On This Page – Quick Medical Summary
You just received your mammogram results, and the report mentions “BI-RADS Category 4” or says you need a callback. Your heart races, questions flood your mind, and you’re desperately searching for answers. Here’s what you need to know immediately: The BI-RADS system is a standardized classification ranging from 0 to 6 that helps doctors communicate mammogram findings consistently, and most callbacks do NOT mean cancer—only about 0.5% of women called back are ultimately diagnosed with breast cancer.
This comprehensive guide breaks down every BI-RADS category, explains exactly what happens after different results, and provides evidence-based strategies to manage anxiety while navigating the breast cancer screening process.
Understanding Your Mammogram Results – The Complete BI-RADS System Explained
What Your Mammogram Report Actually Tells You
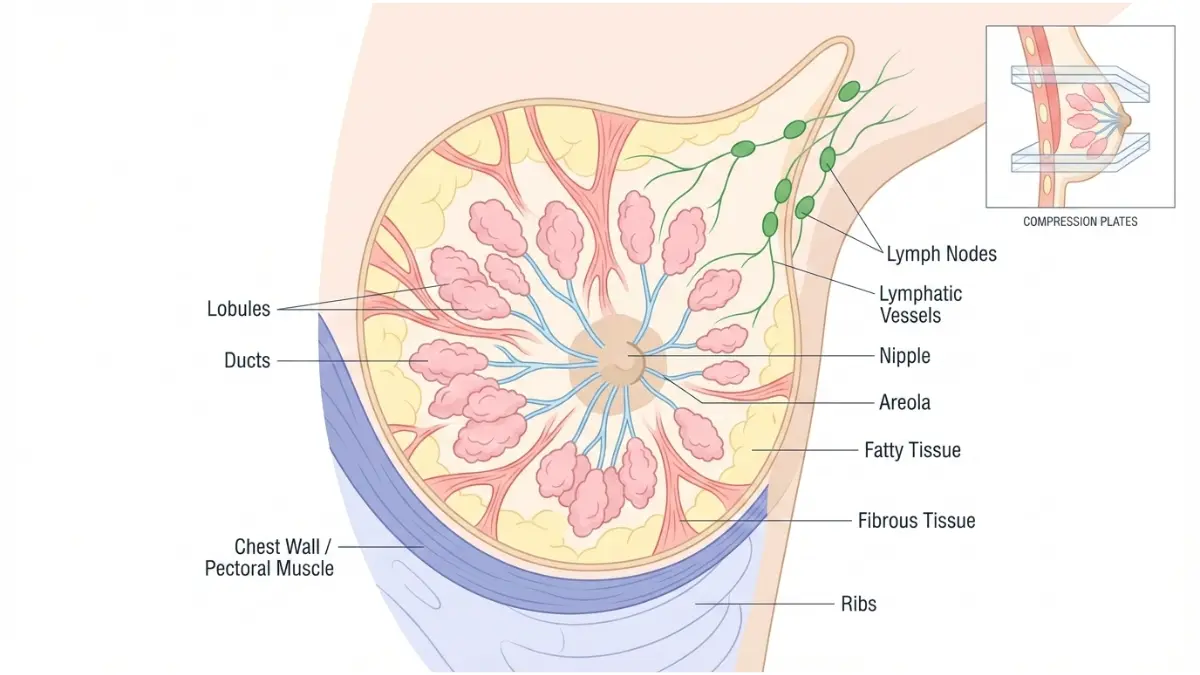
When radiologists review your mammogram images, they’re looking at breast tissue composition, searching for masses, calcifications, architectural distortions, or asymmetries that could indicate abnormalities. The American College of Radiology developed the Breast Imaging-Reporting and Data System (BI-RADS) to standardize how these findings are reported across all imaging facilities in the United States.
Your mammogram report contains several critical pieces of information beyond just the BI-RADS category. The report describes your breast density (categories A through D), details any specific findings observed, and provides management recommendations for your healthcare provider. Understanding these components empowers you to have informed conversations with your medical team about your breast health.
The BI-RADS classification system underwent its most recent update in 2013, with additional clarifications published by the FDA in 2024 regarding breast density reporting requirements.
The BI-RADS Scale: A Quick Reference Guide
The BI-RADS system categorizes mammogram results into seven distinct categories (0 through 6), each with specific meanings and recommended actions:
| BI-RADS Category | Finding | Cancer Risk | Recommended Action |
|---|---|---|---|
| 0 | Incomplete – Need Additional Imaging | Not Determined | Return for diagnostic mammogram/ultrasound |
| 1 | Negative – No abnormalities | 0% | Continue routine screening |
| 2 | Benign findings (cysts, calcifications) | 0% | Continue routine screening |
| 3 | Probably benign | <2% | Follow-up in 6 months |
| 4A | Low suspicion for malignancy | 2-10% | Biopsy recommended |
| 4B | Moderate suspicion | 10-50% | Biopsy recommended |
| 4C | High suspicion | 50-95% | Biopsy strongly recommended |
| 5 | Highly suggestive of malignancy | >95% | Biopsy essential, treatment planning |
| 6 | Known cancer (biopsy-proven) | 100% | Treatment monitoring |
What This Means For You: Understanding your specific category helps you know whether you need immediate action, follow-up imaging, or can simply continue your regular screening schedule. Categories 1, 2, and 3 represent the vast majority of mammogram results.

