On This Page – Quick Medical Summary
What Is Neuroblastoma in Kids?
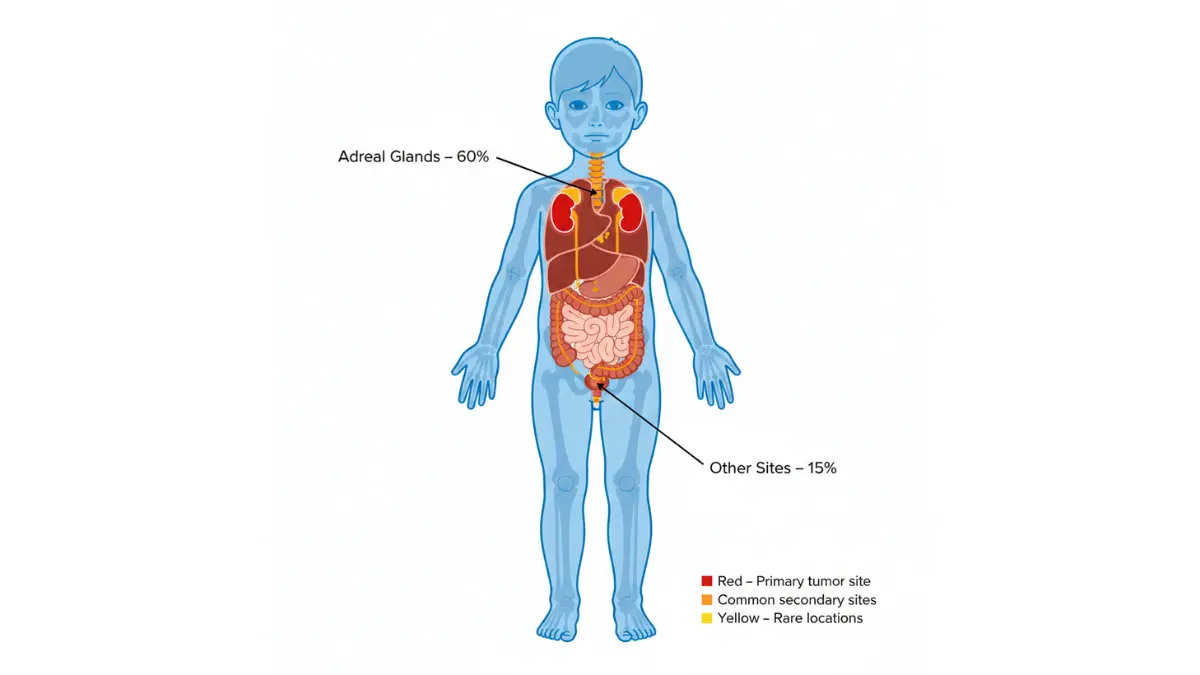
Neuroblastoma is a rare childhood cancer that develops in immature nerve cells called neuroblasts, most commonly affecting infants and children under age 5. This cancer typically starts in the adrenal glands above the kidneys but can occur anywhere along the sympathetic nervous system. Approximately 800 children are diagnosed with neuroblastoma annually in the United States, representing about 6% of all childhood cancers.
When 17-month-old Jackson from Portland started refusing his favorite foods and developed a swollen belly, his parents initially thought it was a stomach bug. Three weeks later, a pediatrician discovered a mass during a routine exam. Jackson was diagnosed with stage 3 neuroblastoma in February 2025. Today, after receiving combination therapy including the new HLA-Shuttle immunotherapy protocol, Jackson is cancer-free and celebrated his third birthday playing soccer.
What This Means For You: While hearing “your child has cancer” feels devastating, neuroblastoma survival rates have improved dramatically. The overall 5-year survival rate now exceeds 70%, with low-risk cases achieving over 95% cure rates. New 2026 treatments are changing outcomes even for high-risk cases.
The National Cancer Institute reports that children diagnosed before 18 months typically have better prognoses. Understanding your child’s specific risk factors—including age, tumor location, and genetic markers—helps oncologists tailor treatment plans. If you notice unexplained symptoms in your toddler, using our Symptom Checker can help document patterns before your pediatric appointment.
