On This Page – Quick Medical Summary
Jennifer, a 42-year-old marketing executive from Seattle, stared at her lab report in disbelief. “ANA: Positive, Titer 1:160, Homogeneous Pattern.” Her hands trembled as she Googled frantically at 11 PM, wondering if this meant lupus or something worse. Three weeks later, after proper testing and monitoring, her rheumatologist confirmed she was perfectly healthy—just one of millions with a benign positive ANA test result.
Your ANA test came back positive, and you’re here because those numbers feel like a medical mystery. Whether your titer reads 1:40, 1:160, or higher, this chart-based guide decodes exactly what your ANA test results mean, which patterns matter most, and what happens next—all backed by January 2026 clinical guidelines from the American College of Rheumatology.
What is an ANA Test?
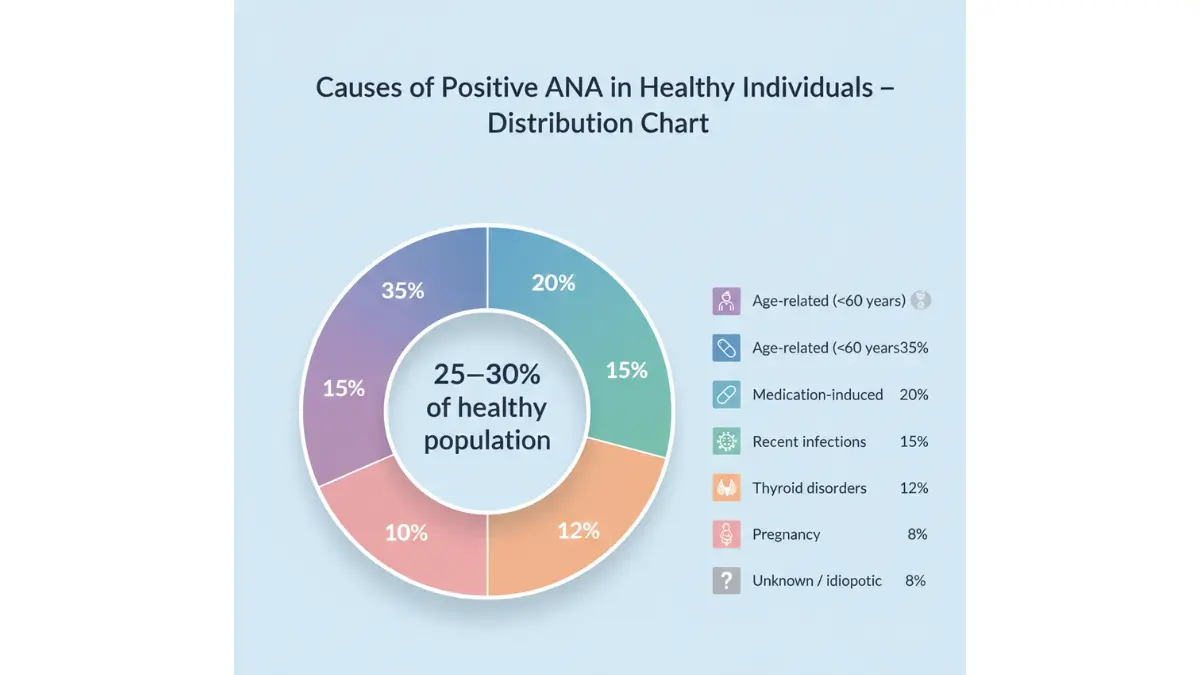
An antinuclear antibody (ANA) test measures autoantibodies that attack your cell nuclei. Doctors order this test when they suspect autoimmune conditions like lupus, Sjögren’s syndrome, or scleroderma. However, 20-30% of healthy adults test positive without any disease, according to NIH autoimmune research data.
Here’s What You’ll Learn:
- ✓ Exact titer level meanings (1:40 through 1:2560)
- ✓ Four major ANA patterns and their disease associations
- ✓ When to worry versus when to relax
- ✓ Complete next-steps action protocol
- ✓ Age-specific false positive rates (2026 data)
Quick Reference: Normal vs. Positive
Most laboratories consider ANA titers below 1:40 as negative. Titers of 1:80 or higher typically warrant further investigation, though context matters more than numbers alone. If you’re experiencing unexplained symptoms alongside your results, using a symptom checker can help identify patterns before your follow-up appointment.
