
Under-50? 1 in 5 Now—Free Test Cuts Deaths 90%
Sarah Martinez celebrated her 34th birthday with persistent stomach cramps she blamed on stress. Six months later, she received a stage 3 colorectal cancer diagnosis that could have been prevented. Colorectal cancer now affects 1 in 5 people diagnosed before age 50—a staggering increase from 1 in 10 just fifteen years ago. The alarming truth: free at-home screening tests like the fecal immunochemical test (FIT) reduce colorectal cancer deaths by 33-40% when completed annually, yet 40% of eligible Americans according to the National Cancer Institute have never been screened.
Early onset colorectal cancer has become the silent epidemic devastating millennials and Gen Z adults. The U.S. Preventive Services Task Force now recommends screening starting at age 45 for average-risk individuals, reflecting this urgent demographic shift. Between 1992 and 2025, colorectal cancer rates in adults under 50 have doubled, with the steepest increases occurring in those aged 20-39 based on SEER cancer statistics tracking data.
The survival difference is staggering. When detected at stage 1 through routine screening, the five-year survival rate exceeds 92%. When diagnosed at stage 4 after symptoms appear, survival plummets to just 15%. Understanding your personal risk factors—from family history to metabolic conditions that affect your BMI Calculator results—empowers you to take preventive action today.
Free colorectal screening is now accessible to most Americans age 45 and older through Medicare coverage, Medicaid, and the Affordable Care Act’s preventive services mandate. No-cost options include annual FIT tests you complete at home, Cologuard DNA testing every three years, or colonoscopy every ten years. Research published in PubMed Central confirms that increased screening compliance could prevent an estimated 12,000 colorectal cancer deaths annually among younger adults.
What This Means For You:
- ✅ If you’re 45+: Order a free FIT test through your insurance or community health center—results in 7 days
- ✅ If you have symptoms: Blood in stool, persistent abdominal pain, or unexplained weight loss requires immediate evaluation with our Symptom Checker
- ✅ If you have family history: Screening should start at age 40 or 10 years before your youngest affected relative’s diagnosis age—assess your hereditary risk with the Genetic Risk Assessment Tool
Colorectal cancer deaths under 50 have increased by 11% in the past decade while declining in older adults due to widespread screening adoption. The message is clear: screening saves lives, and waiting for symptoms is waiting too long.
Disclaimer: This article provides educational information about colorectal cancer screening and is not a substitute for professional medical advice. Consult your healthcare provider for personalized recommendations.
The Rising Crisis – Why Young Adults Are at Risk
Why Colorectal Cancer Cases Have Doubled in Adults Under 50 Since 1992
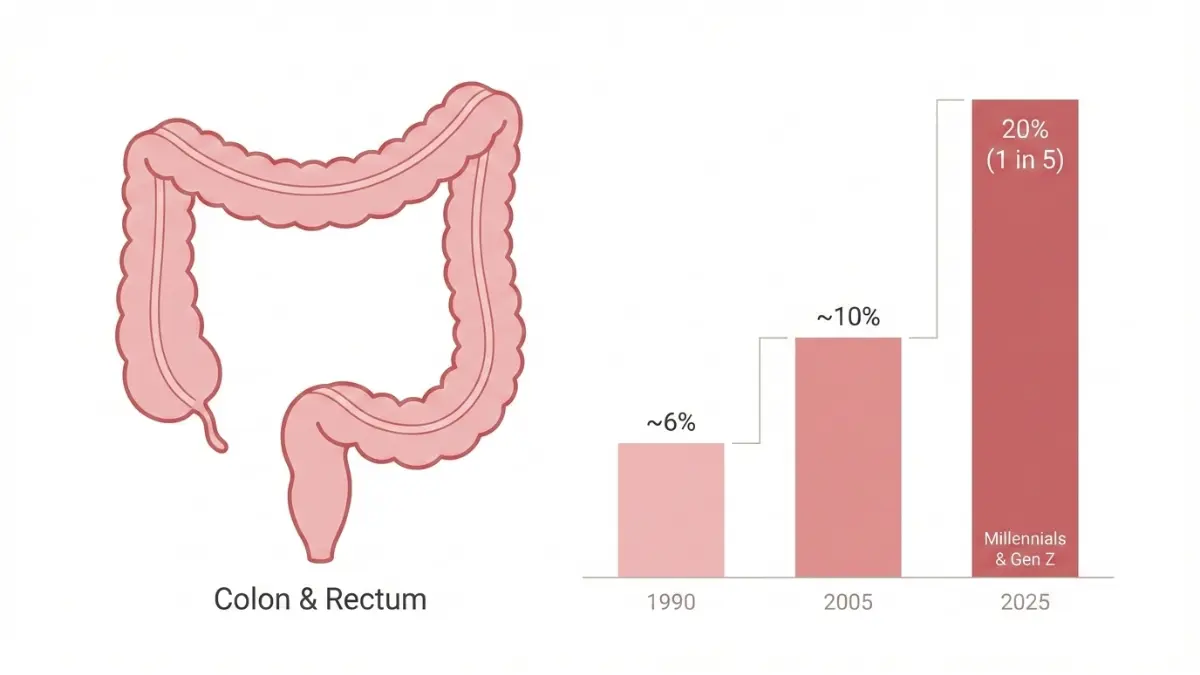
The rise of colorectal cancer under 50 represents one of the most alarming public health reversals of the 21st century. While screening has successfully reduced rates in older adults by 30% since 2000, incidence among those under age 50 has climbed steadily—now representing 20% of all new diagnoses. This demographic shift has prompted researchers to investigate what makes millennials and Gen Z uniquely vulnerable.
The Shocking Statistics: From 1 in 50 to 1 in 5 in Three Decades
In 1992, colorectal cancer diagnosed before age 50 was considered rare, accounting for just 6% of cases. Today, that figure has more than tripled. Adults born in 1990 face double the risk of colon cancer and quadruple the risk of rectal cancer compared to those born in 1950, according to American Cancer Society data. The steepest increases occur in the 20-39 age group, where rates have risen 2.4% annually since 2011.
| Birth Year | Colon Cancer Risk (vs 1950) | Rectal Cancer Risk (vs 1950) |
|---|---|---|
| 1950 | Baseline (1x) | Baseline (1x) |
| 1970 | 1.3x higher | 1.8x higher |
| 1990 | 2.0x higher | 4.0x higher |
| 2000+ | 2.4x higher | 4.6x higher (projected) |
Geographic disparities reveal troubling patterns. The Mississippi Delta, Appalachia, and parts of the rural Midwest show early onset colorectal cancer rates 40-60% higher than national averages. African Americans under 50 experience diagnosis rates 20% higher and mortality rates 40% higher than white Americans of the same age.