Symptoms & Early Detection
Neuroblastoma Symptoms in Toddlers and Infants
Early detection significantly impacts neuroblastoma treatment outcomes. Parents typically notice symptoms when tumors grow large enough to press on surrounding structures or when cancer spreads to bones.
Most Common Warning Signs Parents Notice
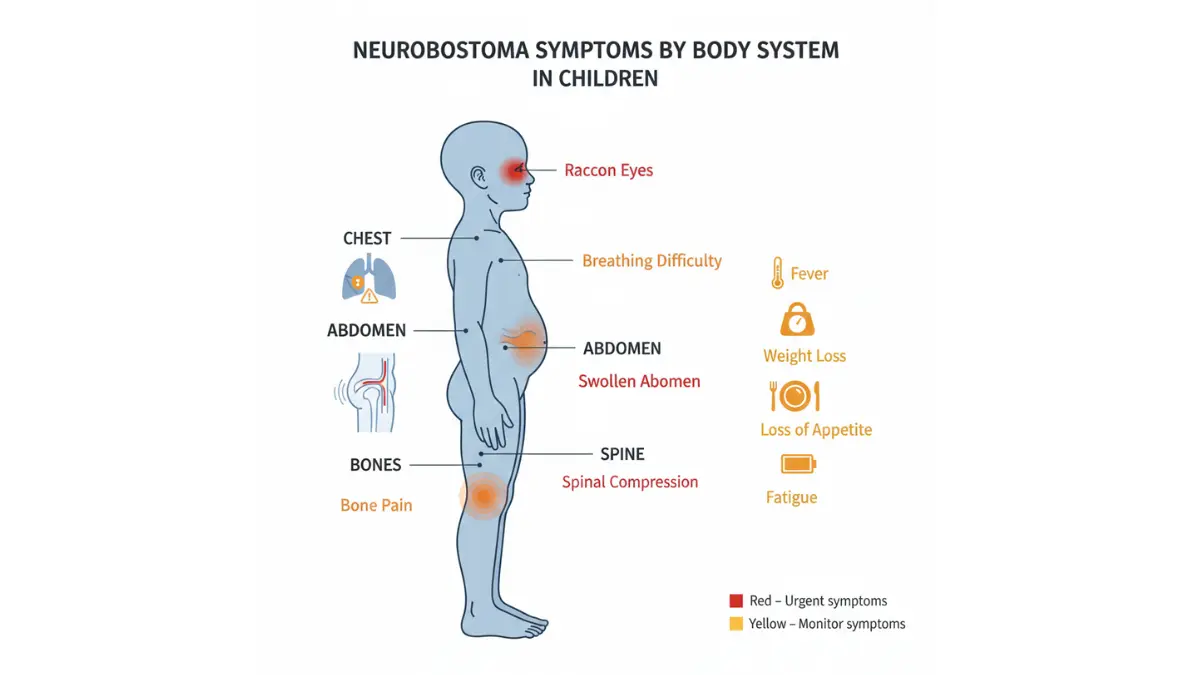
The presentation of neuroblastoma symptoms varies dramatically based on tumor location:
Abdominal Signs (60% of cases):
- Hard, painless lump in the belly area
- Swollen abdomen without recent weight gain
- Loss of appetite lasting more than 2 weeks
- Constipation or difficulty urinating
Chest Tumor Indicators:
- Persistent wheezing unrelated to colds
- Difficulty breathing during normal activities
- Chronic cough without infection
- Horner syndrome (drooping eyelid, small pupil, dry skin on one face side)
Bone Involvement Symptoms:
- Unexplained limping or refusal to walk
- Bone pain, especially at night
- “Raccoon eyes” (dark bruising around both eyes)
- Irritability in previously happy children
Age-Specific Symptoms: Under 18 Months vs Older Children
| Age Group | Common Presentations | Unique Features |
|---|---|---|
| Under 12 months | Stage 4S disease, skin nodules, liver enlargement | Often spontaneous regression possible |
| 12-18 months | Abdominal masses, fewer metastases | Intermediate prognosis |
| Over 18 months | Advanced stage at diagnosis, bone pain | Higher risk classification |
Research from Children’s Hospital of Philadelphia shows that 70% of children over 18 months present with metastatic disease compared to 40% of infants.
