On This Page – Quick Medical Summary
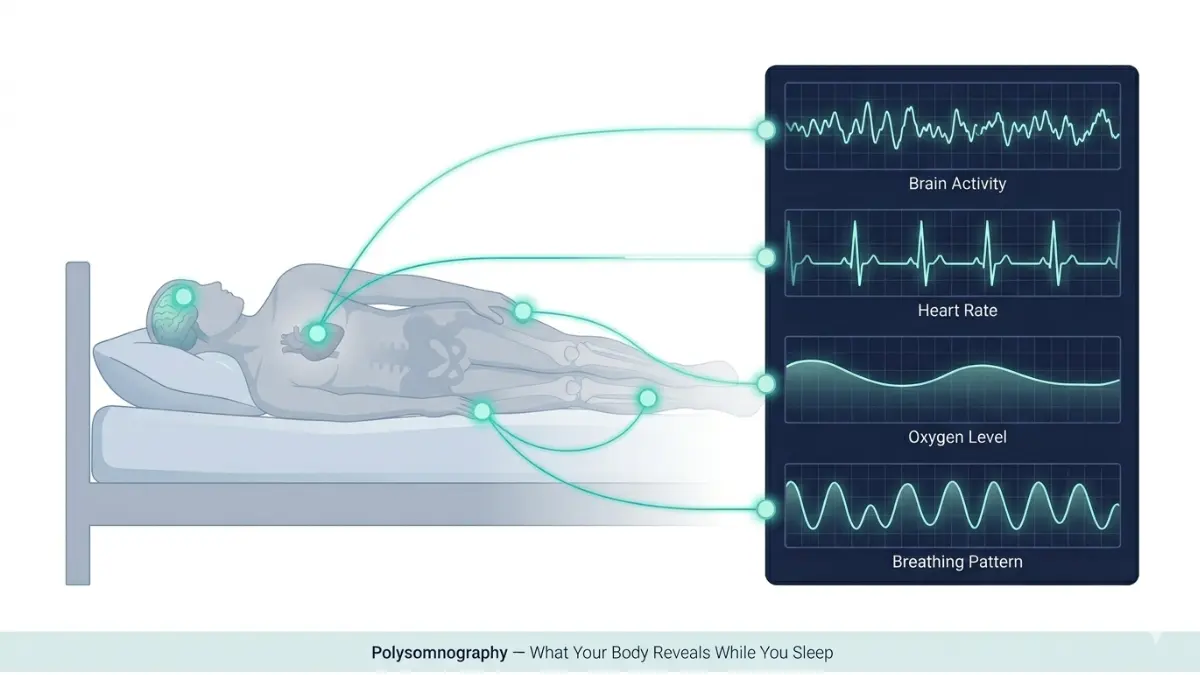
A sleep study, or polysomnography, is an overnight diagnostic test that records your brain waves, breathing patterns, heart rate, blood oxygen levels, and body movements while you sleep. It diagnoses conditions like sleep apnea, narcolepsy, restless legs syndrome, and REM sleep behavior disorder — and most insurance plans cover it fully when medically necessary.
If you’ve been told you need a sleep study, you’re not alone. Over 50 million Americans live with an undiagnosed sleep disorder. One night of testing can change your health trajectory permanently.
⚠️ This article is for educational purposes only and does not constitute medical advice. Always consult a qualified healthcare professional for diagnosis and treatment.
What Is a Sleep Study and Who Actually Needs One?
The Gold Standard for Diagnosing Sleep Disorders
A sleep study — clinically called a polysomnography test or PSG — is the most comprehensive diagnostic tool available for sleep disorders. It doesn’t just record whether you slept; it maps every biological signal your body produces during each sleep cycle, from the deepest slow-wave sleep to rapid eye movement (REM) stages.
The National Heart, Lung, and Blood Institute classifies untreated sleep disorders as a major public health risk, linked to heart disease, hypertension, Type 2 diabetes, and motor vehicle accidents.
A sleep study is typically ordered when a patient shows persistent symptoms that a standard office visit cannot explain. If you’re experiencing any of the following, your physician may refer you for an in-lab sleep study or a home sleep apnea test:
- Loud, chronic snoring reported by a bed partner
- Witnessed breathing pauses during sleep (gasping, choking)
- Waking up exhausted despite 7–9 hours in bed — a sign worth exploring further in our guide on why you’re always tired no matter how much sleep you get
- Excessive daytime sleepiness — falling asleep at work, while driving, or mid-conversation (learn more about excessive daytime sleepiness symptoms)
- Morning headaches upon waking
- Frequent nighttime urination (nocturia) without a urological cause
- Unexplained high blood pressure not responding to medication
- Sleepwalking, night terrors, or acting out dreams
Before your appointment, tracking your actual sleep duration with our free Sleep Calculator can give your doctor valuable baseline data about your patterns.
