On This Page – Quick Medical Summary
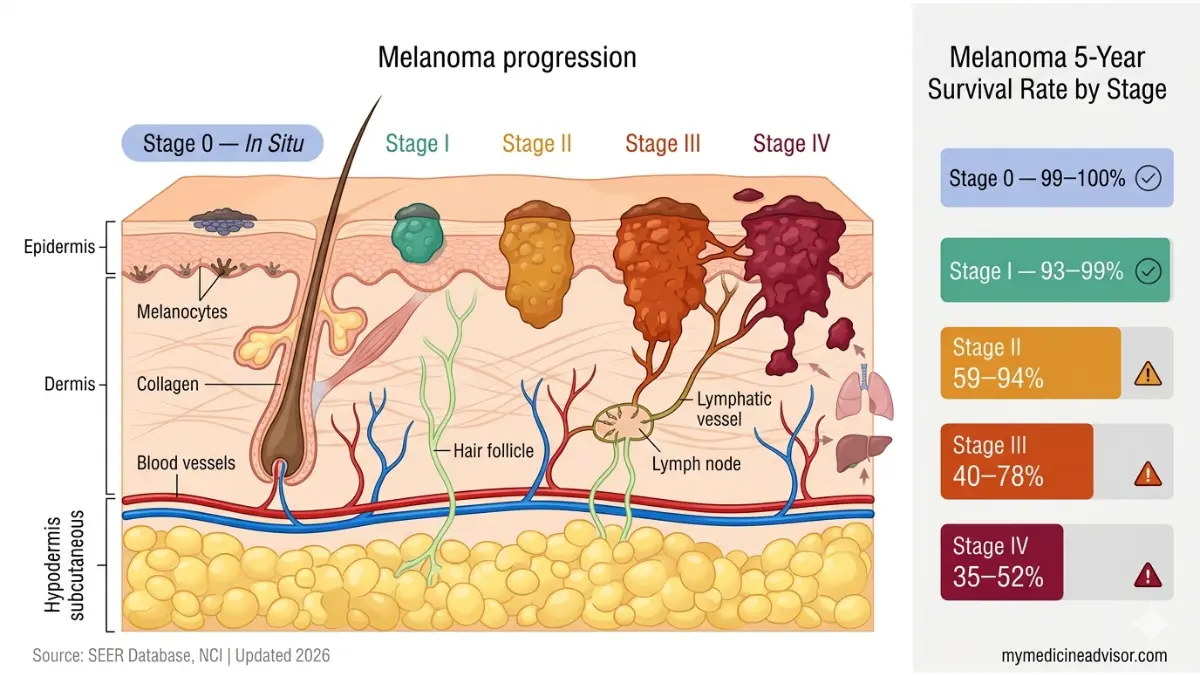
The overall melanoma survival rate in the U.S. is 93.3% — but that single number hides a story that could change everything you think you know. Stage 0 melanoma carries a near-perfect 99–100% 5-year survival rate. Untreated Stage 4 historically sat at 15–20%. Today, thanks to immunotherapy breakthroughs, Stage 4 survival has climbed to 35–52%. Here is exactly what every stage means for real patients in 2026.
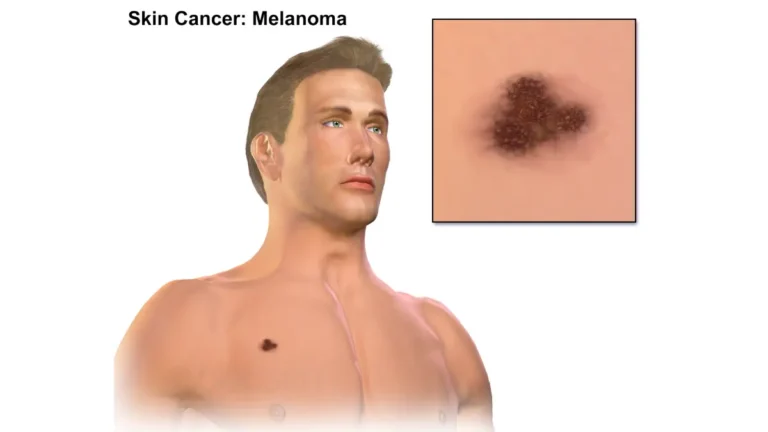
Marcus T., 47, was told his Stage IIC melanoma had a “guarded prognosis.” His dermatologist caught it during a routine skin exam after Marcus noticed a mole changing shape on his back. After surgical excision and adjuvant immunotherapy, Marcus completed 12 months of treatment and is currently 4 years disease-free. His case is not unusual — it reflects exactly what the data shows: stage at diagnosis is the single most powerful predictor of melanoma outcome.
