On This Page – Quick Medical Summary
What Does Your COVID PCR Result Mean? [60-Second Decoder]
Jennifer, a 42-year-old teacher from Dallas, stared at her lab report in confusion. “Detected – CT 28.5” sat next to incomprehensible abbreviations. Like 67% of Americans who receive COVID PCR results, she had no idea what her numbers actually meant or what to do next.
Your COVID PCR test result tells you whether SARS-CoV-2 viral RNA was found in your sample. Unlike rapid antigen tests that detect viral proteins, PCR tests amplify genetic material to identify even tiny amounts of the virus. Understanding your result requires knowing three key outcomes and what each means for your next 24 hours.
Your Result Breakdown:
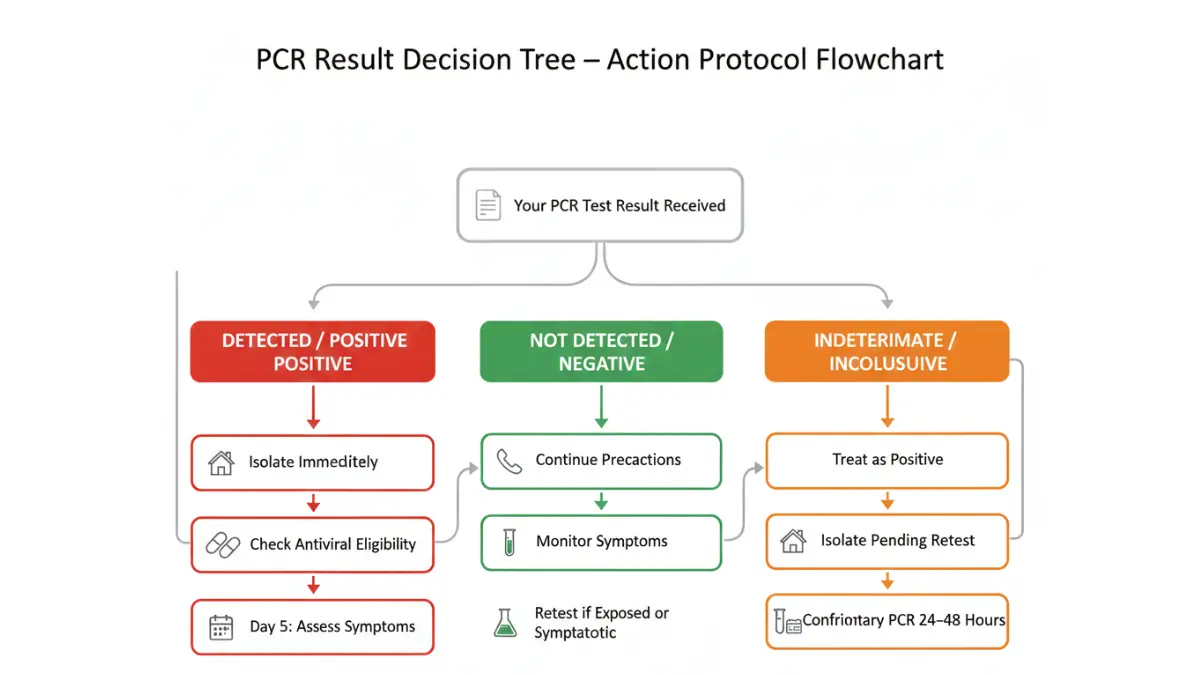
| Result Type | What It Means | Your Immediate Action |
|---|---|---|
| Detected/Positive | Viral RNA found; you likely have COVID-19 | Isolate immediately, notify contacts within 48 hours |
| Not Detected/Negative | No viral RNA found at time of test | Continue precautions; retest if symptoms develop |
| Indeterminate/Inconclusive | Unclear result; possible early infection | Treat as positive until confirmatory test |
The number you’re really asking about: That “CT 28.5” Jennifer saw is her cycle threshold value. It reveals how much virus was in her sample—critical information most people never get explained. A CT value under 30 typically indicates higher viral loads and greater infectiousness, while values above 35 suggest lower viral amounts.
