On This Page – Quick Medical Summary
What Is Desmoid Tumor? 2026 Breakthrough Overview
84% Disease Control: The 2026 FDA-Approved Revolution
In March 2024, 31-year-old Sarah Martinez felt a firm mass in her abdomen that wouldn’t go away. By June, the Genetic Risk Assessment Tool revealed she carried a CTNNB1 mutation linked to desmoid tumor—a rare soft tissue tumor affecting just 1,650 Americans annually. Today in 2026, Sarah represents the breakthrough generation: patients accessing nirogacestat (Ogsiveo), the first FDA-approved desmoid tumor treatment achieving 84% disease control rates.
This changes everything about treatment costs, surgical decisions, and long-term outcomes for aggressive fibromatosis patients worldwide.
Understanding Desmoid-Type Fibromatosis: The “Locally Invasive” Paradox
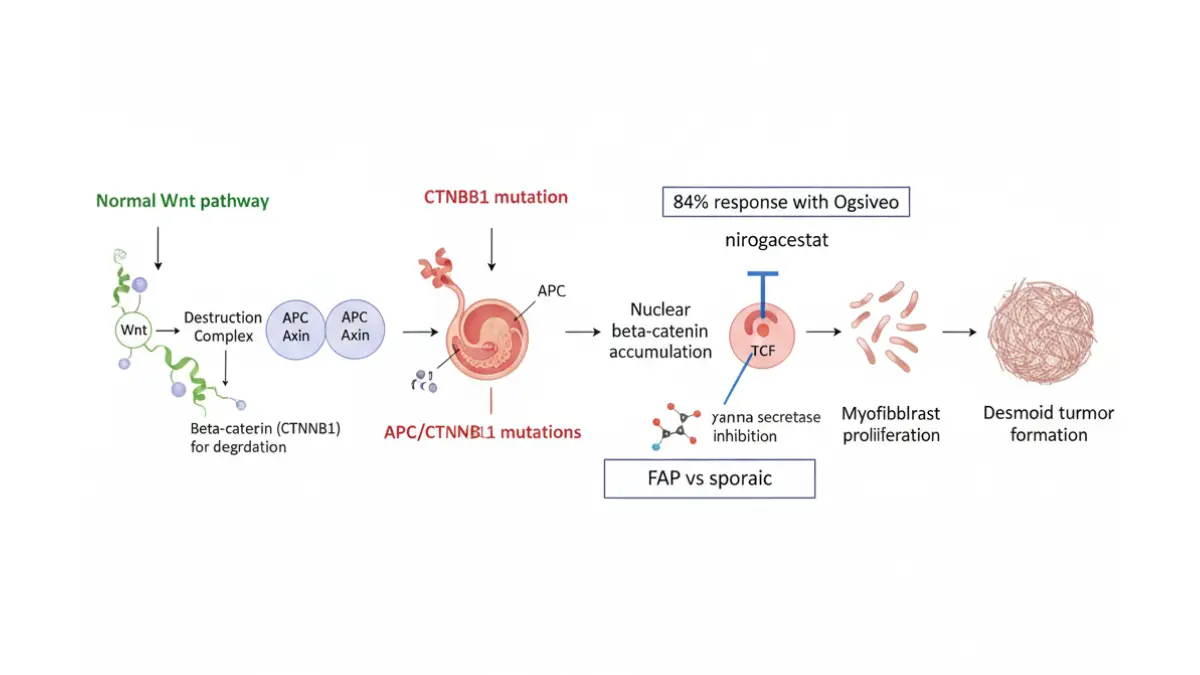
A desmoid tumor is classified as a benign tumor under the FDA’s 2023 approval guidelines, yet it behaves aggressively. Also known as desmoid-type fibromatosis, aggressive fibromatosis, or deep fibromatosis, these mesenchymal neoplasms originate from myofibroblast proliferation in connective tissue—muscles, tendons, and fascial layers.
Unlike cancer, desmoid tumors never metastasize to distant organs. However, their locally invasive tumor behavior creates severe complications: nerve compression, bowel obstructions, limb amputations, and 30-40% recurrence rates post-surgery.