What the Melanoma Survival Rate Actually Means
Understanding the Numbers Before You Read Them
The 5-year relative survival rate answers one question: What percentage of people with this cancer are alive 5 years after diagnosis, compared to people without cancer?
It does not mean a patient will only live 5 years. It is a population average — not a personal forecast.
According to the SEER database maintained by the National Cancer Institute, melanoma survival statistics are tracked across hundreds of thousands of patients diagnosed over multi-year periods. The data you read today reflects patients diagnosed 5–10 years ago, which means current patients likely have better outcomes than what the statistics show — because treatments have improved dramatically since then.
What “Relative Survival” Actually Measures
- Observed survival = the actual percentage of patients alive at a given timepoint
- Relative survival = compares that rate to the general population of the same age/sex — removing deaths from unrelated causes
This distinction matters. A 90% relative survival rate means melanoma patients are about 90% as likely as similar healthy individuals to be alive at 5 years.
Key Takeaway: The melanoma survival rate is a benchmark, not a verdict. Your oncologist’s evaluation of your specific tumor — Breslow depth, ulceration status, BRAF mutation — tells you far more than any population average.
If you have a family history of skin cancer or atypical moles, our Genetic Risk Assessment Tool can help you understand your personal genetic risk profile before symptoms ever appear.
Melanoma Survival Rate by Stage — The Complete 2026 Data Table
The Stage-by-Stage Breakdown Competitors Won’t Give You
Most websites show you three numbers — localized, regional, distant. That is not enough.
The AJCC (American Joint Committee on Cancer) staging system breaks melanoma into substages. Knowing whether you are Stage IIIA or Stage IIID is the difference between a 78% and a 40% 5-year survival rate. That gap matters enormously — and most major health websites bury it in a single “Stage III” figure.
Here is the complete 2026 breakdown, integrating data from the American Cancer Society and updated immunotherapy-era clinical trial results:
📊 Master Melanoma Survival Rate Table by Stage (2026)
| Stage | Sub-stage | 5-Year Survival Rate | Key Characteristics |
|---|---|---|---|
| Stage 0 | Melanoma in situ | 99–100% | Abnormal cells in top skin layer only; near-complete cure |
| Stage I | IA | 97–99% | Thin tumor (≤1mm), no ulceration, no lymph node involvement |
| Stage I | IB | 93–97% | Slightly thicker or with mitosis; still very low recurrence risk |
| Stage II | IIA | 81–94% | Intermediate thickness; higher local recurrence risk begins |
| Stage II | IIB | 73–82% | Thick tumor or ulcerated; classified high-risk |
| Stage II | IIC | 59–67% | Thick + ulcerated; highest-risk Stage II substage |
| Stage III | IIIA | ~78% | Microscopic lymph node spread; often still very treatable |
| Stage III | IIIB–IIIC | ~50–63% | Regional lymph node involvement confirmed |
| Stage III | IIID | ~40% | Extensive regional disease; adjuvant therapy critical |
| Stage IV | Distant (pre-2010) | 15–20% | Historical baseline — chemotherapy era only |
| Stage IV | Distant (2024–2026) | 35–52% | Immunotherapy + targeted therapy era |
Sources: SEER 2021 data; ACS 2024; CheckMate 067 5-year OS data; KEYNOTE-006 trial data
Why Stage III Is Not One Number
Stage IIIA has nearly double the survival rate of Stage IIID. This is the most critical gap in competitor content — they report “Stage III: approximately 63%,” which means nothing to a patient who needs to know their sub-stage.
Always ask your oncologist: “What is my specific AJCC sub-stage — am I IIIA, IIIB, IIIC, or IIID?”
The Stage IV Revolution
A decade ago, a Stage IV melanoma diagnosis meant a median survival of 8–9 months. That is no longer the reality. For a full breakdown of the treatment options driving this change, read our deep-dive on Stage 4 melanoma survival and emerging therapies.
What This Means For You: If you or a loved one received a Stage III or Stage IV diagnosis, immediately ask your oncology team for your full AJCC sub-stage classification. That single conversation could completely reframe your prognosis conversation.
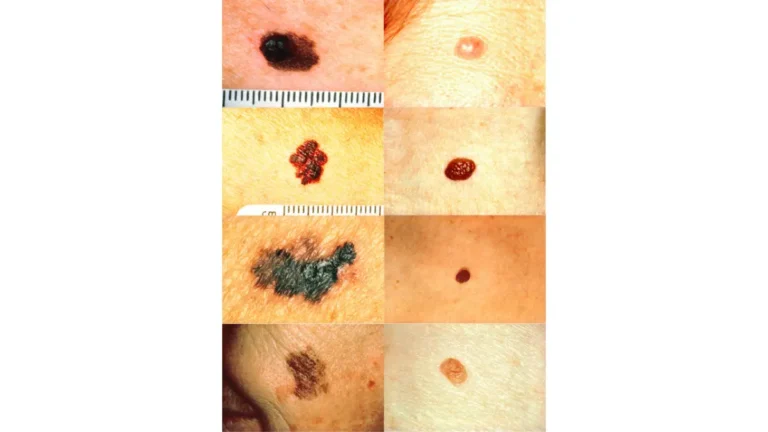
If you notice any changes in existing moles or new skin lesions, use our Symptom Checker to help determine whether an urgent dermatology evaluation is warranted.