How Radiologists Assign Your Category
Radiologists—physicians specially trained in interpreting medical images—analyze multiple factors when assigning a BI-RADS category. They examine mass characteristics including shape (round, oval, or irregular), margin appearance (smooth versus spiculated), and tissue density patterns. Calcifications are evaluated based on their size, distribution, and morphology.
According to National Cancer Institute guidelines, radiologists also compare current mammograms with previous images when available, looking for any changes over time. This comparison is crucial because stability of a finding over years strongly suggests benignity, while new or changing findings warrant closer investigation.
Your breast density significantly impacts how radiologists interpret mammograms. Dense breast tissue appears white on mammograms, as do potential tumors, making detection more challenging. Approximately 40-50% of women undergoing mammography have dense breasts, which is why understanding density categories matters for your screening plan.
Real Patient Outcomes by Category
Understanding actual outcomes across different BI-RADS categories provides reassuring context. Research from the Breast Cancer Surveillance Consortium analyzing over 2.5 million mammograms found that approximately 10% of screening mammograms result in a callback (Category 0). Of these callbacks, only 10-20% proceed to biopsy, and among biopsied cases, roughly one-third are diagnosed with cancer.
This means that out of 1,000 women who get screening mammograms, about 100 receive callbacks. Of those 100, only 10-20 women undergo biopsy, and ultimately only 3-5 are diagnosed with breast cancer. These statistics from CDC breast cancer screening data highlight why callbacks, while anxiety-inducing, most often lead to benign outcomes.
For Category 3 (probably benign) findings, longitudinal studies show that fewer than 2% ultimately prove to be malignant. Category 4A lesions have actual malignancy rates of 7.6%, Category 4B approximately 22%, and Category 4C around 69%, according to research published in the National Mammography Database.
BI-RADS Category 0 – Callbacks, Anxiety & What Happens Next
Why “Category 0” Doesn’t Mean Cancer
Receiving a BI-RADS Category 0 result means your screening mammogram was incomplete or inconclusive—additional imaging is needed before a final assessment can be made. This category does NOT indicate cancer; rather, it signals that radiologists need more information to make an accurate determination.
Common reasons for Category 0 assignments include needing to compare current images with prior mammograms that weren’t immediately available, requiring additional views to better visualize a specific area, or identifying something that needs ultrasound evaluation to characterize properly. First-time mammogram patients receive Category 0 assessments more frequently—up to 16% compared to 10% for subsequent screenings—simply because no comparison images exist.
Real Patient Story: Jennifer, 42, received a callback after her first screening mammogram. The radiologist needed additional views of an area that appeared denser on one side. After targeted imaging, the asymmetry was determined to be normal anatomical variation—her BI-RADS was upgraded to Category 2, and she returned to annual screening.
The Callback Process: A Step-by-Step Timeline
Understanding the callback timeline helps reduce uncertainty. By federal law, you must receive written mammogram results within 30 days, though most facilities provide results within 1-2 weeks. If you need a callback, you may receive a phone call even before the official letter arrives.

Typical Callback Timeline:
- Days 1-7: Initial screening mammogram completed
- Days 3-10: Radiologist reviews images; callback notification sent if needed
- Days 7-21: Diagnostic mammogram appointment scheduled (most facilities aim for 1-2 weeks)
- Same day: Results typically provided immediately after diagnostic imaging
During your diagnostic mammogram appointment, a technologist takes additional targeted images of the area of concern. These may include spot compression views (focused on a specific area) or magnification views (for better detail of calcifications). You may also undergo breast ultrasound during the same visit, particularly if evaluating a potential mass or if you have dense breast tissue.
The radiologist reviews these diagnostic images in real-time while you wait, typically providing results before you leave the facility. This immediate feedback represents one of the few advantages of a callback—you get definitive answers quickly rather than waiting weeks.
Managing Callback Anxiety: Evidence-Based Strategies
Anxiety surrounding mammogram callbacks is not only common but physiologically normal. Research published in medical journals shows that 40-70% of women experience moderate to severe anxiety while awaiting callback appointments. Acknowledging this anxiety as a valid response rather than something to suppress helps you address it effectively.
Immediate Anxiety Management Techniques:
- Cognitive reframing: Remind yourself that 9 out of 10 callbacks result in benign findings
- Limit Dr. Google: Set specific boundaries on health information searching (perhaps 20 minutes, then stop)
- Mindful breathing: Practice 4-7-8 breathing (inhale 4 counts, hold 7, exhale 8) when anxiety spikes
- Social support: Share concerns with trusted friends or family who can provide emotional support
- Schedule promptly: The sooner you complete follow-up imaging, the sooner anxiety resolves
Consider using our Symptom Checker to evaluate any breast changes you’ve noticed, but remember that most callbacks occur without any physical symptoms—they’re purely imaging findings requiring clarification.
Dense Breasts and Callback Rates
As of September 2024, FDA regulations require all mammogram reports to include breast density information and notify patients if they have dense breasts. Dense breast tissue is categorized as either heterogeneously dense (Category C) or extremely dense (Category D), affecting approximately 40-50% of women aged 40 and older.