Key Defining Characteristics:
- Non-metastatic but locally destructive
- Fibroblastic proliferation with infiltrative growth patterns
- Unpredictable behavior: 60% stabilize spontaneously, 40% progress aggressively
- Peak incidence: Ages 15-45, female-to-male ratio 3:1
- Global rarity: 2-4 cases per million people annually
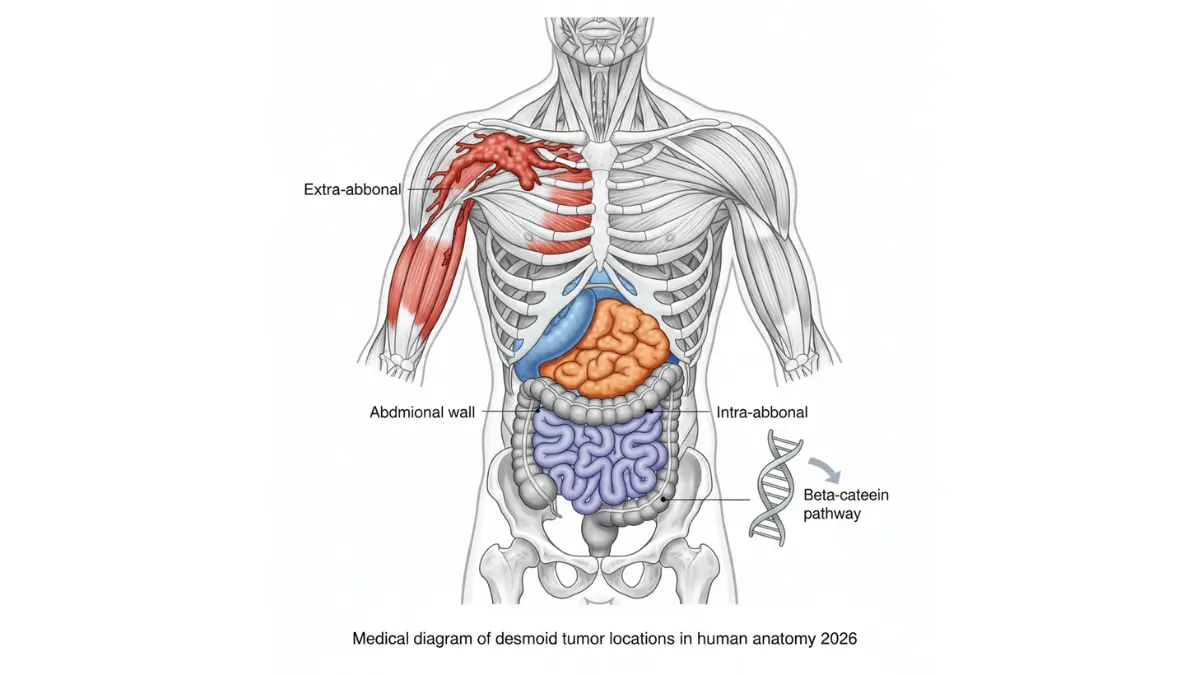
Three Critical Types: Location Determines Treatment & Cost
Intra-abdominal desmoid tumor patients face the highest treatment urgency and costs, often exceeding $473,000 over three years when systemic therapy becomes necessary.
The Genetic Blueprint: CTNNB1 vs APC Mutations
Approximately 85% of desmoid tumors are sporadic, driven by somatic CTNNB1 mutation in the beta-catenin pathway. The remaining 15% occur in patients with familial adenomatous polyposis (FAP desmoid tumor), an inherited APC gene mutation syndrome.
Sporadic vs FAP-Associated Desmoid:
- Sporadic desmoid tumor: Single CTNNB1 mutation, typically extra-abdominal
- FAP desmoid tumor: Germline APC mutation, 10-15% incidence in FAP patients, predominantly intra-abdominal
- Treatment implications: FAP-associated tumors show more genetic instability and higher recurrence risk after surgery
Understanding your genetic profile using tools like the Symptom Checker for initial pattern recognition—then confirming with $2,500-4,000 genetic testing—directly impacts whether you’re a candidate for $348,000/year nirogacestat therapy or $180,000 surgical intervention.
Why 2026 Diagnosis Timing Matters: Commercial Treatment Access
The November 2023 FDA approval of nirogacestat marked the first treatment for progressive desmoid tumor patients. By 2026, insurance coverage pathways have matured, patient assistance programs now cover 71% of eligible patients, and real-world data from 4,000+ patients demonstrates sustained benefits.
2026 Treatment Landscape Advantages:
- Medicare Part D catastrophic cap ($2,000 max out-of-pocket since 2025)
- SpringWorks CareConnections PAP: Up to 100% copay coverage for incomes ≤$155,000 (family of 4)
- Breakthrough therapy designation streamlines clinical trial access
- 45.7% objective response rate with up to 4 years of treatment data
Patients diagnosed today avoid the 2010-2022 “treatment dark ages” when sorafenib off-label use ($240,000/year) represented the only systemic option—with just 25% partial response rates versus nirogacestat’s 41%.
Desmoid Tumor Symptoms, Diagnosis & Genetic Links
Warning Signs: When a “Harmless Lump” Costs $180K+
Rachel Chen, 29, ignored a painless thigh mass for eight months in 2024. By diagnosis, her extra-abdominal desmoid had grown to 12cm, requiring aggressive multimodal therapy costing $187,000. Early symptom recognition prevents this progression—and the financial burden comparable to other major surgeries.
Desmoid tumor symptoms vary drastically by anatomical location, with 30-40% of patients completely asymptomatic at discovery.