7 Factors That Directly Change Your Melanoma Survival Rate
Why Two People With “Stage II” Can Have Very Different Outcomes
The melanoma survival rate by stage is just the starting framework. Within every stage, these seven biological and demographic factors dramatically shift individual prognosis — and most competing articles completely omit them.
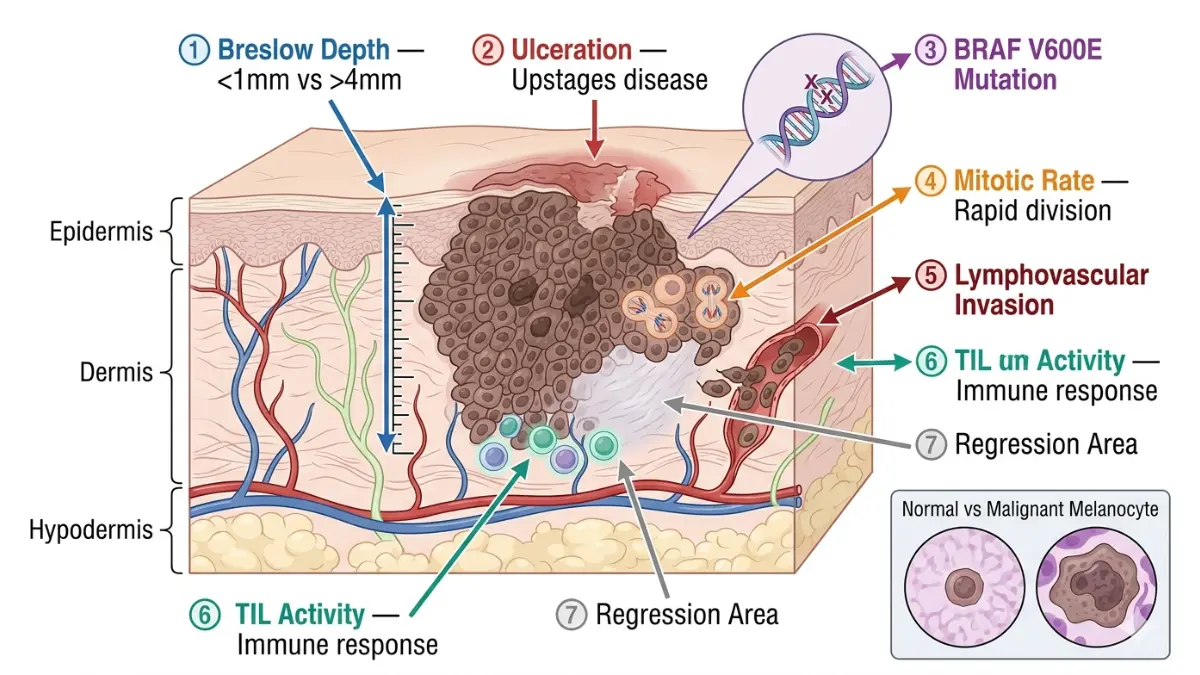
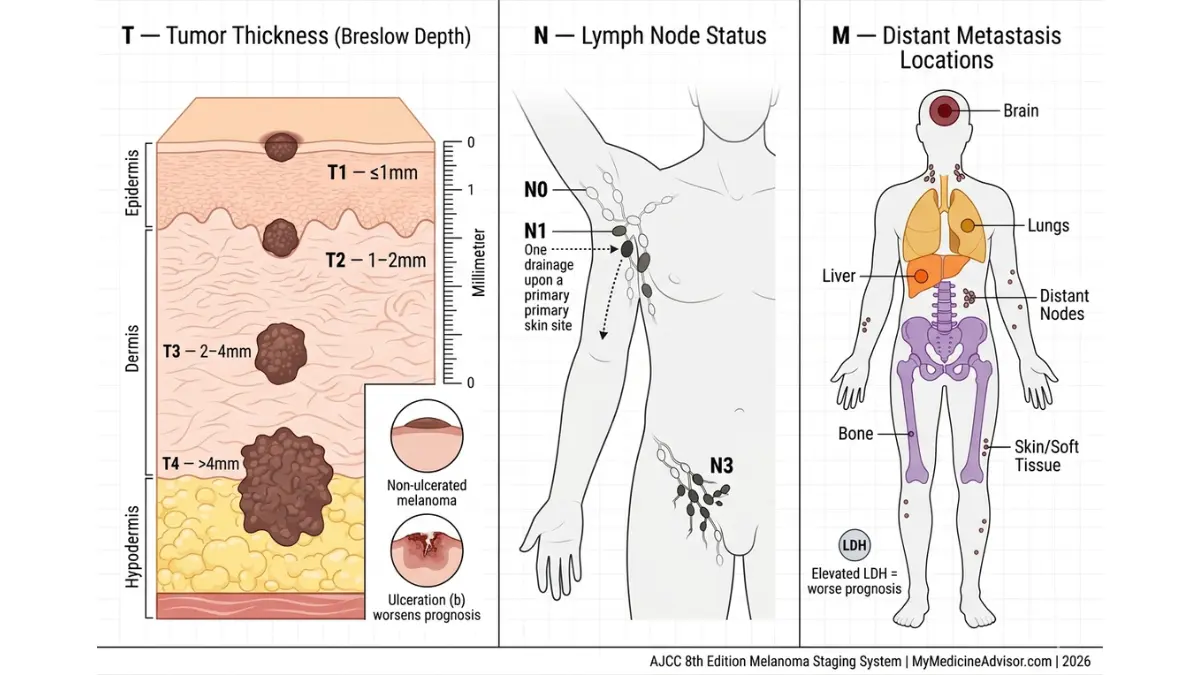
1. Tumor Thickness (Breslow Depth)
This is the single most important pathological factor. Tumors thinner than 1mm (T1) carry dramatically better outcomes than tumors deeper than 4mm (T4). A T1a tumor has a near-98% 5-year survival; a T4b (thick + ulcerated) tumor places a patient in Stage IIC with survival rates dropping to 59–67%.
2. Ulceration Status
Ulceration — the breakdown of skin over the tumor — automatically moves a patient one sub-stage higher. A non-ulcerated 2mm tumor may be Stage IIA; the same tumor with ulceration becomes Stage IIB. This single pathological finding can meaningfully alter your prognosis conversation.
3. BRAF V600E Mutation Status
Approximately 50% of all melanomas carry the BRAF V600E mutation. For these patients, BRAF/MEK inhibitor combinations (dabrafenib + trametinib) offer precision-targeted treatment that significantly improves Stage III–IV survival rates. Every Stage III and IV patient should have BRAF mutation testing performed immediately after diagnosis. You can learn more about melanoma blood tests and biomarkers to understand what labs your oncologist should be ordering.
4. Age at Diagnosis
Younger patients (under 40) consistently outperform older patients at equivalent stages, even after adjusting for stage, depth, and sex. Patients over 65 show higher melanoma-specific mortality at all stages, reflecting immune senescence and later-stage diagnosis patterns.
5. Sex and Gender