Understanding Your Ana Titer Levels
What Your ANA Titer Numbers Actually Mean
ANA test results express antibody concentration through dilution ratios. A 1:160 titer means your blood was diluted 160 times and still tested positive. Higher numbers indicate stronger antibody presence, but they don’t automatically mean disease severity.
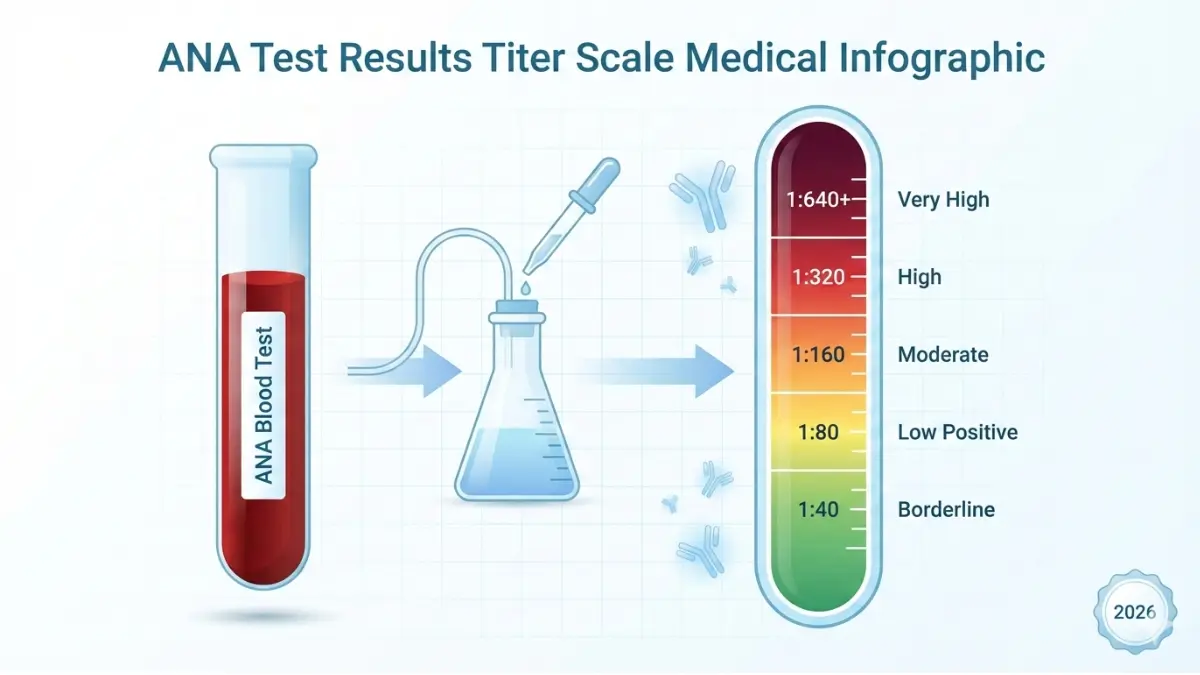
ANA Titer Scale Breakdown
| Titer Level | Interpretation | Clinical Significance | Recommended Action |
|---|---|---|---|
| 1:40 | Borderline/Low | 95% benign in healthy adults | Monitor symptoms only |
| 1:80 | Low Positive | Found in 20-30% of population | Retest in 6-12 months |
| 1:160 | Moderate | Further investigation needed | Additional autoimmune panels |
| 1:320 | High | Strong autoimmune indicator | Rheumatology referral within 4 weeks |
| 1:640+ | Very High | Likely autoimmune disease | Urgent specialist consultation |
Important Context: These thresholds represent general guidelines, but clinical context matters most. A patient with a 1:80 titer and severe joint pain requires more urgent workup than someone with 1:320 and zero symptoms.
Age-Specific False Positive Rates (2026 Data)
The Centers for Disease Control updated age-related false positive statistics in January 2026:
- Ages 20-30: 5% false positive rate
- Ages 40-50: 15% false positive rate
- Ages 60+: 32% false positive rate
- Pregnant women: 18-22% temporary elevation
Women show positive ANA results 2-3 times more frequently than men across all age groups. This gender disparity reflects genuine autoimmune disease prevalence plus higher benign positivity rates.
Real Patient Case: Michael’s Story
Michael, a 55-year-old construction supervisor from Dallas, tested positive at 1:160 during routine bloodwork for life insurance. He had no symptoms, no family history of autoimmune disease, and maintained excellent health through regular exercise tracked via his BMI calculator results. His rheumatologist monitored him annually for two years—his titer remained stable, and he never developed disease. This represents the most common outcome for isolated positive ANA tests in asymptomatic adults.
