeks |
| Chemotherapy | Nearly all cancer drugs | Kills rapidly dividing bone marrow cells | 7-14 days per cycle |
| H2 Blockers | Cimetidine, ranitidine | Rare immune reaction | 2-4 weeks |
| Diuretics | Hydrochlorothiazide, furosemide | Immune mechanism | Variable |
| Antiplatelets | Abciximab, eptifibatide | Direct platelet destruction | 2-7 days |
Timeline note: Most medication-induced thrombocytopenia develops within 7-14 days of starting the drug. If you’ve been taking a medication for years without problems, it’s less likely to suddenly cause low platelets—though it remains possible.
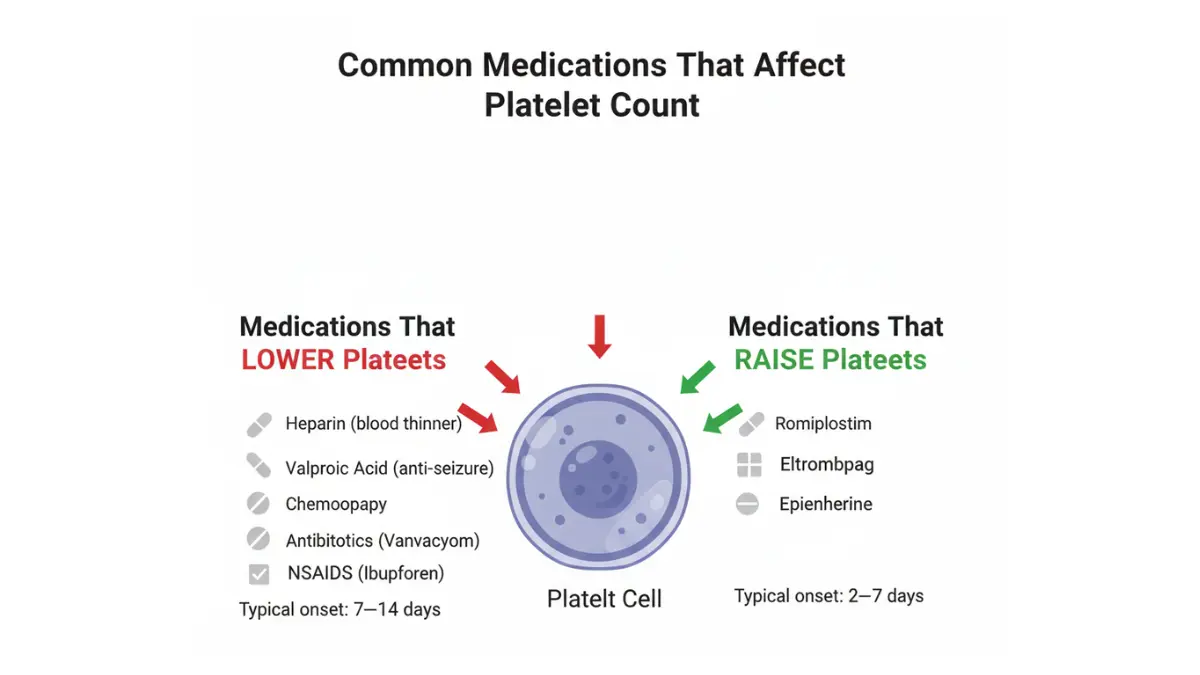
Drugs That RAISE Platelets
These medications are far less common but can cause reactive thrombocytosis:
- All-trans retinoic acid (ATRA) – Used for acute promyelocytic leukemia treatment
- Epinephrine – Emergency allergy medication can temporarily spike counts
- Tretinoin – Prescription acne medication rarely causes elevation
- Romiplostim (Nplate) and Eltrombopag (Promacta) – These are intentional platelet boosters prescribed to treat chronic ITP
What to Do If You’re Taking These Medications
❌ DO NOT stop prescription medications without your doctor’s explicit approval. Stopping certain drugs abruptly (especially anticonvulsants, blood thinners, or heart medications) can cause serious complications including seizures, stroke, or heart attack.
