On This Page – Quick Medical Summary
Why blood clots and pancreatic cancer go together
A pancreatic cancer diagnosis already carries enough fear without a second threat — yet blood clots are among the most common and most dangerous complications of this disease. If you are newly diagnosed and want to understand the risk, the next two sections explain why clots happen and how common they are. If you are a caregiver, or you have noticed leg swelling or breathlessness right now, move straight to the warning signs below. If you are already in treatment, the prevention and blood-thinner sections will matter most.
Here is the honest picture. Pancreatic cancer raises the risk of a clot more than any other cancer type, and a clot that reaches the lungs can become a medical emergency within hours. The reassuring part is that this risk is recognized, often preventable, and very manageable when it is caught early.
This guide is part of our larger resource on understanding pancreatic cancer from first signs to treatment.
ℹ️ Medical Disclaimer: This article is general health education, not a diagnosis, treatment plan, medication recommendation, or substitute for individual medical care. Blood clots can be life-threatening, and decisions about clot prevention, anticoagulant medications, and emergency symptoms must be made with a board-certified oncologist, hematologist, or emergency physician who knows your situation. If you think you may have a clot, seek medical care immediately rather than waiting.
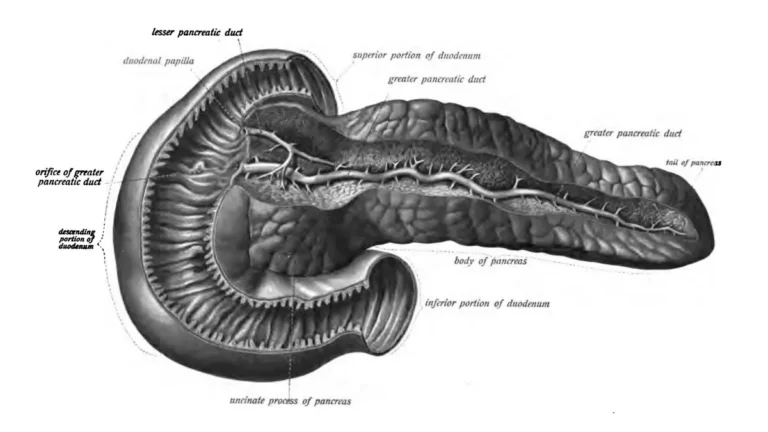
Why does pancreatic cancer cause blood clots?
Pancreatic cancer pushes the body into a clot-prone state by releasing substances that switch on the blood’s clotting machinery. This tendency toward abnormal clotting is called hypercoagulability, and pancreatic tumors drive it more strongly than most cancers.
What the tumor does to your blood
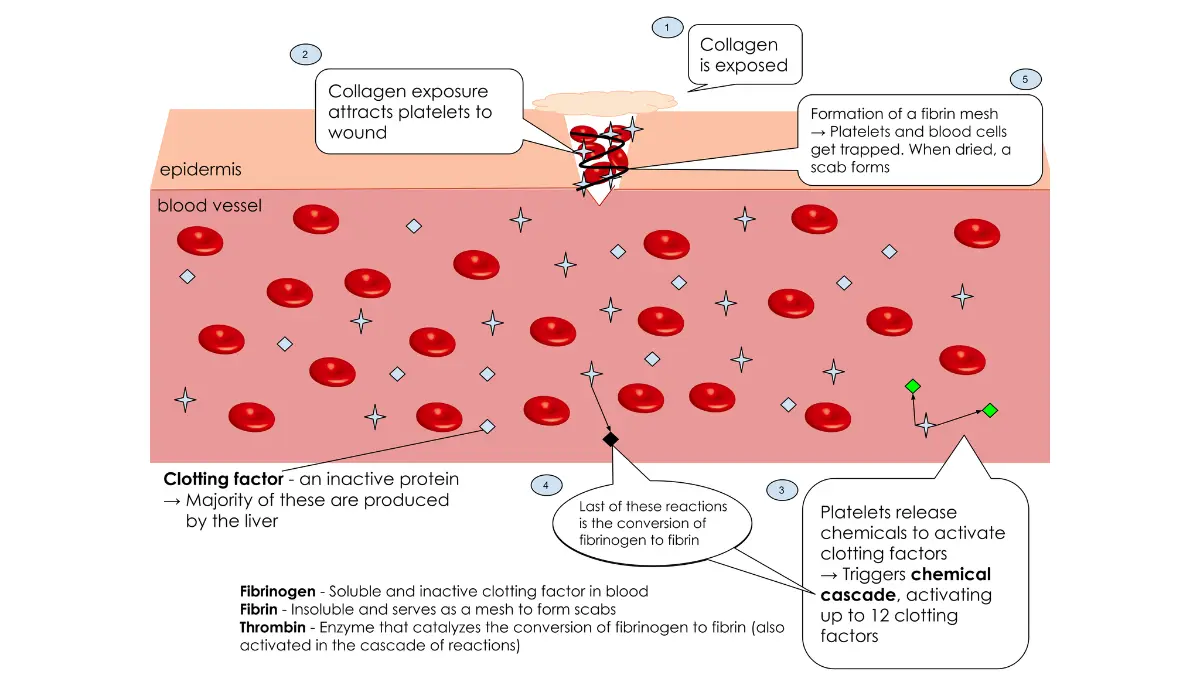
Pancreatic tumor cells over-produce a clot-triggering protein called tissue factor, and they shed tiny particles and inflammatory traps that make platelets stickier and the blood quicker to clot. The result is that a clot can form in a deep vein even without the usual triggers like surgery or long immobility. Understanding how blood clots form helps explain why this complication is so closely tied to the cancer itself.
