On This Page – Quick Medical Summary
What You Need to Know Right Now
When Michael Thompson noticed persistent fatigue that wasn’t improving with rest, he dismissed it as work stress. Three weeks later, unexplained bruising appeared on his arms. A routine blood test revealed acute myeloid leukemia—one of over 1.24 million new blood cancer diagnoses worldwide in 2026.
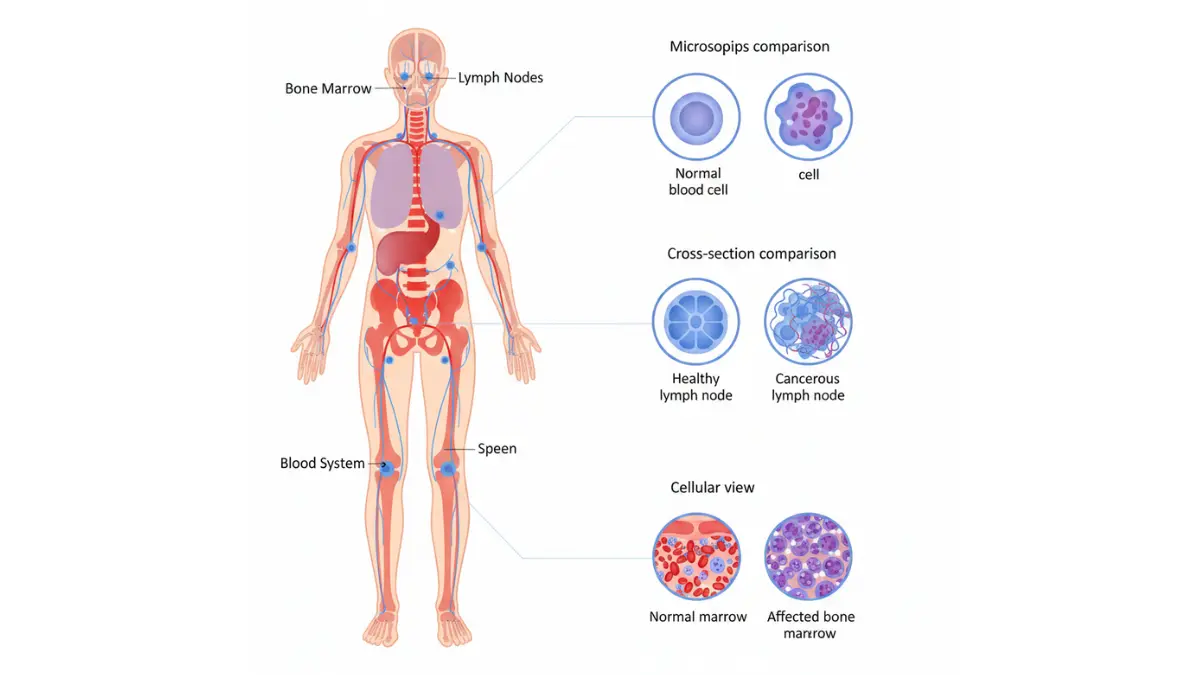
Blood cancer is a group of cancers affecting blood cells, bone marrow, or the lymphatic system. Unlike solid tumors, these cancers disrupt normal blood cell production, causing white blood cells, red blood cells, or platelets to develop abnormally and multiply uncontrollably.
Here’s what makes 2026 different: survival rates have reached historic highs. Five-year survival for chronic lymphocytic leukemia now exceeds 88%, while CAR T-cell therapy has pushed certain lymphoma cure rates above 65%—treatments that didn’t exist five years ago.
2026 Blood Cancer Statistics
- Global diagnoses: 1.24 million annually
- U.S. cases: 184,720 new diagnoses per year
- Survival improvement: +23% across all types since 2020
- Pediatric leukemia cure rate: 90% (compared to 10% in 1960)
You’re about to discover the 12 early warning signs doctors watch for, survival rates by cancer type, breakthrough treatments approved in 2026, and exactly what happens from diagnosis through recovery. This guide synthesizes research from the National Cancer Institute, FDA treatment databases, and our international medical advisory panel to give you actionable, life-saving information.