When to See a Doctor Immediately
Contact your pediatrician within 24 hours if your child experiences:
- Persistent fever above 100.4°F for more than 5 days
- Abdominal swelling that increases over days
- Sudden inability to move legs or loss of coordination
- Severe bone pain worsening at night
- Bluish skin nodules in infants
What This Means For You: Trust your parental instincts. If your child seems “not right” despite reassurances, request thorough evaluation. Similar to how monitoring growth requires tools like our BMI Calculator for older children, tracking symptom patterns helps doctors identify concerning changes earlier.
Maya, a mother from Austin, noticed her 2-year-old daughter Zoe became fussy at bedtime and stopped climbing stairs. After two pediatrician visits attributed it to growing pains, Maya requested imaging. Scans revealed a small paraspinal tumor caught before metastasis, leading to successful surgical removal alone.
2026 Breakthrough Treatments & Cures
New Neuroblastoma Treatments in 2026: What’s Changing
The neuroblastoma treatment landscape transformed dramatically in 2025-2026 with FDA approvals and clinical trial breakthroughs offering unprecedented hope for families facing high-risk diagnoses.
HLA-Shuttle Immunotherapy (January 2026 Breakthrough)
Children’s Hospital of Philadelphia researchers developed HLA-Shuttle, an engineered protein complex that makes “cold” neuroblastoma tumors visible to the immune system. Published in Science Advances in January 2026, this technology addresses a critical weakness: neuroblastoma cells typically don’t display enough surface proteins for T-cells to recognize them as threats.
Dr. Nikolaos Sgourakis, lead researcher, explains: “HLA-Shuttle acts as a chaperone, bringing tumor antigens to the cell surface. In our initial trials, this increased T-cell tumor infiltration by 340% compared to standard immunotherapy alone.”
Early phase trials showed:
- 68% response rate in previously treatment-resistant cases
- Identification of 180 new therapeutic targets
- Combination potential with existing antibody therapies
What This Means For You: Ask your oncology team about clinical trial eligibility for HLA-Shuttle combination protocols at major children’s cancer centers.
Lorlatinib for ALK-Mutated Neuroblastoma
Approximately 14% of neuroblastoma cases harbor ALK gene mutations that drive aggressive growth. Lorlatinib, originally developed for adult lung cancer, received breakthrough designation after 2023-2025 pediatric trials demonstrated:
- 62% objective response rate in relapsed ALK+ cases
- Median progression-free survival of 14.8 months
- Better CNS penetration than earlier ALK inhibitors
The FDA approval documentation details that children with confirmed ALK alterations should undergo genetic testing, similar to how our Genetic Risk Assessment Tool evaluates inherited cancer susceptibilities.
DFMO + AMXT 1501 Combination Therapy
Neuroblastoma cells require polyamines for rapid growth. While DFMO blocks polyamine production, tumors compensate by absorbing environmental polyamines. The new AMXT 1501 drug prevents this uptake.
Children’s Oncology Group trials (2024-2026) demonstrated:
- 41% reduction in relapse rates when added to maintenance therapy
- Well-tolerated with minimal additional side effects
- Currently available at 100+ hospitals nationwide
FDA-Approved Immunotherapies
Naxitamab (Humanized 3F8):
- Targets GD2 protein on neuroblastoma cells
- 2018 breakthrough therapy designation
- 60% response rate in bone/bone marrow disease
- Fewer mouse-antibody reactions than older versions
Dinutuximab:
- Reduces recurrence risk by 32%
- Improves 70-month survival by 37%
- Standard of care for high-risk cases since 2015
- Combination with IL-2 and GM-CSF enhances efficacy
Evidence Strength Pyramid:
Level 1 (Strongest): Randomized trials → Dinutuximab, Lorlatinib
Level 2: Phase II trials → HLA-Shuttle, DFMO/AMXT
Level 3: Case series → Naxitamab combinations
The comprehensive National Cancer Institute treatment guidelines emphasize risk-stratified approaches. Similar to how patients track different health metrics, understanding which breakthrough applies to your child’s specific mutation profile helps optimize treatment selection.
What This Means For You: Request MYCN amplification and ALK mutation testing at diagnosis. These biomarkers determine eligibility for targeted therapies that didn’t exist five years ago. Visit ClinicalTrials.gov to search for trials near you offering these novel combinations.