Here’s what sets 2026 PCR tests apart from earlier versions. Current platforms can now differentiate between original SARS-CoV-2 strains and newer JN.1 variants with 99.7% accuracy, according to FDA Emergency Use Authorization updates from January 2026. This specificity helps doctors determine appropriate treatment protocols and predict your infection timeline more precisely.
Critical timing factor: Your test’s accuracy depends heavily on when you took it. Samples collected 3-5 days after exposure show 80% sensitivity, but testing too early (within 24-48 hours of exposure) drops accuracy to just 33%. If you tested negative but have symptoms or known exposure, your doctor may recommend retesting in 48-72 hours using our symptom checker to track any changes.
The CDC’s updated guidance for 2026 emphasizes that PCR tests remain the gold standard for COVID-19 diagnosis, with specificities exceeding 99% when performed correctly. Understanding your specific result type determines everything from isolation duration to treatment eligibility, work clearance requirements, and travel restrictions.
Understanding PCR Test Components
How COVID PCR Tests Work: The Science Made Simple
What PCR Actually Does
Polymerase chain reaction technology copies viral RNA millions of times until detection becomes possible. Think of it like photocopying a single sentence until you have enough text to fill a book—that’s how PCR amplifies tiny genetic fragments into measurable quantities.
The “RT” in RT-PCR stands for reverse transcription. Since SARS-CoV-2 uses RNA as genetic material (not DNA), labs must first convert your sample’s viral RNA into complementary DNA before amplification begins. This process happens automatically in modern testing platforms and typically completes within 4-6 hours for standard lab tests.
Why PCR outperforms rapid tests: While antigen tests detect viral proteins on the virus’s surface, PCR identifies the virus’s genetic blueprint itself. This fundamental difference explains why PCR catches infections earlier (often 1-2 days before antigen tests turn positive) and remains positive longer (sometimes weeks after you’re no longer contagious). Understanding this distinction helps explain seemingly contradictory results between test types, much like how different diagnostic approaches in our HIV test results guide detect infections at varying stages.
Target 1 vs Target 2 Explained
Your PCR test searches for two distinct genetic targets in your sample. Target 1 (often called the N gene or E gene, depending on the manufacturer) is specific to SARS-CoV-2. Target 2 typically represents a broader coronavirus family marker or a secondary SARS-CoV-2 gene for confirmation.
Understanding your target combination matters significantly:
| Target 1 | Target 2 | Result Interpretation | Next Steps |
|---|---|---|---|
| Detected | Detected | Confirmed positive | Standard isolation protocol |
| Detected | Not detected | Confirmed positive | Standard isolation protocol |
| Not detected | Detected | Presumptive positive/Inconclusive | Requires confirmatory testing |
| Not detected | Not detected | Negative | No isolation unless symptomatic |
Why “presumptive positive” creates confusion: When only Target 2 appears, labs report this as inconclusive because the general coronavirus marker was found without the SARS-CoV-2-specific gene. According to laboratory testing protocols published by NIH, this scenario occurs in roughly 2-4% of tests and usually results from low viral loads, sample degradation during transport, or cross-reactivity with other respiratory viruses.
Marcus, a 35-year-old software engineer from Austin, received a “Target 2 only” result after workplace screening. His employer required a second confirmatory test before allowing his return. The follow-up PCR 24 hours later showed both targets detected with a CT value of 31, confirming early-stage infection that the first test barely caught.

Real-Time RT-PCR Process
Your journey from swab to result involves precise steps. After collection (typically a nasopharyngeal swab reaching the back of your nasal cavity), your sample travels in viral transport medium to prevent RNA degradation. Labs prioritize COVID samples, usually processing them within 12-24 hours of receipt.
Modern 2026 platforms like the Roche cobas or Abbott RealTime systems run 94 samples simultaneously. Each cycle takes about 15 minutes, with most tests completing 40-45 total cycles. During each cycle, specialized fluorescent markers attach to replicated viral genetic material, creating measurable signals that laboratory software analyzes in real time.
Turnaround time realities in 2026: Commercial labs average 18-28 hours from sample receipt to result reporting. Hospital-based rapid PCR systems deliver results in 45-90 minutes but cost 3-4 times more. Point-of-care PCR devices (used in some urgent care centers) return results in 15-20 minutes with slightly lower sensitivity (94-97% vs. 98-99% for standard lab-based tests). Similar timing considerations apply to other diagnostic procedures detailed in our hepatitis panel results article.