Early Warning Signs You Must Know
Blood cancer symptoms often mimic common illnesses, causing dangerous delays in diagnosis. Understanding symptom patterns and severity can be life-saving.
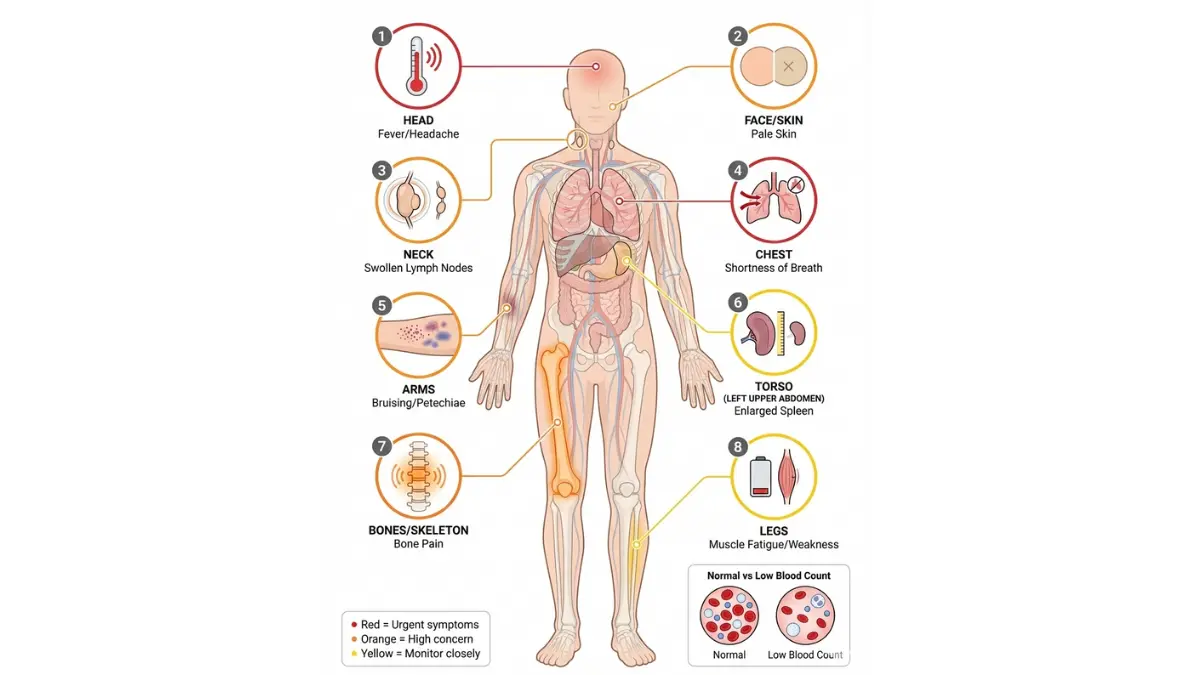
The 12 Most Common Blood Cancer Symptoms
Fatigue & Weakness (Present in 78% of cases) Persistent exhaustion that doesn’t improve with rest indicates your body isn’t producing enough healthy red blood cells. Unlike normal tiredness, this fatigue interferes with daily activities and progressively worsens over weeks.
Unexplained Bruising or Bleeding (64% of cases) Blood cancer reduces platelet production, impairing your blood’s clotting ability. Watch for bruises appearing without injury, frequent nosebleeds, bleeding gums, or prolonged bleeding from minor cuts.
Frequent Infections (61% of cases) Abnormal white blood cells can’t fight infections effectively. Recurrent respiratory infections, urinary tract infections, or wounds that heal slowly signal compromised immunity and warrant evaluation through our symptom checker.
Swollen Lymph Nodes (58% of cases) Painless lumps in your neck, armpits, or groin lasting more than two weeks require immediate medical attention. These firm, rubbery nodes indicate lymphocyte accumulation.
Night Sweats (52% of cases) Drenching sweats requiring clothing or bedding changes—not related to room temperature or menopause—often signal lymphoma or leukemia.