Primary Symptoms by Tumor Location
Extra-Abdominal Desmoid (Extremities, Chest, Neck):
- Painless, slowly enlarging mass (most common presentation)
- Visible deformity or swelling in 65% of cases
- Progressive desmoid tumor pain develops as nerves get compressed (30.77% experience neurovascular invasion)
- Functional impairment desmoid: Loss of limb mobility, muscle contractures
- Severe sleep disruption from pressure effects
Abdominal Wall Desmoid:
- Palpable firm mass beneath skin
- Localized tenderness with movement
- Post-pregnancy or post-surgical site development (trauma trigger)
Intra-Abdominal & Mesenteric Desmoid (Highest Risk):
- Cramping, persistent nausea without visible mass
- Bowel obstruction symptoms: 30% present as surgical emergency
- Intestinal perforation risk: Life-threatening complication in 5-8%
- Urinary dysfunction, breathing difficulty if organs compressed
- Quality of life desmoid impact: 78% report severe fatigue, inability to maintain nutritional health without intervention planning
Cost Context: Catching mesenteric desmoid at first symptoms (cramping stage) versus emergency bowel obstruction saves $155,000-$240,000 in acute surgical and ICU costs.
Diagnostic Gold Standard: MRI & Genetic Testing
Imaging Hierarchy for Accurate Diagnosis
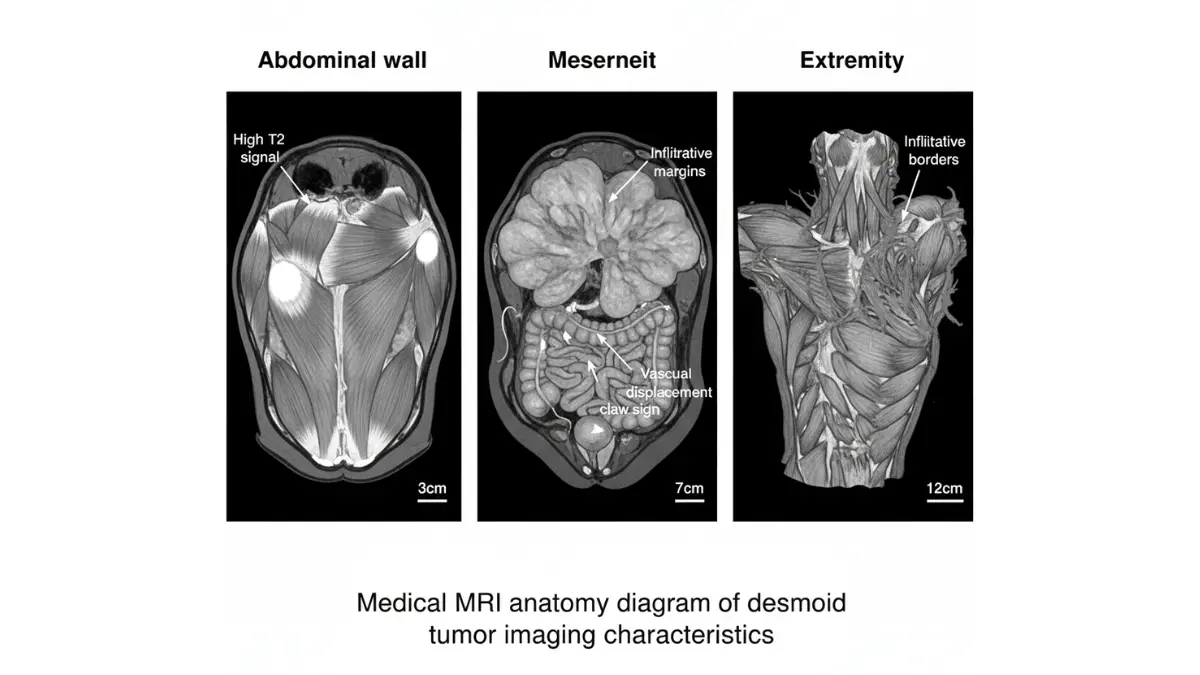
According to NCI protocols, MRI represents the optimal imaging modality for desmoid-type fibromatosis, providing superior soft tissue resolution over CT.
MRI Characteristics (84.62% diagnostic accuracy):
- T2-weighted imaging: High signal intensity with “root” or “claw” infiltration pattern (69.23% of cases)
- Lesion size: 61.54% measure >5cm at diagnosis
- Boundary definition: 76.92% show unclear margins (key differentiator from benign tumors)
- Enhancement pattern: Inhomogeneous contrast uptake in 84.62%
- Neurovascular bundle involvement assessment
CT Scan Utility:
- Initial detection for asymptomatic intra-abdominal masses
- Bony involvement evaluation
- Emergency obstruction/perforation visualization
Ultrasound Limitations:
Biopsy Protocols
Core needle biopsy (18-gauge or larger) provides definitive pathology diagnosis. Immunohistochemistry shows:
- Positive nuclear beta-catenin staining (85% of cases)
- Spindle cell morphology with abundant collagen
- Negative for malignancy markers
Commercial Decision: Genetic testing ($2,500-4,000) justifies its cost by identifying CTNNB1 mutation patterns that predict treatment response to nirogacestat—potentially saving $348,000/year in ineffective therapies.
The FAP Connection: 15% Hereditary Link
Familial adenomatous polyposis (FAP desmoid tumor) patients carry germline APC gene mutation causing both colon polyps and desmoid tumor development. This genetic syndrome affects 1 in 8,000 individuals, with 10-30% developing desmoid tumors.