What Conditions Does a Sleep Study Diagnose?
| Sleep Disorder | PSG Diagnoses It? | Notes |
|---|---|---|
| Obstructive Sleep Apnea (OSA) | ✅ Gold Standard | Most common indication |
| Central Sleep Apnea | ✅ Yes | Requires full PSG |
| Narcolepsy | ✅ Yes (with MSLT follow-up) | Requires additional daytime test |
| Restless Legs Syndrome / PLMD | ✅ Yes | Leg movement sensors required |
| REM Sleep Behavior Disorder | ✅ Yes | In-lab PSG required |
| Sleepwalking / Parasomnia | ✅ Yes | Video monitoring essential |
| Chronic Insomnia alone | ⚠️ Limited | Clinical evaluation usually preferred |
Real Patient Perspective: James, a 48-year-old teacher from Ohio, was referred for a sleep study after his wife noticed he stopped breathing multiple times each night. He assumed he was “just a loud snorer.” His sleep study revealed an AHI of 34 — severe obstructive sleep apnea. Six weeks after starting CPAP therapy, his blood pressure dropped significantly and his daytime fatigue resolved. One night of testing changed his life.
If you’re unsure whether your symptoms qualify for a referral, our Symptom Checker can help you prepare a focused conversation with your doctor. You can also review the warning signs of a sleep disorder that doctors look for before ordering testing.
Types of Sleep Studies — In-Lab vs. At-Home (Which One Will You Have?)
The 4 Official Types of Sleep Studies
Most patients don’t realize there are four distinct types of sleep studies. Your doctor’s choice depends on your symptoms, suspected condition, and insurance coverage. This is a critical gap in nearly every competitor article — they blur these categories together.
| Type | Setting | Channels Monitored | Best Used For |
|---|---|---|---|
| Type 1 (PSG) | Sleep lab — attended by technologist | Full (EEG, EOG, EMG, ECG, airflow, SpO2, leg movement) | Gold standard; complex or unclear cases |
| Type 2 (Portable PSG) | Home — unattended | Full channels, no technologist present | OSA when lab access is limited |
| Type 3 (Cardiorespiratory) | Home | Airflow, breathing effort, SpO2, heart rate | Suspected moderate-to-severe OSA only |
| Type 4 (Single/Dual Channel) | Home | 1–2 channels (usually SpO2 + airflow) | Screening only; not sufficient for diagnosis |
Key clinical rule: Home sleep studies (Types 2–4) can only diagnose obstructive sleep apnea. If your doctor suspects narcolepsy, REM behavior disorder, parasomnia, or periodic limb movement disorder, you will require a Type 1 in-lab polysomnography — no exceptions.
Split-Night Study: What Is It?
A split-night study combines two tests in one overnight session. The first half of the night is used to confirm an OSA diagnosis; if your apnea-hypopnea index (AHI) exceeds 20–30 events per hour in the first few hours, the technologist initiates CPAP titration during the second half. This approach saves time and reduces the cost of a second visit.
CPAP Titration Study
If your initial sleep study confirms moderate or severe sleep apnea, a CPAP titration study determines the precise air pressure setting your CPAP machine needs. Some patients complete this as part of a split-night study; others return for a separate titration night.
Multiple Sleep Latency Test (MSLT) — For Narcolepsy
The MSLT is typically performed the morning after a full overnight PSG. You are given five scheduled 20-minute nap opportunities, two hours apart. Technologists measure how quickly you fall asleep and whether you enter REM sleep during those naps. A sleep latency under 8 minutes with two or more REM-onset periods strongly indicates narcolepsy. Understanding your sleep stages in detail can help you interpret why these REM patterns matter so much clinically.