Women diagnosed with cutaneous melanoma show a statistically significant survival advantage over men at all stages — a finding consistent across multiple large SEER database analyses, including a landmark PMC study of 68,000+ melanoma cases. This advantage persists even after adjusting for depth, ulceration, and lymph node status. The biological mechanism is not fully understood but may involve sex hormone effects on immune surveillance.
6. Immune System Status
Patients with compromised immune systems — organ transplant recipients on immunosuppressive drugs, HIV-positive individuals, or those on long-term corticosteroids — face significantly elevated melanoma-specific mortality at all stages. Their immune systems cannot mount the same defense as immunologically intact patients, and immunotherapy drugs may be less effective.
7. Lactate Dehydrogenase (LDH) Level in Stage IV
Elevated LDH is an independent negative prognostic marker for Stage IV melanoma. It indicates high tumor burden and metabolic activity. Normal LDH in Stage IV carries meaningfully better outcomes than elevated LDH at the same radiographic stage. This is why staging in melanoma involves both imaging and blood biomarkers — not imaging alone.
What This Means For You: At your next oncology appointment, ask specifically about your Breslow depth, ulceration status, and BRAF mutation result. These three data points may matter more to your personal melanoma survival rate than your stage number alone.
How Immunotherapy Is Rewriting Melanoma Survival Rate Statistics in 2026
From 8 Months to 5+ Years: The Most Dramatic Turnaround in Oncology
No other cancer type has seen a more dramatic improvement in survival statistics than melanoma. Understanding this transformation helps patients — especially those at Stage III and IV — make informed decisions about their treatment options.