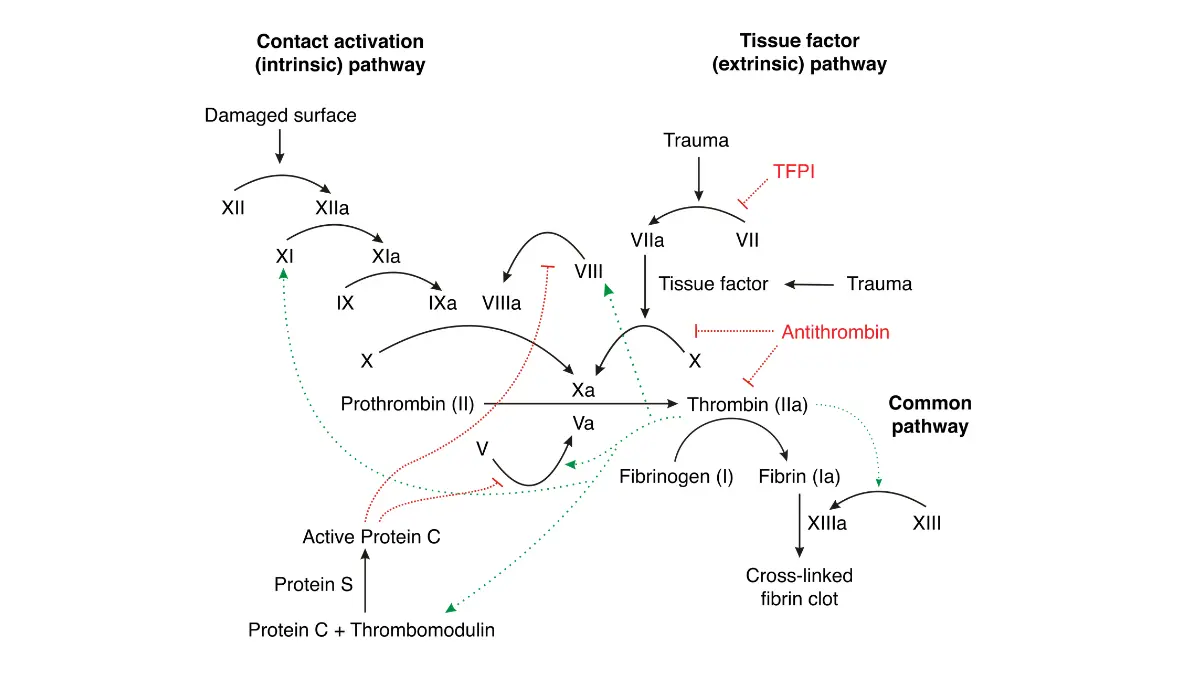
Adapted from Wikimedia Commons [Coagulation_full.svg], licensed under CC BY-SA 3.0.
🔬 How It Works: Normally, clotting only ramps up when a blood vessel is injured, sealing the wound. A pancreatic tumor releases tissue factor and other signals into the bloodstream, so the “seal the wound” switch gets flipped when there is no wound — letting clots form inside otherwise healthy veins.
