On This Page – Quick Medical Summary
What Your Ferritin Levels Really Mean
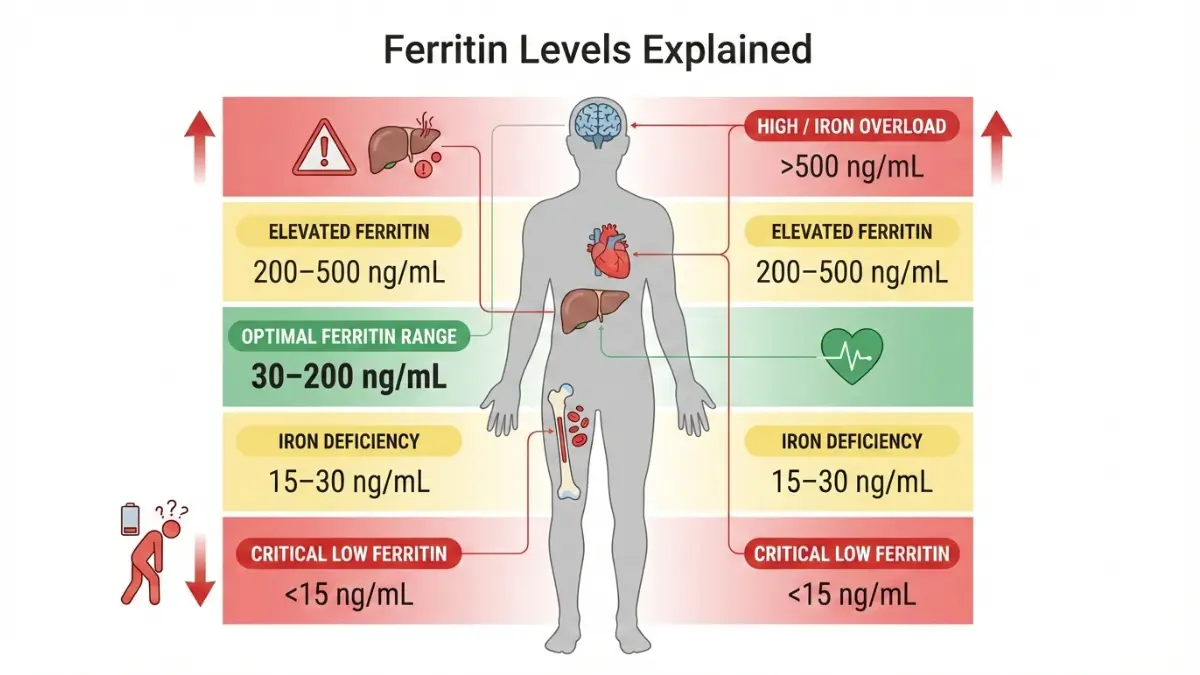
Ferritin Levels: 12-500+ What Each Result Really Means
When Jennifer received her lab results showing a ferritin level of 18 ng/mL, she felt confused and anxious. Her doctor said it was “within normal limits,” yet she could barely climb stairs without exhaustion. This disconnect between lab numbers and how you feel is why understanding your specific ferritin level matters more than just knowing if you’re “normal.”
Ferritin is a protein that stores iron in your body. When doctors measure your ferritin levels, they’re checking how much iron your body has in reserve—not how much is actively circulating in your bloodstream right now.
Here’s what you need to know immediately: your ferritin number tells a specific story about your iron status, energy capacity, and potential health risks. Whether your result is 12, 50, 200, or 500+, each range requires different actions.
Quick Ferritin Level Decoder
| Ferritin Level (ng/mL) | Status | What It Means | Action Required |
|---|---|---|---|
| Below 12 | 🔴 Critical | Severe iron depletion, cellular dysfunction | Emergency medical evaluation |
| 12-30 | 🟡 Deficient | Iron stores depleted, symptoms likely | Start iron supplementation protocol |
| 30-100 (Women) | 🟢 Normal-Low | Functional but may benefit from optimization | Monitor symptoms, consider dietary improvements |
| 100-200 (Women) / 100-300 (Men) | 🟢 Optimal | Healthy iron stores | Maintain current habits |
| 200-500 | 🟡 Elevated | Requires investigation for underlying cause | Additional blood tests needed |
| Above 500 | 🔴 High | Potential serious conditions | Urgent medical workup required |
The National Institutes of Health emphasizes that ferritin testing provides crucial information about iron stores that other iron tests might miss. Unlike serum iron, which fluctuates throughout the day, ferritin levels remain relatively stable and give doctors a clear picture of your long-term iron status.
Understanding Ferritin And Normal Ranges
What Ferritin Actually Measures (And Why It Matters)
Ferritin serves as your body’s iron warehouse. Think of it as a savings account for iron—when your body needs iron for essential functions like making red blood cells or supporting muscle metabolism, it withdraws from ferritin stores first.