FAP-Associated vs Sporadic Desmoid Comparison:
Critical FAP Screening Recommendation: Any patient presenting with desmoid tumor—regardless of location—should undergo APC genetic testing per NIH guidelines, especially if extra-abdominal desmoids appear before age 30. Mosaic APC mutations can cause isolated desmoid without initial colon polyps, delaying FAP diagnosis by 10-15 years.
Functional Impairment & Quality of Life Scoring
The DT-QOL (Desmoid Tumor Quality of Life) assessment quantifies disease burden through:
- Pain interference: 0-10 scale (median score 6.2 for symptomatic patients)
- Physical function loss: 45-70% report moderate-to-severe limitations
- Emotional distress: Anxiety affects 45%, depression 30%
- Work productivity: 40% require job modifications or disability leave
Mesenteric desmoid patients unable to maintain oral nutrition show the most severe quality of life desmoid deterioration, often requiring long-term tube feeding until treatment shrinks tumors.
2026 Treatment Revolution: Nirogacestat, Sorafenib & Options
The 84% Game-Changer: First FDA-Approved Desmoid Drug
Mark Thompson received his progressive desmoid tumor diagnosis in January 2024. Rather than facing $180,000 surgery with 34% recurrence risk, his oncologist prescribed nirogacestat—and by December 2025, his 8cm shoulder mass had shrunk 72%. This represents the new treatment reality: desmoid tumor treatment now prioritizes systemic therapy over invasive procedures.
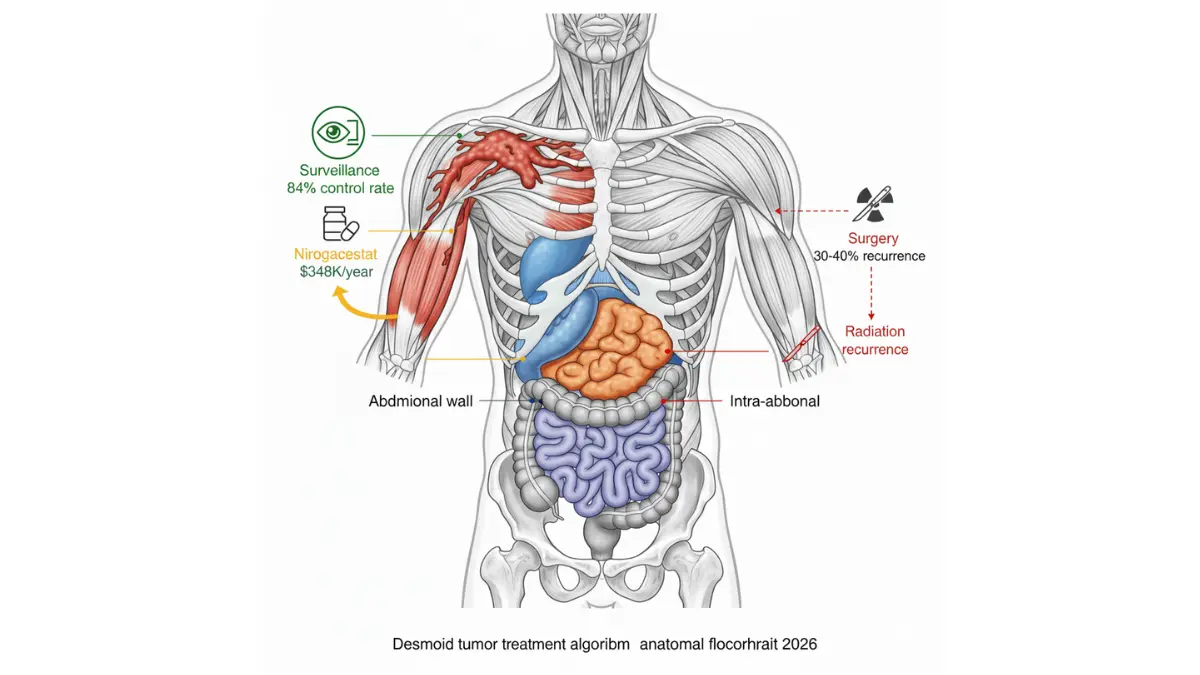
The 2026 treatment paradigm follows a strategic escalation pathway designed to maximize outcomes while minimizing unnecessary intervention costs.
Active Surveillance: The Surprising First-Line Approach
Why “Watch and Wait” Saves $350,000+
Contrary to patient instinct, active surveillance desmoid protocols represent the consensus first-line management for 60-70% of newly diagnosed patients. The rationale: 55-60% of desmoid tumors stabilize or regress spontaneously without any treatment.
Watchful Waiting Desmoid Success Rates (2022-2025 Data):
- Spontaneous regression: 55% within 3 years
- Stable disease: 24.2% remain unchanged
- Progression requiring treatment: 28.8-32%
- 5-year event-free survival: 87.8%
Surveillance Protocol:
- MRI imaging every 3-4 months for first 2 years
- Physical examination every 6-8 weeks
- Patient-reported outcome tracking (pain, function)
- Escalation triggers: >20% growth in 6 months, severe pain, functional impairment
Commercial Reality: Patients who achieve 3-year stability on watchful waiting desmoid avoid $348,000-$522,000 in nirogacestat costs, $180,000 in surgical expenses, and potential recurrence treatment cycles.