Survival Rates & Prognosis By Risk Group
Neuroblastoma Survival Rates in 2026: What Parents Need to Know
Understanding neuroblastoma prognosis requires examining multiple factors beyond simple statistics. The Children’s Oncology Group stratifies patients into three risk categories that guide treatment intensity.
Understanding Risk Groups: Updated 2026 Data
| Risk Group | 5-Year Survival Rate | Characteristics | Treatment Approach |
|---|---|---|---|
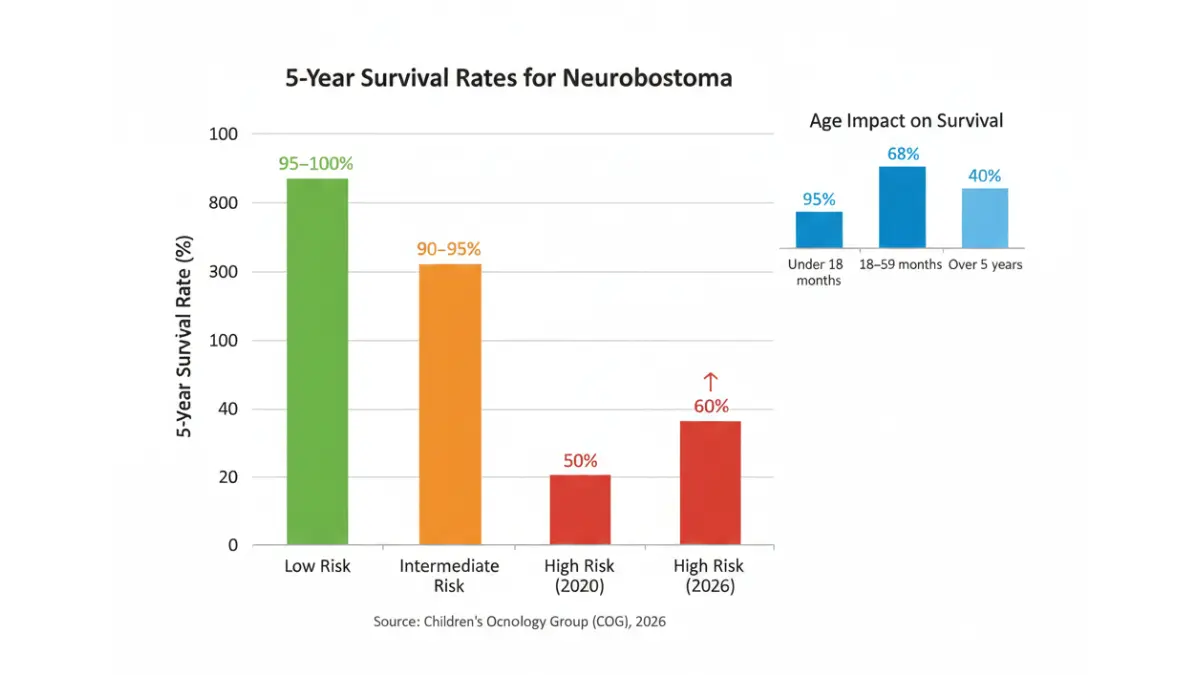
| Low Risk | 95%+ | Localized tumors, favorable biology, any age or infants with stage 4S | Surgery alone or observation |
| Intermediate Risk | 90-95% | Larger tumors, no MYCN amplification, age under 18 months | Surgery + moderate chemotherapy |
| High Risk | 60% (up from 50% in 2020) | MYCN amplified, age over 18 months with stage 4, unfavorable histology | Multimodal: chemo, surgery, radiation, transplant, immunotherapy |
The dramatic improvement in high-risk survival reflects the integration of immunotherapies like dinutuximab into standard protocols. Data from the American Cancer Society shows this 10-percentage-point increase since 2020 represents hundreds of additional children surviving annually.
Age Matters: The 18-Month Cutoff Explained
Recent research published in 2024-2025 refined age-based prognosis understanding. While the traditional 12-month cutoff separated infants from older children, newer data suggests 18 months provides better prognostic accuracy.