Ferritin vs. Other Iron Tests
Many patients get confused when they have multiple iron-related results. Here’s how ferritin differs from other iron markers:
| Test | What It Measures | Why It Matters |
|---|---|---|
| Ferritin | Stored iron in tissues | Long-term iron status, early deficiency detection |
| Serum Iron | Circulating iron in blood | Immediate availability, fluctuates with meals |
| TIBC (Total Iron-Binding Capacity) | Blood’s capacity to carry iron | Shows how hard body is working to transport iron |
| Hemoglobin | Oxygen-carrying protein in red blood cells | Late indicator, drops only after stores depleted |
Your doctor checks ferritin first because it drops long before hemoglobin falls. By the time you develop anemia (low hemoglobin), your ferritin has likely been depleted for months. For those monitoring overall metabolic health, understanding your BMR and calorie needs can help optimize iron absorption through proper nutrition timing.
Normal Ferritin Range by Age and Gender (2026 Guidelines)
The standard “normal” lab range doesn’t tell the whole story. According to the American Society of Hematology, optimal ferritin levels vary significantly by age, gender, and life stage.
Women’s Ferritin Levels
Premenopausal Women (Ages 18-50):
- Lab “normal”: 15-150 ng/mL
- Optimal range: 50-150 ng/mL
- Below 30 ng/mL causes symptoms even if labeled “normal”
Why Women Need Special Attention: Monthly menstrual bleeding depletes iron stores continuously. Women lose approximately 30-40 mg of iron per period. The pregnancy weight gain calculator can help expectant mothers track additional nutritional needs, as pregnancy significantly impacts ferritin levels.
Postmenopausal Women (50+ years):
- Normal range: 30-200 ng/mL
- After menopause, ferritin typically increases as monthly iron loss stops
Pregnancy Ferritin Adjustments:
- First trimester: Maintain 30-50 ng/mL minimum
- Second trimester: Target 40-60 ng/mL
- Third trimester: Critical threshold 50+ ng/mL (baby’s iron stores developing)
Men’s Ferritin Levels
Adult Men (Ages 18-70+):
- Lab normal: 30-400 ng/mL
- Optimal range: 100-300 ng/mL
- Above 300 ng/mL warrants investigation
Men naturally maintain higher ferritin levels due to testosterone’s effect on red blood cell production and absence of menstrual blood loss.
Children’s Ferritin Ranges
| Age Group | Normal Range (ng/mL) |
|---|---|
| 1-5 years | 12-80 |
| 6-12 years | 15-100 |
| 13-17 years | Boys: 20-200 / Girls: 15-150 |
Why “Normal” Doesn’t Always Mean “Optimal”
Jessica’s ferritin measured 35 ng/mL—technically within the lab’s normal range of 15-150 ng/mL. Yet she experienced severe fatigue, hair loss, and restless legs at night. After supplementation raised her ferritin to 75 ng/mL, all symptoms resolved within 12 weeks.
This illustrates a critical gap: lab reference ranges capture 95% of the population, including people with mild deficiency symptoms. Many functional medicine practitioners and hematologists now recognize that ferritin below 50 ng/mL often causes symptoms in women, regardless of what the lab report says.
The Cleveland Clinic notes that iron deficiency symptoms can appear well before anemia develops, making ferritin testing crucial for early detection. If you’re experiencing unexplained fatigue alongside other concerning symptoms, using a symptom checker can help identify patterns worth discussing with your doctor.
Low Ferritin Levels – Complete Guide
Low Ferritin Levels: Causes, Symptoms & Treatment
Low ferritin represents one of the most common nutritional deficiencies worldwide, affecting approximately 2 billion people according to World Health Organization data. Yet it remains underdiagnosed because early symptoms mimic stress or poor sleep.
Critical Deficiency (Below 15 ng/mL)
When ferritin drops below 15 ng/mL, your body enters crisis mode. At this level, cells throughout your body lack sufficient iron to function properly. Mitochondria—the powerhouses of your cells—cannot produce adequate energy.
Emergency Symptoms Requiring Immediate Medical Attention:
- Severe weakness making it difficult to stand or walk
- Chest pain or pressure, especially with minimal activity
- Extreme shortness of breath at rest
- Rapid or irregular heartbeat (palpitations)
- Dizziness with near-fainting episodes
At critically low ferritin levels, doctors often recommend intravenous iron infusions rather than oral supplements. The National Heart, Lung, and Blood Institute confirms that severe iron deficiency requires aggressive treatment to prevent cardiac complications.
Iron Deficiency Range (15-30 ng/mL)
This is the most commonly missed diagnosis range. Lab reports may say “normal,” but your body is already struggling.