What Influences Titer Fluctuation
ANA titers can vary between tests due to:
- Recent infections (viral illnesses temporarily elevate antibodies)
- Medications (discussed in Section 5)
- Laboratory variation (different labs use different testing methods)
- Time of day (immune markers fluctuate with circadian rhythms and sleep patterns)
The Lupus Foundation of America recommends retesting at the same laboratory for accurate comparison, as different testing platforms (ELISA vs. immunofluorescence) yield different sensitivity levels.
Ana Pattern Types Decoded
Decoding Your ANA Pattern: What Each Type Reveals
Beyond titer numbers, your ANA test reports a specific cellular staining pattern visible under immunofluorescence microscopy. These patterns provide crucial diagnostic clues about which autoimmune condition might be present—or rule out disease entirely.
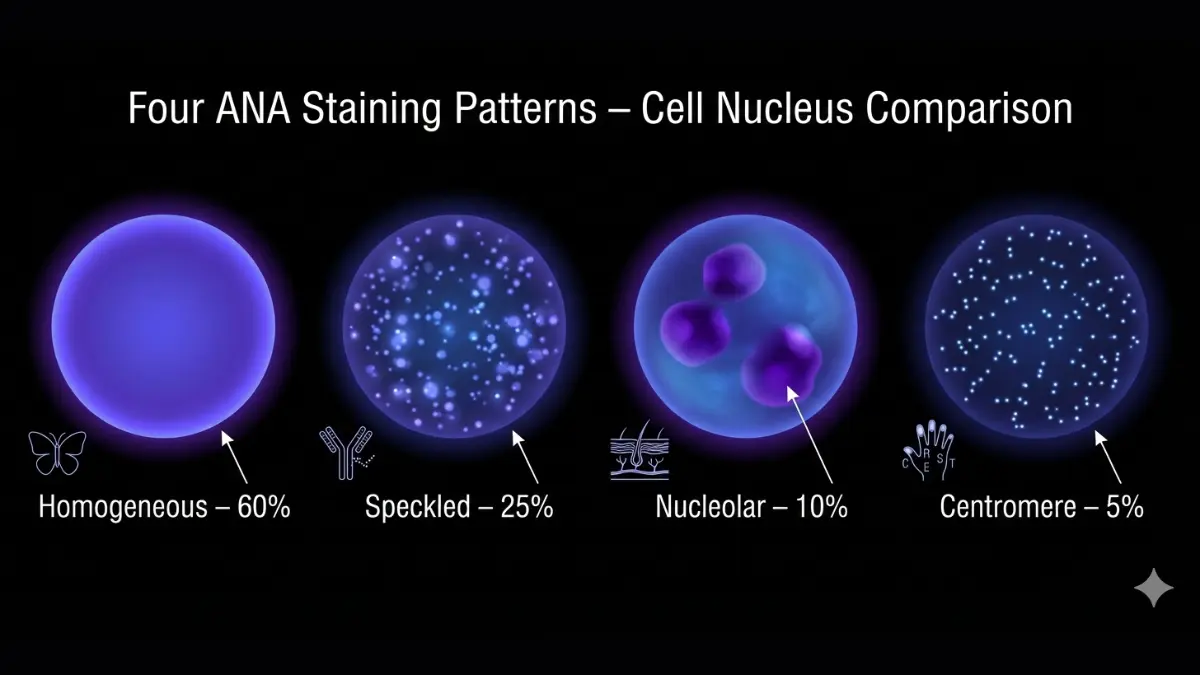
The Four Main ANA Patterns
1. Homogeneous Pattern (60% of positive tests)
This pattern shows uniform nuclear staining across the entire cell nucleus. It’s most commonly associated with systemic lupus erythematosus (SLE) and drug-induced lupus. According to Johns Hopkins Lupus Center research, 95% of lupus patients test positive for ANA, with homogeneous being the predominant pattern.
Monitor for: Joint pain, butterfly-shaped facial rashes, persistent fatigue, unexplained fever
2. Speckled Pattern (25% of positive tests)
Speckled patterns appear as dotted staining throughout the nucleus. This pattern associates with multiple conditions including mixed connective tissue disease, Sjögren’s syndrome, and scleroderma. The speckled pattern often indicates milder disease compared to homogeneous patterns.