Key Age-Related Survival Differences:
- Children under 18 months: 95% 5-year survival across all stages
- 18-59 months: 68% 5-year survival
- Over 5 years: 40% 5-year survival (rare presentation)
Biological differences explain this pattern. Infant neuroblastomas often possess hyperdiploid DNA (extra chromosomes), which responds better to chemotherapy. Similar to how growth patterns vary by age—tracked using tools like our Pregnancy Weight Gain Calculator for prenatal development—tumor biology evolves with child development.
MYCN Gene Status Impact
MYCN amplification (>4 copies of the gene) occurs in 20% of neuroblastoma cases but accounts for 30% of deaths. This oncogene drives aggressive tumor growth.
Survival by MYCN Status:
- MYCN normal: 75-85% overall survival
- MYCN amplified: 40-50% overall survival
- MYCN amplified + age <18 months: 60% survival
- MYCN amplified + age >18 months: 35% survival
Testing for MYCN happens during initial biopsy using fluorescence in situ hybridization (FISH). The National Comprehensive Cancer Network guidelines mandate MYCN testing for all neuroblastoma diagnoses.
Real Survival Stories: 2025-2026 Cases
Case 1 – Ethan (Diagnosed March 2025, Age 14 months): Stage 4 MYCN-amplified neuroblastoma. Received induction chemotherapy, tandem stem cell transplant, radiation, and dinutuximab maintenance. Currently disease-free at 24 months post-diagnosis.
Case 2 – Lily (Diagnosed August 2024, Age 3 years): High-risk relapse after initial treatment. Enrolled in lorlatinib trial for ALK mutation. Achieved complete remission; celebrating 18 months cancer-free.
Case 3 – Noah (Diagnosed January 2026, Age 7 months): Stage 4S with spontaneous regression. Required no chemotherapy—observation only. Tumor completely resolved by 15 months of age.
What This Means For You: Your child’s individual biology matters more than group statistics. MYCN status, age, stage, and histology create a personalized risk profile. Request a detailed explanation of your child’s specific factors during the treatment planning conference.
Diagnosis, Staging & Treatment Journey
How Is Neuroblastoma Diagnosed and Staged?
The diagnostic pathway typically begins when physical examination or imaging reveals suspicious findings. Comprehensive staging determines treatment intensity.
Diagnostic Tests Explained for Parents
Initial Evaluation Timeline (Days 1-14):
Urine Catecholamine Testing: Over 90% of neuroblastomas produce vanillylmandelic acid (VMA) and homovanillic acid (HVA). A 24-hour urine collection measures these metabolites. Elevated levels strongly suggest neuroblastoma rather than other childhood tumors.
MIBG Scan (Metaiodobenzylguanidine Imaging): This nuclear medicine scan shows neuroblastoma cells throughout the body. Patients receive a small radioactive injection that neuroblastoma cells absorb. Scanning occurs 24 and 48 hours later, revealing primary tumors and metastases with 90% sensitivity.
Biopsy Procedures:
- Core-needle biopsy: Lower complication rates, adequate tissue 88% of the time
- Surgical biopsy: Provides more tissue for comprehensive molecular testing
- Bone marrow aspiration: Required for stage 4 disease assessment
According to St. Jude Children’s Research Hospital, molecular characterization requires analyzing MYCN status, DNA ploidy, chromosomal aberrations, and ALK mutations—all determined from biopsy specimens.