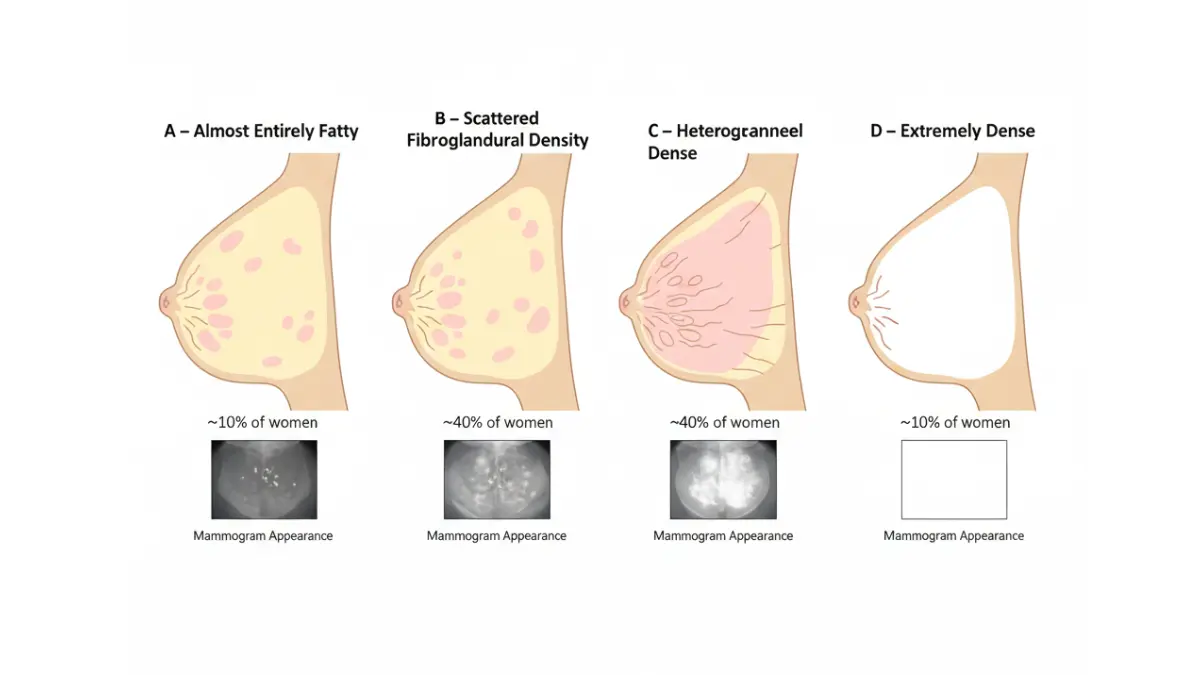
Women with dense breasts experience higher callback rates because dense fibroglandular tissue appears white on mammograms—the same color as potential tumors—making interpretation more challenging. Studies show callback rates of 12-14% for women with extremely dense breasts compared to 8-10% for those with predominantly fatty breasts.
Dense breast tissue also represents an independent risk factor for developing breast cancer, with women having extremely dense breasts facing 2-6 times higher risk than women with fatty breasts. This elevated risk stems partly from the masking effect (cancers hidden by dense tissue) and partly from biological factors researchers are still investigating.
Cost and Insurance Considerations
Under the Affordable Care Act, screening mammograms are covered by most insurance plans without copayment when performed in-network. However, diagnostic mammograms following a callback may involve cost-sharing depending on your specific insurance plan. Typical costs for diagnostic mammography range from $200-500 without insurance.
Financial Planning Tips:
- Verify whether your plan classifies follow-up imaging as “diagnostic” (may have copay) or screening continuation (typically covered)
- Request pre-authorization if your insurance requires it for diagnostic procedures
- Ask about payment plans or financial assistance programs if costs present barriers
- Understand that any biopsies recommended will involve separate charges
Contact your insurance provider before your diagnostic appointment to understand your expected out-of-pocket costs. Many breast imaging centers have financial counselors who can help you navigate insurance questions and explore assistance options if needed.
BI-RADS 1, 2, & 3 – Normal to Probably Benign Results
Category 1: All Clear – What’s Next?
BI-RADS Category 1 represents the ideal mammogram result: negative with no abnormalities detected. The radiologist found no masses, architectural distortions, suspicious calcifications, or concerning findings. Your breast tissue appears symmetrical and unremarkable on imaging.
When you receive a Category 1 result, your recommended action is straightforward—continue your routine screening schedule. For most women, this means annual mammograms starting at age 40, based on American Cancer Society recommendations updated in 2024. Women with elevated risk factors may require more frequent screening or supplemental imaging.
Use this clean bill of health as motivation to maintain other aspects of breast health. Consider evaluating your personal risk factors using our Genetic Risk Assessment Tool, particularly if you have family history of breast or ovarian cancer that might warrant genetic counseling.
Category 2: Benign Findings Explained
BI-RADS Category 2 results indicate that radiologists identified findings that are definitively benign—meaning absolutely not cancerous. These findings might include simple cysts (fluid-filled sacs), benign calcifications from previous breast infections or trauma, intramammary lymph nodes, or surgical clips from previous biopsies.
Common Category 2 Findings:
- Simple cysts: Round, fluid-filled structures with smooth borders that appear black on ultrasound
- Calcified fibroadenomas: Previously benign solid masses that developed calcifications over time
- Fat necrosis: Areas of damaged fatty tissue, often from previous surgery or injury
- Lymph nodes: Normal immune system structures within breast tissue
- Skin calcifications: Calcium deposits in skin rather than breast tissue
Despite these benign findings being documented, your management remains the same as Category 1—continue annual screening mammograms. The radiologist notes these findings in your report so future radiologists know they’re longstanding benign features, not new concerning changes.