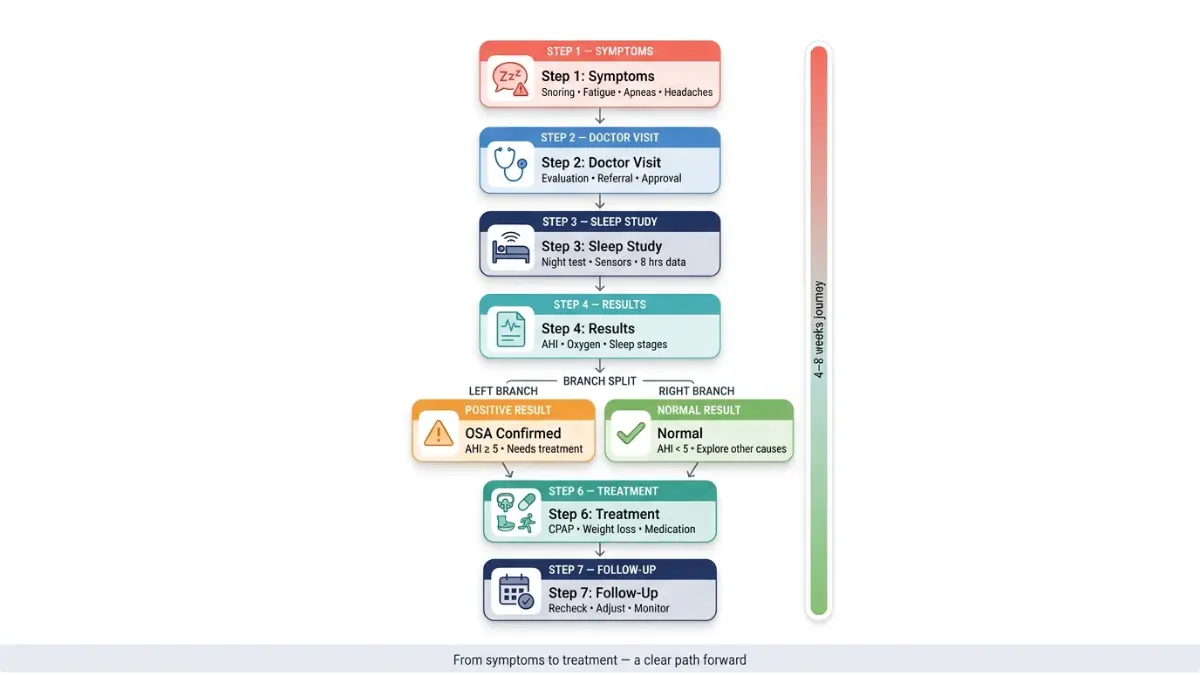
What Actually Happens During a Sleep Study? A Step-by-Step Timeline
This is the section most patients search for most urgently — and where almost every competitor fails to provide enough reassuring detail.
Before You Arrive: How to Prepare for a Sleep Study
Your preparation begins 24–48 hours before the test. Following these instructions carefully ensures your data is accurate and your night is as comfortable as possible.
Avoid on the day of your sleep study:
- Caffeine after noon (coffee, tea, energy drinks, sodas) — read why caffeine disrupts sleep architecture so profoundly
- Alcohol at any point during the day
- Daytime napping (prevents natural sleep pressure from building)
- Sleeping pills unless your doctor specifically instructs otherwise
- Heavy perfumes or scented products (interfere with sensor adhesion)
Bring with you:
- Comfortable sleepwear (two-piece pajamas are easiest with sensors)
- Your usual toiletries, pillow if preferred, and any book or light entertainment
- A complete list of your current medications
- Your insurance card and any referral paperwork
Arrival and Check-In (Typically 8–9 PM)
You arrive at the sleep center approximately 2 hours before your normal bedtime. Most accredited sleep centers in the US — particularly those certified by the American Academy of Sleep Medicine — provide private rooms that resemble a comfortable hotel, not a hospital ward. You change into your sleepwear, meet your sleep technologist, and settle in before sensor placement begins.