Monitor for: Dry eyes and mouth, muscle weakness, skin thickening, difficulty swallowing
3. Nucleolar Pattern (10% of positive tests)
Nucleolar patterns show distinct dark spots in the nucleolus region. This highly specific pattern strongly suggests scleroderma (systemic sclerosis) or polymyositis. Research from the National Institute of Arthritis and Musculoskeletal and Skin Diseases indicates 85% of scleroderma patients display this pattern.
Monitor for: Raynaud’s phenomenon (fingers turning white in cold), skin tightening, chronic heartburn, shortness of breath
4. Centromere Pattern (5% of positive tests)
Centromere patterns display discrete speckles during cell division. This highly specific pattern indicates limited scleroderma (CREST syndrome) with 90% predictive value. Patients with this pattern rarely develop severe organ involvement.
Monitor for: Finger color changes, calcium deposits under skin, acid reflux, visible blood vessels on face
Pattern-Disease Association Matrix
| Pattern | Primary Associated Conditions | Diagnostic Specificity | Typical Titer Range |
|---|---|---|---|
| Homogeneous | Lupus (SLE), Drug-induced lupus | Moderate (60%) | 1:320-1:2560 |
| Speckled | Mixed CTD, Sjögren’s, Scleroderma | Low-Moderate (40%) | 1:160-1:640 |
| Nucleolar | Scleroderma, Polymyositis | High (75%) | 1:320-1:1280 |
| Centromere | Limited Scleroderma (CREST) | Very High (90%) | 1:160-1:640 |
Critical Insight: Patterns combined with specific secondary antibody tests (anti-dsDNA, anti-Smith, anti-Scl-70) provide far more diagnostic value than ANA titers alone. Your doctor will likely order these follow-up tests based on your pattern and clinical symptoms, similar to how specialists use comprehensive blood panels for diagnosis.
What Happens Next – Complete Action Protocol
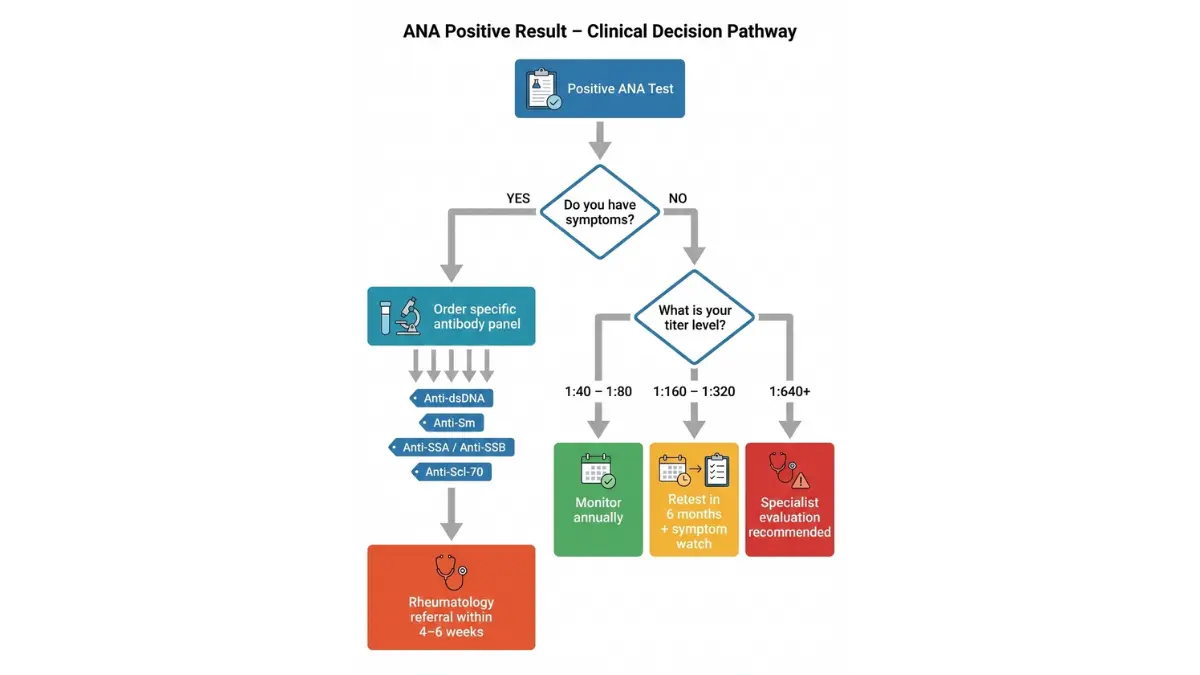
Your Positive ANA Result: Step-by-Step Next Actions
Receiving positive ANA test results triggers understandable anxiety, but knowing exactly what comes next transforms uncertainty into manageable action. Here’s your complete timeline protocol based on American College of Rheumatology 2026 guidelines.