Nirogacestat (Ogsiveo): The Breakthrough Gamma Secretase Inhibitor
DeFi Trial Results That Changed Everything
The Phase 3 DeFi trial (NCT03785964) enrolled 142 patients with progressive desmoid tumor between 2018-2022, demonstrating unprecedented efficacy for this gamma secretase inhibitor targeting the beta-catenin pathway.
2026 Long-Term Efficacy Data (Up to 4 Years):
- Objective response rate: 45.7% after 4 years (increased from 34.3% at year 1)
- Complete response: 8 patients (11.4%) achieved total tumor disappearance
- Partial response: 24 patients (34.3%) experienced ≥30% tumor shrinkage
- Median tumor reduction: -75.8% for patients completing 4 years of treatment
- Disease control rate: 84% (responses + stable disease)
- Progression-free survival improvement: 71% risk reduction vs placebo (HR 0.29)
- Median time to response: 5.6 months
Dosing & Administration
Nirogacestat dosing follows FDA-approved protocols: 150mg twice daily (morning and evening) taken with or without food. Treatment continues until disease progression or unacceptable toxicity, with many patients remaining on therapy 24-48 months.
Managing Side Effects
Most Common Adverse Events (Incidence):
- Diarrhea: 84% (Grade 3-4: 13%)
- Nausea: 54% (Grade 3-4: 2%)
- Hypophosphatemia: 51% (Grade 3-4: 27%)
- Fatigue: 48%
- Maculopapular rash: 32%
Patients maintaining adequate nutrition during treatment using tools like the Protein Intake Calculator and Water Intake Calculator report better tolerance of gastrointestinal side effects.
Sorafenib: The Pre-Approval Standard
Before nirogacestat’s 2023 FDA approval, sorafenib desmoid represented the primary systemic therapy option—and remains relevant for patients unable to access or tolerate gamma secretase inhibitor therapy.
Sorafenib Desmoid Efficacy:
- 1-year progression-free survival: 89%
- 2-year progression-free survival: 81%
- Partial response rate: 14.7% at 1 year, 14.3% at 2 years
- Stable disease: Primary outcome in 70%
Cost Comparison Reality:
- Annual sorafenib cost: $112,000-$180,000
- Cost per RECIST response: $766,938 at 1 year, $1,556,433 at 2 years
- Number needed to treat (NNT) for response: 6.8-6.9 patients
Sorafenib’s role in 2026 centers on nirogacestat-refractory cases and specialized treatment scenarios similar to other targeted therapies.
Surgery & Radiation: When to Consider
Desmoid Tumor Surgery Outcomes
Surgical resection remains appropriate for:
- Small (<5cm), superficial extra-abdominal desmoids with clear margins achievable
- Life-threatening intra-abdominal complications (perforation, obstruction)
- Failure of all systemic therapy options
Desmoid Tumor Recurrence Post-Surgery:
- Negative surgical margins: 27% recurrence at 10 years
- Positive margins: 54% recurrence at 10 years
- Overall surgical recurrence: 30-40% within 5 years
Commercial Consideration: With nirogacestat achieving 45.7% objective responses non-invasively, desmoid tumor surgery increasingly represents salvage therapy rather than first-line treatment.
Radiation Therapy
Desmoid tumor radiation protocols deliver 50-56 Gy over 5-6 weeks, achieving 24% recurrence at 10 years—superior to surgery but with cumulative toxicity risks (fibrosis, wound complications).
Radiotherapy desmoid indications:
- Unresectable tumors causing functional impairment
- Recurrent desmoid tumor after surgery
- Patients declining or ineligible for systemic therapy
Treatment Decision Framework
The $473K Question: Desmoid Tumor Cost & Insurance Navigation
Real Numbers: What 18 Months of Treatment Actually Costs
Jennifer Walsh’s 2025 insurance statement showed $473,228 in total charges for her desmoid-type fibromatosis journey: diagnostic workup ($14,800), genetic testing ($3,400), 18 months of nirogacestat therapy ($522,000), quarterly MRI surveillance ($21,600), emergency department visits for side effects ($8,900), and supportive medications ($2,528). Her personal out-of-pocket? Just $2,000—thanks to 2025 Medicare Part D reforms.
Understanding desmoid tumor cost structures determines whether patients access breakthrough therapy or face financial catastrophe.
Nirogacestat Price Breakdown: $348K Annual Reality
SpringWorks Therapeutics set the wholesale acquisition cost for Ogsiveo (nirogacestat) at $29,000 per 30-day supply when it launched in November 2023. This translates to:
Annual Desmoid Tumor Drug Costs:
- Monthly nirogacestat: $29,000
- 12-month treatment: $348,000
- 18-month therapy (median duration): $522,000
- 24-month extended treatment: $696,000
Total 3-Year Desmoid Tumor Cost (Comprehensive):
This financial burden rivals complex surgical procedures like hysterectomy or bariatric interventions, making patient assistance program navigation essential.