✅ DO inform your doctor of:
- Exactly when you started each medication
- Whether you had normal platelet counts before starting the drug
- Any bleeding symptoms like unusual bruising, prolonged cuts, or nosebleeds
- All supplements and vitamins (many people forget to mention these)
Your doctor will weigh the risks of continuing the medication against the benefits for your primary condition. Often, switching to an alternative medication in the same class resolves the platelet problem while continuing effective treatment for your underlying disease.
Retesting Timeline + FAQs
When to Retest Your Platelet Count
Appropriate retest timing depends on your initial count severity, underlying cause, and whether you’ve started treatment. Following evidence-based guidelines from the American Society of Hematology, here’s when your doctor will likely reorder bloodwork:
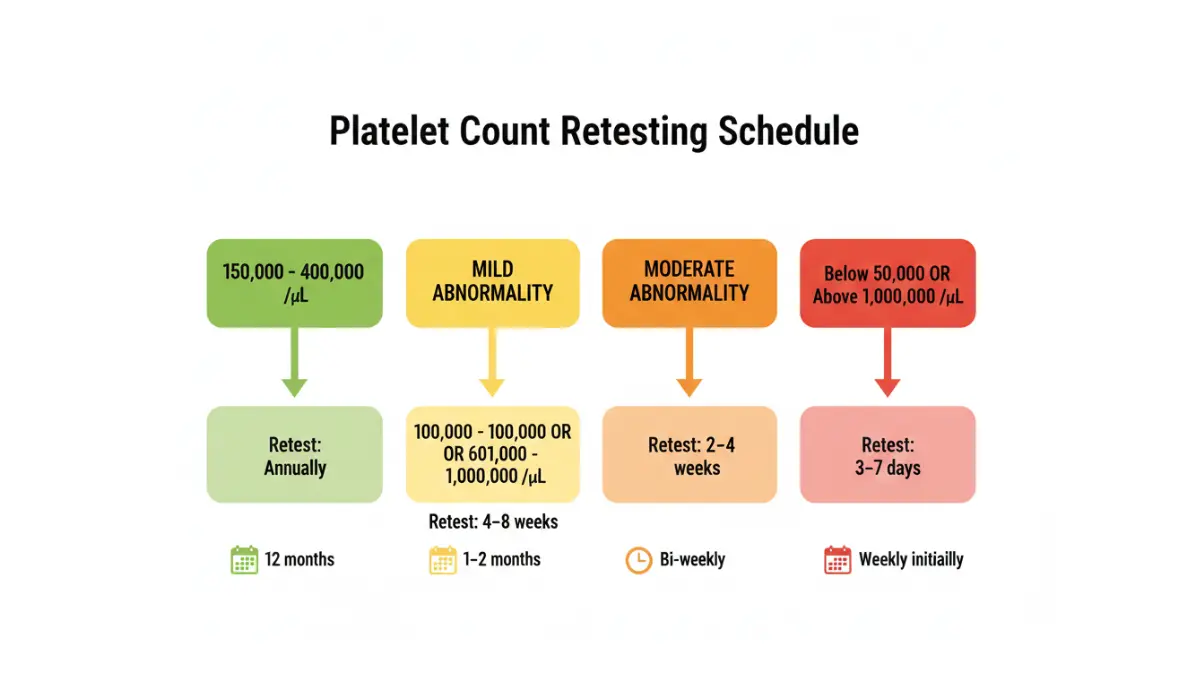
🟢 Normal range (150,000-400,000/µL):
- Retest interval: Annual physical exam
- Retest sooner if: Starting chemotherapy, pregnancy, developing new symptoms like unexplained bruising
- Purpose: Routine health screening
🟡 Mild abnormality (100,000-149,000 OR 401,000-600,000/µL):
- Retest interval: 4-8 weeks
- Purpose: Confirm the abnormality wasn’t temporary or lab error, identify trends
- Action: Your doctor investigates underlying causes during this period
🟠 Moderate abnormality (50,000-100,000 OR 600,000-1,000,000/µL):
- Retest interval: 2-4 weeks initially, then monthly once stable
- Purpose: Monitor stability and response to treatment
- Action: Likely specialist referral if counts don’t improve
🔴 Severe abnormality (below 50,000 OR above 1,000,000/µL):
- Retest interval: 3-7 days initially, then weekly during active treatment
- Purpose: Assess immediate treatment response and adjust therapy
- Action: Close medical supervision required
After treatment stabilizes your count:
- Weekly monitoring for 4 weeks
- Monthly checks for 3 months
- Every 3 months for 1 year
- Every 6-12 months thereafter as maintenance monitoring
Understanding Your Complete CBC Report
Your platelet count doesn’t exist in isolation. Other values on your complete blood count provide critical context that helps your doctor determine the underlying cause:
Mean Platelet Volume (MPV):
- Normal range: 7.5-11.5 femtoliters (fL)
- High MPV + low platelet count = Your bone marrow is producing new platelets rapidly, but something is destroying them in your bloodstream (suggests ITP, drug reaction, or consumption)
- Low MPV + low platelet count = Your bone marrow isn’t producing enough platelets (suggests bone marrow disorder, B12/folate deficiency, or marrow suppression)
Platelet Distribution Width (PDW):