The Pre-Immunotherapy Baseline (Before 2011)
Before 2011, metastatic melanoma was treated primarily with dacarbazine chemotherapy. Median overall survival for Stage IV patients was approximately 8–9 months. The 5-year melanoma survival rate for distant metastases sat at 15–20%. Clinical oncologists referred to it as one of oncology’s most treatment-resistant cancers.
📊 The Immunotherapy Revolution — Stage IV Survival Over Time
| Era | Stage IV 5-Year Survival | Key Treatment |
|---|---|---|
| Pre-2010 | 15–20% | Dacarbazine chemotherapy |
| 2011–2014 | ~25% | Ipilimumab (CTLA-4 inhibitor) |
| 2014–2019 | 35–44% | Pembrolizumab / Nivolumab (anti-PD-1) |
| 2020–2024 | 44–52% | Nivolumab + Ipilimumab combination |
| 2024–2026 | 51%+ | TIL cell therapy + checkpoint combos |
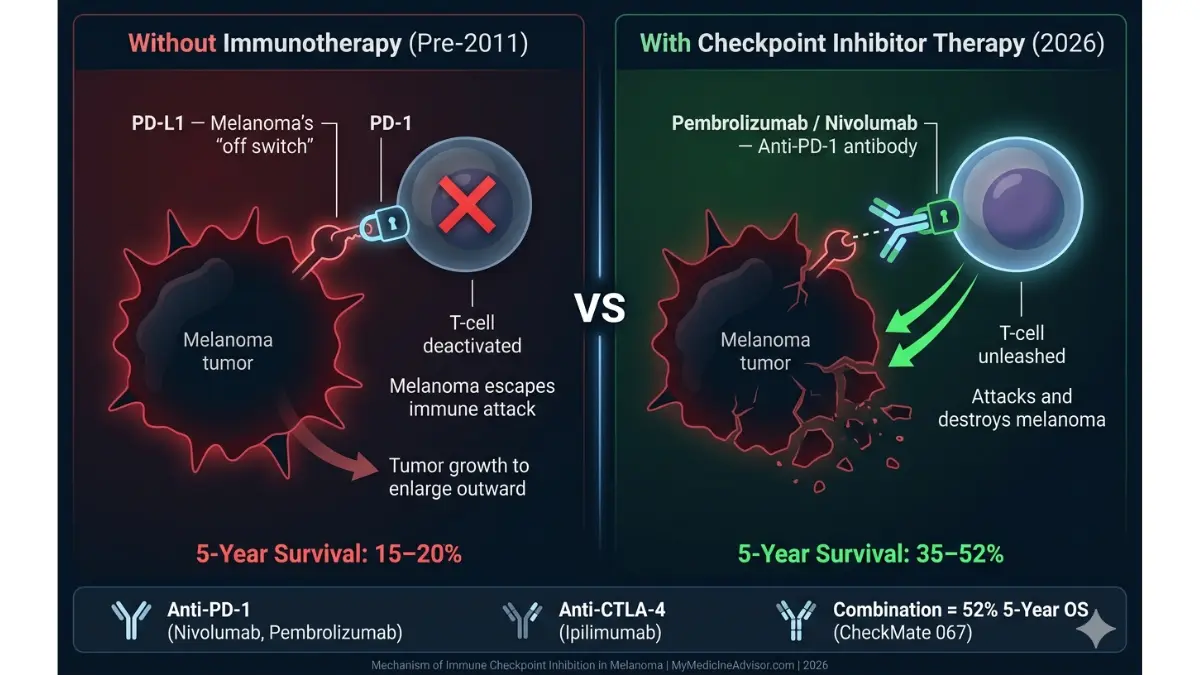
Checkpoint Inhibitors: The Game-Changer
The KEYNOTE-006 trial demonstrated that pembrolizumab improved 2-year overall survival to 55% compared to 43% with ipilimumab alone — a statistically significant breakthrough. In the CheckMate 067 trial, published in the New England Journal of Medicine via PubMed Central, combination nivolumab + ipilimumab achieved a 5-year overall survival rate of 52% in metastatic melanoma patients. This compared to just 26% with ipilimumab alone.
These are not marginal improvements. They represent a fundamental change in what Stage IV melanoma means for patients diagnosed today. To understand how immunotherapy works at a biological level, our article on how immunotherapy works explains the mechanism in clear, accessible terms.
BRAF-Targeted Therapy for Mutation-Positive Patients
For the approximately 50% of melanoma patients with the BRAF V600E mutation, targeted therapy combinations (dabrafenib + trametinib; vemurafenib + cobimetinib) offer rapid tumor reduction with 5-year OS data now ranging from 34–44% in Stage IV. These drugs are often used in patients with high tumor burden who need rapid response before immunotherapy can take effect.