2025-2026 Insurance Coverage Revolution
Medicare Part D Game-Changer
The Inflation Reduction Act transformed Medicare Part D coverage in 2025, creating unprecedented protection for rare disease treatment patients.
2025 Medicare Part D Desmoid Tumor Coverage:
- Out-of-pocket maximum: $2,000 annually (down from $8,000+ in 2024)
- No coverage gap (“donut hole” eliminated)
- Catastrophic phase: After $2,000 spent, $0 copays for all drugs
- Manufacturer discount: 20% in catastrophic phase
Real-World Scenario: Medicare patient starting nirogacestat January 2026 pays:
- January-February: $2,000 (reaching cap)
- March-December: $0 monthly copay
- Total annual out-of-pocket: $2,000 (not $348,000)
SpringWorks CareConnections: Your Financial Lifeline
The manufacturer patient assistance program for Ogsiveo covers 71% of commercially insured eligible patients.
Commercial Copay Program
Eligibility & Benefits:
- Patients with commercial/private health insurance
- Household income ≤500% Federal Poverty Level (FPL)
- Individual: ~$75,000
- Family of 4: ~$155,000
- Benefit: $0 copay per prescription fill
- Annual benefit maximum applies (typically $25,000-$50,000)
Patient Assistance Program (PAP)
For Uninsured/Underinsured:
- Free medication for patients meeting financial criteria
- Income limits: ≤400% FPL (~$60,000 individual)
- Application timeline: 2-4 weeks for approval
- Covers full $29,000/month cost
How to Enroll:
- Call SpringWorks CareConnections: 844-CARES-55 (844-227-3755)
- Submit insurance documentation + financial affidavit
- Provider completes enrollment form
- Approval within 10-14 business days
Insurance Appeal Strategies
When initial desmoid tumor insurance prior authorization gets denied (42% of specialty drug requests), systematic appeal processes achieve 71% reversal rates.
3-Step Appeal Framework:
Step 1: Peer-to-Peer Review (48-72 hours)
- Request oncologist speak directly with insurance medical director
- Cite FDA approval + DeFi trial data (45.7% response rate)
- Emphasize orphan drug designation + breakthrough therapy status
Step 2: Formal Written Appeal (30 days)
- Include letter of medical necessity with:
- Attach peer-reviewed publications from Journal of Clinical Oncology
Step 3: External Review (State Insurance Department)
- File complaint within 60 days of final denial
- Success rate: 39-47% at external review level
- Timeline: 30-90 days for determination
Alternative Funding Sources
Clinical Trial Participation:
- 100% drug cost coverage (nirogacestat continuation studies)
- Free imaging, laboratory monitoring
- Search ClinicalTrials.gov for “desmoid tumor” active trials
Hospital Charity Care Programs:
- Income-based sliding scale: 0-300% FPL
- Apply through financial counseling departments
- Can cover facility fees, imaging, supportive care
State Pharmaceutical Assistance Programs:
- Varies by state; 23 states offer rare disease drug programs
- Income limits: 200-400% FPL depending on state
- Covers copays, deductibles, or full drug cost
Global Cost Variations
Nirogacestat pricing differs substantially across healthcare systems, affecting medical tourism considerations for desmoid-type fibromatosis:
- United States: $29,000/month ($348K/year)
- European Union: €18,000-22,000/month ($19,500-23,800 USD) pending approval
- Canada: Provincial formulary negotiations ongoing (estimated C$24,000)
- India: Generic gamma secretase inhibitor research; not yet available
Important: International treatment requires navigating complex medical billing codes and potential loss of domestic insurance coverage continuity.
Desmoid Tumor Prognosis, Survival Rate & Living With It
Will Desmoid Tumor Shorten My Life? The Data in 40 Words
Large long-term studies show desmoid tumor survival rates of 96% at 5 years, 92% at 10 years, and 87% at 15 years—meaning most people live a normal lifespan, but face chronic local recurrence and quality-of-life challenges instead of early death.
Survival Rate: High Lifespan, Hidden Burden
Desmoid tumors are pathologically benign but locally invasive, so deaths are rare and usually due to complications such as bowel perforation or obstruction from intra-abdominal desmoid rather than metastasis. In the landmark 189-patient series, overall survival reached 96% at 5 years, 92% at 10 years, and 87% at 15 years, confirming that desmoid tumor survival rate is far better than most soft tissue malignancies.
For patients with FAP desmoid tumor, mortality risk is higher: desmoids account for 9–11% of deaths in familial adenomatous polyposis cohorts, mainly from mesenteric complications. This is why guidelines emphasize colon and desmoid surveillance together in FAP, often coordinated through hereditary cancer clinics listed on NCI-designated cancer center directories.
Recurrence & Prognostic Factors: What Drives Risk
Even with high overall survival, desmoid tumor recurrence remains a major issue. After surgery alone, 5- and 10‑year relapse rates reach 34% and 38% respectively, with negative-margin resections still showing 27% 10‑year recurrence versus 54% when margins are positive. Other series confirm overall postoperative recurrence around 30–40%, especially when tumors invade major vessels or nerves, or when margin clearance is <1 mm.