Many women feel confused that their mammogram is “abnormal” (because something was found) yet they’re told to do nothing differently. Understanding that Category 2 truly means “nothing to worry about” helps alleviate this confusion.
Category 3: The “Watch and Wait” Approach
BI-RADS Category 3 indicates a probably benign finding with less than 2% likelihood of malignancy. While this small risk exists, immediate biopsy isn’t recommended because the probability of cancer remains extremely low. Instead, radiologists recommend short-term follow-up imaging to establish stability of the finding.
Common Category 3 findings include non-calcified, solid masses with smooth borders and round or oval shape, focal asymmetries that lack the suspicious features of true masses, and clusters of round calcifications. The key principle: if these findings remain stable over 2 years of follow-up imaging, their benign nature is confirmed.
Typical Category 3 Follow-Up Schedule:
- Initial diagnostic workup establishing Category 3 assessment
- First follow-up mammogram or ultrasound at 6 months
- Second follow-up at 12 months
- Third follow-up at 24 months
- If stable throughout, return to routine annual screening
Research shows that Category 3 lesions found to be growing during surveillance have favorable prognosis when biopsied and treated, with over 95% survival rates. This validates the watch-and-wait approach—we catch anything concerning early while avoiding unnecessary biopsies for the vast majority that prove benign.
Follow-Up Imaging Schedules and Why They Matter
Adhering to your recommended follow-up schedule is crucial for Category 3 findings. When patients miss follow-up appointments, radiologists lose the ability to confirm stability, potentially requiring reclassification to Category 4 and biopsy recommendation simply due to incomplete information rather than concerning changes.
Set calendar reminders immediately upon receiving your Category 3 result. Treat follow-up appointments with the same importance as the initial screening. Studies show that women who maintain consistent follow-up imaging have earlier detection of the rare Category 3 lesions that do progress to cancer, resulting in better treatment outcomes.
Some patients request immediate biopsy for Category 3 findings to eliminate the anxiety of waiting and monitoring. Discuss this option with your healthcare provider—while generally not recommended (given the low malignancy rate), your personal anxiety level and risk tolerance matter in shared decision-making about your care.
Similar to how medical imaging results require proper follow-up, echocardiogram results and other diagnostic tests benefit from consistent monitoring when initial findings warrant surveillance rather than immediate intervention.
Section 4: BI-RADS 4 (4A, 4B, 4C) & 5 – Suspicious Findings and Biopsy Recommendations
Understanding Category 4 Subdivisions
BI-RADS Category 4 encompasses findings that don’t have the classic appearance of malignancy but remain sufficiently suspicious to justify tissue sampling. Because this category covers a wide malignancy probability range (2-95%), the American College of Radiology recommends subdividing Category 4 into three levels based on suspicion degree.
Category 4A represents low suspicion (2-10% malignancy likelihood), Category 4B indicates moderate suspicion (10-50% likelihood), and Category 4C signals high suspicion (50-95% likelihood). National Mammography Database analysis of over 125,000 Category 4 examinations found actual cancer rates of 7.6% for 4A, 22% for 4B, and 69% for 4C.
These subdivisions help patients understand their specific situation better and allow physicians to tailor follow-up recommendations. For instance, some Category 4A findings might be approached with very short-interval follow-up imaging before proceeding to biopsy, while Category 4C findings warrant prompt tissue diagnosis.
What Makes a Finding “Suspicious”?
Radiologists classify findings as suspicious based on specific imaging characteristics that correlate with malignancy in research studies. Understanding these features demystifies why your radiologist recommends biopsy even when nothing is palpable.
Suspicious Mass Characteristics:
- Irregular or spiculated margins: Jagged, star-burst edges extending into surrounding tissue
- Irregular shape: Asymmetric, not round or oval
- Non-parallel orientation: Taller than wide when viewed from the side
- Posterior acoustic shadowing: Sound waves blocked behind the mass on ultrasound
Suspicious Calcification Patterns:
- Pleomorphic (varied shapes and sizes): Irregular, heterogeneous appearance
- Linear or branching: Following duct patterns
- Segmental distribution: Affecting one duct system
- Clustered tight grouping: Multiple calcifications in small area
Architectural Distortion:
- Disrupted normal tissue architecture: Spiculations radiating from a point without central mass
- Often subtle: Can represent scarring from previous surgery or underlying cancer
According to National Cancer Institute imaging guidelines, these suspicious features indicate areas requiring tissue sampling to definitively rule out malignancy, as imaging alone cannot provide pathologic diagnosis.
Biopsy Types and Procedures: A Complete Guide
If your radiologist recommends biopsy, several technique options exist depending on the finding’s characteristics and location. Understanding these procedures reduces anxiety about the unknown.