TIL Cell Therapy: The 2024 FDA Breakthrough
In February 2024, the FDA approved lifileucel (Amtagvi) — a tumor-infiltrating lymphocyte (TIL) cell therapy — for unresectable or metastatic melanoma that has progressed on prior immunotherapy. Early data shows objective response rates of 36% and 5-year survival projections exceeding 51% in heavily pre-treated patients. This is particularly significant for the approximately 30% of Stage IV patients who do not respond adequately to first-line checkpoint inhibitors.
What This Means For You: If you received a Stage IV melanoma diagnosis before 2020, your statistics are almost certainly more optimistic today. Always ask your oncologist whether you qualify for current clinical trials — you can search active melanoma trials at ClinicalTrials.gov.
Melanoma Survival Rate by Age, Gender, Race & Global Comparisons
The Data Points That Mainstream Articles Ignore Completely
The melanoma survival rate is not uniform across all demographics — and understanding these variations helps patients contextualize their personal outlook.
By Age at Diagnosis
| Age Group | Stage I–II 5-Yr Survival | Stage III–IV 5-Yr Survival |
|---|---|---|
| Under 40 | 98–99% | Significantly better than average |
| 40–65 | 93–95% | Moderate advantage over 65+ |
| Over 65 | 87–91% | Lower due to immune senescence |
Younger patients derive greater benefit from immunotherapy, show stronger immune responses, and are more likely to achieve complete remission at Stage III–IV.
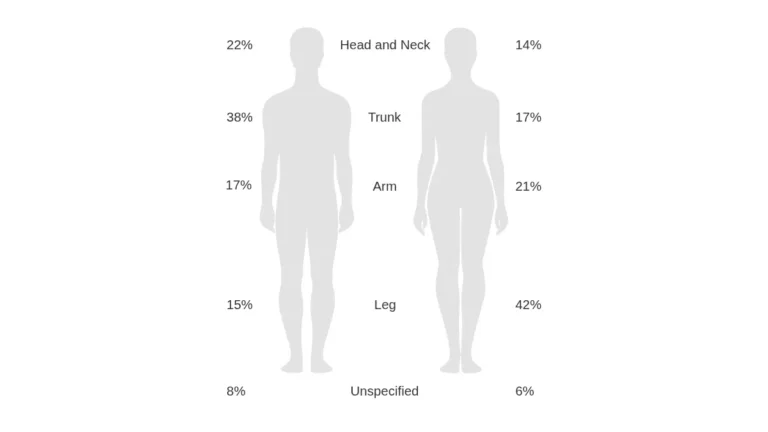
By Gender
Women at every melanoma stage show measurably better 5-year survival than men. This survival advantage persists even after controlling for stage, age, Breslow depth, and ulceration status. The most widely supported hypothesis involves differences in immune regulation influenced by sex hormones — though behavioral factors (women seek earlier dermatological evaluation) also contribute.
By Race and Ethnicity
Patients of color are disproportionately diagnosed at later melanoma stages, contributing to lower aggregate survival statistics. This is not a biological difference — it reflects systemic inequities in dermatological access and awareness. Acral lentiginous melanoma, which occurs on palms, soles, and nail beds, is more common in Black and Asian patients and is frequently diagnosed at later stages due to lower index of suspicion. For information on nail-based melanoma specifically, our article on subungual and nail melanoma covers the warning signs in detail.
🌍 Global Melanoma Survival Rate Comparison
| Country | Overall 5-Year Survival | Notable Factors |
|---|---|---|
| USA | 93.3% | Advanced treatment access; SEER 2021 data |
| Australia | ~96% (20-year data) | Early detection culture; high UV awareness |
| UK | ~87% | NHS access timelines; later-stage detection |
| Europe (avg.) | 85–90% | Varies significantly by healthcare system |
Australia’s superior long-term survival data reflects decades of aggressive public health education and earlier-stage detection culture. The Cancer Research UK melanoma survival statistics document the NHS gap compared to US outcomes, particularly at Stage III.
The Australian Institute of Health and Welfare melanoma data confirms that Australia’s 20-year survival rate for localized melanoma reaches approximately 96% — a benchmark that reflects what aggressive early detection can achieve at the population level.
What This Means For You: If you are a man over 50 with fair skin and a family history of melanoma, you are statistically in the highest-risk demographic. Annual full-body skin checks and awareness of the ABCDE warning signs of melanoma are your most powerful tools — not treatment, but prevention and early detection.
Staying well-hydrated during cancer treatment supports immune function and recovery. Our Water Intake Calculator can help you calculate your optimal daily fluid intake during and after treatment.