Trousseau syndrome: a 150-year-old clue
The link is not new. Roughly 150 years ago, physician Armand Trousseau described migrating clots as a sign of hidden internal cancer — a pattern now called Trousseau syndrome and strongly associated with pancreatic cancer.
Can a clot appear before the cancer is found?
Sometimes a clot is the first clue. An unexplained clot can precede a pancreatic cancer diagnosis, which is one reason doctors occasionally look harder for an underlying cause after an out-of-the-blue clot. You can read more about the broader early signs of pancreatic cancer.
How common are blood clots in pancreatic cancer?
About 1 in 5 people with pancreatic cancer develop a venous blood clot — the highest rate of any cancer type. That makes venous thromboembolism (the medical term for a clot in a vein, abbreviated VTE) a complication worth understanding rather than fearing blindly.
About 1 in 5 patients
In a large study that followed people from the time of diagnosis, roughly 20% developed a clot, with the risk building over the first year. The two main forms are deep vein thrombosis (a clot in a deep vein, usually the leg) and pulmonary embolism (a clot that travels to the lungs).
📊 Clinical Data Point: Pancreatic cancer is associated with the highest incidence of venous thromboembolism of any cancer; about 1 in 5 patients (≈20%) are affected. — Source: Frere et al., Gastroenterology (BACAP study), 2020, the highest rate of any cancer type.
Risk rises with advanced stage and chemotherapy
The risk is not the same for everyone. It climbs with more advanced disease and during chemotherapy, and in people with advanced cancer receiving treatment, reported clot rates can reach roughly 40%. Lower-stage, resectable cancer carries a meaningfully lower risk.
Adapted from Wikimedia Commons [Blood_clot_formation.svg], licensed under CC BY-SA 3.0.
When clots are most likely to happen
Clots cluster in the months after diagnosis rather than appearing at random. In the same study, the average time from diagnosis to a clot was about 4 to 5 months — which is exactly the window where awareness pays off most.
Warning signs of a blood clot: when to get help
Knowing what a clot feels like is the single most useful thing on this page, because a clot in the lungs can be fatal if it is ignored. Seek urgent care for any of these symptoms — do not wait to see whether they improve.
Signs of a clot in the leg or arm (DVT):
- Swelling in one leg or arm (usually just one side)
- Pain, tenderness, or cramping, often starting in the calf
- Warmth in the affected area
- Red or discolored skin over the area
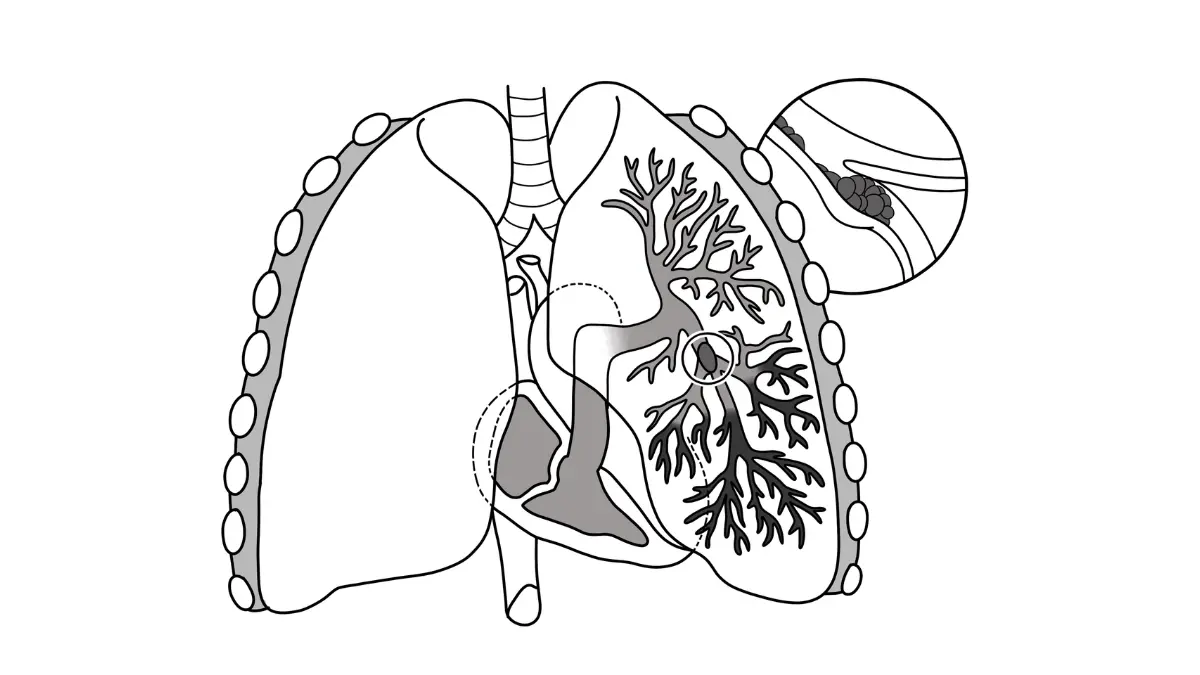
Signs of a clot in the lungs (PE) — a medical emergency:
- Sudden, unexplained shortness of breath
- Chest pain that worsens when you breathe in
- Coughing, sometimes coughing up blood
- A fast heartbeat, lightheadedness, or fainting
When to call 911 versus call your oncology team
Lung-clot symptoms are an emergency: call 911 or go to the nearest emergency department. Leg or arm symptoms also need prompt attention — call your oncology team or seek same-day care, because an untreated leg clot can travel to the lungs. You can learn more about pulmonary embolism symptoms, and our symptom checker can help you organize what you are feeling — though it is never a substitute for emergency care.