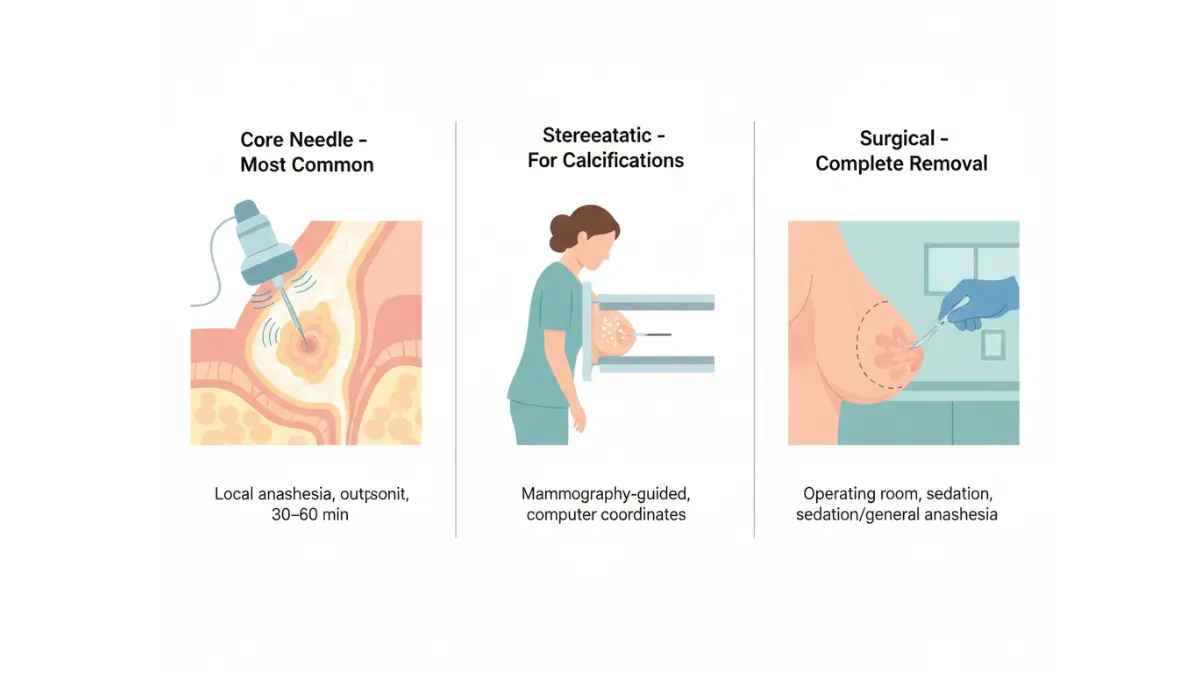
Core Needle Biopsy (Most Common):
- Performed with local anesthesia in outpatient setting
- Uses imaging guidance (ultrasound, mammography, or MRI)
- Removes several tissue samples (cores) using hollow needle
- Takes 30-60 minutes; minimal discomfort during and after
- Results typically available in 3-7 business days
Stereotactic Biopsy:
- Specifically for calcifications visible only on mammography
- You lie face-down on special table with breast compressed
- Computer calculates exact coordinates for needle placement
- Clips placed at biopsy site to mark location for future reference
Ultrasound-Guided Biopsy:
- Used for masses visible on ultrasound
- You lie on your back; real-time ultrasound guides needle
- Often quickest and most comfortable biopsy method
- No radiation exposure
Surgical/Excisional Biopsy:
- Removes entire lesion in operating room under sedation or general anesthesia
- Reserved for findings not amenable to needle biopsy
- Longer recovery time (1-2 weeks)
What This Means For You: Core needle biopsy provides accurate diagnosis in 95-98% of cases while avoiding surgery. Most women describe the experience as less uncomfortable than anticipated, with soreness similar to a bruise for 2-3 days afterward.
Category 5: High Suspicion Results
BI-RADS Category 5 indicates findings highly suggestive of malignancy, with greater than 95% cancer likelihood. These findings have the classic imaging appearance of breast cancer, prompting radiologists to recommend immediate tissue diagnosis and often concurrent surgical consultation.
When you receive a Category 5 result, biopsy is essential—not optional. The goal shifts from ruling out cancer to confirming the diagnosis pathologically and beginning treatment planning. While this news is understandably frightening, remember that early detection through mammography screening means most breast cancers are found at highly treatable stages.
The time from Category 5 biopsy to treatment initiation typically spans 2-4 weeks, allowing for comprehensive workup including additional imaging, genetic testing of the tumor, and multidisciplinary treatment team consultations. This waiting period, while difficult, ensures optimal treatment planning rather than rushed decisions.
Getting a Second Opinion: When and Why
For Category 4C and Category 5 results, consider obtaining a second opinion on your mammogram interpretation before proceeding to biopsy, particularly if you have access to a dedicated breast imaging center or university medical center. Research shows that subspecialist breast radiologists sometimes identify findings that general radiologists miss, and vice versa.
Second opinions become especially valuable when the clinical picture doesn’t match imaging findings (for example, a Category 5 result with no palpable mass in a young woman with no risk factors). Many major academic medical centers offer rapid second opinion services for mammography, with results available within 48-72 hours.
Just as seeking second opinions on MRI report findings can provide valuable perspective on complex imaging, having another expert review your mammogram ensures confidence in the recommended next steps.
Timeline: From Biopsy to Diagnosis
Understanding realistic timelines reduces anxiety while waiting for results. After your biopsy, the tissue samples go to a pathologist who examines them under a microscope to determine whether cancer cells are present.
Typical Biopsy Results Timeline:
- Days 1-3: Pathologist performs initial microscopic examination
- Days 3-5: Additional testing if cancer found (hormone receptors, HER2 status)
- Days 5-7: Final pathology report completed
- Within 1 week: Your physician contacts you with results
If benign, you receive clear reassurance that no cancer was found, with specific benign diagnosis noted (fibroadenoma, fibrocystic changes, etc.). If cancer is diagnosed, your physician discusses the specific type, grade, and hormone receptor status, and coordinates referral to breast surgical oncology and medical oncology specialists.