Early Onset Colorectal Cancer: Millennials and Gen Z at Higher Risk
The “birth cohort effect” explains why younger generations face disproportionate risk. Millennials and Gen Z grew up during the explosion of ultra-processed foods, sedentary screen-based lifestyles, and childhood obesity epidemic. By age 35, today’s adults have accumulated decades more exposure to dietary and environmental risk factors than previous generations encountered in their lifetimes.
Colorectal cancer millennials face unique challenges beyond incidence rates. Tumors in younger patients tend to be more aggressive, diagnosed at later stages, and located in the left colon or rectum rather than the right colon. The median age at diagnosis has dropped from 72 years in 2000 to 66 years in 2025, with the fastest growth occurring in the 45-49 age bracket.
Colon cancer Gen Z statistics project even more alarming trends. Current 20-year-olds may face lifetime colorectal cancer risk approaching 1 in 15 if incidence continues rising at current rates—comparable to the risk their grandparents faced in their 70s.
Risk Factors Hitting Younger Generations Harder
The convergence of multiple lifestyle and metabolic risk factors creates the perfect storm for early onset colorectal cancer. Understanding these modifiable risks empowers preventive action:
Diet-Related Risk Factors:
- Western diet pattern: High consumption of red meat (beef, pork, lamb) increases risk by 18% per 100g daily serving
- Processed meats: Hot dogs, bacon, deli meats raise risk by 16% per 50g daily serving
- Ultra-processed foods: Foods with added sugars, preservatives, and artificial ingredients now comprise 60% of American calorie intake
- Sugar-sweetened beverages: Two or more servings daily associated with 2x higher risk before age 50
- Low fiber intake: Less than 25g daily fiber intake increases risk by 40%
Metabolic and Lifestyle Factors:
- Obesity and metabolic syndrome: Adults with BMI over 30 face 30-50% higher colorectal cancer risk, with abdominal obesity particularly dangerous
- Sedentary behavior: Less than 150 minutes weekly physical activity increases risk by 30-40%
- Type 2 diabetes: Diabetics have 30-40% higher colorectal cancer risk and worse survival outcomes
- Alcohol consumption: More than 2 drinks daily increases risk by 20%, with binge drinking patterns common in younger adults showing stronger associations
Medical Warning Signs:
- Iron deficiency anemia colon cancer connection: Unexplained low hemoglobin and ferritin levels may indicate chronic intestinal bleeding months before visible symptoms appear
- Inflammatory bowel disease: Crohn’s disease and ulcerative colitis increase lifetime risk 2-3x, requiring earlier and more frequent screening
- Gut microbiome disruption: Antibiotic overuse, C. difficile infections, and dysbiosis alter intestinal environments in ways that may promote tumor development
The metabolic syndrome epidemic particularly impacts colorectal cancer risk factors in younger populations. The combination of elevated blood pressure, high blood sugar, excess abdominal fat, and abnormal cholesterol creates chronic inflammation that damages DNA and promotes cancer cell growth.
What This Data Means:
The rise in colorectal cancer under 50 is not inevitable. Most risk factors are modifiable through dietary changes, increased physical activity, weight management, and early screening. Young adults experiencing symptoms like bowel changes should advocate for prompt evaluation rather than accepting dismissive “you’re too young” responses from healthcare providers.
Symptoms You Can’t Ignore + When to Get Screened
Colorectal Cancer Symptoms in Young Adults: Early Warning Signs
Marcus Thompson, a 38-year-old software engineer, dismissed rectal bleeding for eight months as hemorrhoids before seeking medical attention. His stage 3 diagnosis could have been caught at stage 1 if he’d acted on the first symptom. Colorectal cancer symptoms young adults experience are often misattributed to less serious conditions, leading to dangerous delays averaging 4-6 months between first symptom and diagnosis.
The tragedy of early onset colorectal cancer lies in its detectability. Unlike pancreatic or ovarian cancer, colorectal tumors produce recognizable warning signs months before advancing to late stages. Yet young adults and their doctors frequently discount these symptoms due to age-related assumptions.
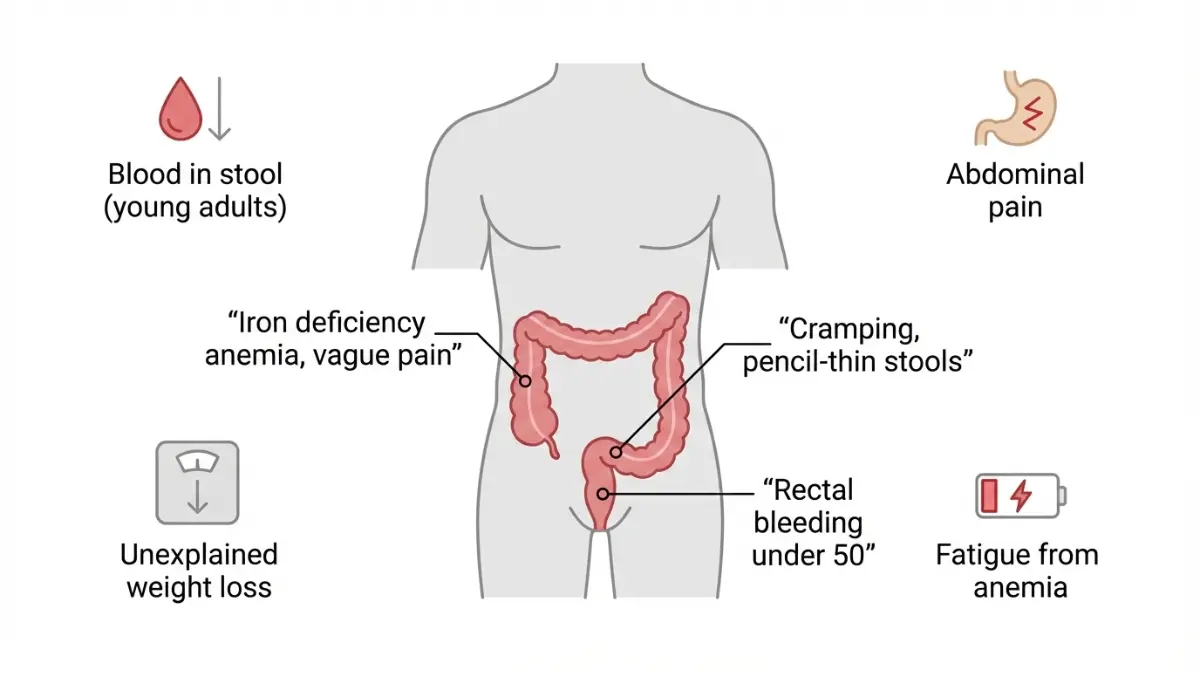
7 Symptoms That Demand Immediate Medical Attention
1. Rectal Bleeding Under 50
Visible blood in toilet water, on toilet paper, or coating stool represents the most common early warning sign. Bright red blood typically indicates lower colon or rectal sources, while dark, tarry stools suggest upper GI bleeding. The Centers for Disease Control reports that 45% of young adults with colorectal cancer experienced rectal bleeding as their first symptom, yet most delayed seeking care for 3+ months.