⚠️ Clinical Warning: A pulmonary embolism can stop blood flow to the lungs and become life-threatening within hours. Sudden shortness of breath, chest pain, or fainting in a person with pancreatic cancer is a 911 emergency — do not drive yourself and do not wait for the feeling to pass. The CDC outlines how to recognize the warning signs of DVT and PE.
✅ Patient Action: Save your oncology team’s after-hours number in your phone now, and ask them directly: “Which clot symptoms should send me to the emergency room, and which should I call you about first?”
What raises your clot risk, and how doctors measure it
Not every person with pancreatic cancer faces the same clot risk, and doctors use a structured tool to estimate it before chemotherapy. Understanding what raises your risk turns a vague worry into a specific conversation with your care team.
The Khorana score: how clot risk is estimated
The Khorana score is a validated tool that estimates the risk of a clot in cancer patients starting chemotherapy. It adds points for five factors: the type of cancer, a high platelet count, low hemoglobin (or use of red-cell-boosting drugs), a high white blood cell count, and a body mass index of 35 or higher. Pancreatic cancer sits in the highest-risk tumor category, so it alone contributes the maximum cancer-type points — you can check your BMI to see where one of those factors falls for you.
Why advanced stage and chemotherapy raise risk
Two of the strongest drivers are stage and treatment. More advanced or metastatic pancreatic cancer stages carry a substantially higher clot risk, and starting chemotherapy for pancreatic cancer raises it further.
Other factors: surgery, immobility, and a prior clot
Several familiar factors add to the risk: major surgery, long periods of reduced mobility, a central venous catheter, and a previous clot. Blood markers such as a raised D-dimer blood test can also flag higher risk, though they are interpreted by your clinician, not on their own.
✅ Patient Action: Before starting chemotherapy, ask your oncologist or a hematologist: “Based on my Khorana score and stage, do you recommend medication to help prevent blood clots?”
Preventing and treating clots: blood thinner options
When a clot needs to be prevented or treated, the main tool is anticoagulation — medicines commonly called blood thinners. This section is general education; the right choice depends on your situation and belongs to your oncology team.
Blood thinners used in cancer-related clots
Despite the nickname, blood thinners do not dissolve a clot you already have — they stop clots from forming or getting bigger while your body breaks them down, as MedlinePlus explains about how blood thinners work. For cancer-related clots, current guidelines support two main approaches: injectable low-molecular-weight heparin, and certain oral pills called direct factor Xa inhibitors, such as rivaroxaban or apixaban. Both are generally preferred over older warfarin-type drugs for clots linked to active cancer.