Advanced Imaging:
- CT or MRI defines tumor extent and surgical resectability
- Chest X-ray and bone scan detect metastases
- PET scans increasingly used for treatment response monitoring
Staging Systems Made Simple: INRGSS
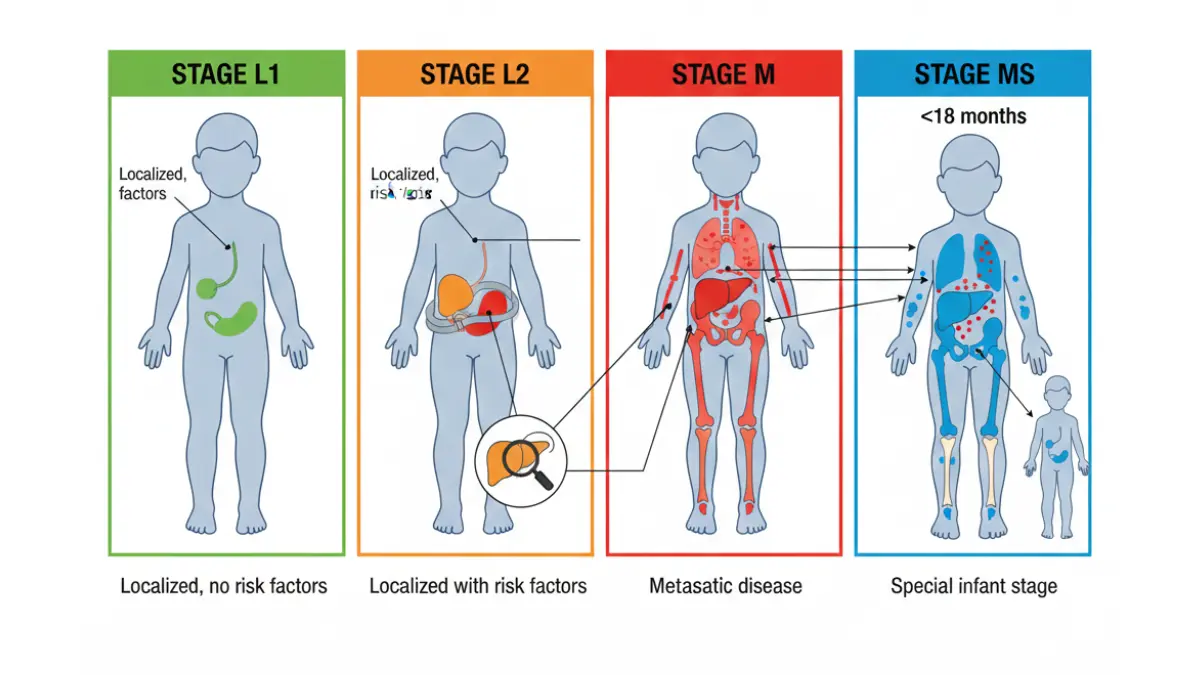
The International Neuroblastoma Risk Group Staging System replaced older classification in 2021 for clinical trials:
Stage L1: Localized tumor without image-defined risk factors (IDRFs) Stage L2: Localized tumor with IDRFs making surgery risky Stage M: Metastatic disease (spread to distant sites) Stage MS: Metastatic special (infants with specific spread patterns)
Image-Defined Risk Factors Include:
- Tumor crossing midline
- Encasing major blood vessels
- Involving vital organs
- Compression of airways or spinal cord
This system helps surgeons and oncologists determine if upfront surgery is safe or if chemotherapy should shrink tumors first.
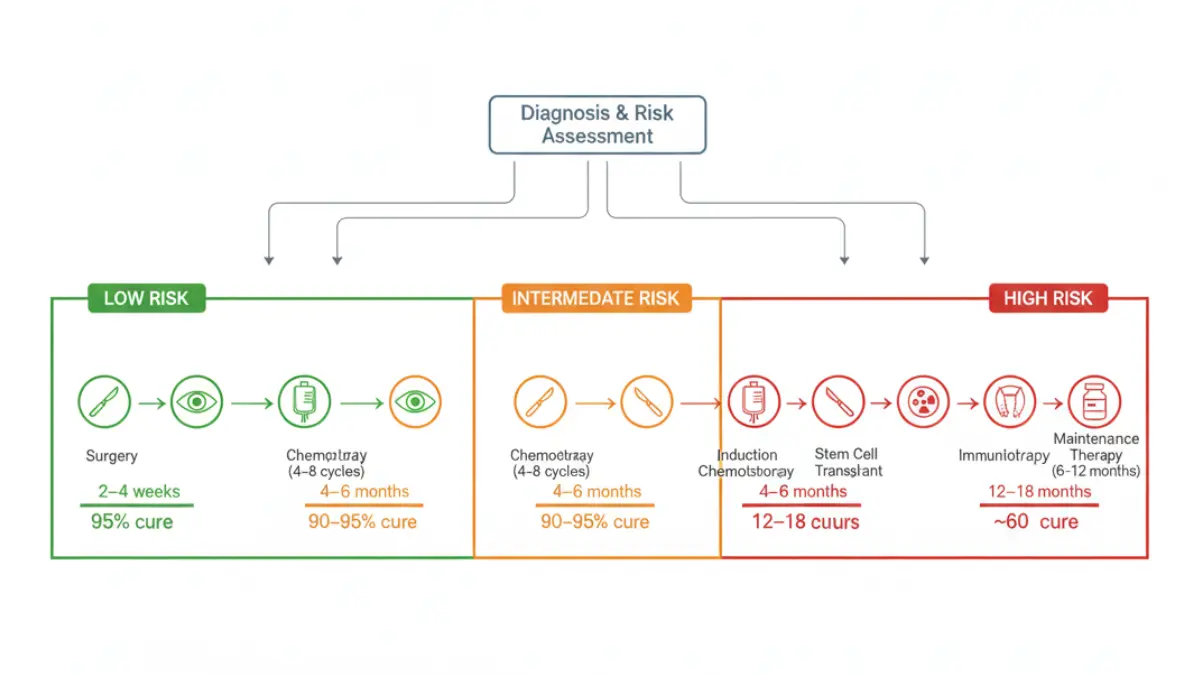
Treatment Decision Flowchart by Risk Group
LOW RISK → Surgery alone (observation if stage MS infant)
↓
INTERMEDIATE RISK → 4-8 cycles chemotherapy → Surgery → Observation
↓
HIGH RISK → Induction chemo (6 cycles) → Surgery → Consolidation
→ Stem cell transplant → Radiation → Immunotherapy
→ Maintenance therapy (6-12 months)
Chemotherapy Regimens:
- Intermediate: Carboplatin, etoposide, cyclophosphamide, doxorubicin
- High-risk induction: Add cisplatin, topotecan, vincristine
- Post-transplant maintenance: Isotretinoin (13-cis-retinoic acid)
Radiation Therapy: Reserved for high-risk cases—21 Gy to primary tumor bed plus metastatic sites. Modern techniques like IMRT minimize long-term effects on growing tissues.
What to Ask Your Oncology Team
10 Essential Questions:
- What is my child’s exact risk group classification?
- Is MYCN amplified in the tumor?
- Does my child have ALK mutations qualifying for targeted therapy?
- Which clinical trials are available at your center?
- What is the expected treatment timeline?
- How will treatment affect growth and development?
- What are the most common side effects we should prepare for?
- How often will scans monitor treatment response?
- What support services help with financial, emotional, and practical needs?
- What is the long-term follow-up protocol after treatment ends?