2. Blood in Stool Young Adults Often Ignore
Occult (hidden) blood detected only through fecal testing may precede visible bleeding by months. This microscopic bleeding causes progressive iron deficiency anemia colon cancer patients experience—symptoms include extreme fatigue, shortness of breath with minimal exertion, pale skin, and brittle nails. Annual FIT tests detect occult blood 79% of the time when cancer is present.
3. Persistent Abdominal Pain Cancer Indicators
Cramping, bloating, or sharp pain lasting more than two weeks warrants evaluation. Pain patterns vary by tumor location: right-sided colon cancers cause dull, constant aching; left-sided tumors produce cramping with bowel movements; rectal cancers trigger urgency and incomplete evacuation sensations. Pain that interferes with sleep or daily activities requires prompt investigation beyond symptom management.
4. Unexplained Weight Loss Exceeding 5% Body Weight
Unintentional weight loss of 10+ pounds over 3-6 months despite normal eating patterns signals metabolic disruption. Cancer cells consume significant energy and alter metabolism through inflammatory cytokine release. Track changes with an Ideal Weight Calculator to identify subtle but significant losses.
5. Iron Deficiency Anemia Colon Cancer Connection
Low hemoglobin and ferritin levels without obvious cause demand colonoscopy evaluation. Chronic intestinal bleeding depletes iron stores months before visible blood appears. Symptoms include crushing fatigue, difficulty concentrating, dizziness, cold hands/feet, and rapid heartbeat with exertion. Request complete blood count testing if unexplained fatigue persists beyond two weeks.
6. Changes in Bowel Habits Lasting 14+ Days
New-onset constipation, diarrhea, or alternating patterns indicate potential obstruction or inflammation. Pencil-thin stools suggest narrowing from tumor growth. The National Cancer Institute emphasizes that persistent changes—not occasional variations—require diagnostic evaluation through colonoscopy.
7. Persistent Fatigue and Weakness Beyond Normal Tiredness
Exhaustion that doesn’t improve with rest, interferes with work or social activities, or feels qualitatively different from typical tiredness may indicate anemia, metabolic disruption, or inflammatory burden. This symptom rarely occurs alone but compounds other warning signs like bleeding or pain.
Colon Cancer Screening Age 45: New Guidelines Explained
The U.S. Preventive Services Task Force updated colorectal cancer screening guidelines in 2021, lowering the starting age from 50 to 45 for average-risk adults. This change reflects the 51% increase in colorectal cancer under 50 cases between 1994 and 2019 documented in federal cancer surveillance data.
Current Colorectal Cancer Screening Guidelines:
| Risk Category | Start Age | Recommended Test | Frequency |
|---|---|---|---|
| Average risk | 45 | Colonoscopy OR FIT/Cologuard | 10 years OR annually/3 years |
| First-degree relative with CRC | 40 or 10 years before relative’s age | Colonoscopy | Every 5 years |
| Multiple affected relatives | 40 or 10 years before youngest case | Colonoscopy | Every 3-5 years |
| Lynch syndrome | 20-25 | Colonoscopy + genetic counseling | Every 1-2 years |
| Inflammatory bowel disease | 8 years after diagnosis | Colonoscopy | Every 1-3 years |
Colon cancer screening age 45 applies to individuals without symptoms or increased risk factors. Those experiencing warning signs require immediate diagnostic evaluation regardless of age—screening guidelines don’t apply when symptoms are present.
Who Needs Earlier Screening? High-Risk Groups
Colorectal Cancer Family History Criteria:
Genetic predisposition accounts for approximately 20-30% of colorectal cancers. First-degree relatives (parents, siblings, children) of colorectal cancer patients face 2-4x higher lifetime risk. The risk intensifies when relatives were diagnosed before age 60 or when multiple family members are affected.
Lynch syndrome represents the most common hereditary colorectal cancer syndrome, affecting 1 in 300 Americans. This genetic condition causes 70-80% lifetime colorectal cancer risk and significantly elevated risks for endometrial, ovarian, stomach, and other cancers. Genetic testing through the Genetic Risk Assessment Tool helps identify candidates for genetic counseling.
Lynch Syndrome Red Flags:
- Colorectal cancer diagnosed before age 50
- Multiple primary cancers in same individual
- Three or more relatives with Lynch-associated cancers
- Two successive generations affected
- Endometrial cancer before age 50
Inflammatory Bowel Disease Considerations:
Ulcerative colitis and Crohn’s disease patients face 2-3x elevated colorectal cancer risk after 8-10 years of disease activity. Chronic inflammation damages DNA and promotes cellular mutations over time. Surveillance colonoscopy every 1-3 years starting 8 years after diagnosis enables early detection before symptoms develop.
Symptom-Based Decision Making:
The presence of any persistent warning sign overrides age-based screening guidelines. A 28-year-old with rectal bleeding under 50 requires colonoscopy, not reassurance about being “too young.” Detailed symptom information appears in our comprehensive guide on colon cancer symptoms under 50.