Just Diagnosed? What Your Melanoma Survival Rate Really Means for You
Turn Statistics Into Action — 6 Steps That Change Outcomes
A melanoma diagnosis is terrifying. The first 72 hours after receiving staging results are often characterized by information overload, fear, and a desperate search for context. Here is the structured action plan that translates melanoma survival statistics into real, outcome-changing steps.
Step 1: Confirm Your Exact AJCC Sub-Stage
Do not accept “Stage II” or “Stage III” as a final answer. Ask your oncologist: “Am I Stage IIA, IIB, or IIC?” or “Am I Stage IIIA, IIIB, IIIC, or IIID?” As shown in the survival table above, these sub-stages carry dramatically different 5-year survival rates — sometimes spanning a 30–40 percentage point gap.
Step 2: Request BRAF Mutation Testing Immediately
Every Stage III and Stage IV melanoma patient should have molecular tumor profiling completed within the first week of diagnosis. A positive BRAF V600E result opens access to highly effective targeted therapy combinations that could meaningfully improve your melanoma prognosis. Understanding your melanoma diagnosis process will help you ask the right questions at every appointment.
Step 3: Ask About Clinical Trial Eligibility
As of 2026, dozens of active melanoma clinical trials are enrolling patients — including Stage II high-risk (IIC) patients, not just Stage III and IV. The survival data underpinning modern treatments came from clinical trials. You can search active trials by stage and location at ClinicalTrials.gov.
Step 4: Seek a Second Opinion at an NCI-Designated Cancer Center
The National Cancer Institute’s melanoma treatment information recommends specialist evaluation for all high-risk melanoma cases. NCI-designated comprehensive cancer centers have melanoma multidisciplinary tumor boards that review cases weekly. A second opinion is not disloyalty to your doctor — it is a standard of care at this level.
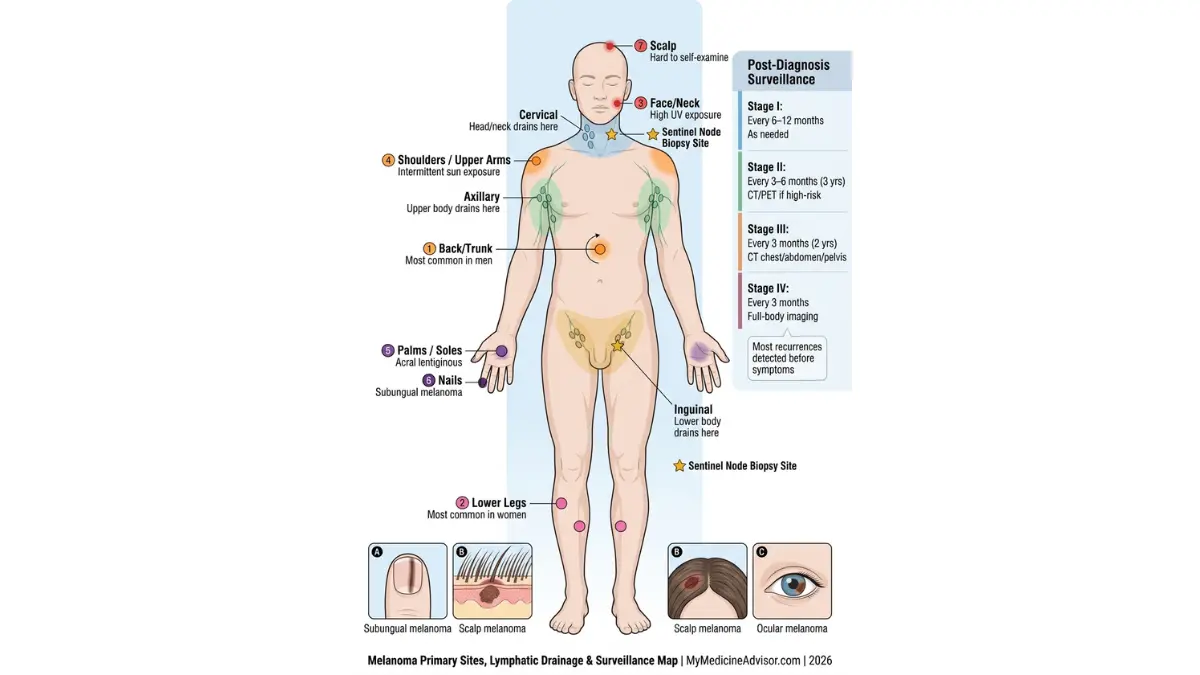
Step 5: Establish Your Surveillance Schedule
- Stage I: Full skin examination every 6–12 months for 5 years
- Stage II: Every 3–6 months for 3 years, then annually
- Stage III–IV: Every 3 months for 2 years, with imaging as directed
Most melanoma recurrences are detectable before symptoms appear — if you are being monitored correctly. Regular monitoring also extends to your overall health. Quality sleep directly supports immune function during and after treatment; our Sleep Calculator can help you optimize your rest schedule around treatment cycles.