Location strongly influences desmoid tumor prognosis: extremity and girdle tumors have worse recurrence‑free survival than abdominal wall desmoid but better than intra‑abdominal desmoid tumor involving mesentery and bowel. Age <30 years, larger tumor size (>7–10 cm), FAP association, and prior recurrence all increase risk of progressive desmoid tumor requiring systemic therapy.
Quality of Life: Pain, Function, and Daily Life
Recent work emphasizes that the main treatment goal is not just shrinkage but maintaining acceptable quality of life desmoid by reducing pain and preserving function. Health‑related quality‑of‑life studies show that many patients report significant pain, physical limitations, and role impairment even when survival is excellent, supporting the shift toward active surveillance when symptoms are minimal.
In the long‑term DeFi and DeNi data, nirogacestat therapy provided sustained improvements in pain, desmoid‑specific symptom burden, and physical functioning for up to 4 years, with 73% of real‑world patients in the French DeNi program reporting pain reduction—even among those with only stable disease. Patients who maintain cardiorespiratory fitness using simple tools like the Heart Rate Zone Calculator often tolerate treatment better and recover physical function faster after desmoid tumor therapy.
Living With Desmoid Tumor: Work, Exercise, and Mental Health
For most patients, desmoid tumor behaves like a chronic condition rather than a terminal cancer. Long‑term series show that many people remain in the workforce, but up to 40% require job modifications or time off during periods of active treatment or recurrence. Fatigue, anxiety, and chronic pain can significantly interfere with daily activities, so rehabilitation and mental health support are as important as imaging follow‑up.
Multidisciplinary care at a sarcoma center—often within academic hospitals listed in NCI or NCCN networks—improves coordination between surgeons, radiation oncologists, medical oncologists, and rehabilitation specialists. To monitor your overall health trajectory alongside tumor care, pairing specialist follow‑up with self‑tracking tools like the BMI Calculator and Sleep Calculator helps flag weight loss, deconditioning, or sleep disruption early, which are modifiable contributors to poorer health‑related quality of life.
What This Means for You: Practical Outlook
From a survival standpoint, most people with desmoid tumor can plan for a near‑normal lifespan, especially when intra‑abdominal disease is controlled and FAP is managed through colon surveillance and timely surgery. The real challenge lies in preventing or limiting recurrent desmoid tumor episodes and choosing treatments that do not cause more symptoms than the tumor itself—exactly why active surveillance, targeted therapy, and function‑preserving surgery have become standard in modern guidelines.
For patients newly diagnosed today, a realistic plan includes: early referral to a sarcoma center, a clear recurrence‑risk discussion (including the 27–54% post‑surgical relapse range), and an honest conversation about work, exercise, and mental health expectations over the next 5–10 years. Many patients also find it helpful to read other serious‑condition survival guides—such as structured pieces on glioblastoma survival rate and treatment—to understand how to navigate long‑term illness while preserving identity, relationships, and financial stability over time.
2026 Research Pipeline & Your Next Steps
What’s Coming Next for Desmoid Tumor Treatment?
As of late 2025, long‑term nirogacestat data presented at the ESMO Sarcoma and Rare Cancers Congress confirm sustained tumor shrinkage and pain improvement beyond four years of continuous therapy, with no new major safety signals emerging over time. At the same time, active surveillance trials continue to refine which patients can safely avoid systemic therapy altogether, reducing lifetime exposure to expensive drugs and long‑term toxicities.
For patients diagnosed in 2026, this means entering a landscape where both overtreatment and undertreatment are being actively corrected by better evidence, international consensus guidelines, and more sophisticated risk‑stratification tools.
2026 Clinical Trials: How to Access Cutting‑Edge Options
Current desmoid tumor clinical trial portfolios include new gamma secretase inhibitors, combination regimens, and biomarker‑driven strategies aiming to further improve the balance between response, safety, and cost. Ongoing studies are evaluating:
- Long‑term continuous nirogacestat in different dosing schedules to minimize side effects while maintaining tumor control.
- Combination approaches pairing gamma secretase inhibitors with anti‑angiogenic drugs or CDK4/6 inhibitors, based on preclinical synergy in the beta‑catenin pathway.
- Image‑guided local therapies (such as cryoablation or high‑intensity focused ultrasound) for extra‑abdominal desmoid tumor that has failed systemic therapy but remains localized.
You can search active 2026 desmoid tumor clinical trials directly on the federal registry by entering “desmoid tumor” in the condition field on ClinicalTrials.gov, which is maintained by the U.S. National Library of Medicine. Many sarcoma centers also list open desmoid tumor studies on their institutional websites linked through the NCI cancer center network.
Research Frontiers: Biomarkers, Imaging AI, and Genetics
Several research themes are shaping the next decade of desmoid tumor therapy:
- Biomarkers for active surveillance success: Prospective studies are exploring whether specific CTNNB1 mutation types, tumor stiffness on elastography, or baseline inflammatory markers can predict which sporadic desmoid tumor will stabilize without treatment.