When to Use Emergency Services:
Severe symptoms require immediate emergency department evaluation rather than waiting for scheduled appointments:
- Heavy rectal bleeding soaking through clothing
- Severe abdominal pain with fever
- Complete inability to pass stool or gas
- Vomiting blood or material resembling coffee grounds
- Confusion or fainting associated with bleeding
Free Screening Options – Tests That Save Lives
Free Colorectal Screening: How a $0 Test Reduces Deaths by 40%
Jennifer Park, a 47-year-old teacher without health insurance, discovered free colorectal screening through her local community health center. The at-home colon cancer test she received at no cost detected early-stage cancer that responded completely to treatment. Her story illustrates a critical reality: cost should never prevent life-saving screening.
Free colorectal screening has been federally mandated since 2010 under the Affordable Care Act’s preventive services provision. Most Americans age 45 and older qualify for zero-cost screening through Medicare, Medicaid, private insurance, or community programs—yet awareness remains dangerously low.
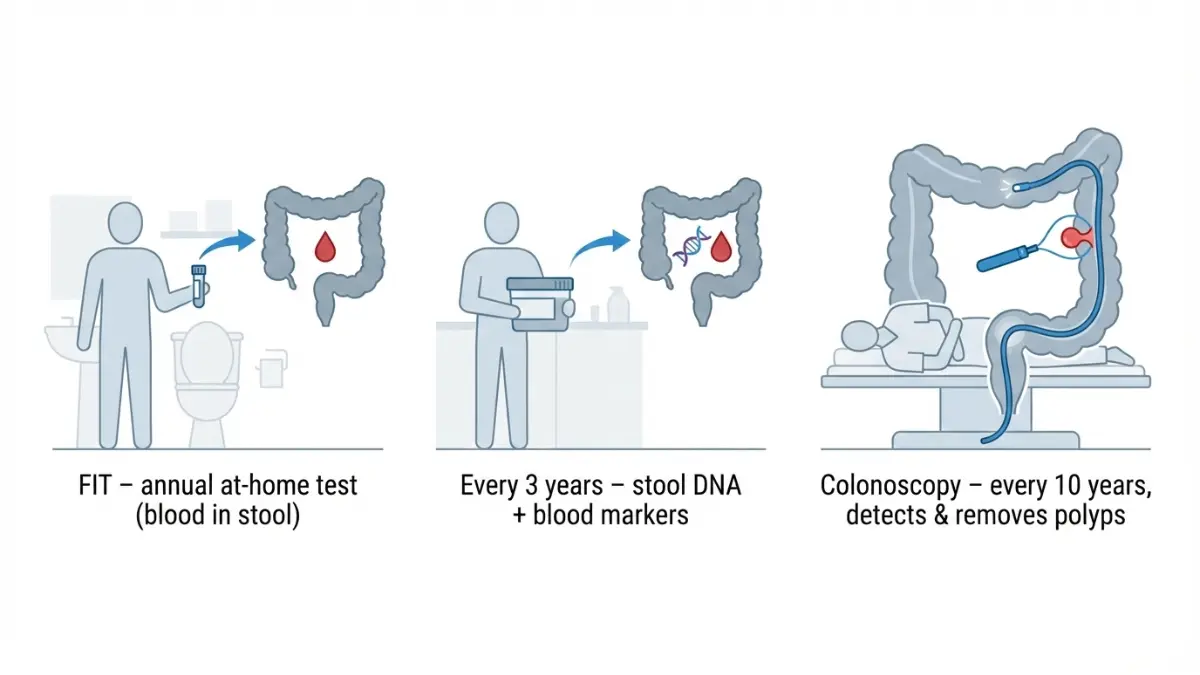
FIT Test vs Cologuard vs Colonoscopy: Complete Comparison
Understanding the differences between screening options enables informed decision-making based on individual preferences, risk factors, and circumstances. All three primary methods reduce colorectal cancer deaths when completed as recommended.
| Screening Test | Out-of-Pocket Cost (Uninsured) | Medicare/Medicaid Coverage | Frequency Needed | Sensitivity for Cancer | Preparation Required | Time Investment |
|---|---|---|---|---|---|---|
| FIT (Fecal Immunochemical Test) | $24-$35 | FREE (100% covered) | Annually | 79% for cancer, 24% for polyps | None – collect sample at home | 5 minutes |
| Cologuard (Stool DNA Test) | $649 | FREE (100% covered) | Every 3 years | 92% for cancer, 42% for polyps | None – collect sample at home | 15 minutes |
| Colonoscopy | $2,000-$3,500 | FREE (100% covered) | Every 10 years | 95% for cancer, 95% for polyps | Full bowel prep – 24 hours | 4-6 hours (prep, procedure, recovery) |
| Flexible Sigmoidoscopy | $600-$1,200 | FREE with insurance | Every 5 years | 70-80% (left colon only) | Enema prep – 2 hours | 2-3 hours |
| CT Colonography | $400-$800 | Variable – check coverage | Every 5 years | 90% for polyps 10mm+ | Full bowel prep – 24 hours | 3-4 hours |
Key Performance Differences:
The at-home colon cancer test options (FIT and Cologuard screening) offer convenience and eliminate procedural risks but require colonoscopy follow-up if results are positive. Approximately 5-10% of FIT tests and 10-15% of Cologuard tests return positive results, necessitating diagnostic colonoscopy.
Colonoscopy vs Cologuard comparison reveals distinct advantages for each. Colonoscopy simultaneously detects and removes precancerous polyps during a single procedure, providing both screening and prevention. Cologuard detects existing tumors and advanced adenomas but cannot remove polyps, requiring colonoscopy for any abnormal finding.
False-positive rates matter significantly. FIT produces false positives in 5-10% of tests, while Cologuard’s false-positive rate reaches 13%, meaning 1 in 8 positive results don’t indicate cancer or advanced polyps. These false positives lead to anxiety and unnecessary colonoscopies but represent the trade-off for convenient at-home testing.
How to Get Free Colorectal Cancer Screening (No Insurance Required)
Medicare Coverage (Age 45+):
Medicare Part B covers colorectal cancer screening with zero copayment, coinsurance, or deductible for beneficiaries age 45 and older. Covered services include annual FIT tests, Cologuard every three years, and colonoscopy every 10 years for average-risk individuals. High-risk individuals qualify for more frequent colonoscopy without cost-sharing.
Important distinction: screening colonoscopy remains free even if polyps are removed during the procedure. The 2022 policy change eliminated the previous loophole that converted screening procedures to diagnostic when polyps were found, potentially triggering cost-sharing.