Immediate Steps (First 2 Weeks)
Don’t Panic—Context is Everything
Between 20-30% of healthy Americans test positive for ANA without ever developing autoimmune disease. Your single lab value doesn’t define your health status. Take a deep breath and follow these steps:
Week 1 Action Items:
- ✓ Schedule follow-up with your primary care physician (within 7-10 days)
- ✓ Document any symptoms in a daily journal (joint pain, rashes, fatigue, fever)
- ✓ Avoid excessive Googling that amplifies anxiety
- ✓ Continue normal activities—positive ANA doesn’t require lifestyle changes yet
Week 2 Focus:
- ✓ Prepare symptom timeline for your doctor
- ✓ List all current medications (some cause false positives)
- ✓ Note any recent viral illnesses or infections
- ✓ Compile family history of autoimmune conditions
Follow-Up Tests Your Doctor May Order
Based on your ANA pattern, titer level, and symptoms, expect these common secondary tests:
For Lupus Investigation:
- Anti-dsDNA antibodies (95% specific for lupus)
- Anti-Smith (Sm) antibodies (99% specific but only in 30% of lupus patients)
- Complement levels (C3, C4—low levels indicate active disease)
For Sjögren’s Syndrome:
- Anti-SSA (Ro) and Anti-SSB (La) antibodies
- Schirmer test (measures tear production)
For Scleroderma:
- Anti-Scl-70 antibodies
- Anticentromere antibodies
- Pulmonary function tests
General Inflammation Markers:
- ESR (erythrocyte sedimentation rate) – covered in our ESR test results guide
- CRP (C-reactive protein) – detailed in our CRP levels analysis
- Complete blood count – explained in our CBC interpretation article
Symptom Tracking Checklist
Monitor these symptoms daily and rate intensity (0-10 scale):
- ☐ Joint pain, stiffness, or swelling (especially morning stiffness lasting >30 minutes)
- ☐ Skin rashes (particularly facial “butterfly” rash across cheeks)
- ☐ Persistent fatigue not relieved by rest
- ☐ Unexplained fever above 100.4°F
- ☐ Hair loss beyond normal shedding
- ☐ Dry eyes or dry mouth requiring frequent water
- ☐ Muscle weakness affecting daily activities
- ☐ Chest pain with deep breathing
- ☐ Fingers turning white/blue in cold (Raynaud’s phenomenon)
Managing Anxiety While Waiting
“What This Means For You” Insight:
Most positive ANA tests lead to monitoring, not treatment. Research from Stanford Medicine shows that among patients with isolated positive ANA (titer 1:80-1:160) and no symptoms, fewer than 8% develop autoimmune disease within five years.
Anxiety Reduction Strategies:
- Focus on controllable factors like sleep quality using a sleep calculator to optimize rest
- Maintain regular exercise and stress management
- Avoid catastrophizing—your titer number doesn’t predict your future health
- Connect with support groups only after diagnosis confirmation
Real Patient Story: Patricia’s Journey
Patricia, a 38-year-old teacher from Boston, tested positive at 1:320 with a homogeneous pattern during pregnancy screening. Her initial panic led to three sleepless nights researching lupus. Extensive testing revealed no anti-dsDNA, normal complement levels, and zero symptoms. Three years later, her titer decreased to 1:160, and she remains disease-free with annual monitoring. Her rheumatologist explained that pregnancy temporarily elevates many immune markers, which resolve postpartum—a common scenario documented by National Institutes of Health pregnancy immunology research.
Timeline for Diagnosis
Realistic Expectations:
- Initial follow-up tests: 2-4 weeks for results
- Rheumatology consultation: 4-8 weeks wait time (varies by region)
- Complete diagnostic workup: 2-6 months typically
- Monitoring period: 6-24 months for borderline cases
Patience during this process proves essential. Autoimmune conditions rarely emerge overnight, and careful, methodical evaluation prevents misdiagnosis.
False Positives & When Not To Worry
False Positive ANA Results: More Common Than You Think
Understanding false positive rates provides crucial perspective when interpreting your ANA test results. The term “false positive” means your test shows positive results without any underlying autoimmune disease present.