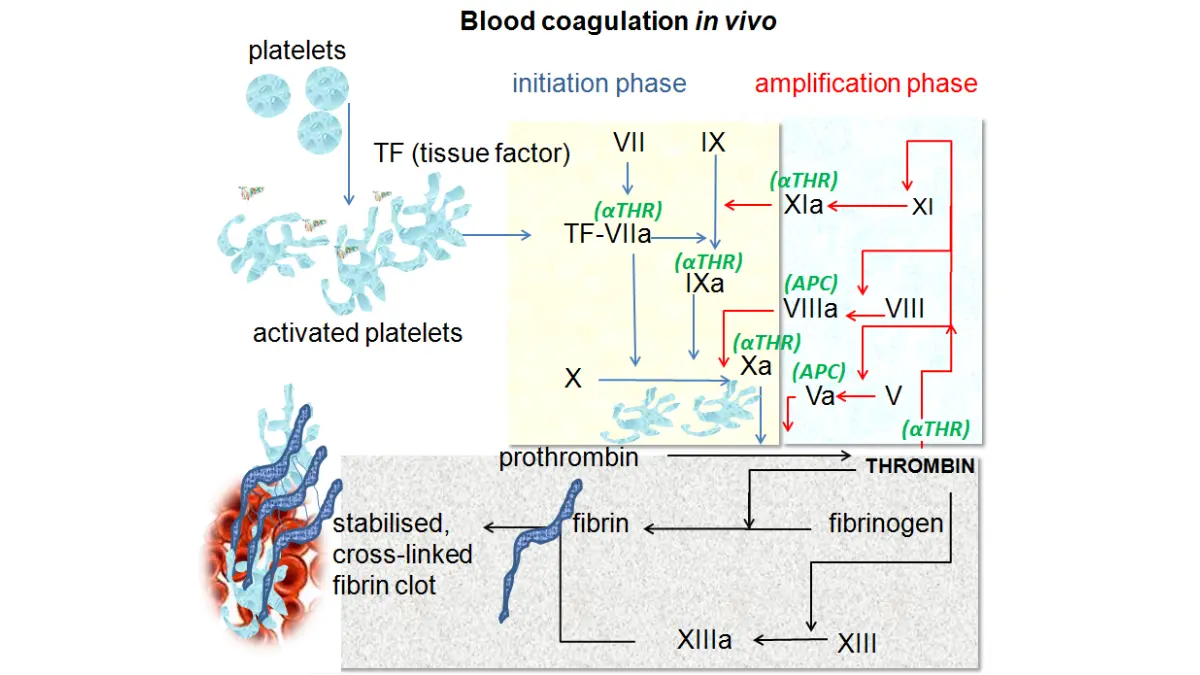
Adapted from Wikimedia Commons [Coagulation_in_vivo.png], licensed under CC BY-SA 3.0.
🔬 How It Works: Clotting depends on a chain of proteins called clotting factors. Low-molecular-weight heparin and factor Xa inhibitors each interrupt a step in that chain, so the blood is slower to form new clots — buying time for an existing clot to stabilize and shrink.
A caution specific to pancreatic and GI cancers
Drug choice matters here in a way that is easy to miss. The oral factor Xa inhibitors can carry a higher risk of stomach and intestinal bleeding in people with gastrointestinal cancers, which includes pancreatic cancer.
⚠️ Clinical Warning: Because pancreatic cancer is a gastrointestinal cancer, oral blood thinners like rivaroxaban and apixaban may raise the risk of stomach or bowel bleeding compared with injectable options. Current oncology guidelines specifically advise caution with these pills in this setting — which is why the choice must be individualized by your clinician.
How long is treatment, and who gets prevention?
Treatment for a cancer-related clot is generally continued for at least 6 months, and often longer while the cancer is active. For prevention before a clot, guidelines suggest considering medication mainly for higher-risk patients rather than everyone.
✅ Patient Action: Ask your oncologist: “Given my bleeding risk and that this is a GI cancer, which blood thinner is safest for me — an injection or a pill — and for how long?”
What a blood clot means for your outlook
If you have already had a clot, it is natural to wonder what it means for the road ahead — and the honest answer needs context, not alarm. A clot is associated with a tougher outlook, but it is a signal, not a sentence.
Why clots are linked to a tougher prognosis
Research links clots in pancreatic cancer with shorter survival on average. The most likely reason is that clots tend to appear alongside more advanced, more aggressive disease — so the clot is often a marker of what the cancer is doing, rather than the thing driving the outcome by itself.
What you can control
The encouraging part is how much falls within reach. Recognizing the warning signs early, having the prevention conversation before chemotherapy, and treating a clot promptly all directly improve safety. For trustworthy background on the disease overall, the National Cancer Institute’s pancreatic cancer information is a reliable starting point.