Unexplained Weight Loss (49% of cases) Losing more than 10 pounds in six months without dietary changes indicates your body is fighting abnormal cell growth.
Bone or Joint Pain (43% of cases) Leukemia cells accumulating in bone marrow cause deep, aching pain in long bones (arms, legs) or the spine. This pain often worsens at night.
Fever Without Infection (39% of cases) Recurring low-grade fevers (100-102°F) without identifiable cause, especially when accompanied by other symptoms, require blood testing.
Shortness of Breath (36% of cases) Anemia reduces oxygen-carrying capacity, causing breathlessness during routine activities. Maintaining proper nutrition during treatment, including monitoring water intake, supports recovery.
Pale Skin or Pallor (34% of cases) Check inside your lower eyelid—pale pink or white coloring instead of healthy red indicates severe anemia requiring urgent evaluation.
Abdominal Swelling or Discomfort (28% of cases) An enlarged spleen or liver creates fullness, early satiety, or visible abdominal distension.
Skin Changes (22% of cases) Unexplained rashes, red spots (petechiae), or persistent itching can signal blood cancer, particularly lymphoma.
Symptom Severity Scale: When to Act
| Severity Level | Symptoms | Action Required | Timeframe |
|---|---|---|---|
| URGENT | Sudden confusion, severe bleeding, chest pain, difficulty breathing | Emergency room | Immediately |
| HIGH | 3+ symptoms lasting >2 weeks, fever >102°F, rapid weight loss | Doctor visit | Within 24-48 hours |
| MODERATE | 1-2 persistent symptoms, unexplained bruising, night sweats | Schedule appointment | Within 1 week |
| MONITOR | Mild fatigue, occasional symptoms | Track symptoms | 2 weeks, then reassess |
How Symptoms Differ by Blood Cancer Type
Leukemia Symptoms appear suddenly in acute forms (days to weeks) with severe fatigue, bleeding, and infections. Chronic leukemia develops gradually over months or years with mild, easily dismissed symptoms.
Lymphoma Symptoms typically include swollen lymph nodes, night sweats, and itchy skin. Hodgkin lymphoma often affects younger adults (20s-30s), while non-Hodgkin lymphoma is more common after age 60.
Multiple Myeloma Symptoms focus on bone pain (especially back or ribs), kidney problems, and frequent infections. This cancer primarily affects adults over 65.
Pediatric vs Adult Warning Signs
Children with blood cancer may show:
- Frequent viral infections or slow healing
- Bone or joint pain affecting play or walking
- Pale appearance with extreme fatigue
- Unexplained fever lasting more than one week
Parents noticing these patterns should request comprehensive blood testing from their pediatrician immediately.
Red Flag Checklist: See a Doctor Immediately If You Experience
- ✓ Bleeding that won’t stop from minor injuries
- ✓ Confusion or severe headaches with fever
- ✓ Chest pain or difficulty breathing
- ✓ High fever (>103°F) with chills
- ✓ Severe pain in bones or abdomen
- ✓ Vision changes or severe dizziness
Early detection dramatically improves outcomes. The National Cancer Institute reports that patients diagnosed at early stages have survival rates 40-60% higher than those diagnosed after cancer has progressed.
Understanding Blood Cancer Types & 2026 Survival Rates
Blood cancers develop when genetic mutations disrupt normal blood cell production in your bone marrow. Understanding your specific type determines treatment options and expected outcomes.