Colorectal Screening Medicaid Coverage:
All state Medicaid programs cover colorectal cancer screening without cost-sharing as mandatory preventive services. Coverage includes FIT, Cologuard, and colonoscopy for eligible adults age 45-75. Medicaid expansion states provide broader eligibility, covering adults with incomes up to 138% of federal poverty level ($20,783 for individuals in 2025).
Private Insurance Under the Affordable Care Act:
The ACA requires all private insurance plans to cover colorectal cancer screening without copayments, coinsurance, or deductibles for adults age 45-75. This mandate applies to both marketplace plans and employer-sponsored insurance. If your insurer charges for routine screening, file an appeal—the coverage is legally guaranteed.
Free Cancer Screening Near Me – Community Resources:
Colorectal screening without insurance remains accessible through multiple programs:
- Federally Qualified Health Centers (FQHCs): Over 1,400 community health centers nationwide provide free or sliding-scale colorectal screening based on income
- CDC’s Colorectal Cancer Control Program: Operates in 24 states, providing free screening to low-income uninsured adults age 50-64
- Local health departments: Many offer free FIT test distribution and colonoscopy referrals
- Hospital charity care programs: Nonprofit hospitals must provide free or discounted care to qualifying low-income patients under IRS requirements
- Pharmaceutical patient assistance: Some programs cover Cologuard costs for uninsured individuals
At-Home Colon Cancer Test: Which One Is Right for You?
FIT Test Advantages:
The fecal immunochemical test detects hidden blood in stool using antibodies specific to human hemoglobin. Unlike older guaiac-based tests, FIT doesn’t require dietary restrictions or medication adjustments before testing. The test detects approximately 79% of colorectal cancers and 24% of advanced adenomas (precancerous polyps).
Annual FIT testing provides cumulative benefit. Completing FIT every year for 10 consecutive years approaches colonoscopy’s effectiveness for cancer detection, though it misses many polyps that colonoscopy would remove before they become cancerous.
Cologuard Screening Advantages:
Cologuard combines FIT technology with DNA mutation analysis to detect both blood and abnormal cells in stool. The enhanced detection identifies 92% of cancers and 42% of advanced adenomas—substantially better than FIT alone. The three-year testing interval offers convenience for those who prefer less frequent screening.
Cologuard works best for average-risk individuals without symptoms. The test is not appropriate for those with personal history of colorectal cancer, inflammatory bowel disease, or certain hereditary syndromes.
When to Choose Colonoscopy:
Certain situations favor colonoscopy over at-home testing:
- Family history: First-degree relative with colorectal cancer warrants colonoscopy starting at age 40
- Symptom presence: Blood in stool, persistent bowel changes, or abdominal pain requires diagnostic colonoscopy, not screening tests
- Previous polyps: Personal history of adenomas necessitates surveillance colonoscopy every 3-5 years
- Genetic syndromes: Lynch syndrome and familial adenomatous polyposis demand colonoscopy every 1-2 years
- Inflammatory bowel disease: Crohn’s disease or ulcerative colitis requires colonoscopy surveillance
Colonoscopy Cost Breakdown: What to Expect Without Insurance
Understanding colonoscopy cost components helps uninsured individuals plan and negotiate:
Facility Fee: $1,200-$2,000
- Hospital outpatient departments charge significantly more than ambulatory surgery centers
- Negotiating cash-pay discounts can reduce facility fees 30-50%
Physician Fee (Gastroenterologist): $400-$800
- Includes procedure performance and pathology interpretation
- Some practices offer self-pay discounts if paid in advance
Anesthesia Fee: $300-$600
- Depends on procedure duration and anesthesia type
- Conscious sedation costs less than general anesthesia
Pathology Fee (if polyps removed): $150-$400 per specimen
- Multiple polyps multiply pathology costs
- Some labs offer bundled pricing
Total Uninsured Cost: $2,000-$3,500 typical range
Cost-Saving Strategies:
- Ambulatory surgery centers cost 40-60% less than hospitals
- Self-pay discounts average 30-40% when negotiated upfront
- Payment plans spread costs over 6-24 months interest-free at many facilities
- Medical credit cards (CareCredit, AccessOne) offer promotional zero-interest periods
- Hospital financial assistance policies provide free or discounted care based on income—nonprofit hospitals must offer charity care to qualify for tax-exempt status
What This Section Means:
No American should develop preventable colorectal cancer due to cost barriers. Free screening is legally guaranteed for most adults through insurance mandates, and community resources provide access for the uninsured. The test that saves your life is the one you actually complete—whether that’s a $0 FIT test at home or a free colonoscopy at a community health center.
Treatment Breakthroughs + Survival Rates in 2025
Colorectal Cancer Treatment Cost and Breakthrough Immunotherapy Options
David Chen received his stage 3 colorectal cancer diagnosis at age 42 in 2023. After surgery and chemotherapy, his cancer returned in 2024 with liver metastases. Genetic testing revealed his tumor had microsatellite instability-high (MSI-H) status, making him eligible for FDA approved immunotherapy colon cancer treatment with nivolumab plus ipilimumab. Eighteen months later, his scans show no evidence of disease—a outcome impossible just five years ago for his cancer subtype.
Early detection colon cancer transforms survival from dire to exceptional. The difference between stage 1 and stage 4 diagnosis represents not just percentage points but years of life and quality of living.