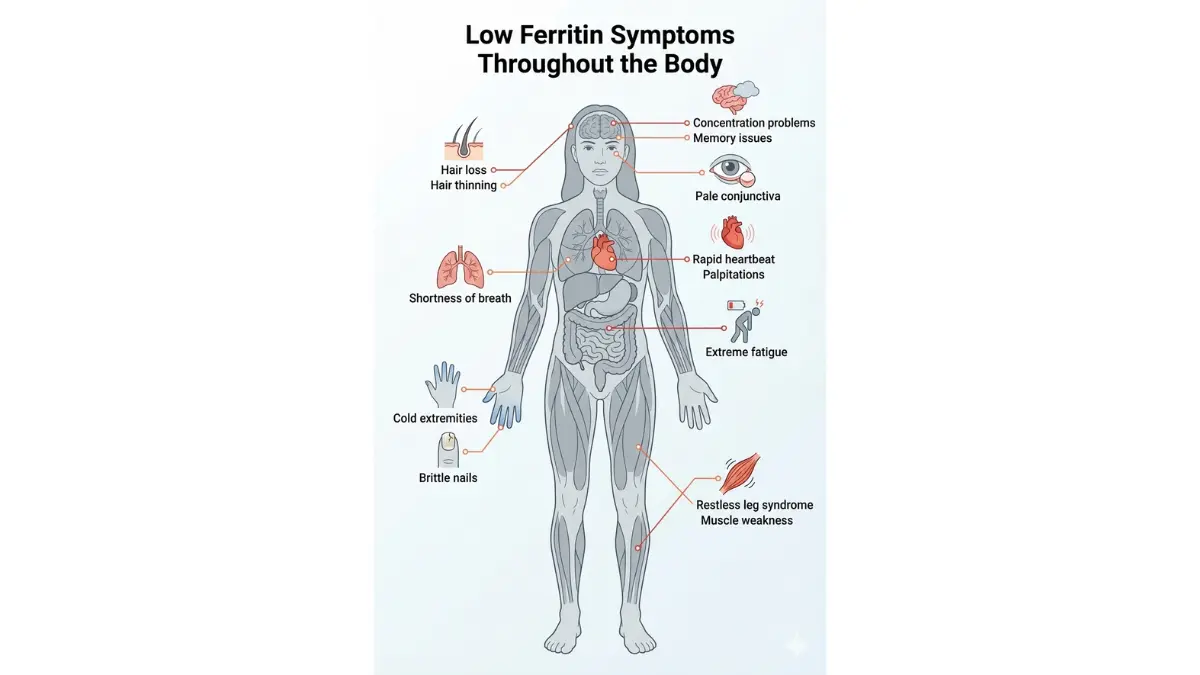
Classic Low Ferritin Symptoms:
- Extreme fatigue: Not improved even after 8-10 hours of sleep
- Restless leg syndrome: Uncomfortable sensations in legs, worse at night
- Hair loss: Especially noticeable in women, may lose 100-200+ hairs daily
- Brittle nails: Spoon-shaped nails (koilonychia) in severe cases
- Pale skin and mucous membranes: Check inside lower eyelids
- Cold intolerance: Constantly feeling cold, especially hands and feet
- Brain fog: Difficulty concentrating, poor memory, mental exhaustion
- Rapid heartbeat: Heart works harder to deliver oxygen with fewer red blood cells
- Shortness of breath: Particularly noticeable during physical activity
Michael, a 42-year-old marathon runner, saw his performance decline drastically over six months. His ferritin had dropped to 22 ng/mL despite eating a balanced diet. After supplementation brought his level to 85 ng/mL, his race times improved by 8% within three months. Athletes often need to monitor ferritin alongside their heart rate zones to optimize training capacity.
Common Causes of Low Ferritin
Understanding why your ferritin dropped is essential for preventing recurrence:
Heavy Menstrual Bleeding (Leading Cause in Women):
- Periods lasting more than 7 days
- Soaking through pads/tampons every 1-2 hours
- Passing large clots
- May lose 60-80+ mg iron per cycle
Pregnancy and Breastfeeding:
- Developing baby requires 300-500 mg iron during pregnancy
- Breastfeeding depletes maternal iron stores
- Using a pregnancy due date calculator helps women plan iron supplementation throughout pregnancy
Vegetarian/Vegan Diet Without Proper Supplementation:
- Plant-based iron (non-heme) has only 2-10% absorption rate
- Animal iron (heme) absorbs at 15-35% rate
- Vegan athletes particularly vulnerable
Gastrointestinal Bleeding:
- Ulcers, polyps, gastritis
- Often asymptomatic until ferritin severely depleted
- May need endoscopy if ferritin doesn’t respond to supplementation
Celiac Disease and Inflammatory Bowel Disease:
- Damaged intestinal lining cannot absorb iron properly
- Associated with other nutritional deficiencies too
- Requires treatment of underlying condition plus supplementation
Frequent Blood Donation:
- Each donation removes 200-250 mg iron
- Body needs 3-6 months to fully replace iron from one donation
- Frequent donors should check ferritin every 6 months
Intense Endurance Training:
- “Foot strike hemolysis” destroys red blood cells
- Increased iron loss through sweat
- Higher red blood cell production demands
For those examining their complete blood count results, low ferritin often appears before changes in hemoglobin or hematocrit.