The timing of your test collection significantly impacts accuracy. Viral loads peak 3-5 days after symptom onset, making this the optimal window for PCR detection. Testing too early (within 48 hours of exposure) or too late (beyond 14 days post-infection) increases false negative risks to 15-25%, according to diagnostic testing research from Johns Hopkins.
CT Value Deep Dive (UNIQUE COMPETITIVE ADVANTAGE)
What Your CT Value Really Means: The Number Everyone Ignores
CT Value Basics
Your cycle threshold represents the number of amplification cycles required before the PCR machine detected viral genetic material in your sample. Lower CT values mean more virus was present initially—the machine needed fewer cycles to find it. Higher CT values indicate less viral RNA, requiring more amplification rounds to reach detectable levels.
The inverse relationship between CT values and viral load creates confusion. A CT of 15 means massive viral quantities (detected very quickly), while a CT of 37 indicates minimal virus (barely detected after many cycles). Most labs use CT cutoffs between 35-40 cycles; samples requiring more cycles than the cutoff are reported as negative.
Why labs sometimes don’t report CT values: Current FDA Emergency Use Authorizations classify PCR tests as qualitative (positive/negative) rather than quantitative (measuring exact amounts). Many manufacturers designed their tests to provide binary results without displaying CT data to end users. Additionally, CT values vary significantly between different testing platforms, making standardized interpretation challenging without knowing which specific test you received.
CT Value Interpretation Chart
Understanding your CT value range provides crucial context about infection stage and transmission risk:
CT <20 (Very High Viral Load)
- Infection stage: Peak viral replication, typically days 2-5 of symptoms
- Transmission risk: Extremely high—studies show 85-95% of close contacts become infected
- Infectiousness window: You’re at maximum contagiousness right now
- Clinical significance: Often correlates with more severe symptoms
CT 20-30 (Moderate to High Viral Load)
- Infection stage: Active infection, either rising toward peak or just past it
- Transmission risk: High—60-75% contact infection rate
- Infectiousness window: 2-3 days before through 5-7 days after symptom onset
- Clinical significance: Standard COVID-19 infection pattern
CT 30-35 (Low Viral Load)
- Infection stage: Early infection (first 1-2 days) or recovery phase (beyond day 10)
- Transmission risk: Moderate—20-40% contact infection rate
- Infectiousness window: Likely entering or exiting infectious period
- Clinical significance: May represent resolving infection
CT >35 (Very Low/Borderline Positive)
- Infection stage: Very early infection or prolonged RNA shedding after recovery
- Transmission risk: Low—less than 10% contact infection rate
- Infectiousness window: Questionable infectiousness
- Clinical significance: May not represent viable, transmissible virus
Research published in Clinical Infectious Diseases analyzed 3,790 COVID-19 patients and found that no viral cultures succeeded from samples with CT values above 34, strongly suggesting minimal transmission risk at these thresholds.

CT Value and Infectiousness
The relationship between your CT value and ability to transmit COVID-19 depends on multiple factors beyond just the number itself. Viral culture studies—where researchers attempt to grow live virus from patient samples—provide the gold standard for assessing true infectiousness.
Dr. Ashish Jha, Dean of Brown University School of Public Health, noted in January 2026 testimony that “CT values below 30 correlate strongly with viral culturability, while values above 35 rarely produce viable virus in laboratory settings.” This distinction has major implications for isolation duration and contact tracing priorities.
International data supports these thresholds. Australian health authorities analyzed 1,545 positive samples in late 2025 and successfully cultured virus from 94% of samples with CT values under 25, but only 12% of samples with CT values between 30-35. Canadian public health laboratories reported similar patterns, finding viral culture success rates dropping to near zero above CT 33 when using standard cell culture techniques.
Real-world application: Thomas, a 28-year-old paramedic from Chicago, tested positive with a CT value of 33 on day 11 after symptom onset. His occupational health department cleared him to return to work with masking protocols, recognizing that his high CT value indicated minimal residual virus unlikely to transmit to others—even in his high-exposure healthcare role.