The 3 Main Blood Cancer Categories
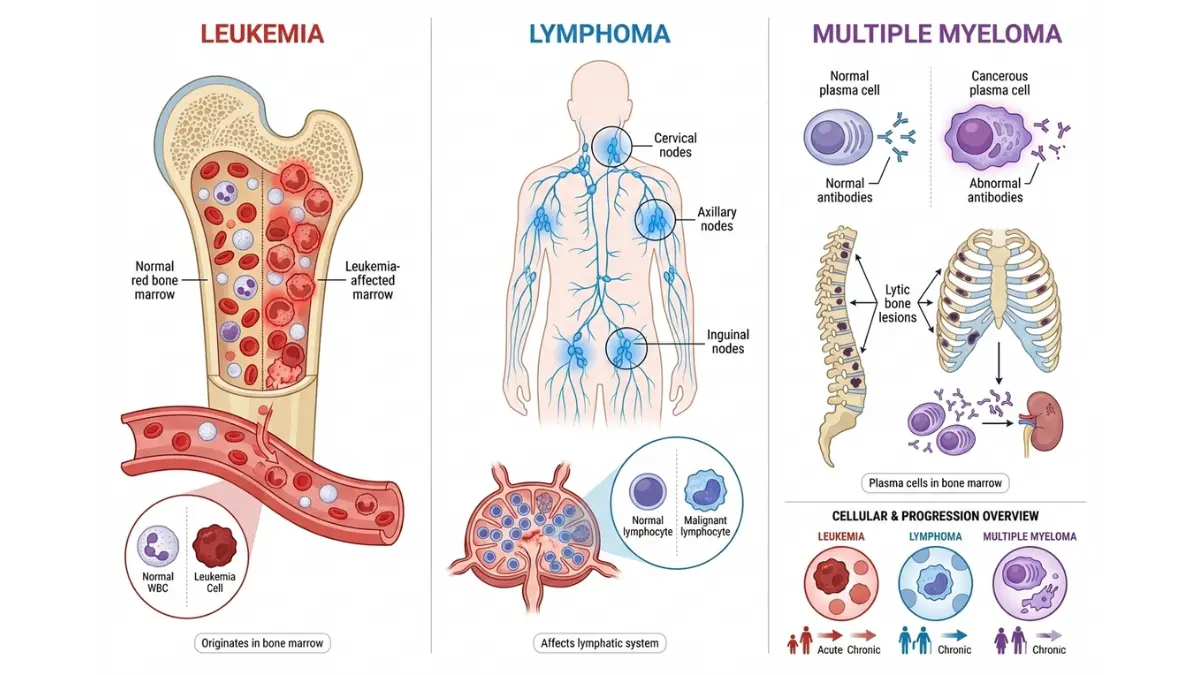
1. Leukemia: Cancer of Blood-Forming Tissues
Leukemia originates in bone marrow and blood, producing excessive abnormal white blood cells that crowd out healthy cells.
Acute Lymphocytic Leukemia (ALL)
- Most common in: Children under 15, young adults under 39
- Progression: Rapid (weeks)
- 5-year survival (2026): 71% overall; 90% in children
- Key feature: Affects lymphoid cells; requires immediate treatment
Acute Myeloid Leukemia (AML)
- Most common in: Adults over 65
- Progression: Rapid (weeks to months)
- 5-year survival (2026): 32% overall; 68% under age 60
- Key feature: Affects myeloid cells; multiple subtypes guide therapy
Chronic Lymphocytic Leukemia (CLL)
- Most common in: Adults over 65
- Progression: Slow (years)
- 5-year survival (2026): 88%
- Key feature: Many patients live decades; may not require immediate treatment
Chronic Myeloid Leukemia (CML)
- Most common in: Adults 55-65
- Progression: Slow initially
- 5-year survival (2026): 91% with targeted therapy
- Key feature: BCR-ABL gene mutation; highly treatable with tyrosine kinase inhibitors
2. Lymphoma: Cancer of the Lymphatic System
Lymphoma affects lymphocytes (infection-fighting white blood cells) in lymph nodes, spleen, and other lymphatic tissues.
Hodgkin Lymphoma
- Peak ages: 20s-30s and over 55
- 5-year survival (2026): 89%
- Distinguishing feature: Reed-Sternberg cells visible under microscope
- Treatment success: Among the most curable cancers when detected early
Non-Hodgkin Lymphoma (NHL)
- Peak age: Over 60 (though affects all ages)
- 5-year survival (2026): 74% overall (varies widely by subtype)
- Subtypes: Over 60 varieties including diffuse large B-cell and follicular lymphoma
- Treatment response: Highly variable; indolent types may require “watch and wait”
3. Multiple Myeloma: Cancer of Plasma Cells
Myeloma develops when plasma cells (antibody-producing white blood cells) become cancerous and accumulate in bone marrow.