How to Raise Ferritin Levels (Evidence-Based Protocol)
Supplementation Strategy:
Elemental iron dosing varies by supplement type:
- Ferrous sulfate: 325 mg tablet contains 65 mg elemental iron (20%)
- Ferrous gluconate: 325 mg tablet contains 36 mg elemental iron (11%)
- Iron bisglycinate: Better absorbed, causes less gastrointestinal upset
Optimal Dosing Protocol:
- Take 65-200 mg elemental iron daily
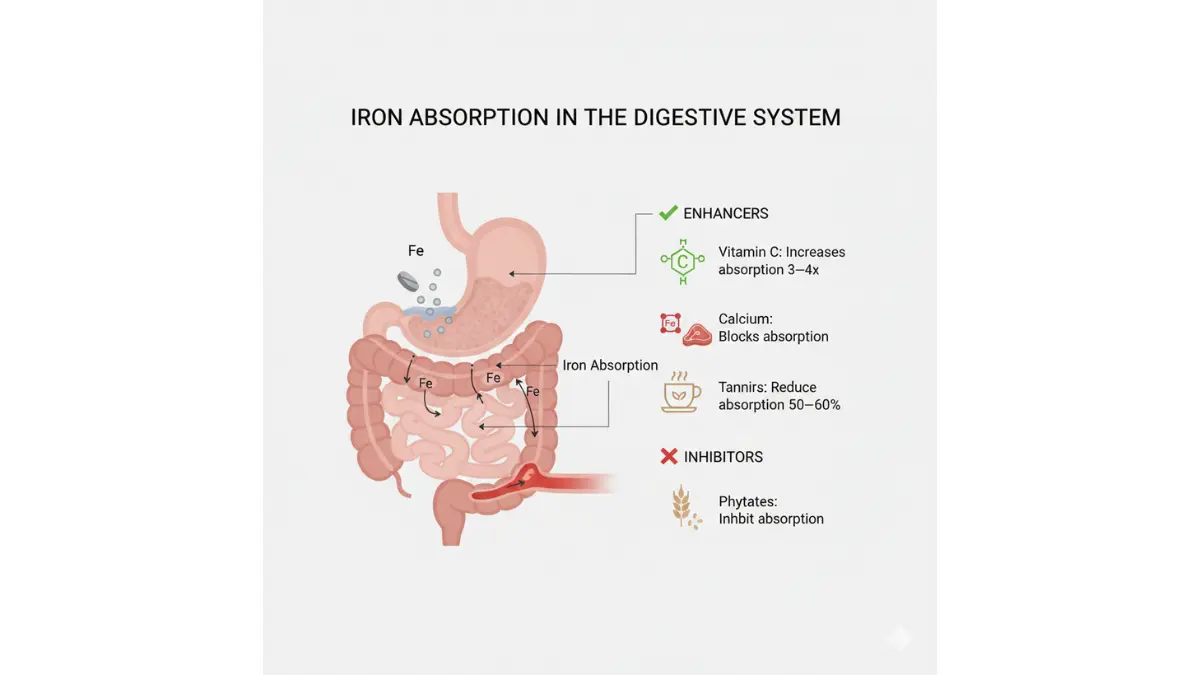
- Consume on empty stomach when possible (1 hour before or 2 hours after meals)
- Pair with 500 mg vitamin C to increase absorption by 3-4x
- Avoid within 2 hours: Calcium supplements, dairy products, tea, coffee, antacids
Expected Timeline:
- Week 1-4: Side effects peak (nausea, constipation, dark stools)
- Week 4-8: Energy may begin improving
- Week 8-12: Recheck ferritin—should increase 20-50 ng/mL
- Month 4-6: Ferritin reaches optimal levels if compliant
Research published by the National Institutes of Health shows that iron absorption increases significantly when taken with vitamin C, making this combination essential for rapid recovery.
Dietary Iron Sources:
Heme Iron (Animal Sources – 15-35% Absorption):
- Beef liver: 5 mg per 3 oz
- Oysters: 8 mg per 3 oz
- Beef: 2-3 mg per 3 oz
- Chicken: 1-2 mg per 3 oz
Non-Heme Iron (Plant Sources – 2-10% Absorption):
- Spinach (cooked): 3 mg per 1/2 cup
- Lentils: 3 mg per 1/2 cup
- Fortified cereals: 18 mg per serving
- Tofu: 3 mg per 1/2 cup
- Dark chocolate: 3 mg per oz
Pro Tip: Eating meat with plant iron sources increases absorption of both. Pair iron-rich meals with vitamin C sources like citrus, tomatoes, or bell peppers.
Real Case Example – Low Ferritin Recovery
Patient: Rachel, 32-year-old teacher
- Initial Ferritin: 14 ng/mL
- Symptoms: Exhaustion despite 9 hours sleep, severe hair loss, restless legs preventing sleep, cold hands even in summer
- Underlying Cause: Heavy periods (7-day duration, moderate-heavy flow)
- Treatment Protocol:
- 325 mg ferrous sulfate daily (65 mg elemental iron)
- Taken with orange juice (vitamin C boost)
- Avoided coffee for 2 hours after dose
- Used water intake calculator to stay hydrated and reduce constipation
- 8-Week Recheck: Ferritin 62 ng/mL
- Outcome: Complete symptom resolution by week 10, hair regrowth visible at 4 months, restless legs eliminated
Rachel’s case demonstrates why checking ferritin early matters. She had suffered for 18 months before diagnosis, assuming her fatigue was just from her demanding job.
High Ferritin Levels: When to Worry and What to Do
Elevated ferritin presents a diagnostic challenge because it doesn’t automatically mean iron overload. Ferritin acts as an acute-phase reactant—it rises during inflammation, infection, or tissue damage even when iron levels are normal.