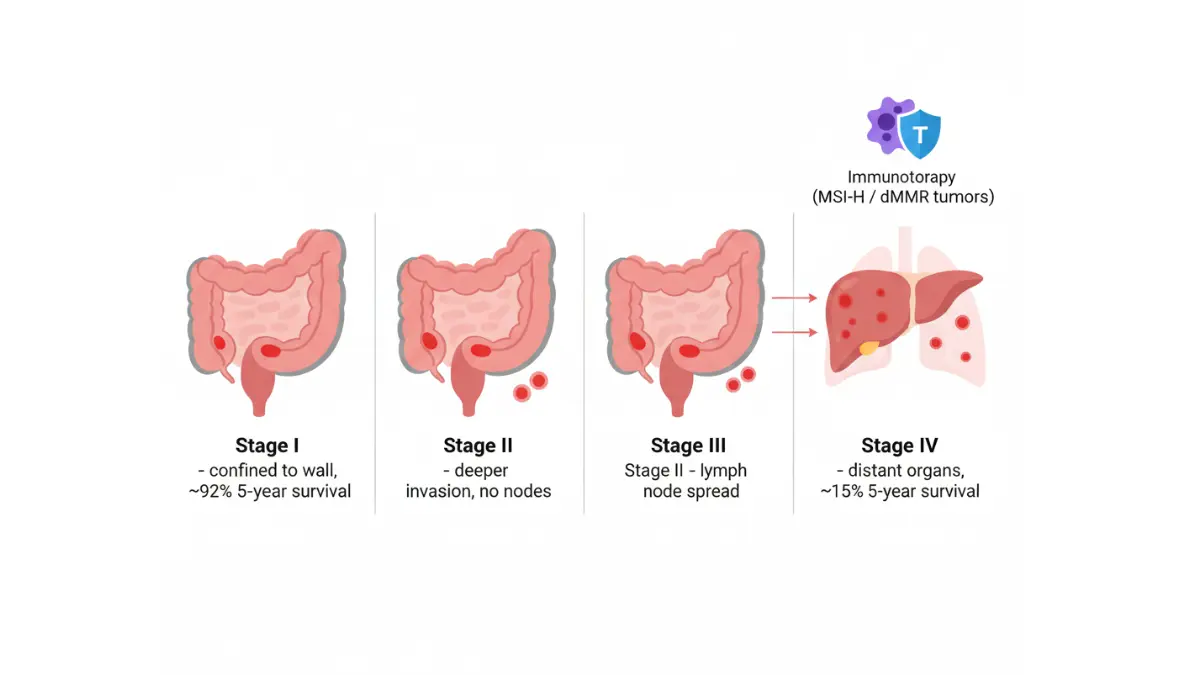
Colorectal Cancer Survival Rate: Early Detection Changes Everything
Stage at diagnosis determines survival more than any other factor. Colorectal tumors detected through screening when confined to the intestinal wall achieve cure rates exceeding 90%. Once cancer spreads beyond regional lymph nodes to distant organs, five-year survival plummets to 15%.
| Stage at Diagnosis | Tumor Extent | 5-Year Survival Rate (With Treatment) | Median Survival Without Treatment |
|---|---|---|---|
| Stage I | Limited to inner colon/rectal wall | 92% | 12-18 months |
| Stage II | Grown through wall, no lymph node spread | 87% | 8-12 months |
| Stage III | Spread to regional lymph nodes | 72% | 6-10 months |
| Stage IV | Metastases to liver, lungs, or other organs | 15% | 3-6 months |
| Stage IV (oligometastatic) | 1-3 resectable metastases | 40-50% | Variable |
Critical Context for Young Adults:
Colorectal cancer under 50 presents with unique patterns affecting survival outcomes. Younger patients more frequently develop left-sided colon and rectal cancers, which tend to be more aggressive but also more responsive to modern chemotherapy combinations. The median age of death from colorectal cancer has decreased from 73 in 2000 to 68 in 2025, reflecting rising mortality among 45-54 year-olds.
Stage migration explains some survival improvements. Better imaging technology (PET-CT, MRI) detects metastases missed by older methods, “upstaging” patients who would have been classified as earlier stage decades ago. This technical improvement inflates apparent survival rates for early stages while deflating rates for late stages.
Real Patient Survival Timeline (Stage III Example):
- Month 0: Diagnosis following colonoscopy for rectal bleeding
- Month 1: Surgery (colectomy) removes primary tumor and 18 lymph nodes (6 positive)
- Month 2-8: FOLFOX chemotherapy (12 cycles over 6 months)
- Month 9-60: Surveillance with CEA blood tests every 3 months, CT scans every 6 months
- 5-Year Mark: No recurrence detected—considered “cured” with 72% probability
FDA-Approved Immunotherapy Colon Cancer: 2025 Game-Changers
Colorectal cancer immunotherapy has revolutionized treatment for specific genetic subtypes. Approximately 15% of colorectal cancers exhibit microsatellite instability-high (MSI-H) or mismatch repair deficient (dMMR) status, making them highly responsive to immune checkpoint inhibitors.
2025 FDA Approvals – Breakthrough Treatments:
Nivolumab + Ipilimumab (Opdivo + Yervoy) Combination:
- Approved May 2025 for first-line treatment of MSI-H/dMMR metastatic colorectal cancer
- CheckMate-8HW trial results: 79% response rate vs 59% with chemotherapy
- Median progression-free survival not yet reached (>24 months) vs 8.3 months with chemotherapy
- Severe side effects in 23% (vs 45% with chemotherapy)
Pembrolizumab (Keytruda) Monotherapy:
- Confirmed accelerated approval for MSI-H/dMMR advanced colorectal cancer after any prior treatment
- KEYNOTE-177 five-year data: 49% alive without progression on immunotherapy vs 7% on chemotherapy
- Quality of life substantially better than chemotherapy due to fewer side effects
Dostarlimab (Jemperli) Breakthrough:
- 2025 approval for MSI-H rectal cancer based on unprecedented clinical trial
- 100% complete response rate in initial 18 patients—all tumors disappeared without surgery or radiation
- Long-term follow-up shows sustained remission at 2+ years in 94% of patients
Who Qualifies for Colorectal Cancer Breakthrough Treatments:
Genetic testing determines immunotherapy eligibility. MSI-H/dMMR status results from inherited Lynch syndrome (3-5% of cases) or sporadic mutations (10-12% of cases). Right-sided colon cancers exhibit MSI-H status more frequently than left-sided or rectal cancers.
Testing recommendations:
- All colorectal cancers should undergo MSI/MMR testing at diagnosis
- Universal testing costs $200-$500 but guides treatment decisions worth $200,000+
- Results available within 5-7 business days from tumor biopsy
Insurance Coverage Reality:
Medicare and most private insurers cover FDA approved immunotherapy colon cancer treatments for appropriate indications. Out-of-pocket costs range from $0 (for Medicare/Medicaid) to $3,000-$8,000 annual maximum for private insurance with out-of-pocket caps. Manufacturer patient assistance programs provide immunotherapy at reduced or zero cost for uninsured patients meeting income criteria.
Stage 4 Colorectal Cancer Treatment: New Hope for Advanced Disease
Advanced stage colorectal cancer treatment has evolved from purely palliative to potentially curative in select cases. Oligometastatic disease—limited metastases to 1-5 sites, typically liver or lung—may be curable with aggressive multimodal therapy combining chemotherapy, targeted agents, surgical resection, and ablation.