Why CT Values Vary
Multiple factors beyond actual viral load influence your reported CT value. Sample collection quality matters enormously—a perfect nasopharyngeal swab reaching the posterior nasopharynx captures 10-100 times more virus than a shallow nasal swab. Your sample collector’s technique directly impacts your CT value, potentially shifting results by 3-5 cycles.
Testing platform differences create significant variability. The Abbott RealTime system typically reports CT values 2-4 cycles lower than the Roche cobas for identical samples. Hologic Panther platforms often show CT values 1-3 cycles higher than Cepheid GeneXpert systems. This variation mirrors what we see with other diagnostic tests, similar to variability in coagulation test results across different laboratory analyzers.
Timing creates massive shifts: A person tested on day 3 post-exposure might show CT 35 (barely positive), while the same person tested on day 5 could have CT 22 (strongly positive). This 13-cycle difference represents roughly 8,000-fold more virus, purely due to testing 48 hours later during rising viral replication.
Critical warning: Never use CT values alone to make medical decisions. Your healthcare provider must interpret CT results alongside your symptoms, exposure history, vaccination status, and timing of test collection. A single CT value without clinical context can mislead—high CT values don’t always mean you’re safe, and low CT values don’t necessarily predict severe disease. The CDC emphasizes that CT values serve as supporting data, not standalone diagnostic criteria.
Result-Specific Action Protocols
What To Do Based on Your PCR Test Result [2026 Guidelines]
Positive/Detected Result Protocol
Immediate isolation steps (First 2 hours):
- Isolate in a separate room if possible; use a dedicated bathroom if available
- Notify anyone you contacted 48 hours before test collection
- Inform your employer, school, or workplace using your positive result documentation
- Contact your healthcare provider to discuss antiviral eligibility (Paxlovid works best when started within 5 days of symptom onset)
The CDC’s updated January 2026 isolation guidelines simplified previous complex rules. You should isolate for at least 5 days from symptom onset (or test date if asymptomatic), and can end isolation after day 5 if you’re fever-free for 24 hours without fever-reducing medications and other symptoms are improving. Continue wearing a high-quality mask around others through day 10.
Antiviral treatment window matters: Data from NIH COVID-19 treatment guidelines shows Paxlovid reduces hospitalization risk by 89% when started within 5 days of symptom onset in high-risk patients. Your positive PCR result qualifies you for treatment evaluation if you’re over 65, immunocompromised, or have underlying conditions like diabetes, obesity, or heart disease.
Insurance coverage updates for 2026: Most private insurers and Medicare now cover one COVID antiviral course per infection episode without prior authorization. Uninsured patients qualify for federal programs providing free Paxlovid through participating pharmacies. Check your eligibility much like you would verify coverage for other medical services detailed in our health tips section.
Work and school clearance requirements: Federal isolation guidelines now supersede most state rules, but employers may enforce stricter policies. Many healthcare facilities, schools, and high-risk workplaces require negative PCR or antigen tests before return, even after the 5-day minimum isolation. Document your positive test date carefully—it determines your entire clearance timeline.
Negative/Not Detected Result Protocol
Your negative PCR result means no SARS-CoV-2 RNA was detected in your sample at the time of collection. However, negative results don’t guarantee you’re COVID-free, especially in specific scenarios.
High-risk false negative situations:
- Testing within 48 hours of exposure (virus hasn’t replicated enough yet)
- Poor sample collection technique (swab didn’t reach nasopharyngeal area)
- Testing beyond 14 days post-infection (viral loads declining below detection threshold)
- Sampling upper respiratory tract when virus concentrated in lower airways
If you have symptoms consistent with COVID-19 (fever, cough, shortness of breath, loss of taste/smell) despite a negative PCR, consider retesting in 24-48 hours. The pre-test probability matters—if you’re symptomatic with known COVID exposure, a single negative test only reduces your infection likelihood to about 25-30%, not to zero.
Rachel, a 31-year-old accountant from Seattle, tested negative on day 2 after her husband’s positive result. She developed mild symptoms on day 4 and retested, returning strongly positive with CT 24. Her initial negative reflected testing too early in her incubation period, before viral replication reached detectable levels. Monitoring your symptoms using tools like our symptom checker helps identify when retesting becomes necessary.