Moderately Elevated (200-500 ng/mL)
This range requires investigation but rarely represents an emergency. Context is everything.
Common Causes of Moderate Elevation:
- Acute infection or inflammation: Flu, pneumonia, COVID-19
- Chronic liver disease: Fatty liver, hepatitis, cirrhosis
- Metabolic syndrome: Obesity, insulin resistance, type 2 diabetes (check your ideal weight and metabolic markers)
- Alcohol consumption: Even moderate drinking elevates ferritin
- Hyperthyroidism: Overactive thyroid increases iron turnover
- Recent injury or surgery: Tissue damage releases stored ferritin
- Certain medications: Estrogen, testosterone, iron supplements
Next Steps When Ferritin is 200-500 ng/mL:
- Request inflammatory markers: CRP, ESR
- Check liver function tests (ALT, AST, bilirubin)
- Complete iron panel: serum iron, TIBC, transferrin saturation
- Fasting glucose and hemoglobin A1c (rule out diabetes)
- Consider hepatitis B and C screening
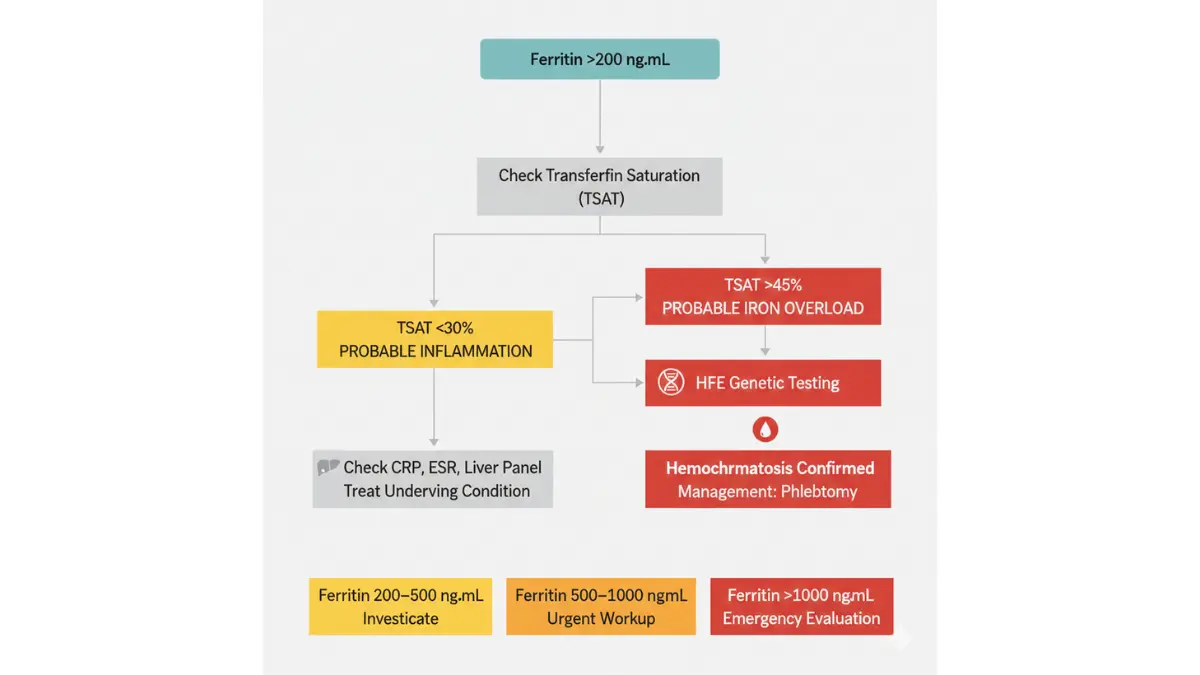
The Mayo Clinic explains that elevated ferritin with normal transferrin saturation usually indicates inflammation rather than iron overload, changing the entire treatment approach.
Severely Elevated (500-1000 ng/mL)
This range demands urgent investigation. While inflammation can still cause these levels, iron overload conditions become more likely.
Primary Concerns:
- Hereditary hemochromatosis: Genetic condition causing excess iron absorption
- Liver cirrhosis: Advanced liver damage
- Joint damage risk: Iron deposits in joints, especially knuckles, causing arthritis
- Cardiac complications: Iron accumulation in heart muscle
- Endocrine dysfunction: Diabetes, hypogonadism from iron in glands
Critical Tests at This Level:
- HFE genetic testing: Checks for C282Y and H63D mutations
- Transferrin saturation: If >45%, strongly suggests hemochromatosis
- Liver MRI or FibroScan: Assesses liver iron content and damage
- Echocardiogram: Rules out cardiac iron deposition
Thomas, a 48-year-old accountant, discovered his ferritin was 720 ng/mL during routine blood work. He felt fine and attributed occasional joint stiffness to aging. Genetic testing revealed he was homozygous for the C282Y mutation—hereditary hemochromatosis. Without treatment, he faced a 30% risk of cirrhosis by age 60.
Dangerously High (Above 1000 ng/mL)
Ferritin exceeding 1000 ng/mL requires immediate medical evaluation. This level may indicate life-threatening conditions beyond simple iron overload.