- Normal range: 10-17%
- Elevated PDW indicates your platelets vary significantly in size, suggesting active platelet production as your bone marrow tries to compensate for losses
- Useful for distinguishing reactive thrombocytosis from primary bone marrow disorders
White Blood Cell Count:
- Low platelets + low white cells + low red cells = Suggests bone marrow failure (aplastic anemia, leukemia, or bone marrow infiltration)
- High platelets + high white cells = Often indicates infection, inflammation, or certain blood cancers
Hemoglobin and Hematocrit:
- Low hemoglobin + high platelets = Classic combination for iron deficiency anemia causing reactive thrombocytosis
- Low hemoglobin + low platelets = Suggests bleeding disorder, bone marrow problem, or B12/folate deficiency
If you’re managing multiple health metrics, understanding your complete metabolic picture through tools like our Ideal Weight Calculator and Water Intake Calculator helps ensure proper nutrition that supports healthy blood cell production.
Most Common Questions About Platelet Count
1. Can stress affect my platelet count?
Yes, but minimally. Acute stress (surgery, trauma, intense exercise) can temporarily raise platelets by 10-15% for 1-2 hours as your body releases stored platelets from your spleen. Chronic psychological stress may cause mild elevation (5-10%) through inflammatory pathways. Neither typically causes clinically significant changes requiring treatment.
2. Does exercise change platelet levels?
Intense exercise temporarily increases platelet count by 20-30% for 1-2 hours post-workout. This is normal and protective—your body prepares for potential injuries by increasing clotting capacity. Extreme endurance athletes (marathon runners, ultra-cyclists) may maintain chronically elevated baseline counts of 400,000-600,000/µL due to repeated exercise-induced inflammation.
3. Will my platelet count return to normal?
This depends entirely on the cause. Secondary thrombocytosis (reactive high platelets) usually normalizes within 4-12 weeks once you treat the underlying condition. Medication-induced changes typically reverse 7-14 days after stopping the offending drug. Primary bone marrow disorders like essential thrombocythemia require long-term management and counts may never fully normalize without medication.
4. Can diet affect platelet count?
Indirectly, yes. Iron deficiency from inadequate dietary iron or poor absorption can raise platelet counts. Vitamin B12 and folate deficiency can lower counts. However, no specific foods directly increase or decrease platelet production in healthy individuals. Alcohol abuse significantly lowers counts through direct bone marrow toxicity.