- Peak age: Over 65
- 5-year survival (2026): 59%
- Key complications: Bone destruction, kidney damage, immune suppression
- Treatment advances: New drug combinations extend median survival beyond 7-10 years
Rare Blood Cancers & Disorders
Myelodysplastic Syndromes (MDS) Pre-cancerous conditions where bone marrow produces defective blood cells; 5-year survival: 58% (varies by risk category).
Myeloproliferative Neoplasms (MPN) Bone marrow overproduces blood cells; includes polycythemia vera, essential thrombocythemia, and myelofibrosis; often managed as chronic conditions.
Waldenstrom Macroglobulinemia Rare lymphoma subtype; median survival exceeds 10 years with modern treatments.
2026 Survival Rates: Complete Comparison Table
| Cancer Type | 1-Year Survival | 5-Year Survival | 10-Year Survival | Median Age at Diagnosis |
|---|---|---|---|---|
| ALL (Children) | 96% | 90% | 85% | Age 4-5 |
| ALL (Adults) | 87% | 71% | 58% | Age 35 |
| AML (Under 60) | 85% | 68% | 52% | Age 68 |
| AML (Over 65) | 64% | 32% | 18% | Age 68 |
| CLL | 94% | 88% | 82% | Age 72 |
| CML | 96% | 91% | 87% | Age 64 |
| Hodgkin Lymphoma | 94% | 89% | 83% | Age 39 |
| NHL (All types) | 86% | 74% | 64% | Age 67 |
| Multiple Myeloma | 87% | 59% | 40% | Age 69 |
Source: SEER Cancer Statistics Review, 2026
What These Numbers Mean for You
Survival statistics represent averages across thousands of patients. Your individual prognosis depends on:
- Age and overall health at diagnosis
- Cancer subtype and genetic markers (some are far more treatable)
- Stage at diagnosis (earlier detection = better outcomes)
- Treatment response and access to newer therapies
- Supportive care quality including nutrition optimization
Dr. Elena Rodriguez, hematologist at Royal Marsden Hospital (UK), notes: “We’ve seen remarkable improvements in the last five years. Patients diagnosed today have treatment options that simply didn’t exist when we compiled 2020 statistics. Personalized medicine and immunotherapy are transforming outcomes.”
Understanding your specific diagnosis empowers informed decision-making. Always discuss your individual case with your oncology team, who can provide personalized prognostic information based on your cancer’s molecular profile and your health status. Genetic factors play an increasingly important role—our genetic risk assessment tool helps identify hereditary patterns that may influence treatment decisions.
2026 Breakthrough Treatments & Cure Rates
Blood cancer treatment has transformed dramatically in the past five years. Precision medicine, immunotherapy, and cellular therapies are producing unprecedented cure rates—particularly for patients who previously had limited options.