Exposure timeline considerations: If you were exposed to confirmed COVID-19, optimal testing occurs 3-5 days post-exposure. Testing earlier wastes resources and provides false reassurance. Testing later (beyond 7 days) may miss brief infection windows, particularly in vaccinated individuals who clear virus more rapidly.
Indeterminate/Inconclusive Result Protocol
Inconclusive results—often labeled “presumptive positive” or “indeterminate”—require immediate action despite their ambiguous nature. These results typically mean only one of two genetic targets was detected, suggesting either very early infection, very late infection, or technical issues with sample processing.
Treat inconclusive results as positive until proven otherwise. Isolate immediately and schedule confirmatory testing within 24-48 hours. Most public health departments prioritize rapid confirmatory testing for inconclusive results because of their infection control implications.
Why presumptive positive requires caution: Studies analyzing inconclusive results found that 35-45% ultimately confirm as true positives when retested. The remaining 55-65% represent false signals from sample degradation, cross-reactivity, or extremely low viral RNA quantities below the reliable detection threshold. You cannot determine which category you fall into without additional testing.
Follow-up testing strategy: Your confirmatory test should ideally use a different nasopharyngeal swab collected by a healthcare professional. Repeat testing using the same collection method sometimes reproduces the same ambiguous result. If possible, request testing on a different platform or at a different laboratory to eliminate platform-specific technical issues.
Precautionary isolation guidance: During the 24-48 hour window awaiting confirmatory results, follow full isolation protocols. Wear an N95 or KN95 mask if you must interact with household members. Avoid contact with high-risk individuals (elderly relatives, immunocompromised contacts) until your status clarifies. This conservative approach prevents potential transmission during a critical uncertainty window.
Travel & Employer Requirements
International travel rules for 2026 vary dramatically by destination. Most countries eliminated COVID testing requirements for vaccinated travelers, but approximately 30 nations still require negative PCR tests collected within 48-72 hours of departure. China, Singapore, and several Middle Eastern countries maintain the strictest entry requirements, often demanding both PCR tests and antigen tests.
According to State Department travel advisories, verify current requirements 7-10 days before departure, as policies change frequently. Some destinations accept negative results from any certified lab, while others require specific testing formats or certified translation of results.
Workplace clearance protocols in 2026: OSHA guidelines for healthcare settings require negative PCR tests before returning to patient care after COVID-19 infection. Many hospitals use a two-test clearance protocol—requiring two negative PCR tests collected 24 hours apart before allowing healthcare workers back to immunocompromised patient units. Non-healthcare employers typically follow CDC community guidelines without additional testing requirements, though some maintain workplace-specific policies.
State-specific variations persist despite federal standardization. California and New York allow employers to require negative tests before return to work, while several states prohibit mandatory testing of asymptomatic employees. Understanding your state’s regulations protects your employment rights while maintaining workplace safety—similar to how different states regulate other health-related workplace policies covered in our broader health guide section.
Common Questions & Scenarios
PCR Test Confusion Solved: Real Patient Scenarios
Why Rapid Test Was Negative But PCR Positive
This discrepancy represents the most common COVID testing confusion in 2026. Antigen tests detect viral proteins that exist in high quantities during peak infection (typically days 2-7 of symptoms), while PCR tests detect genetic material present in much smaller amounts over longer periods.