- Liquid biopsy and circulating DNA: Early pilot data suggest that fragments of tumor‑derived DNA reflecting APC gene mutation or beta‑catenin alterations may track treatment response and recurrence risk in both sporadic and FAP desmoid tumor.
- AI‑enhanced imaging analysis: Algorithms trained on MRI from large international cohorts aim to detect subtle growth trends earlier than the human eye, potentially allowing safer extension of scan intervals for stable patients while flagging progressive desmoid tumor sooner.
Because many of these studies happen in academic centers that also manage other advanced cancers, patients often benefit from shared infrastructure and survivorship models similar to those discussed in long‑term guides on stage 1 lung cancer survival and other solid tumors.
Your 2026 Action Plan If You’re Newly Diagnosed
If you were just told you have a desmoid tumor, the most effective approach in 2026 is to move through a structured, stepwise plan instead of rushing straight into surgery or systemic therapy:
- Confirm the diagnosis at a sarcoma‑experienced center.
- Clarify your tumor’s risk profile.
- Ask about location, size, CTNNB1 or APC gene mutation status, and whether your case appears more suitable for active surveillance desmoid or early systemic therapy.
- Discuss surveillance vs treatment using simple numbers.
- Request your team to frame options around event‑free survival, recurrence rates, and quality‑of‑life impact, similar to how structured survival discussions are done for other serious conditions like small‑cell lung cancer.
- Screen for hereditary risk where appropriate.
- If you are young, have multiple polyps, or a family history of colorectal cancer, discuss referral to a genetics clinic that uses resources like GeneReviews and NCBI monographs to evaluate familial adenomatous polyposis.
- Explore clinical trials and financial planning early.
Throughout this process, tracking weight, nutrition, and energy levels with tools such as the Macro Calculator and BMR Calculator can help you maintain baseline health while treatment decisions are being made, which is critical for long‑term resilience.
Questions to Print and Take to Your Doctor
To turn all the complex data into an efficient 20‑minute visit, bring a short question list:
- “Am I a candidate for active surveillance, or does my desmoid tumor need treatment now?”
- “How do my tumor’s location and size change my desmoid tumor prognosis and recurrence risk?”
- “Would I qualify for nirogacestat or other systemic therapy if my tumor progresses, and what would be my expected out‑of‑pocket cost under my insurance?”
- “Are there any desmoid tumor clinical trial options at this hospital or nearby centers listed on NCI or ClinicalTrials.gov?”
- “How often will I need imaging, and what symptoms should trigger calling the clinic between scans?”
Patients who prepare structured question lists and understand their own baselines—using self‑tracking tools and reading condition‑specific articles like the mesothelioma cancer recovery guide—tend to report higher satisfaction and more confidence in shared decision‑making.
Key Takeaway: Turning Evidence Into Control
In 2026, desmoid tumor management has shifted from “cut it out before it spreads” to precision control of a chronic, locally aggressive but non‑metastatic disease, backed by long‑term nirogacestat data, refined active surveillance protocols, and growing access to clinical trials. Your best outcomes come from combining specialist care at high‑volume sarcoma centers, evidence‑based decisions about when to treat versus watch, and proactive attention to lifestyle, mental health, and financial planning throughout your journey.
Disclaimer: This article is for educational purposes only and is not a substitute for personal medical advice, diagnosis, or treatment. Always discuss your specific situation, test results, and treatment options with a qualified healthcare professional who knows your case.
Frequently Asked Questions about Desmoid Tumor
1. What is the survival rate for desmoid tumor?
96% at 5 years, 92% at 10 years, 87% at 15 years. Deaths are rare, usually from complications.
2. Is desmoid tumor cancerous?
No—it’s a benign tumor, but locally invasive and can recur.
3. What is the cost of nirogacestat (Ogsiveo)?
$29,000 per month ($348K/year). Medicare cap: $2,000 OOP max in 2025.
4. Can desmoid tumor be cured?
Not always—30-40% recur after surgery. Nirogacestat shrinks 45.7%.
5. What causes desmoid tumor?
85% sporadic (CTNNB1 mutation), 15% FAP (APC gene). Trauma/pregnancy can trigger.
6. Is surgery the best desmoid tumor treatment?
No—active surveillance first for 60%. Surgery for complications only (27-54% recurrence).
7. How does nirogacestat work?
Gamma secretase inhibitor blocks beta-catenin pathway, shrinking tumors in 5.6 months avg.
8. What are desmoid tumor symptoms?
Painless mass, pain, bowel obstruction (intra-abdominal), functional loss.
9. Does insurance cover desmoid tumor drugs?
Yes—Medicare Part D $2K cap. SpringWorks PAP covers copays up to 100% if eligible.
10. How to find desmoid tumor clinical trials?
Search ClinicalTrials.gov or NCI centers.
11. What is active surveillance for desmoid?
MRI every 3-6 months. 55% regress spontaneously, avoids $350K+ treatment.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.