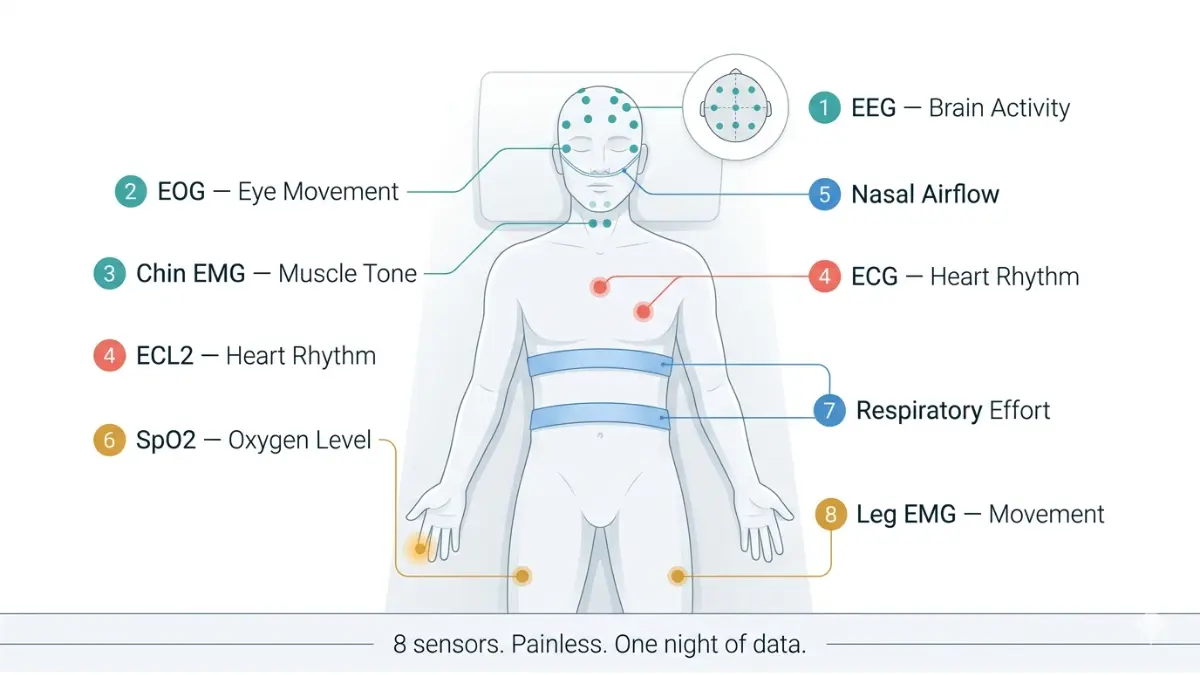
Sensor Placement — What Are All Those Wires For?
This is the step that makes most patients anxious — and the step that almost universally turns out to be painless. Here is exactly what each sensor measures:
| Sensor | Placement | What It Records |
|---|---|---|
| EEG electrodes | Scalp (paste or gel) | Brain wave activity; identifies sleep stages N1, N2, N3, REM |
| EOG leads | Outer edges of eyes | Eye movements; confirms REM sleep onset |
| EMG electrodes | Chin and legs | Muscle tone and leg movements (REM paralysis, PLMD) |
| ECG leads | Chest | Heart rhythm; detects arrhythmias during sleep |
| Pulse oximeter | Fingertip | Blood oxygen saturation (SpO2) continuously |
| Nasal pressure transducer | Nostrils | Airflow; detects apneas and hypopneas |
| Chest/abdominal bands | Torso | Breathing effort and movement |
| Body position sensor | Chest | Whether apnea worsens in specific sleep positions |
The entire setup process takes 30–45 minutes. Despite the number of sensors, most patients fall asleep within 30–45 minutes of lights-out — the sensors are not painful and the rooms are temperature-controlled and darkened.
If you need to use the bathroom during the night, the technologist monitoring you via video will disconnect your sensors temporarily and reconnect them when you return.
During the Night
A trained sleep technologist monitors your data in real time from an adjacent room throughout the entire night. They observe your sleep stages, breathing events, oxygen levels, and body movements as they happen. If a split-night study is planned and your AHI reaches the threshold, they will enter your room gently to fit you with a CPAP mask for the second half of the night.
Morning: What Happens When You Wake Up?
You are typically woken at 6–7 AM. The sensors are removed — this takes about 10 minutes — and you are free to leave. Most patients are discharged by 7:30 AM and can go directly to work.
Your results are not available immediately. The raw data from your sleep study is reviewed and scored by a board-certified sleep medicine physician, a process that typically takes 1–2 weeks.
💡 Important: Many patients ask whether they can take sleep medications before their study. In most cases, the answer is no — medications that alter sleep architecture (including common sleep aids and certain antidepressants) can significantly distort your results. Review medications that cause insomnia and discuss your full medication list with your ordering physician before the test.
Since obesity is a major independent risk factor for obstructive sleep apnea, your referring doctor may also assess your body weight as part of your evaluation. You can check your own risk profile using our BMI Calculator.