The majority of breast cancers detected through screening mammography are early-stage, with over 90% five-year survival rates according to American Cancer Society data, highlighting the value of regular screening and prompt follow-up of suspicious findings.
BI-RADS 6 & Life After Diagnosis – Treatment Monitoring
What BI-RADS 6 Means for Your Care
BI-RADS Category 6 is assigned only when you have known, biopsy-proven breast cancer that is currently undergoing treatment or additional pre-treatment imaging evaluation. This category doesn’t represent a new finding but rather indicates mammography’s role in monitoring known disease.
You receive Category 6 designations when getting pre-surgical imaging after your diagnosis to fully map disease extent, during neoadjuvant chemotherapy (chemotherapy before surgery) to assess treatment response, or when imaging tumor sites to guide surgical planning. The category clearly communicates to all healthcare providers that active cancer treatment is underway.
Once your breast cancer treatment is complete and you transition to survivorship care, subsequent mammograms no longer receive Category 6 designations. Instead, radiologists assign categories 1-5 based on imaging findings, just as for any screening patient, though your cancer history influences their interpretation and follow-up recommendations.
Monitoring Treatment Response
For patients receiving neoadjuvant chemotherapy, serial mammograms or other imaging modalities track how the tumor responds to treatment. Radiologists measure tumor size changes, evaluate for new suspicious findings in other breast areas, and assess regional lymph nodes.
Treatment Monitoring Imaging Schedule:
- Baseline diagnostic imaging at diagnosis
- Mid-treatment imaging (after 3-4 chemotherapy cycles)
- Pre-surgical imaging (1-2 weeks before planned surgery)
- Post-surgical imaging (establishing new baseline)
Significant tumor shrinkage on imaging correlates with better long-term outcomes and may allow less extensive surgery than originally planned. Conversely, if imaging shows lack of response or disease progression, your oncology team can adjust the treatment regimen promptly.
Modern imaging techniques including MRI and molecular breast imaging provide even more detailed assessment of treatment response than mammography alone. Your oncology team determines which imaging modalities best suit your specific situation based on tumor characteristics and treatment plan.
From Treatment to Survivorship Screening
After completing active breast cancer treatment, you transition to survivorship care with ongoing surveillance mammography. National Comprehensive Cancer Network guidelines recommend mammography every 6-12 months for the first 2-3 years post-treatment, then annually thereafter.
Survivorship Mammography Differs From Screening:
- More frequent initially: Semi-annual rather than annual
- Often diagnostic rather than screening: Includes spot compression views of treated areas
- Bilateral: Both breasts imaged even if cancer was unilateral
- May include ultrasound: Particularly of lumpectomy sites or reconstructed breasts
- Compared to post-treatment baseline: Looking for any new changes
Women who’ve had breast cancer face increased risk of second primary breast cancers—either recurrence in the treated breast (if lumpectomy performed) or new cancer in the opposite breast. This elevated risk justifies more intensive surveillance compared to women without cancer history.
Many breast cancer survivors experience significant anxiety surrounding follow-up mammograms, a phenomenon called “scanxiety.” Acknowledge these feelings as normal and employ anxiety management strategies developed during your initial treatment. Support groups specifically for breast cancer survivors can provide validation and coping strategies from others who understand this experience.
Support Resources and Next Steps
No one navigates cancer diagnosis and treatment alone. Numerous evidence-based resources support you through this journey:
National Organizations:
- American Cancer Society: 1-800-227-2345 (24/7 support, information, and resource navigation)
- National Cancer Institute Cancer Information Service: 1-800-4-CANCER
- CancerCare: Free counseling, support groups, financial assistance navigation
Many hospitals offer comprehensive breast cancer programs with nurse navigators who guide you through appointments, coordinate care between specialists, and provide emotional support throughout treatment. These navigators serve as your advocate and “quarterback,” ensuring nothing falls through the cracks.
Consider connecting with other patients through in-person or online support groups. Research consistently shows that peer support improves quality of life and reduces distress during cancer treatment. Organizations like the Cancer Support Community offer professionally-facilitated groups at no cost.
Maximizing Your Breast Health – Screening Guidelines, Risk Factors & Prevention
Who Should Get Mammograms and When?
Mammography screening recommendations have evolved as research clarifies the balance between early detection benefits and potential harms of overdiagnosis. The American Cancer Society’s 2024 updated guidelines recommend that women at average risk begin annual screening at age 40 and continue as long as they’re in good health with life expectancy of 10+ years.
Screening Guidelines by Risk Level:
Average Risk (No significant risk factors):
- Start annual screening at age 40
- Continue yearly mammograms
- Discuss individual preferences with healthcare provider
Higher Risk (Family history, genetic mutations, prior chest radiation):
- May start screening earlier (age 30 or even 25 for some high-risk groups)
- May include supplemental MRI screening in addition to mammography
- Work with breast specialist or genetic counselor to develop personalized plan
Very High Risk (BRCA1/2 mutation carriers):
- Annual breast MRI starting age 25-30
- Annual mammography starting age 30-40
- Consider risk-reducing strategies including medications or surgery
Women with extremely dense breasts may benefit from supplemental screening beyond mammography, though optimal approaches continue to be studied in clinical trials. Discuss your breast density and personalized screening plan with your healthcare provider.