Step 6: Know the Warning Signs of Recurrence
- New or enlarged lymph nodes
- New skin lesions or satellite nodules near the original site
- Unexplained fatigue, weight loss, or bone pain
If you notice any of these, do not wait for your next scheduled appointment. Use the Symptom Checker to assess urgency, and contact your oncology team the same day.
The Number That Matters Most
The statistics in this article represent thousands of patients averaged across years of data. They do not represent you specifically. Thousands of people diagnosed with Stage IV melanoma today are alive and in sustained remission. Stage IIC patients who were classified “high risk” 10 years ago are now achieving outcomes once reserved for Stage I.
“The most important number is not the survival statistic. It is how quickly you acted, the quality of your oncology team, and whether you asked the right questions at the right time.”
For the full clinical picture of melanoma — from warning signs through treatment options and surveillance — our comprehensive Melanoma Symptoms, Stages & Treatment guide covers every stage of the patient journey in one place. And if you have a family history that concerns you, our Genetic Risk Assessment Tool provides a personalized genetic risk profile based on your family history and biological factors.
Frequently Asked Questions About Melanoma Survival Rate
Q1: What is the overall melanoma survival rate in the United States?
The overall 5-year relative melanoma survival rate in the U.S. is approximately 93.3%, based on SEER 2021 data. However, this figure varies dramatically from near-perfect at Stage 0 to 35–52% at Stage IV with modern immunotherapy.
Q2: What is the melanoma survival rate for Stage 4 in 2026?
With checkpoint inhibitor therapy, the 5-year Stage 4 melanoma survival rate now ranges from 35% (standard data) to 52% (combination nivolumab + ipilimumab). This compares to just 15–20% in the pre-immunotherapy era before 2011. The AIM at Melanoma Foundation documents this transformation in its updated Stage IV prognosis section.
Q3: Can you survive Stage 3 melanoma?
Yes — and many patients do. Stage IIIA carries a 5-year survival rate of approximately 78%. Even Stage IIID, the most advanced regional stage, carries a ~40% rate — and that number is improving with adjuvant immunotherapy now being recommended for all Stage III substages.
Q4: Is any stage of melanoma truly incurable?
No stage of melanoma is automatically incurable. Even Stage IV patients can achieve complete and durable remission with checkpoint inhibitor combinations and TIL cell therapy. Long-term survivors of Stage IV melanoma now exist in significant numbers in clinical registry data.
Q5: How much does early detection improve melanoma survival?
Dramatically. Stage 0 melanoma detected before invasion carries a 99–100% 5-year survival rate. Delayed diagnosis to Stage IV drops this to 35%. Every stage of delay reduces survival odds — making annual skin checks and early reporting of melanoma warning signs the single most powerful intervention available.
Q6: How does BRAF mutation status affect melanoma survival rate?
Approximately 50% of melanomas carry the BRAF V600E mutation. For these patients, BRAF/MEK inhibitor combinations can rapidly reduce tumor burden and significantly improve Stage III–IV outcomes. BRAF testing should be performed at diagnosis for all patients with Stage III or IV disease.
Q7: Is melanoma survival rate different for men and women?
Yes. Women consistently show better 5-year melanoma survival rates than men at all stages, even after controlling for stage, depth, ulceration, and age. This advantage is most pronounced in patients under 55.
Q8: How accurate are melanoma survival statistics in 2026?
They are accurate as population-level historical data — but inherently lag current reality. Statistics reflect patients diagnosed 5–10 years ago. Patients diagnosed today, with access to TIL therapy and combination immunotherapy, may significantly outperform published survival figures.
Q9: What is the sentinel lymph node biopsy’s role in melanoma survival?
The sentinel lymph node biopsy (SLNB) determines whether melanoma has reached the regional lymph nodes — directly informing AJCC staging and, therefore, survival estimates. Our detailed guide on sentinel lymph node biopsy explains the procedure, interpretation, and what results mean for staging.
Q10: How does immunotherapy improve melanoma survival rate?
Combination immunotherapy (nivolumab + ipilimumab) achieved a 52% 5-year overall survival rate in the CheckMate 067 trial for metastatic melanoma. This compares to 26% with ipilimumab alone — nearly doubling survival odds through dual checkpoint blockade. The Melanoma Research Alliance provides updated immunotherapy-era survival data for all stages.
Q11: What is the melanoma survival rate for patients under 40?
Young adults under 40 consistently show better survival outcomes at all melanoma stages compared to older patients. Their immune systems respond more robustly to immunotherapy, and they are more likely to achieve complete remission at Stage III and early Stage IV.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.