What Does a Sleep Study Actually Measure? Every Metric Explained
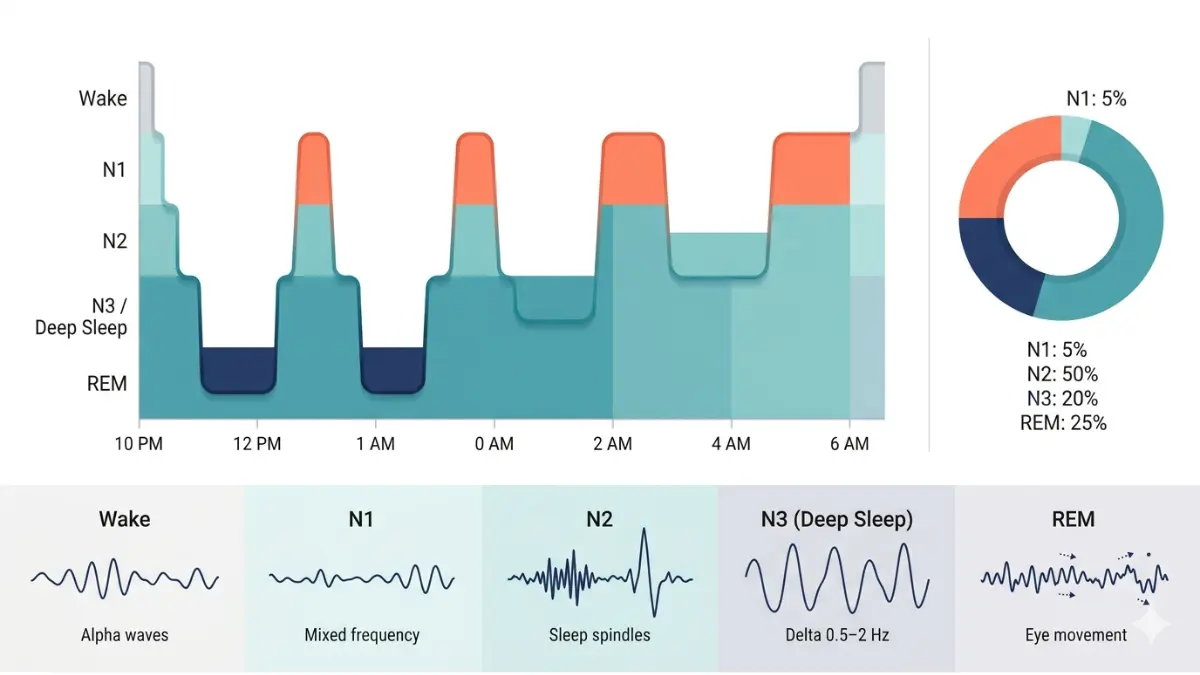
Brain Wave Activity: Mapping Your Sleep Architecture
The EEG component of your polysomnography maps exactly which sleep stage you are in throughout the night. A healthy adult cycles through approximately 4–5 complete sleep cycles per night, each lasting 90–110 minutes.
| Sleep Stage | EEG Pattern | Normal % of Night | What Abnormalities Suggest |
|---|---|---|---|
| N1 (Light Sleep) | Theta waves | 5% | Excessive N1 = fragmented, non-restorative sleep |
| N2 (Intermediate) | Sleep spindles, K-complexes | 45–55% | Reduced N2 seen in insomnia |
| N3 (Deep/Slow-Wave) | Delta waves | 15–20% | Reduced in aging, depression, alcohol use |
| REM Sleep | Desynchronized, rapid eye movements | 20–25% | Loss of REM atonia = REM behavior disorder |
Understanding what REM sleep actually does and why its disruption matters can help you interpret your results with much greater clarity.
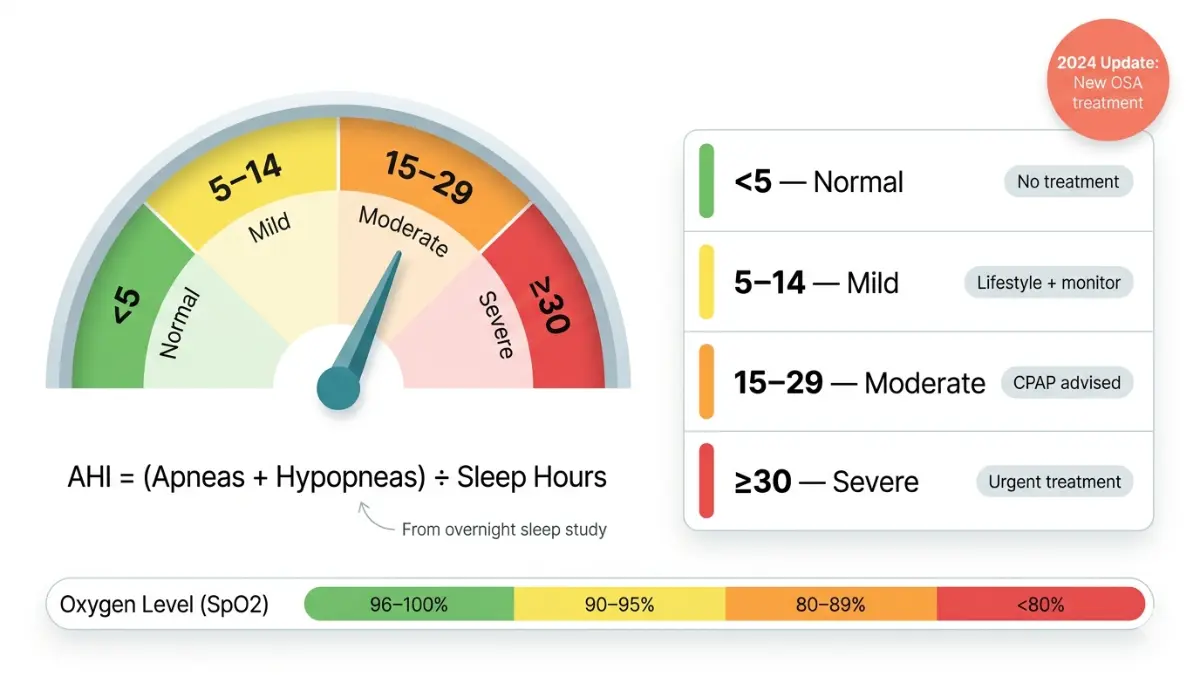
The AHI Score: The Single Most Important Number in Your Results
The Apnea-Hypopnea Index (AHI) is calculated by dividing the total number of apneas (complete breathing pauses lasting ≥10 seconds) and hypopneas (partial breathing reductions) by total sleep time in hours. It is the primary metric used to diagnose and classify obstructive sleep apnea.
| AHI Score | Classification | Clinical Action |
|---|---|---|
| < 5 events/hour | Normal | No sleep apnea diagnosis |
| 5–14 events/hour | Mild OSA | Lifestyle changes; CPAP may be recommended with symptoms |
| 15–29 events/hour | Moderate OSA | CPAP therapy strongly recommended |
| ≥ 30 events/hour | Severe OSA | Urgent CPAP initiation; cardiovascular risk assessment |
🆕 2026 Clinical Update: In December 2024, the FDA approved tirzepatide (Zepbound) as the first medication specifically indicated for moderate-to-severe obstructive sleep apnea in adults with obesity. This landmark approval means that for patients who cannot tolerate CPAP, a pharmacological option now exists. This was confirmed in clinical trials showing tirzepatide reduced AHI by up to 62.8% in participants. Discuss eligibility with your sleep specialist.
Blood Oxygen Saturation (SpO2): Reading the Desaturation Data
Your sleep study will report your minimum SpO2 level and the percentage of time spent below 90% saturation. Here is how to interpret these values:
| SpO2 Level | Classification | Health Implication |
|---|---|---|
| 96–100% | Normal | Healthy oxygenation during sleep |
| 90–95% | Mild Desaturation | May indicate sleep-disordered breathing |
| 80–89% | Moderate Desaturation | Increased cardiovascular strain |
| < 80% | Severe Desaturation | Urgent intervention required |
According to Harvard Medical School’s Division of Sleep Medicine, oxygen desaturation events are independently associated with long-term cardiac arrhythmia risk, even at AHI levels that would be classified as mild.
AHI vs. RDI — The Number Your Doctor May Not Explain
This distinction is almost completely absent from competitor content — yet it matters enormously for many patients.
- AHI counts only full apneas and hypopneas (with ≥3–4% oxygen drops)
- RDI (Respiratory Disturbance Index) also includes respiratory effort-related arousals (RERAs) — subtle breathing disturbances that fragment sleep and cause daytime fatigue without meeting the AHI threshold
Two patients can have an identical AHI of 8 (technically “mild”) yet have drastically different RDI scores and symptom severity. If you feel exhausted after your sleep study despite a “low” AHI — ask your doctor specifically for your RDI.
💡 What This Means For You: Your AHI alone does not tell the complete story. Request your minimum SpO2, time below 90% SpO2, RDI, and sleep efficiency percentage when reviewing your results with your physician.
Sleep Study Cost, Insurance Coverage, and How to Read Your Results
How Much Does a Sleep Study Cost in 2026?
Cost is the single biggest concern preventing Americans from getting tested — and competitors either bury this information or omit insurance nuance entirely.
| Study Type | Without Insurance | With Insurance (Typical In-Network) |
|---|---|---|
| In-lab PSG (Type 1) | $1,000–$10,000 (avg. ~$3,000) | $0–$200 post-deductible |
| At-home sleep apnea test (HSAT) | $150–$1,000 | $0–$50 post-deductible |
| CPAP Titration Study | $1,000–$3,000 | $0–$150 post-deductible |
| MSLT (Narcolepsy follow-up) | $1,500–$4,000 | Variable by plan |
The dramatic price range for in-lab studies reflects facility charges (hospital-based sleep centers bill significantly more than freestanding centers), geographic variation, and whether your deductible has been met.