Understanding Your Personal Risk Factors
Breast cancer risk results from complex interactions between genetic, hormonal, lifestyle, and environmental factors. While you cannot control some risk factors like age or family history, understanding your overall risk profile helps you make informed screening decisions.
Non-Modifiable Risk Factors:
- Age: Risk increases significantly after 50
- Family history: First-degree relatives with breast/ovarian cancer
- Genetic mutations: BRCA1, BRCA2, PALB2, and others
- Personal history: Previous breast cancer or certain benign breast diseases
- Dense breasts: Independent risk factor
- Reproductive history: Early menstruation, late menopause, first pregnancy after 30
Potentially Modifiable Risk Factors:
- Hormone therapy: Combined estrogen-progesterone therapy increases risk
- Alcohol consumption: Even moderate intake elevates risk
- Obesity: Particularly after menopause
- Physical inactivity: Regular exercise reduces risk
- Radiation exposure: Particularly chest radiation in teens/twenties
Use our Genetic Risk Assessment Tool to evaluate whether genetic counseling and testing might benefit you based on your family history. Women with BRCA1 or BRCA2 mutations face lifetime breast cancer risks of 45-85%, significantly higher than the 13% average risk.
Supplemental Screening for Dense Breasts or High Risk
Women with dense breasts face unique challenges because mammography sensitivity decreases as density increases. Supplemental screening options help detect cancers that might be masked by dense tissue.
Supplemental Screening Modalities:
3D Mammography (Tomosynthesis):
- Takes multiple x-ray images from different angles
- Reconstructs 3D breast image reducing tissue overlap
- Increases cancer detection by 20-65% compared to 2D
- Reduces callbacks by 15-40%
- Covered by most insurance for routine screening
Whole Breast Ultrasound:
- Uses sound waves rather than x-rays
- Particularly good for evaluating masses
- Can detect additional 1.8-4.2 cancers per 1,000 screened dense-breast women
- Increases false positives requiring biopsy
- May not be covered by insurance as supplemental screening
Breast MRI:
- Most sensitive breast imaging modality
- Recommended for high-risk women (lifetime risk >20%)
- Detects cancers missed by mammography and ultrasound
- High cost ($800-2,000) and limited availability
- Requires intravenous contrast injection
Molecular Breast Imaging:
- Functional imaging showing metabolic activity
- Useful for dense breasts
- Minimal radiation exposure (comparable to mammography)
- Limited availability, primarily at specialized centers
According to research from the University of California breast cancer research programs, combining mammography with supplemental ultrasound in women with dense breasts increases cancer detection rates while maintaining acceptable false-positive rates.
Lifestyle Modifications for Breast Health
While screening enables early detection, lifestyle choices can actually reduce breast cancer risk. The World Health Organization estimates that 30-50% of cancers are preventable through healthy lifestyle choices.
Evidence-Based Risk Reduction Strategies:
- Maintain healthy weight: Obesity increases postmenopausal breast cancer risk by 20-40%
- Exercise regularly: 150 minutes moderate activity weekly reduces risk by 10-20%
- Limit alcohol: Each daily drink increases risk by 7-10%
- Avoid or limit hormone therapy: Use shortest duration at lowest dose if needed
- Breastfeed if possible: Lowers risk, particularly if continued 1+ years
- Eat Mediterranean-style diet: Emphasizing vegetables, fruits, whole grains, healthy fats
Consider using our BMI Calculator and Weight Loss Calculator to assess whether weight management might reduce your breast cancer risk along with other health benefits.
For women at very high risk, chemoprevention with medications like tamoxifen or raloxifene can reduce breast cancer incidence by 40-50%. Discuss these options with your healthcare provider if you have significantly elevated risk.
Preparing for Your Next Mammogram
Optimizing your mammogram experience increases comfort and ensures high-quality images for accurate interpretation.
Pre-Mammogram Preparation Tips:
- Schedule during first week after your period (breasts less tender)
- Avoid caffeine 1-2 weeks before if you have fibrocystic breasts
- Don’t apply deodorant, powder, or lotion on exam day (can mimic calcifications)
- Wear two-piece outfit for easier changing
- Bring previous mammograms if changing facilities
- List any breast symptoms or concerns to share with technologist
During the exam, communicate with your technologist about any discomfort. While some compression is necessary for optimal imaging, it should never be unbearable. The compression lasts only a few seconds per image, with most exams taking 15-20 minutes total.
Request immediate read results if available at your facility. While many screening centers batch-read films and send results by mail, some offer same-day preliminary results that can reduce anxiety. However, understand that all screening mammograms undergo final interpretation by radiologists, and the official report within 1-2 weeks represents your definitive result.
Understanding breast health extends beyond mammography. Stay alert for concerning symptoms between screenings and maintain regular health checkups. Just as recognizing early warning signs of various cancers empowers proactive healthcare, understanding mammogram results helps you navigate breast cancer screening confidently and make informed decisions about your care.
Frequently Asked Questions (FAQs)
1. How soon will I get my mammogram results after screening?
By federal law, you must receive written results within 30 days, though most facilities provide results within 1-2 weeks. If immediate concerns arise, you may receive a phone call before the official letter. Some breast centers offer same-day preliminary results, though official reports follow within days.