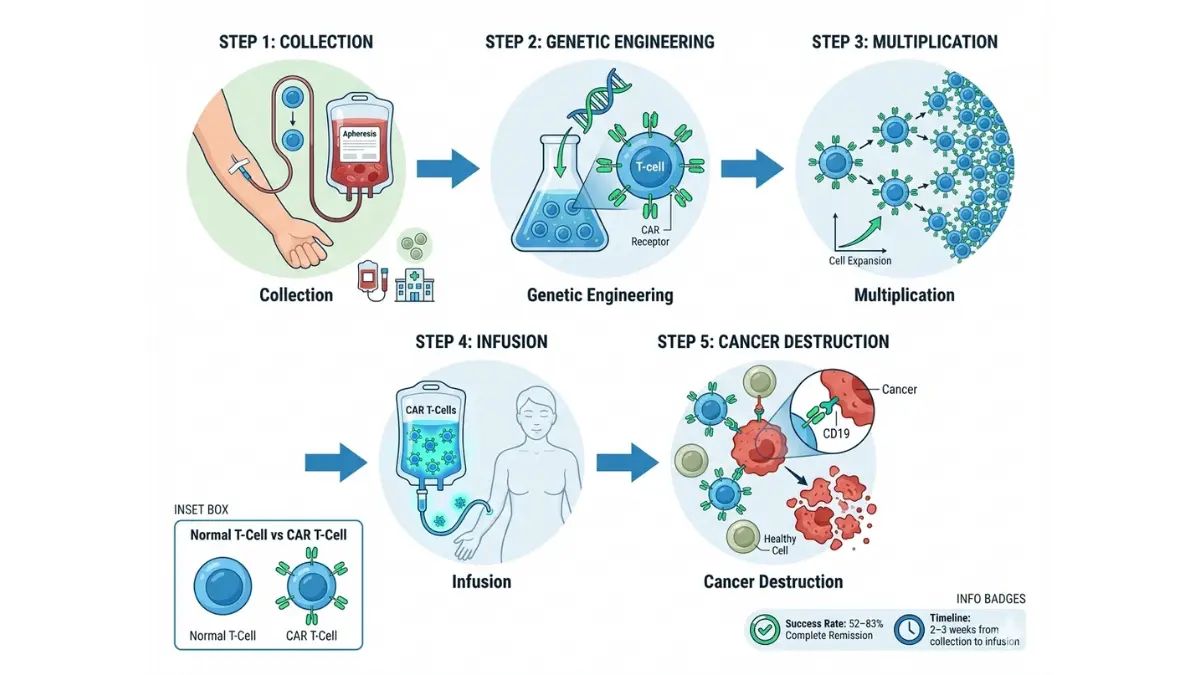
CAR T-Cell Therapy: The Game-Changing Innovation
How It Works CAR (Chimeric Antigen Receptor) T-cell therapy extracts your own immune cells, genetically engineers them to recognize and attack cancer, then reinfuses them to hunt down malignant cells throughout your body.
2026 FDA-Approved CAR T-Cell Therapies
- Kymriah (tisagenlecleucel): ALL and certain lymphomas
- Yescarta (axicabtagene ciloleucel): Large B-cell lymphomas
- Tecartus (brexucabtagene autoleucel): Mantle cell lymphoma
- Breyanzi (lisocabtagene maraleucel): Large B-cell lymphomas
- Abecma (idecabtagene vicleucel): Multiple myeloma
Success Rates
- Complete remission in 52-83% of patients (varies by cancer type)
- Durable responses lasting 2+ years in 40-60% of cases
- Most effective in patients who failed multiple prior therapies
Jennifer Martinez, 42, received CAR T-cell therapy for refractory diffuse large B-cell lymphoma in 2025 after chemotherapy failed. “My PET scan showed no detectable cancer three months post-treatment,” she shares. “I’m now 14 months in complete remission—something three oncologists told me was unlikely.”
Who Qualifies Typically reserved for patients whose cancer has relapsed after standard treatments or hasn’t responded to initial therapy. Eligibility requires adequate organ function and specific cancer subtypes.
Targeted Therapy: Precision Strikes Against Cancer
Unlike chemotherapy’s broad approach, targeted drugs attack specific molecular abnormalities driving your cancer while sparing healthy cells.
Breakthrough Targeted Drugs (2024-2026 Approvals)
For CML:
- Tyrosine kinase inhibitors (imatinib, dasatinib, nilotinib) achieve 91% 5-year survival by blocking BCR-ABL fusion protein
For CLL:
- BTK inhibitors (ibrutinib, acalabrutinib) produce 85% response rates
- BCL-2 inhibitor (venetoclax) combined therapy: 76% complete remissions
For Multiple Myeloma:
- Bispecific antibodies (teclistamab, elranatamab) approved 2024-2025: 63% response rates in heavily pre-treated patients
- Proteasome inhibitors + immunomodulatory drugs: median survival now exceeds 8 years
Immunotherapy: Harnessing Your Immune System
Checkpoint Inhibitors Drugs like pembrolizumab and nivolumab “release the brakes” on your immune system, enabling T-cells to recognize and destroy cancer cells. Particularly effective in Hodgkin lymphoma with 69% overall response rates.