Modern Treatment Approaches:
Resectable Metastatic Disease:
- Chemotherapy (4-6 months) shrinks tumors → Surgery removes primary tumor and metastases → Additional chemotherapy (3-6 months)
- Five-year survival: 40-50% for completely resected liver/lung metastases
- Repeat resection possible for isolated recurrences
Unresectable Initially, Conversion Therapy:
- Aggressive chemotherapy + targeted therapy (bevacizumab or cetuximab/panitumumab based on RAS/BRAF status)
- 20-30% of initially unresectable metastases become resectable after tumor shrinkage
- Conversion to resectable disease associated with median survival exceeding 5 years
Unresectable Permanently:
- Chemotherapy extends median survival to 24-30 months (vs 6 months untreated)
- Sequential chemotherapy regimens (FOLFOX → FOLFIRI → regorafenib) maintain disease control
- Immunotherapy for MSI-H tumors achieves durable remissions in 40-50%
Colon Cancer Treatment Cost Breakdown:
| Treatment Component | Typical Cost Range | Insurance Coverage |
|---|---|---|
| Surgery (colectomy, lymph node removal) | $20,000-$50,000 | 80-100% after deductible |
| Chemotherapy (6 months FOLFOX) | $30,000-$100,000 | 80-100% after deductible |
| Targeted therapy (bevacizumab, 6 months) | $50,000-$80,000 | 80-100% after deductible |
| Immunotherapy (pembrolizumab, 12 months) | $180,000-$220,000 | 80-100% after deductible |
| Radiation therapy (rectal cancer, 6 weeks) | $15,000-$50,000 | 80-100% after deductible |
| Metastasis surgery (liver/lung resection) | $40,000-$100,000 | 80-100% after deductible |
| Total for Stage IV (first year) | $200,000-$400,000 | Variable by plan |
Patient Out-of-Pocket Reality:
Most insured patients with advanced colorectal cancer hit annual out-of-pocket maximums ($9,450 for individuals, $18,900 for families in 2025) within the first 2-3 months of treatment. Subsequent care throughout the year incurs no additional cost-sharing. Uninsured patients face catastrophic costs but may qualify for hospital charity care, pharmaceutical assistance programs, and clinical trials providing free experimental treatments.
What These Advances Mean:
The survival gap between early and late-stage colorectal cancer remains massive, but closing gradually. Immunotherapy transforms outcomes for MSI-H tumors regardless of stage. Aggressive surgical approaches combined with modern chemotherapy extend survival in stage 4 disease from months to years. Yet screening remains 1000x more cost-effective than treating advanced cancer—prevention beats even the best treatments.
Colon Cancer Prevention: Evidence-Based Steps to Reduce Your Risk
Emma Rodriguez, 39, watched her mother battle colorectal cancer at 58. Determined to change her trajectory, Emma adopted an intensive colon cancer prevention strategy combining dietary overhaul, regular exercise, and early screening starting at age 35. Eight years later, her colonoscopy revealed three small polyps—precancerous growths removed before they could transform into cancer. Her story illustrates a fundamental truth: most colorectal cancers are preventable through modifiable lifestyle choices and timely screening.
The American Institute for Cancer Research estimates that 47% of colorectal cancer cases could be prevented through healthy weight maintenance, physical activity, proper nutrition, and limited alcohol consumption. Combining these lifestyle interventions with screening starting at age 45 could prevent up to 70% of colorectal cancer deaths in the population.
8 Lifestyle Changes That Lower Colorectal Cancer Risk by 40%
1. Maintain Healthy Weight (BMI 18.5-24.9)
Obesity increases colorectal cancer risk by 30-50%, with abdominal fat posing particular danger. Excess weight promotes insulin resistance, chronic inflammation, and altered hormone levels that fuel cancer development. Use a Weight Loss Calculator to establish realistic goals—losing just 5-10% of body weight significantly reduces cancer risk even if you don’t reach ideal BMI.
2. Exercise 150+ Minutes Weekly
The National Cancer Institute confirms that regular physical activity reduces colorectal cancer risk by 20-30%. Moderate-intensity exercise (brisk walking, cycling, swimming) for 30 minutes five days weekly meets minimum recommendations. Vigorous activity provides even greater protection—track your cardiovascular fitness with a Pace Calculator to optimize your running or walking routine for maximum cancer prevention benefit.
3. Adopt Mediterranean or Plant-Forward Diet Pattern
Diets high in vegetables, fruits, whole grains, legumes, and fish while limiting red meat protect against colorectal cancer through multiple mechanisms—fiber promotes healthy gut bacteria, antioxidants neutralize DNA-damaging compounds, and anti-inflammatory omega-3 fatty acids suppress tumor promotion. Calculate optimal macronutrient ratios to ensure adequate protein intake while emphasizing plant-based sources like beans, lentils, and tofu.
4. Limit Red Meat to <18 Ounces Weekly
Evidence from the World Cancer Research Fund demonstrates that consuming more than 18 ounces of red meat weekly increases colorectal cancer risk by 12-17%. Beef, pork, and lamb contain heme iron and compounds formed during high-temperature cooking that damage intestinal DNA. Replace red meat with poultry, fish, or plant proteins at least 4-5 meals weekly.
5. Eliminate Processed Meats Completely
Hot dogs, bacon, sausage, deli meats, and other processed meats increase colorectal cancer risk by 16% per 50-gram daily serving. Nitrites used for preservation convert to carcinogenic N-nitroso compounds in the digestive tract. No safe consumption level exists—elimination provides maximum protection.
6. Limit Alcohol to <7 Drinks Weekly
Alcohol metabolism produces acetaldehyde, a DNA-damaging compound that promotes colorectal tumor development. Men consuming 2+ drinks daily and women consuming 1+ drink daily face 20% higher colorectal cancer risk than non-drinkers. If you drink, limit intake to 7 drinks weekly maximum, with several alcohol-free days.
7. Increase Fiber to 30+ Grams Daily
Dietary fiber accelerates transit time, dilutes potential carcinogens, and feeds beneficial gut bacteria producing protective short-chain fatty acids. Americans average just 15 grams daily—doubling intake to 30+ grams reduces colorectal cancer risk by 10-20%. Focus on whole grains, beans, vegetables, and fruits rather than isolated fiber supplements.