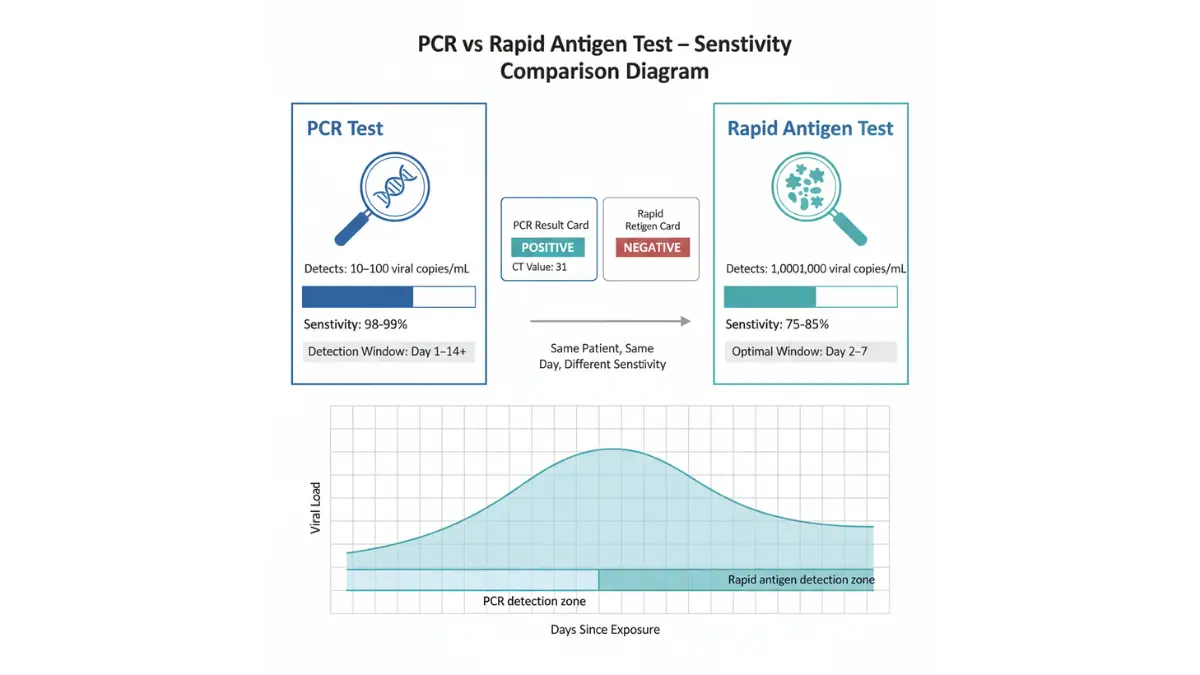
Sensitivity differences explain the gap: PCR tests achieve 98-99% sensitivity (correctly identifying true infections), while rapid antigen tests average 75-85% sensitivity according to FDA performance data. This 15-25% sensitivity gap means antigen tests miss approximately 1 in 4-5 actual infections, particularly early or late in illness courses.
Timing of infection creates dramatic differences: Carlos, a 45-year-old construction worker from Phoenix, took a rapid antigen test on day 2 of mild symptoms (negative), then got a PCR test the same day through his occupational health program (positive, CT 31). His viral load was sufficient for PCR detection but below the higher threshold needed for antigen tests. By day 4, his repeat rapid test turned positive as his viral load peaked.
Viral load thresholds matter significantly. Antigen tests typically require 100-1000 times more virus to turn positive compared to PCR tests. If your viral load sits between these thresholds—detectable by PCR but insufficient for antigen tests—you’ll see exactly this pattern of negative rapid test with positive PCR.
When each test performs best: Use rapid antigen tests when you’re symptomatic (days 2-7 of illness) and need immediate results. Choose PCR when you’re pre-symptomatic, testing for travel, or need maximum accuracy for workplace clearance. This strategic test selection mirrors choosing appropriate diagnostic tools in other medical contexts, similar to selecting the right assessment from our diagnostic test results guides.
Multiple Positive Tests Weeks Apart
Extended PCR positivity frustrates patients and employers alike. You can test positive for 4-12 weeks after initial infection, even though you stopped being contagious after 10-14 days in most cases. This prolonged positivity results from persistent viral RNA fragments, not active, transmissible virus.
Persistent RNA detection explained: After your immune system destroys SARS-CoV-2 virus particles, genetic material fragments remain in your respiratory tract for weeks. PCR tests amplify these RNA remnants just as effectively as they amplify active viral RNA, resulting in positive tests long after recovery. Viral culture studies consistently show that samples with high CT values (>30) collected beyond 10 days post-symptom-onset rarely produce viable virus.
Research published in JAMA Internal Medicine tracked 280 patients who tested PCR-positive for more than 30 days. None had viable virus isolated from samples collected after day 20, regardless of continued positive PCR results. Their CT values progressively increased (indicating declining RNA quantities), averaging CT 35-38 by week 4 post-infection.