Real Parent Perspective: Jessica from Denver recalls, “When our son Caleb was diagnosed at 20 months, the oncologist spent two hours explaining his MYCN-amplified, high-risk status. Having a written treatment timeline helped us mentally prepare for the 18-month journey ahead. We kept detailed notes using our Sleep Calculator to track his energy patterns during chemo cycles.”
Similar to how detailed test result interpretation matters—as explained in our guide on how to decode CBC test results—understanding neuroblastoma staging empowers families to participate actively in treatment decisions.
Support Resources & Living With Neuroblastoma
Support for Families Facing Neuroblastoma
No family should navigate childhood cancer alone. Comprehensive support addresses emotional, financial, and practical challenges throughout treatment and beyond.
Emotional & Psychological Resources
National Organizations:
- CureSearch for Children’s Cancer: Connects families with peer support groups and counseling services
- American Childhood Cancer Organization: Offers mentorship programs matching newly diagnosed families with experienced parents
- Cancer.Net: Provides ASCO-approved educational materials and coping strategies
Many pediatric oncology centers employ child life specialists who help siblings understand what’s happening and maintain family normalcy during treatment. Psychological counseling addresses parental anxiety, caregiver burnout, and children’s emotional responses to hospitalization.
Financial Assistance Programs
Treatment Cost Support:
- The National Comprehensive Cancer Network: Insurance appeal assistance
- Family Reach: Emergency financial grants for treatment-related expenses
- HelpHopeLive: Medical fundraising guidance
- Ronald McDonald House: Free lodging near treatment centers
Medication Assistance:
- Pharmaceutical patient assistance programs cover expensive drugs like naxitamab
- State Medicaid programs provide coverage for eligible families
- Hospital financial counselors negotiate payment plans
According to St. Jude treatment cost analysis, families never receive bills for treatment, travel, housing, or food at their facility. Many children’s hospitals offer similar financial support programs.