8. Ensure Adequate Calcium and Vitamin D
Calcium (1,200mg daily) and vitamin D (1,000-2,000 IU daily) work synergistically to suppress abnormal cell growth in colon tissue. Dairy products, fortified plant milks, leafy greens, and fatty fish provide these nutrients. Supplementation may be necessary in northern climates or for those with limited sun exposure.
Your Personalized Screening Schedule: When to Start
Action trumps information—knowing your screening schedule matters only if you follow through. Use this decision matrix to determine your personal timeline.
| Your Situation | Start Screening At | Test Type | Frequency | Next Steps |
|---|---|---|---|---|
| Age 45+, no symptoms, average risk | Age 45 | FIT test OR colonoscopy | Annually OR every 10 years | Order FIT online or schedule colonoscopy |
| Age 40+, parent/sibling had CRC | Age 40 OR 10 years before relative’s diagnosis age | Colonoscopy | Every 5 years | Consult gastroenterologist, genetic counseling if relative diagnosed <50 |
| Any age with symptoms | Immediately regardless of age | Diagnostic colonoscopy | As needed | Schedule within 2 weeks, don’t wait |
| Lynch syndrome diagnosed | Age 20-25 | Colonoscopy + genetic counseling | Every 1-2 years | Register with Lynch syndrome clinical program |
| IBD for 8+ years | 8 years after diagnosis | Colonoscopy with extensive biopsies | Every 1-3 years based on inflammation | Coordinate with gastroenterologist managing IBD |
| Previous adenomas found | Follow physician recommendation | Colonoscopy | Every 3-5 years based on polyp characteristics | Surveillance colonoscopy more important than initial screening |
Understanding Colorectal Cancer Genetic Testing:
Lynch syndrome and other hereditary colorectal cancer syndromes account for 5-10% of cases. Genetic testing costs $200-$3,000 but identifies family members needing intensive surveillance. Consider genetic counseling if:
- You or close relative diagnosed with colorectal cancer before age 50
- Multiple relatives across generations affected by colorectal, endometrial, ovarian, or stomach cancers
- You have 10+ colon polyps
- Personal history of both colorectal and endometrial cancer
Immediate Action Plan – What to Do Today:
✅ If you’re 45+ and haven’t screened: Call your insurance for free FIT test or colonoscopy coverage—complete this week
✅ If you have symptoms: Schedule colonoscopy within 14 days, not FIT test—symptoms require diagnostic evaluation
✅ If you have family history: Contact gastroenterology for early screening—don’t wait until age 45
✅ Calculate your personal risks: Use Body Fat Calculator to assess metabolic health, which connects to colorectal cancer risk through insulin resistance pathways
✅ Optimize nutrition foundation: Calculate your protein intake needs to ensure adequate nutrition during dietary shifts toward plant-based eating patterns
✅ Support overall cancer prevention: Explore evidence-based strategies in our comprehensive guide on preventing heart disease, since cardiovascular and cancer prevention share common lifestyle foundations
Colorectal cancer statistics 2025 paint a concerning picture for adults under 50, with 1 in 5 cases now occurring before age 50. Yet this cancer remains one of the most preventable and treatable when caught early. Free screening eliminates cost barriers. Evidence-based lifestyle modifications reduce risk by 40-50%. Breakthrough immunotherapy provides hope even for advanced disease. The only failure is inaction—screening saves lives, and today is the day to start.
Frequently Asked Questions About Colorectal Cancer Under 50
1. What does “1 in 5” colorectal cancer cases mean?
1 in 5 (20%) of all new colorectal cancer diagnoses now occur in people under age 50, up from 1 in 10 just 15 years ago. This represents a doubling of early-onset cases since the 1990s.
2. At what age should I start colorectal cancer screening?
Age 45 for average-risk individuals. Start at age 40 or 10 years before your youngest relative’s diagnosis age if you have a family history. Start immediately at any age if you have symptoms like rectal bleeding or persistent abdominal pain.
3. Is colorectal cancer screening really free?
Yes. Medicare, Medicaid, and all private insurance plans must cover colorectal screening (FIT test, Cologuard, or colonoscopy) with zero copay or deductible for adults age 45-75 under the Affordable Care Act.
4. What are the early warning signs of colon cancer in young adults?
Rectal bleeding, blood in stool, persistent abdominal pain lasting 2+ weeks, unexplained weight loss over 10 pounds, changes in bowel habits, pencil-thin stools, and extreme fatigue from iron deficiency anemia.
5. Can colorectal cancer be cured if caught early?
Yes. Stage 1 colorectal cancer has a 92% five-year survival rate when detected through screening. Early detection through colonoscopy allows removal of precancerous polyps before they become cancer.
6. How much does colonoscopy cost without insurance?
$2,000-$3,500 for self-pay patients, including facility fees ($1,200-$2,000), physician fees ($400-$800), anesthesia ($300-$600), and pathology if polyps are removed ($150-$400). Ambulatory surgery centers cost 40-60% less than hospitals.
7. What’s the difference between FIT test and Cologuard?
FIT detects hidden blood in stool (79% cancer detection, done annually, costs $24). Cologuard detects blood plus abnormal DNA (92% cancer detection, done every 3 years, costs $649). Both are free with insurance and require colonoscopy if positive.
8. What causes colorectal cancer in people under 50?
Combination of obesity, Western diet high in processed/red meat, sedentary lifestyle, alcohol consumption, gut microbiome changes, and possible environmental exposures. Family history and genetic syndromes (Lynch syndrome) account for 20-30% of cases.
9. Can lifestyle changes really prevent colon cancer?
Yes. Maintaining healthy weight, exercising 150+ minutes weekly, eating high-fiber Mediterranean diet, limiting red meat to under 18 oz/week, eliminating processed meats, and limiting alcohol reduces colorectal cancer risk by 40-47%.
10. What is Lynch syndrome and should I get tested?
Lynch syndrome is the most common hereditary colorectal cancer syndrome (1 in 300 Americans), causing 70-80% lifetime cancer risk. Get tested if you or close relatives had colorectal cancer before age 50, or multiple family members across generations had colorectal, endometrial, ovarian, or stomach cancers.
11. What are the new immunotherapy treatments for colorectal cancer?
FDA-approved immunotherapy drugs (nivolumab plus ipilimumab, pembrolizumab, dostarlimab) work for 15% of colorectal cancers with MSI-H/dMMR genetic status. These treatments achieve 79-92% response rates with fewer side effects than chemotherapy, and in some cases cause complete tumor disappearance.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.