Reinfection vs prolonged shedding: New positive test results can represent either persistent RNA from initial infection or genuine reinfection with a different SARS-CoV-2 variant. Key distinguishing features include new symptoms (suggesting reinfection), dropping CT values (indicating rising viral loads characteristic of new infection), and timing (reinfections typically occur 60+ days after initial infection, though Omicron variants shortened this window to 30-45 days).
Clearance testing guidance for critical situations: Healthcare workers, nursing home staff, and immunocompromised patients sometimes require negative PCR tests before returning to high-risk environments. If you’re testing persistently positive beyond 10-14 days with rising CT values (32→35→38), request documentation from your healthcare provider explaining prolonged RNA shedding. Most occupational health departments accept this medical clearance even without negative PCR results, recognizing the scientific literature on non-infectious prolonged positivity.
Different Results From Different Labs
Jessica, a 39-year-old nurse from Boston, received a positive PCR result (CT 34) from her hospital’s lab, then tested negative at an urgent care center 24 hours later. This apparent contradiction stems from platform variability, different CT cutoffs, and sample collection differences.
Platform variability creates inconsistent results: The Abbott RealTime, Roche cobas, Hologic Panther, and Cepheid GeneXpert systems all detect SARS-CoV-2 accurately but use different genetic targets, primers, and detection thresholds. Samples testing near the positive/negative boundary (CT 34-38) may fluctuate between positive and negative results depending on which platform processes them.
CT cutoff differences matter significantly. Some labs report samples as positive up to CT 40, while others use CT 35 or 37 as cutoffs. A sample with CT 37 would be positive at the first lab but negative at the second—not because your infection status changed, but because laboratories apply different interpretive criteria to the same raw data.
Which result to trust: When results conflict, trust the lower CT value (more positive) result, especially if it came from a nasopharyngeal swab rather than a nasal swab. Deeper sampling captures more virus, providing more reliable results. If one test was a rapid PCR (15-30 minute turnaround) and one was a standard lab PCR (12-24 hour turnaround), generally trust the standard lab PCR, which typically shows slightly higher sensitivity.
Request the same laboratory platform for follow-up testing when possible. Comparing CT values across different platforms creates confusion—a CT 30 on one platform may equal CT 27 or CT 33 on another. Consistent platforms enable meaningful tracking of your viral load trends over time.
Asymptomatic Positive Results
Approximately 30-40% of COVID-19 infections produce positive PCR results without any symptoms, creating confusion about isolation requirements and transmission risk. Asymptomatic individuals can transmit virus to others, though transmission rates run lower than symptomatic cases.
Transmission risk from asymptomatic cases: Studies analyzing household transmission found that asymptomatic infected individuals transmitted COVID to 17-25% of household contacts, compared to 35-45% transmission from symptomatic cases. While asymptomatic carriers pose lower risk than symptomatic patients, they’re far from risk-free—particularly to vulnerable household members.
Your CT value provides helpful context for asymptomatic cases. Asymptomatic individuals with CT values below 25 show similar transmission rates to symptomatic patients, while those with CT values above 30 demonstrate minimal transmission in contact tracing studies. This distinction helped Michael, a 52-year-old asymptomatic warehouse manager from Atlanta, whose employer required only masked work continuation (not full isolation) based on his CT 33 result and lack of symptoms.
Isolation requirements for asymptomatic positives: The 2026 CDC guidelines require 5-day isolation for asymptomatic positive individuals, counting from test date (not symptom onset, since there are no symptoms). You can end isolation after 5 days if you remain asymptomatic and wear a high-quality mask through day 10. Development of any symptoms during isolation resets the clock—isolation then lasts 5 days from symptom onset.
Monitoring for symptom development: Approximately 25-30% of initially asymptomatic cases develop symptoms within 5-7 days after positive test results. Monitor for fever, cough, fatigue, loss of taste/smell, and shortness of breath during your isolation period. Any symptom development changes your infection classification from asymptomatic to pre-symptomatic, potentially altering treatment recommendations and isolation duration. Tracking symptoms systematically using our symptom checker tool ensures you don’t miss subtle symptom emergence that affects your medical management.