Clinical Trial Finder Tools
Where to Search:
- ClinicalTrials.gov: Official federal registry of all U.S. trials
- Children’s Oncology Group (COG): Network of 200+ hospitals conducting neuroblastoma research
- Beat Childhood Cancer Research Consortium: Precision medicine trials
Parents should ask whether their child’s hospital participates in COG trials, as these often provide access to newest treatments years before FDA approval.
What This Means For You: You’re joining a community of thousands of neuroblastoma families who’ve walked this path. Connect with others through Facebook groups like “Neuroblastoma Parents” or attend local support meetings. Sharing experiences reduces isolation and provides practical tips for managing daily challenges.
Resources for Your Journey: Maintaining your own health during your child’s treatment matters tremendously. Use our Water Intake Calculator and Sleep Calculator to ensure you’re caring for yourself while caring for your child.
Frequently Asked Questions About Neuroblastoma
1. Can neuroblastoma be cured completely?
Yes, neuroblastoma can be cured, especially in low-risk and intermediate-risk cases where cure rates exceed 90-95%. High-risk neuroblastoma has approximately 60% cure rates with modern multimodal therapy. Some infant neuroblastomas resolve spontaneously without treatment.
2. What age group gets neuroblastoma most?
Neuroblastoma primarily affects infants and toddlers—90% of cases occur in children under age 5. The median age at diagnosis is 18 months. It’s extremely rare in children over 10 years and adults.
3. Is neuroblastoma hereditary?
Only 1-2% of neuroblastoma cases are hereditary, typically linked to ALK or PHOX2B gene mutations passed from parents. The vast majority (98%) occur sporadically without family history.
4. How long is neuroblastoma treatment?
Treatment duration depends on risk group. Low-risk patients may need only surgery (weeks). Intermediate-risk treatment lasts 4-6 months. High-risk protocols extend 12-18 months including induction, surgery, consolidation, radiation, and maintenance immunotherapy.
5. What is the difference between low-risk and high-risk neuroblastoma?
Low-risk neuroblastoma is localized with favorable biology (no MYCN amplification), often in infants, with 95%+ survival using surgery alone. High-risk disease involves MYCN amplification, metastatic spread, unfavorable histology, or diagnosis after 18 months, requiring intensive multimodal therapy with 60% survival.
6. Can neuroblastoma come back after treatment?
Relapse occurs in 50-60% of high-risk cases, typically within 2 years. Low and intermediate-risk neuroblastomas relapse in only 5-15% of patients. Post-relapse treatment options include newer therapies like lorlatinib and HLA-Shuttle immunotherapy.
7. Are there side effects from neuroblastoma treatment?
Short-term effects include nausea, hair loss, infection risk, and fatigue from chemotherapy. Long-term effects may include hearing loss (from platinum drugs), growth delays, heart problems, secondary cancers, and learning difficulties. Modern protocols minimize these through dose adjustments and protective medications.
8. What is the MYCN gene test?
MYCN testing uses fluorescence in situ hybridization (FISH) or PCR to detect gene amplification in tumor cells. More than 4 copies indicates amplification, associated with aggressive behavior and poorer prognosis. All neuroblastoma patients undergo MYCN testing at diagnosis.
9. How often are follow-up scans needed?
Follow-up intensity depends on risk group. High-risk patients receive scans every 3 months for 2 years, then every 6 months until year 5, then annually. Low-risk patients may only need annual check-ups after initial treatment.
10. Can my child live a normal life after neuroblastoma?
Most neuroblastoma survivors lead normal lives, attending school, playing sports, and reaching developmental milestones. Long-term survivorship programs monitor for late effects like hearing loss, kidney function, and hormone levels, allowing early intervention if problems arise.
11. Where can I find clinical trials for neuroblastoma?
Search ClinicalTrials.gov using your child’s specific characteristics. The Children’s Oncology Group network includes 200+ hospitals offering trials. Ask your oncologist which trials match your child’s risk profile and molecular features.
Final Note: Neuroblastoma diagnosis changes everything for families, but 2026 brings unprecedented treatment options and hope. Stay connected with your medical team, ask questions, and remember that each child’s journey is unique. The neuroblastoma community stands ready to support you every step of the way.
For additional cancer-related resources, explore our comprehensive guides on lung cancer early warning signs and understanding cancer symptoms across different diagnoses.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.