Leading Causes of False Positives
Statistical Reality (2026 CDC Data):
According to updated Centers for Disease Control autoimmune statistics, 25-30% of the general healthy population may test positive for ANA. Women test positive at rates 2-3 times higher than men (35% vs. 12%), even without disease.
1. Medications (15% of false positives)
Numerous common medications trigger positive ANA results:
- Blood pressure drugs: Hydralazine, methyldopa
- Antibiotics: Minocycline, isoniazid
- Heart medications: Procainamide, quinidine
- Biologics: Anti-TNF drugs (Humira, Enbrel, Remicade)
- Antifungals: Terbinafine
If you’re taking any of these, discuss alternatives with your doctor. Drug-induced lupus resolves within weeks to months after stopping the causative medication, unlike true systemic lupus.
2. Recent Infections
Viral and bacterial infections temporarily activate your immune system:
- Epstein-Barr virus (EBV) – detailed in our EBV symptoms guide
- Cytomegalovirus (CMV) – explained in our CMV test results article
- Hepatitis C – covered in our hepatitis B symptoms overview
- HIV (less common with modern treatment approaches)
These infection-related positive ANA tests typically resolve within 3-6 months post-recovery.
3. Other Medical Conditions
Several non-autoimmune conditions cause positive ANA:
- Thyroid disorders: Hashimoto’s thyroiditis, Graves’ disease (see thyroid function testing)
- Chronic liver disease: Cirrhosis, hepatitis
- Kidney disease: Chronic renal failure
- Cancer: Some malignancies trigger autoantibody production
When to Actually Worry
Red Flag Symptoms Requiring Urgent Attention:
Contact your doctor immediately if you experience:
- ⚠️ Persistent fever (>100.4°F) lasting more than 3 days with facial rash
- ⚠️ Multiple joint swelling affecting daily function
- ⚠️ Chest pain worsening with deep breathing (potential pericarditis)
- ⚠️ Seizures or severe neurological symptoms (confusion, severe headaches)
- ⚠️ Blood in urine with facial/leg swelling (kidney involvement)
- ⚠️ Significant unexplained weight loss (>10 pounds in one month)
These symptoms combined with positive ANA warrant emergency evaluation, as they may indicate active autoimmune disease requiring immediate treatment.
Green Light Scenarios (Likely Benign):
✓ Titer 1:40-1:80 with zero symptoms – Monitor annually, no treatment needed
✓ Single positive test, normal follow-ups – Retest in 6-12 months
✓ Positive during pregnancy – Often normalizes postpartum; track with pregnancy monitoring tools
✓ Positive with recent infection history – Recheck after 3-6 months recovery
✓ Family history of autoimmune disease but personally asymptomatic – Annual monitoring sufficient
The Importance of Clinical Context
Dr. Michelle Rodriguez, rheumatologist at Mayo Clinic, emphasizes: “ANA is one piece of a diagnostic puzzle, never a standalone answer. We need symptoms, physical findings, and confirmatory tests before diagnosing autoimmune disease.”
Real-World Example: David’s Experience
David, a 48-year-old accountant from Chicago, tested positive at 1:80 during a workplace health screening. With no symptoms and excellent overall health maintained through balanced nutrition calculated via his macro calculator routine, his doctor recommended watchful waiting. Five annual retests remained stable at 1:80, and David never developed disease. His case exemplifies the most common trajectory for low-titer positive ANA—benign monitoring without intervention.
Ana Results By Specific Conditions
ANA Results in Common Autoimmune Diseases
Understanding how ANA test results correlate with specific autoimmune conditions helps set realistic expectations about your diagnosis journey. Remember that positive ANA supports but never confirms a diagnosis alone.