5. Are platelet count changes noticeable?
Usually no. Most people feel completely normal with mild to moderate abnormalities (100,000-600,000/µL). Symptoms typically only appear at extremes—below 50,000/µL you might notice easy bruising and prolonged bleeding, while above 1,000,000/µL can cause headaches, dizziness, or vision changes.
6. Can I donate blood with abnormal platelet count?
Most blood donation centers require 150,000-400,000/µL for whole blood donation. Platelet-specific donation (plateletpheresis) requires a minimum of 150,000/µL but prefers donors with counts above 200,000/µL since the procedure removes a large quantity of platelets. Check with your local blood bank for specific requirements, as standards vary by facility.
7. Should I take supplements to change my platelet count?
Only if blood tests confirm a specific deficiency. Taking iron supplements when you’re not iron deficient won’t lower high platelets—it might actually raise them further. Similarly, random platelet-boosting supplements lack scientific evidence and may interfere with medications or blood testing. Always consult your doctor before starting any supplement regimen.
8. How long until medication-induced changes reverse?
Most medication-induced thrombocytopenia resolves within 7-14 days after stopping the offending drug. Your platelets completely turn over every 8-10 days, so once the medication clears your system, your bone marrow replaces destroyed platelets with new, healthy ones. Some drugs (like gold therapy or certain antibiotics) can cause prolonged suppression lasting 4-8 weeks.
9. What’s the difference between platelets and white blood cells?
Platelets are cell fragments (not complete cells) that primarily stop bleeding by forming clots. White blood cells are complete cells that fight infections and foreign invaders. Your body makes them in different areas of bone marrow and they have completely different functions—you need both for optimal health. Low platelets increase bleeding risk but don’t affect infection fighting ability.
10. Can platelet count predict serious disease?
Sometimes. Persistent unexplained high platelet counts (especially above 600,000/µL lasting more than 3 months) warrant thorough cancer screening, as 6-8% of cases stem from hidden malignancies. Very low counts (below 50,000/µL) that don’t respond to treatment may indicate bone marrow disorders or leukemia. However, most abnormal platelet counts have benign causes—infection, medication reactions, or nutritional deficiencies.
11. Do I need a hematologist for abnormal results?
Not always. Your primary care doctor can manage most mild abnormalities (100,000-149,000 or 400,000-600,000/µL) by treating underlying causes. Hematology referral becomes necessary when counts are severely abnormal (below 50,000 or above 1,000,000/µL), fail to normalize after 8-12 weeks of treatment, require specialized medications, or when your doctor suspects primary bone marrow disorders.
Key Takeaways
Your platelet count is one number in your complete health picture. An abnormal result doesn’t automatically mean serious disease—it’s a signal to investigate further with your doctor’s guidance.
Remember these essential points:
- Most platelet abnormalities are mild and temporary
- Secondary causes (infection, medication, inflammation) are 10-20 times more common than primary blood disorders
- Early detection through routine screening prevents complications
- Your personal baseline and trends matter more than single isolated numbers
- Treatment success depends on identifying and addressing the root cause
Understanding related blood work results helps you see the complete picture—if you’ve also had inflammatory markers tested, our guides on CRP test results and ESR levels provide the same clear, actionable explanations.
Medical Disclaimer
This article is for educational purposes only and does not constitute medical advice. Platelet count interpretation requires consideration of your complete medical history, symptoms, other laboratory values, and clinical context that only your healthcare provider can properly evaluate. Always discuss your specific results with your doctor or a qualified hematologist.
Never stop prescribed medications or delay seeking medical care based solely on information from this article. If you have a medical emergency or experience symptoms like uncontrolled bleeding, severe headache, chest pain, or difficulty breathing, call 911 or go to your nearest emergency room immediately.
Additional Resources:
- Explore our complete health library at MyMedicineAdvisor Health Tips
- Track your overall wellness with our comprehensive health tools
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.