Critical Conditions to Rule Out:
- Adult-onset Still’s disease: Rare inflammatory disorder
- Hemophagocytic lymphohistiocytosis (HLH): Life-threatening immune activation
- Advanced cirrhosis or liver failure
- Certain malignancies: Leukemia, lymphoma, advanced solid tumors
- Severe infections: Sepsis, severe COVID-19
Emergency Protocol:
- Hospital admission may be required
- Comprehensive metabolic panel
- Complete blood count with differential
- Bone marrow biopsy if malignancy suspected
- Intensive care monitoring if hemophagocytic syndrome considered
High Ferritin With Normal Iron Studies
This pattern confuses many patients and doctors. Your ferritin is 400 ng/mL, but serum iron and transferrin saturation are normal—what does this mean?
Key Insight: Ferritin rises as an inflammatory marker, similar to C-reactive protein or ESR. Think of it as your body’s alarm system responding to inflammation or infection.
Common Scenarios:
- Chronic inflammatory conditions (rheumatoid arthritis, lupus)
- Ongoing infection (sometimes subclinical)
- Liver inflammation (non-alcoholic fatty liver disease)
- Obesity-related inflammation
This pattern actually rules out iron overload, redirecting investigation toward inflammatory causes. For comprehensive evaluation, reviewing your complete metabolic panel helps identify liver or kidney involvement.
Treatment for Iron Overload
When high ferritin results from true iron overload (high ferritin + high transferrin saturation), treatment focuses on removing excess iron.
Therapeutic Phlebotomy Protocol:
- Remove 500 mL blood every 1-2 weeks initially
- Continue until ferritin drops below 100 ng/mL
- Maintenance: Remove blood every 2-4 months to keep ferritin 50-100 ng/mL
- Each session removes approximately 200-250 mg iron
- Similar to blood donation but prescribed medically
Dietary Modifications:
- Reduce red meat consumption (high heme iron)
- Avoid iron supplements and multivitamins with iron
- Limit vitamin C supplements (enhances iron absorption)
- Drink tea with meals (tannins inhibit iron absorption)
- Consider calcium supplements with meals (blocks iron uptake)
Medications:
- Iron chelators (deferasirox, deferoxamine) if phlebotomy not possible
- Reserved for patients who cannot tolerate blood removal
Real Case Example – High Ferritin Discovery
Patient: David, 45-year-old engineer
- Initial Ferritin: 780 ng/mL (discovered during pre-employment physical)
- Symptoms: Mild joint stiffness in hands, no other complaints
- Workup Results:
- Transferrin saturation: 68% (severely elevated)
- HFE gene test: C282Y homozygous (hereditary hemochromatosis confirmed)
- Liver MRI: Grade 2 iron overload, early fibrosis
- Treatment: Therapeutic phlebotomy every 2 weeks for 6 months
- 6-Month Results: Ferritin 120 ng/mL, joint pain resolved, liver enzymes normalized
- Long-term Plan: Maintenance phlebotomy every 3 months
- Key Takeaway: Early detection prevented cirrhosis and diabetes
David’s case illustrates why screening family members matters. His two siblings were tested—one brother also had hemochromatosis and started treatment before developing any organ damage.
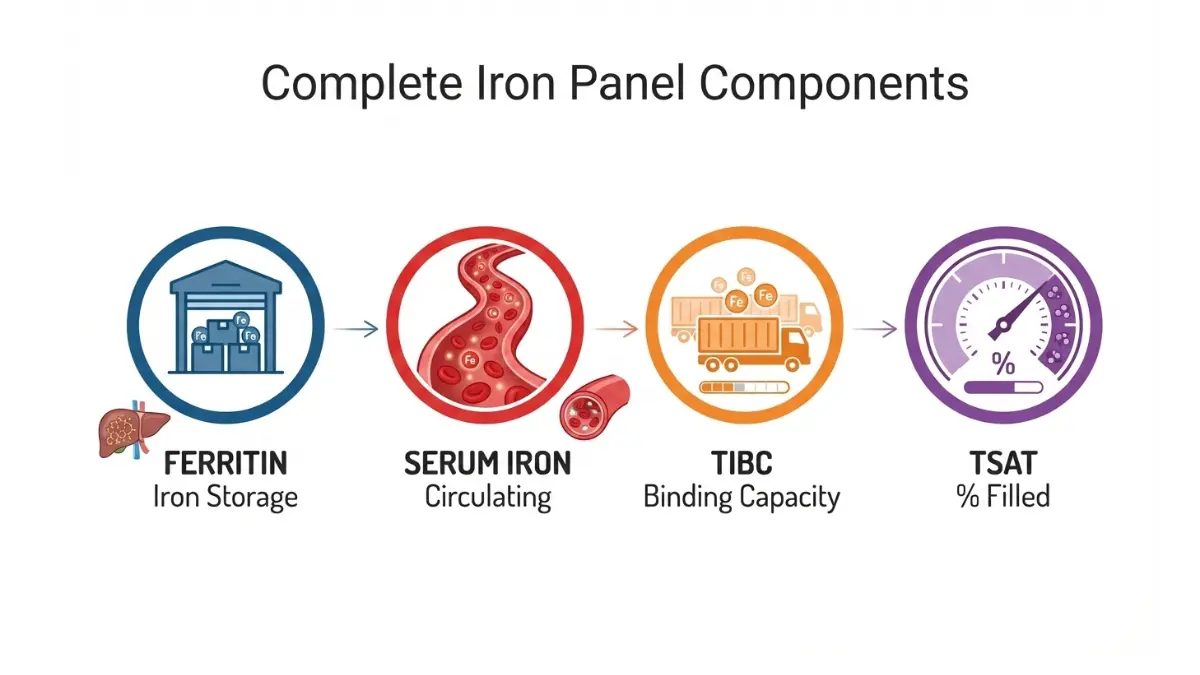
Beyond Ferritin: Understanding Your Complete Iron Panel
Ferritin tells only part of your iron story. A complete iron panel provides the full picture of how your body stores, transports, and utilizes iron.