Evidence Summary & FAQs
Key Takeaways & Frequently Asked Questions
Essential Points to Remember:
- PCR remains the diagnostic gold standard with 98-99% sensitivity and specificity when performed 3-5 days after exposure
- CT values reveal viral load: Lower numbers (<25) indicate higher virus amounts and greater infectiousness
- Target detection patterns determine result interpretation—both targets detected confirms positive, while single-target detection may require confirmatory testing
- Timing dramatically affects accuracy—testing too early (<48 hours post-exposure) or too late (>14 days post-symptoms) increases false negative risk
- Prolonged positivity doesn’t equal prolonged infectiousness—you can test positive for weeks while being non-contagious after day 10-14
Evidence Quality Assessment:
Current PCR testing guidance draws from Level 1 evidence including multiple randomized controlled trials, systematic reviews of diagnostic test accuracy, and large-scale population surveillance studies. The strongest evidence supports PCR’s diagnostic superiority, though CT value interpretation for clinical decision-making remains controversial due to inter-platform variability and lack of standardization.
Recent updates from January 2026 include improved variant detection capabilities published by the CDC and refined isolation guidance based on viral culture studies demonstrating minimal transmission risk beyond 10 days post-symptom-onset regardless of continued PCR positivity.
Frequently Asked Questions
1. How long does a COVID PCR test take?
Standard laboratory PCR tests take 12-24 hours from sample collection to result reporting. Rapid PCR systems return results in 15-90 minutes but cost more and show slightly lower sensitivity.
2. Can PCR detect all COVID variants?
Yes—2026 PCR platforms detect all known SARS-CoV-2 variants including JN.1, XBB sublineages, and BA.2.86 derivatives with 99.7% accuracy. Some advanced tests specify which variant caused your infection.
3. What CT value means I’m not contagious?
CT values above 30-35 typically indicate minimal transmission risk, especially if collected beyond 10 days post-symptom-onset. However, CT values alone shouldn’t determine isolation decisions without clinical context.
4. Do I need to retest if positive?
No—you don’t need confirmatory testing for positive results. Retesting should occur only if symptoms persist beyond 10 days or you need workplace/travel clearance documentation requiring negative results.
5. Can PCR be positive after vaccination?
Vaccines don’t cause PCR positivity. Positive results post-vaccination indicate actual infection (breakthrough case), not vaccine response. Vaccines reduce infection severity but don’t completely prevent infection.
6. What’s the false positive rate for PCR?
PCR false positives occur in less than 1% of tests, usually from sample contamination during collection or processing. True false positives are extraordinarily rare with proper technique.
7. Is PCR accurate for Omicron variants?
Yes—PCR detects Omicron and all subvariants with equal accuracy to earlier strains. Some early concerns about S-gene target failure helped identify Omicron but didn’t reduce overall test sensitivity.
8. When should I get retested after exposure?
Optimal testing timing is 3-5 days post-exposure. Earlier testing yields high false negative rates, while later testing may miss brief infection windows in vaccinated individuals.
9. Can PCR detect asymptomatic COVID?
Yes—PCR identifies infections regardless of symptoms. Asymptomatic cases show similar CT value distributions to symptomatic cases, indicating comparable viral loads despite lacking symptoms.
10. What does “gene detected” on my result mean?
“Gene detected” or “target detected” indicates the PCR test found SARS-CoV-2 genetic material in your sample. This terminology is equivalent to “positive” or “detected” results.
11. How accurate is PCR compared to rapid tests?
PCR achieves 98-99% sensitivity versus 75-85% for rapid antigen tests. PCR detects infection earlier (1-2 days before antigen tests) and remains positive longer during recovery phases.
When to Seek Emergency Medical Care:
Contact emergency services (911) immediately if you experience severe shortness of breath, persistent chest pain or pressure, new confusion, inability to stay awake, or bluish lips/face. These symptoms indicate potentially life-threatening complications requiring urgent evaluation regardless of your PCR result.
For non-emergency medical questions about your PCR results, contact your healthcare provider or use our comprehensive health resources to explore related diagnostic testing information.
Medical Disclaimer: This article provides educational information about COVID-19 PCR test results and should not replace professional medical advice. Always consult your healthcare provider for personalized medical guidance regarding test interpretation, isolation requirements, and treatment decisions. Test result interpretation depends on individual clinical context including symptoms, exposure history, vaccination status, and underlying health conditions. Visit mymedicineadvisor.com for additional health information and diagnostic resources.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.