Disease-Specific ANA Patterns and Titers
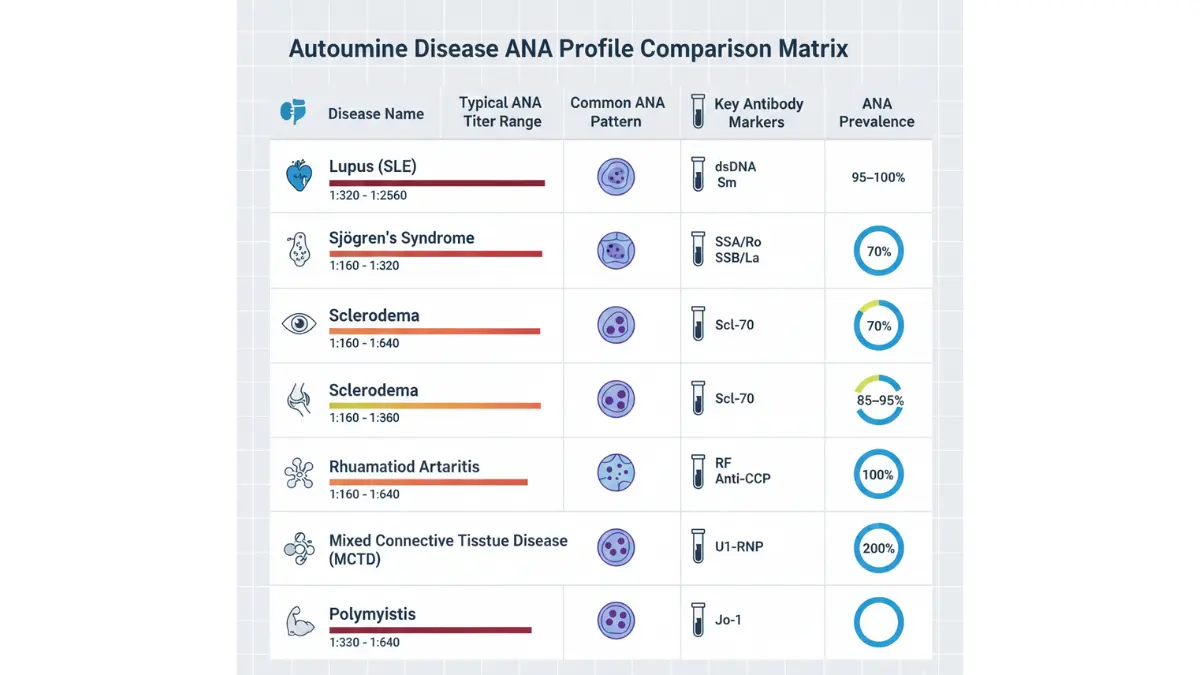
| Condition | Typical Titer | Common Pattern | Key Additional Markers | ANA Prevalence |
|---|---|---|---|---|
| Lupus (SLE) | 1:320-1:2560 | Homogeneous, Rim | Anti-dsDNA, Anti-Sm, Low C3/C4 | 95-100% positive |
| Sjögren’s Syndrome | 1:160-1:320 | Speckled | Anti-SSA/Ro, Anti-SSB/La | 70% positive |
| Scleroderma | 1:160-1:640 | Nucleolar, Centromere | Anti-Scl-70, Anticentromere | 85-95% positive |
| Rheumatoid Arthritis | 1:40-1:160 | Variable (often negative) | RF, Anti-CCP (more specific) | 20-30% positive |
| Mixed Connective Tissue Disease | 1:160-1:2560 | Speckled | Anti-U1-RNP (required for diagnosis) | 100% positive |
| Polymyositis/Dermatomyositis | 1:160-1:640 | Nucleolar, Speckled | Anti-Jo-1, Elevated muscle enzymes | 60-80% positive |
Critical Diagnostic Insight:
ANA serves as an excellent screening tool but lacks specificity. A patient with rheumatoid arthritis (covered extensively in our rheumatoid factor levels guide) might test ANA-negative yet have active disease confirmed by anti-CCP antibodies and joint imaging.
2026 Diagnostic Criteria Updates
The American College of Rheumatology and European Alliance of Associations for Rheumatology updated classification criteria in January 2026 with significant changes:
Key Updates:
- Lupus classification: Now requires positive ANA (1:80 minimum) as entry criterion, plus weighted scoring of clinical/immunologic criteria
- Sjögren’s syndrome: Emphasis shifted to anti-SSA/Ro antibodies and objective dry eye/mouth measures over ANA alone
- Mixed connective tissue disease: Anti-U1-RNP now mandatory alongside ANA for classification
What This Means for Patients:
Modern diagnosis relies heavily on clinical symptoms plus multiple antibody tests, not just ANA. Your rheumatologist constructs diagnosis like assembling puzzle pieces—ANA represents just one piece among many including detailed examination findings, imaging studies, and specific autoantibody profiles.
The Role of Anti-dsDNA in Lupus Diagnosis
For patients with positive ANA and suspected lupus, anti-dsDNA antibodies provide crucial confirmation. According to National Institute of Arthritis research, anti-dsDNA shows:
- Specificity: 95-98% for lupus (rarely positive in other conditions)
- Sensitivity: 70% (30% of lupus patients test negative)
- Disease activity correlation: Rising titers often predict disease flares
Our comprehensive anti-dsDNA test results guide explores this connection in depth.