The Four Key Iron Markers
| Test | What It Measures | Normal Range | What Low Means | What High Means |
|---|---|---|---|---|
| Ferritin | Stored iron in tissues | Women: 30-200 ng/mL<br>Men: 30-300 ng/mL | Depleted iron stores, imminent deficiency | Iron overload or inflammation |
| Serum Iron | Iron circulating in blood right now | 60-170 µg/dL | Active iron deficiency, poor absorption | Excess iron, hemochromatosis risk |
| TIBC (Total Iron-Binding Capacity) | Blood’s maximum capacity to carry iron | 240-450 µg/dL | Iron overload (body needs less capacity) | Iron deficiency (body increases capacity to find iron) |
| TSAT (Transferrin Saturation) | Percentage of iron-binding sites filled | 20-50% | Insufficient iron delivery to tissues | Excess iron absorption or release |
Think of these markers like checking your car’s fuel system: ferritin is the fuel tank, serum iron is the fuel in the fuel line, TIBC is the size of your fuel line, and TSAT tells you what percentage of the line is filled.
Pattern Recognition – What Combinations Mean
Understanding how these markers interact reveals your true iron status better than any single test.
Pattern 1: True Iron Deficiency
- Low ferritin (<30 ng/mL)
- Low serum iron (<60 µg/dL)
- High TIBC (>400 µg/dL)
- Low TSAT (<20%)
- Interpretation: Body has depleted stores and is desperately trying to absorb more iron
- Action: Iron supplementation required
Pattern 2: Inflammation (Not Iron Overload)
- High ferritin (>200 ng/mL)
- Normal or low serum iron
- Normal or low TIBC
- Low or normal TSAT (<30%)
- Interpretation: Ferritin rising as inflammatory marker, not excess iron
- Action: Investigate inflammatory cause, do NOT remove iron
Pattern 3: Hemochromatosis/Iron Overload
- High ferritin (>300 ng/mL)
- High serum iron (>170 µg/dL)
- Normal or low TIBC
- High TSAT (>50%)
- Interpretation: Genuine iron overload requiring treatment
- Action: Genetic testing, consider phlebotomy
Pattern 4: Early Deficiency or Recent Blood Loss
- Normal ferritin (30-100 ng/mL)
- Low serum iron (<60 µg/dL)
- High TIBC (>400 µg/dL)
- Low TSAT (<15%)
- Interpretation: Circulating iron depleted but stores not yet critically low
- Action: Identify and treat blood loss source, supplement preventively
Laboratory testing guidelines from the National Institute of Standards and Technology emphasize that comprehensive iron assessment requires all four markers, not ferritin alone.
Action Steps Based on Your Results
Protocol for Ferritin <30 ng/mL (Iron Deficiency):
Week 1-2:
✓ Start iron supplement (65-200 mg elemental iron daily)
✓ Take with vitamin C on empty stomach
✓ Avoid calcium, coffee, tea within 2 hours
✓ Expect side effects: dark stools, mild nausea, constipation
Week 4-6:
✓ Side effects should improve as body adjusts
✓ Monitor energy levels—should start improving
✓ Continue supplementation consistently
✓ Use fiber and adequate hydration for constipation
Week 8-12:
✓ Recheck complete iron panel
✓ Target ferritin increase: 20-50 ng/mL from baseline
✓ If not improving: evaluate for absorption issues
✓ Consider GI workup (celiac test, H. pylori, endoscopy)
Month 4-6:
✓ Continue until ferritin reaches 50-100 ng/mL
✓ Symptoms should be resolved by this point
✓ Transition to maintenance dose or dietary management
For those tracking broader health metrics, monitoring your protein intake ensures adequate nutritional support for red blood cell production.