🩺 Physician Note: Current guidance treats clot risk as something to manage actively throughout cancer care — not a fixed fate. Catching a clot early and matching the right anticoagulant to the patient are the levers that change outcomes, which is why awareness matters as much as any single statistic.
Pancreatic cancer and blood clots: common questions
1. Why does pancreatic cancer cause blood clots?
Pancreatic cancer blood clots happen because tumor cells release tissue factor and other substances that activate the blood’s clotting system, creating a hypercoagulable state. This makes platelets stickier and the blood quicker to clot, so clots can form in deep veins even without the usual triggers like surgery or immobility.
2. How common are blood clots in pancreatic cancer?
About 1 in 5 people with pancreatic cancer (roughly 20%) develop a venous blood clot, the highest rate of any cancer type. The risk builds over the first year after diagnosis and rises further with advanced-stage disease and during chemotherapy, reaching as high as about 40% in some advanced cases.
3. What are the first signs of a blood clot?
A leg clot often causes swelling, pain or cramping, warmth, and red or discolored skin, usually in one leg. A lung clot causes sudden shortness of breath, chest pain that worsens with breathing, a fast heartbeat, or fainting. Lung-clot symptoms are an emergency — call 911 immediately.
4. Can a blood clot be the first sign of pancreatic cancer?
Yes, sometimes. An unexplained blood clot can appear before pancreatic cancer is diagnosed, which is one reason doctors may investigate further after an out-of-the-blue clot. This historical pattern of clots signaling a hidden cancer is known as Trousseau syndrome. Any unexplained clot should be evaluated by a physician.
5. What is Trousseau syndrome?
Trousseau syndrome describes migrating blood clots that can signal an underlying internal cancer, a pattern first described about 150 years ago and strongly linked to pancreatic cancer. It reflects the same hypercoagulable state the tumor creates. It is one of the reasons pancreatic cancer and blood clots are so closely connected.
6. Do all pancreatic cancer patients need blood thinners?
No. Guidelines generally suggest considering preventive blood thinners mainly for higher-risk patients — assessed using tools like the Khorana score and weighed against bleeding risk — rather than everyone with pancreatic cancer. Anyone who actually develops a clot does need treatment. Your oncologist should decide whether prevention is right for you.
7. Which blood thinner is used for pancreatic cancer?
Guidelines support injectable low-molecular-weight heparin or oral factor Xa inhibitors like rivaroxaban or apixaban for cancer-related clots. Because pancreatic cancer is a gastrointestinal cancer, the oral pills can carry a higher bleeding risk, so the choice is individualized. Discuss the safest option for you with your oncologist or hematologist.
8. How long do you take blood thinners with cancer?
Treatment for a pancreatic cancer blood clot is generally continued for at least 6 months, and often longer while the cancer remains active or you are still receiving chemotherapy. The decision to continue is reviewed periodically to balance clot prevention against bleeding risk. Your care team should reassess this with you over time.
9. Does chemotherapy increase blood clot risk?
Yes. Starting chemotherapy is a recognized risk factor for clots in pancreatic cancer, which is why the Khorana score is often calculated before treatment begins. The combination of active cancer and chemotherapy raises the clotting tendency. Ask your oncologist whether clot prevention is appropriate before you start.
10. What does a blood clot mean for pancreatic cancer prognosis?
On average, a blood clot is associated with shorter survival in pancreatic cancer, largely because clots tend to occur alongside more advanced, aggressive disease. The clot is usually a marker of what the cancer is doing rather than the cause of a worse outcome. Early recognition and prompt treatment improve safety.
11. Can blood clots in pancreatic cancer be prevented?
Often, yes. Preventive blood thinners can lower clot risk in selected higher-risk patients, and recognizing early warning signs allows fast treatment before a clot becomes dangerous. Prevention is matched to your individual risk and bleeding profile. Talk with your oncologist about whether preventive medication fits your situation.
Your next step
Blood clots are a real and serious part of pancreatic cancer, but they are also among the most manageable risks you face. The two things that matter most are within your control: recognize the warning signs of a leg or lung clot, and have a direct conversation with your oncology team about whether you should be on preventive medication.
If you take one action today, make it this — write down the emergency clot symptoms, keep your care team’s number close, and raise the prevention question at your next appointment. For the full picture of this disease, return to our guide on understanding pancreatic cancer from first signs to treatment.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.