Real Patient Scenario: Angela’s Diagnostic Journey
Angela, a 31-year-old nurse from Phoenix, presented with joint pain, facial rash, and fatigue. Her initial labs showed ANA 1:640 (homogeneous pattern). Follow-up revealed strongly positive anti-dsDNA (220 IU/mL), low complement C3 (65 mg/dL), and protein in urine. Combined with her clinical symptoms, these findings confirmed systemic lupus erythematosus diagnosis. She started hydroxychloroquine treatment and now manages her condition successfully with regular monitoring including comprehensive metabolic panels to check medication effects.
When ANA Stays Positive Without Disease
Some patients maintain persistently positive ANA for decades without ever developing autoimmune conditions. This phenomenon, called “benign ANA positivity,” occurs most commonly in:
- Elderly populations (especially women over 65)
- First-degree relatives of autoimmune disease patients
- Individuals with chronic low-grade inflammation
These patients require annual monitoring but typically never need treatment. The key differentiator: absence of clinical symptoms despite positive laboratory values.
Monitoring Protocol for Benign ANA Positivity:
- Annual ANA titer recheck
- Yearly clinical examination by primary care physician
- Symptom awareness education
- No immunosuppressive medications unless disease develops
Important Note: Anyone with positive ANA should maintain optimal overall health through balanced nutrition (calculate your needs with our calorie deficit calculator), regular exercise monitored via heart rate zone tracking, and adequate sleep for immune system support.
Quick Answers – Ana Test Results FAQs
Q1: Can stress cause a positive ANA test?
No, stress itself doesn’t cause positive ANA results. However, chronic stress may worsen symptoms in people with established autoimmune disease. Stress management remains important for overall health, but it won’t change your ANA status.
Q2: Should I retest if my ANA is positive once?
Yes, single positive tests often require confirmation in 3-6 months, especially if you’re asymptomatic. ANA can fluctuate, and repeat testing provides better diagnostic accuracy.
Q3: Can ANA go from positive to negative?
Yes, particularly with low titers (1:40-1:80). Temporary elevations from infections or medications often resolve. However, high titers (1:320+) with autoimmune disease rarely become negative without treatment.
Q4: Is 1:40 considered clinically significant?
Borderline. Many laboratories now use 1:80 as the threshold for clinical significance. Isolated 1:40 results without symptoms typically don’t warrant extensive workup.
Q5: Do I need to see a rheumatologist immediately?
Not always. With low titers (1:40-1:80) and no symptoms, your primary care doctor may monitor initially. High titers (1:320+) or any titer with concerning symptoms should prompt rheumatology referral within 4-6 weeks.
Q6: Can pregnancy cause positive ANA?
Yes, pregnancy temporarily elevates many immune markers including ANA. These often normalize within 6-12 months postpartum. Pregnant women should discuss results with their obstetrician.
Q7: Does positive ANA mean I’ll definitely develop disease?
Absolutely not. Studies show 70-85% of people with isolated positive ANA (especially titers under 1:160) never develop autoimmune disease during decades of follow-up.
Q8: How often should I retest my ANA?
For asymptomatic low positives: every 6-12 months initially, then annually if stable. For diagnosed autoimmune disease: every 3-6 months or as your rheumatologist recommends based on disease activity.
Q9: Can diet or supplements affect ANA results?
No direct evidence shows dietary changes alter ANA status. However, anti-inflammatory diets may help manage symptoms in diagnosed autoimmune conditions. Focus on overall wellness tracked through tools like our water intake calculator.
Q10: Are there medications specifically to lower ANA titers?
No medications target ANA reduction directly. Treatment addresses underlying autoimmune disease if present, which may secondarily affect titers. Never start immunosuppressive drugs based solely on positive ANA without confirmed disease.
Q11: Can children have positive ANA tests?
Yes, though less common (5-10% of healthy children). Pediatric positive ANA requires careful evaluation by pediatric rheumatology specialists, as childhood autoimmune diseases present differently than adult forms.
Medical Disclaimer
This article provides educational information about ANA test results and should not replace professional medical advice. Always consult your physician or qualified healthcare provider for interpretation of your specific laboratory results and personalized medical recommendations. Never delay seeking medical attention due to information read on this website.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.