Does Insurance Cover a Sleep Study?
Most major insurance plans cover sleep studies when medically necessary. This includes Medicare, Medicaid, and private insurers including Aetna, UnitedHealthcare, Cigna, and BlueCross BlueShield. However, specific requirements apply.
To maximize coverage:
- Ensure your doctor documents your symptoms in your medical record before the referral
- Confirm your chosen sleep center is in-network before scheduling
- Ask whether your insurer requires a home sleep test first (many prefer HSAT for uncomplicated suspected OSA)
- Use HSA or FSA funds — sleep studies qualify as eligible medical expenses under IRS guidelines, effectively reducing your cost by 20–30% depending on your tax bracket
Medicare Coverage for Sleep Studies — 2026 Update
Medicare Part B covers polysomnography and home sleep apnea tests when ordered by a physician to screen for obstructive sleep apnea, narcolepsy, or parasomnia.
2026 Medicare Part B specifics:
- Annual deductible: $283
- Monthly premium: $185 (2025 rate; 2026 update pending)
- Patient coinsurance: 20% of Medicare-approved amount
- Medicare pays: 80%
Important: Medicare does not cover sleep studies ordered solely to diagnose chronic insomnia. The ordering physician must document clinical signs of a covered condition. For full coverage criteria, refer directly to the CMS Medicare Coverage Database — Polysomnography Article A56903.
When Will You Get Your Sleep Study Results?
Your raw polysomnography data is typically reviewed by a board-certified sleep medicine physician within 1–2 weeks of your study date. You will then receive a follow-up appointment to discuss findings.
After a positive sleep study:
- Mild OSA: Lifestyle modification discussion (weight management, positional therapy, alcohol reduction)
- Moderate OSA: CPAP therapy initiation; possible return titration study
- Severe OSA (AHI ≥ 30): Urgent CPAP prescription, typically within 2–4 weeks; cardiovascular risk evaluation
- Narcolepsy confirmed: Referral to sleep neurologist; medication management discussion
💡 Lifestyle Connection: Untreated sleep apnea is independently associated with elevated cardiovascular risk and insulin resistance. As part of your post-diagnosis management, tracking your daily water intake and understanding your metabolic baselines matters. Use our Water Intake Calculator to support hydration goals during recovery — dehydration worsens daytime fatigue in OSA patients.
Should You Ask for a Sleep Study? Red Flags, Special Populations, and Expert Guidance
7 Symptoms That Should Prompt a Sleep Study Referral — 2026 Clinical Checklist
Per current American Academy of Sleep Medicine guidelines, the following symptoms in any combination constitute sufficient clinical grounds to request a polysomnography referral:
- Habitual snoring (most nights, loud enough to disturb others)
- Witnessed apneas — a partner observes you stop breathing during sleep
- Waking gasping or choking — even if you don’t recall it in the morning
- Unrefreshing sleep — consistently tired despite adequate sleep hours; if this sounds familiar, our article on why you’re always tired no matter how much sleep you get explores the full clinical picture
- Morning headaches — caused by CO₂ accumulation during apnea events
- Hypertension resistant to medication — OSA is a secondary cause in up to 30% of resistant hypertension cases
- Frequent nocturnal urination (nocturia) — often caused by negative intrathoracic pressure during apnea events stimulating atrial natriuretic peptide release
Special Populations — What Competitors Completely Miss
Children: The diagnostic threshold for pediatric OSA is different. An AHI above 1 event per hour is considered abnormal in children, compared to the adult threshold of 5. Children with Down syndrome, enlarged tonsils, obesity, or attention deficit disorders should be screened proactively. Knowing recommended sleep hours by age helps parents identify whether their child’s sleep quantity and quality fall within healthy ranges.
Pregnant women: OSA prevalence increases significantly during the second and third trimesters due to weight gain and hormonal changes affecting airway muscle tone. The American College of Obstetricians and Gynecologists recommends sleep apnea screening for pregnant patients with hypertension, obesity, or snoring. If you are pregnant and tracking weight gain, our Pregnancy Weight Gain Calculator can help identify whether your gain trajectory aligns with guidelines.
Shift workers: Many accredited sleep centers offer sleep studies during daytime hours, scheduled around the patient’s natural sleep window. Night-shift nurses, truck drivers, and emergency responders are significantly underdiagnosed because they assume their fatigue is occupational rather than pathological. It isn’t always.