Protocol for Ferritin >300 ng/mL (Potential Overload):
Immediate Actions:
✓ Request additional blood tests (CMP, hepatic panel, CRP, ESR)
✓ Check transferrin saturation—if >45%, strongly consider hemochromatosis
✓ HFE genetic testing (C282Y and H63D mutations)
✓ Stop all iron supplements and multivitamins containing iron
✓ Limit dietary iron temporarily
Week 2-4:
✓ Specialist referral to hematology or gastroenterology
✓ Liver imaging (MRI or FibroScan) to assess iron deposition
✓ Echocardiogram if cardiac symptoms present
✓ Review family history for hemochromatosis
Ongoing Management:
✓ If hemochromatosis confirmed: therapeutic phlebotomy
✓ If inflammation-related: treat underlying condition
✓ Maintenance monitoring every 3-6 months
✓ Screen first-degree relatives if genetic condition found
When to Retest Your Ferritin Levels
Timing of follow-up testing depends on your initial result and treatment:
After Iron Supplementation: 8-12 weeks
- Allows time to see meaningful increase
- Earlier testing may miss gradual improvement
- Expect 20-50 ng/mL rise if compliant
After Treatment for High Ferritin: 3-6 months
- Phlebotomy: recheck after 6-8 sessions
- Inflammation treatment: assess response to underlying condition therapy
Routine Monitoring (History of Iron Issues): Annually
- Catch trends before symptoms develop
- Particularly important for menstruating women
- Athletes should test every 6 months
During Pregnancy: Each trimester
- First trimester: establish baseline
- Second trimester: adjust supplementation
- Third trimester: ensure adequate stores for delivery and breastfeeding
- Related monitoring with pregnancy weight tracking
If Asymptomatic and Normal: Every 2-3 years with routine physical
- Part of comprehensive metabolic screening
- Earlier if risk factors develop
Research from Johns Hopkins University indicates that regular ferritin monitoring in at-risk populations prevents both deficiency complications and overload damage when tracked appropriately.
Emergency Warning Signs: When to Seek Urgent Care
Most ferritin abnormalities allow time for careful evaluation, but certain combinations of lab results and symptoms demand immediate attention.
Critical Thresholds Requiring Emergency Room Visit
Ferritin Below 10 ng/mL PLUS Any of These Symptoms:
- Severe weakness: Cannot stand or walk without assistance
- Chest pain or pressure: Especially worsening with activity
- Shortness of breath at rest: Breathing difficulty even when sitting still
- Rapid or irregular heartbeat: Palpitations, heart racing over 120 bpm at rest
- Dizziness with near-fainting: Syncope episodes or pre-syncope
- Confusion or altered mental status: Brain fog progressing to disorientation
At critically low ferritin with these symptoms, your heart is working dangerously hard to deliver oxygen with insufficient red blood cells. Cardiac complications can develop rapidly.
Ferritin Above 1000 ng/mL PLUS Any of These Symptoms:
- Severe abdominal pain: Especially right upper quadrant (liver area)
- Jaundice: Yellow discoloration of skin or whites of eyes
- Confusion or altered mental state: May indicate liver failure or HLH
- Unexplained weight loss: More than 10 pounds without trying
- High fever with ferritin >5000 ng/mL: Potential hemophagocytic syndrome
These combinations may indicate life-threatening conditions like liver failure, hemophagocytic lymphohistiocytosis, or severe systemic disease requiring hospital-level care.
When to Schedule Urgent Doctor Visit (Within 24-48 Hours)
Not every abnormal ferritin requires an ER visit, but these situations need prompt medical evaluation:
Rapid Ferritin Changes:
- Ferritin doubled or halved in less than 3 months
- May indicate new bleeding source, developing hemochromatosis, or acute illness
New Symptoms With High Ferritin (>300 ng/mL):
- Joint pain, especially in knuckles or wrists
- Unexplained fatigue despite adequate sleep
- Bronze or gray skin discoloration
- Loss of libido or sexual function
Family History Red Flags:
- Parent or sibling diagnosed with hemochromatosis
- Your ferritin is >300 ng/mL
- Need genetic screening and early intervention
Persistent Symptoms Despite Normal Ferritin:
- Ongoing fatigue, hair loss, restless legs
- May need additional iron studies beyond ferritin
- Could indicate other conditions mimicking iron deficiency
For comprehensive symptom evaluation, using a clinical symptom checker can help document patterns to share with your physician.
Emergency Decision Flowchart
Your Ferritin Result
↓
Severe Symptoms Present?
↓
YES → Emergency Room Now (Call 911 if chest pain, severe weakness, confusion)
↓
NO → Moderate Symptoms?
↓
YES → Schedule Doctor Visit Within 48 Hours
↓
NO → Routine Follow-up (2-4 weeks acceptable)
According to emergency medicine protocols published by the Centers for Disease Control and Prevention, severe anemia symptoms with extremely low ferritin constitute a medical emergency due to cardiac strain risks.
The key is recognizing when an abnormal number transitions from “needs attention” to “needs attention NOW.” When in doubt, err on the side of caution—emergency departments would rather evaluate and reassure than miss a critical diagnosis.
Medical Disclaimer
This article is for educational and informational purposes only and does not constitute medical advice. Ferritin levels should always be interpreted by a qualified healthcare provider in the context of your complete medical history, symptoms, and other laboratory results. Individual circumstances vary significantly, and treatment protocols must be personalized to each patient’s specific situation. If you have concerns about your ferritin levels or experience severe symptoms such as chest pain, extreme weakness, difficulty breathing, or altered mental status, seek immediate medical attention. Never start, stop, or modify iron supplementation or any treatment without consulting your physician, as both iron deficiency and iron overload can have serious health consequences.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.