2. What percentage of callbacks result in a cancer diagnosis?
Only about 0.5% of all women called back after screening mammograms are ultimately diagnosed with breast cancer. Approximately 10% of screening mammograms result in callbacks, but 90-95% of those callbacks lead to benign findings after additional imaging.
3. Is BI-RADS 0 the same as BI-RADS 4?
No, these categories are fundamentally different. BI-RADS 0 means incomplete—more images are needed before assigning a final category. BI-RADS 4 indicates suspicious findings requiring biopsy. After additional imaging, a BI-RADS 0 might become any category from 1-5 depending on what’s found.
4. What’s the difference between a screening and diagnostic mammogram?
Screening mammograms are routine annual exams for women without symptoms, using standard two-view images of each breast. Diagnostic mammograms involve additional targeted views, often with spot compression or magnification, to investigate specific areas of concern. Radiologists read diagnostic mammograms immediately while patients wait, whereas screening exams are batch-read later.
5. Should I be worried if I have dense breasts?
Dense breasts are very common, affecting 40-50% of women aged 40+. While dense tissue is associated with moderately increased breast cancer risk (2-4 times baseline), most women with dense breasts never develop cancer. The main concern is reduced mammography sensitivity, which is why discussing supplemental screening options with your healthcare provider is important.
6. How accurate are mammograms in detecting breast cancer?
Mammography sensitivity (ability to detect cancer when present) ranges from 77-95% depending on breast density and imaging technique. Sensitivity is highest (95%) in fatty breasts and lowest (60-70%) in extremely dense breasts. Specificity (correctly identifying absence of cancer) is approximately 90-95%. 3D mammography improves accuracy compared to traditional 2D imaging.
7. Can I refuse a biopsy if recommended?
Yes, you always have the right to decline any medical procedure. However, biopsy remains the only definitive way to diagnose or rule out breast cancer. If declining biopsy due to fear or misconceptions, discuss your concerns openly with your healthcare provider—they can address questions and potentially suggest alternatives like very short-interval follow-up imaging for lower-suspicion findings.
8. What does “probably benign” (Category 3) really mean?
Category 3 indicates findings with less than 2% cancer likelihood—meaning over 98% prove benign. Rather than immediately biopsying, radiologists recommend short-term follow-up imaging (typically at 6, 12, and 24 months) to establish stability. If stable throughout, the finding is confirmed benign. This approach avoids unnecessary biopsies for the vast majority of Category 3 lesions.
9. How long does it take to get biopsy results?
Most breast biopsy results are available within 5-7 business days. Pathologists need time to process tissue samples, examine them microscopically, and perform additional tests if cancer is found (hormone receptor status, HER2 testing). If results require special stains or expert consultation, timing may extend to 10-14 days, though this is uncommon.
10. Will insurance cover a diagnostic mammogram and biopsy?
The Affordable Care Act mandates coverage of screening mammograms without cost-sharing. However, diagnostic mammograms may involve copayments or deductibles depending on your insurance plan. Biopsies are typically covered as medically necessary procedures when recommended by physicians. Contact your insurance provider before procedures to understand your specific out-of-pocket costs.
11. What are the chances of a false positive on my mammogram?
False positive rates (being called back when no cancer is present) vary by age and breast density. Overall, cumulative false positive risk after 10 annual mammograms is approximately 50-60%, meaning half of women will experience at least one callback during a decade of screening. While callbacks cause anxiety, they’re an inherent part of mammography’s careful approach to not missing cancers.
12. When should I get a second opinion on my mammogram results?
Consider second opinions for Category 4 or 5 results before proceeding to biopsy, especially if you have access to subspecialist breast radiologists at dedicated breast centers. Second opinions are also valuable when clinical findings don’t match imaging (such as a palpable mass called Category 1-2 on mammography) or when you want additional perspective on Category 3 findings before committing to 2 years of surveillance.
13. Do all women over 40 need yearly mammograms?
Current American Cancer Society guidelines recommend starting annual mammography at age 40 for women at average risk, continuing as long as they’re in good health with 10+ year life expectancy. However, screening remains a personal choice—some women choose to start later or screen less frequently. Discuss your individual risk factors, preferences, and values with your healthcare provider to make the best decision for your circumstances.
Disclaimer: This article provides educational information about mammogram results and the BI-RADS classification system. It is not intended as medical advice, diagnosis, or treatment. Always consult with your healthcare provider about your specific mammogram results and individual breast health needs. If you have received abnormal mammogram results, follow your doctor’s recommendations for additional testing or evaluation.
About this content
This medical content is prepared through a structured publishing workflow with expert writing, clinical review and editorial quality checks.

Board Certifications: Medical Oncology (1999); Hematology (2000) Experience: 26 years | Location: Milan, Italy Education: MD, University of Milan (1996); Oncology Residency, European Institute of Oncology (1999); Fellowship…

Board Certifications: Obstetrics & Gynecology (2003); Reproductive Endocrinology (2008) Experience: 22 years | Location: Pune, India Education: MBBS, Armed Forces Medical College (2000); MD OB-GYN, All India Institute…

Board Certifications: Clinical Psychology License (India, 2010); Cognitive Behavioral Therapy Certification (Beck Institute, 2012) Experience: 15 years | Location: Bengaluru, India Education: BA Psychology, University of Delhi (2006);…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.