Expert Global Panel: What Sleep Specialists Want You to Know
“Untreated sleep apnea doubles the risk of systemic hypertension and significantly elevates the risk of atrial fibrillation. I’ve seen patients spend years on blood pressure medications who simply needed a sleep study. One overnight test can be genuinely life-saving.” — Dr. Omar Hassan, MD, Internal Medicine, mymedicineadvisor.com Expert Panel
“We now have robust data linking obstructive sleep apnea with insulin resistance and worsened glycemic control in Type 2 diabetes. Any of my diabetic patients with unexplained fatigue or poor glucose control gets screened for OSA — it’s become standard practice in our endocrinology clinic.” — Dr. Vikram Nair, MD, Endocrinology, mymedicineadvisor.com Expert Panel
“The most common thing patients tell me after their sleep study is that they didn’t sleep ‘as well as usual’ because of the wires. What they don’t realize is that the study doesn’t require perfect sleep — even 2–3 hours of solid data is usually sufficient for an accurate diagnosis.” — Dr. Aditi Menon, MD, mymedicineadvisor.com Expert Panel
What This Means For You — Your Action Steps Today
If you have two or more of the symptoms listed above, do not wait.
- ✅ Use our Symptom Checker to document your symptoms clearly before your GP visit
- ✅ Track your nightly sleep patterns for 1–2 weeks using our Sleep Calculator
- ✅ Check whether your BMI places you in a higher OSA risk category with our BMI Calculator
- ✅ Ask your doctor specifically: “Do my symptoms warrant a sleep study referral?”
- ✅ Contact your insurance provider to confirm in-network sleep centers before scheduling
A sleep study takes one night. The diagnosis it delivers can add years — and quality — to your life.
Frequently Asked Questions About Sleep Studies
1. Can I actually fall asleep during a sleep study with all those wires?
Yes — the vast majority of patients do fall asleep. The sensors are painless and the room is darkened and temperature-controlled. Studies show sufficient diagnostic data is collected even from patients who feel they “slept poorly.”
2. How long does a sleep study take?
An in-lab sleep study lasts 8–9 hours. You arrive approximately 2 hours before your usual bedtime and are discharged in the morning, typically by 7:30 AM.
3. What should I avoid before a sleep study?
Avoid caffeine after noon, alcohol throughout the day, daytime napping, and sleeping medications (unless specifically instructed). Arrive with clean, product-free hair for better electrode adhesion.
4. Can I bring my own pillow to a sleep study?
Yes. Most sleep centers actively encourage patients to bring their own pillow, blanket, and sleepwear to make the environment feel as home-like as possible. Comfort improves data quality.
5. Is a sleep study painful?
No. Sensors are applied using gentle adhesive paste or tape. No needles, no invasive procedures. The most common complaint is mild scalp itchiness from the electrode paste, which washes out easily in the morning.
6. What is a normal AHI score on a sleep study?
An AHI below 5 events per hour is considered normal in adults. Mild OSA is 5–14, moderate is 15–29, and severe is 30 or more events per hour.
7. Can a sleep study detect anxiety or depression?
A sleep study does not directly diagnose anxiety or depression, but it can identify sleep architecture disruptions — such as shortened REM latency or fragmented N3 sleep — that are strongly associated with both conditions. Sleep and depression are deeply connected, and treating one often improves the other.
8. How much does a sleep study cost without insurance in 2026?
An in-lab sleep study averages approximately $3,000 without insurance, with a range of $1,000–$10,000 depending on facility type and location. Home sleep apnea tests range from $150 to $1,000.
9. Is a home sleep test as accurate as an in-lab sleep study?
For diagnosing moderate-to-severe obstructive sleep apnea in otherwise healthy adults, home tests are reasonably accurate. However, they underestimate OSA severity in some cases and cannot diagnose any other sleep disorder. If your home test is negative but symptoms persist, an in-lab PSG is the recommended next step.
10. What happens if my sleep study comes back normal but I still feel tired?
A normal PSG rules out sleep-disordered breathing, but does not rule out all causes of fatigue. Your doctor may investigate circadian rhythm disorders, upper airway resistance syndrome (UARS — detected by RDI, not AHI), insomnia, or medical causes. Read our full breakdown on what causes insomnia and explore sleep disorder symptoms and causes for next steps.
11. How soon will I get my sleep study results?
Typically 1–2 weeks after your test date. Your sleep physician scores and interprets the full data set, then a follow-up appointment is scheduled to review findings and discuss treatment options.
Sources: National Heart, Lung, and Blood Institute | Harvard Medical School Division of Sleep Medicine | CMS Medicare Coverage Database | American Academy of Sleep Medicine | MedlinePlus — Polysomnography
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.