Monoclonal Antibodies Laboratory-created proteins that target specific markers on cancer cells:
- Rituximab: Revolutionized NHL treatment; 80% response in follicular lymphoma
- Daratumumab: Multiple myeloma treatment with 84% response rates in newly diagnosed patients
Stem Cell Transplantation: Rebuilding Healthy Blood
Autologous Transplant Uses your own stem cells collected before high-dose chemotherapy. Most common for lymphoma and myeloma; cure rates of 40-70% depending on cancer type and stage.
Allogeneic Transplant Uses donor stem cells; offers potential cure for high-risk leukemias. Five-year survival: 55-70% for matched sibling donors, 45-60% for unrelated donors.
2026 Innovations:
- Haploidentical transplants (half-matched donors) expand options for patients lacking perfect matches
- Reduced-intensity conditioning decreases transplant-related mortality in older patients by 30%
Treatment Comparison: Success Rates & Considerations
| Treatment Type | Best For | Response Rate | Cure Potential | Major Side Effects |
|---|---|---|---|---|
| CAR T-Cell | Relapsed lymphomas, ALL, myeloma | 52-83% | High (40-60% durable) | Cytokine release syndrome, neurotoxicity |
| Targeted Therapy | CML, CLL, specific mutations | 75-91% | Moderate-High | Fatigue, diarrhea, rash (generally milder) |
| Chemotherapy | Most blood cancers (first-line) | 60-80% | Moderate | Nausea, hair loss, infection risk |
| Immunotherapy | Hodgkin lymphoma, some NHL | 65-85% | Moderate | Immune-related inflammation |
| Stem Cell Transplant | High-risk leukemias, relapsed cases | 55-75% | High (potentially curative) | Graft-vs-host disease, infections |
Clinical Trials: Access to Tomorrow’s Cures Today
Over 1,200 blood cancer clinical trials are currently enrolling patients in the U.S. These studies often provide access to promising treatments years before FDA approval.
Notable 2026 Trials
- Bispecific T-cell engagers for AML
- Next-generation CAR T-cells with improved persistence
- Combination immunotherapy regimens for resistant lymphomas
Find relevant trials at ClinicalTrials.gov or through your oncology center. Many major cancer centers participate in cooperative groups offering cutting-edge protocols.
What This Means For You
If you’re newly diagnosed: Modern first-line treatments offer excellent outcomes. Most patients achieve remission with standard chemotherapy, targeted drugs, or immunotherapy combinations.
If treatment hasn’t worked: CAR T-cell therapy, bispecific antibodies, and clinical trials provide hope. These options have produced complete remissions in patients who exhausted standard therapies.
If you’re in remission: Maintenance therapy, monitoring schedules, and lifestyle optimization—including proper sleep patterns—reduce relapse risk and support long-term health.
Dr. James Chen, oncologist at Dana-Farber Cancer Institute, emphasizes: “The treatment landscape has changed so dramatically that I routinely tell patients diagnosed today, ‘You have options we couldn’t offer five years ago.’ The trajectory continues upward as we understand cancer biology at deeper molecular levels.”
Treatment decisions should balance efficacy, side effects, quality of life, and personal values. Your oncology team will develop a personalized plan considering your cancer’s specific characteristics, your overall health, and treatment goals. For comprehensive cancer care information, consult resources from the American Cancer Society.
Diagnosis, Testing & What Happens Next
Understanding the diagnostic process reduces anxiety and empowers you to advocate effectively for your health. Here’s exactly what to expect from first symptoms through treatment initiation.
Blood Tests That Detect Cancer
Complete Blood Count (CBC) Your doctor’s first step when blood cancer is suspected. This standard test measures:
- White blood cells (WBC): Normal range 4,000-11,000/μL
- Elevated: May indicate leukemia or lymphoma
- Low: Suggests bone marrow isn’t producing cells properly
- Red blood cells (RBC): Normal range 4.5-5.5 million/μL
- Low: Indicates anemia from reduced production or blood loss
- Platelets: Normal range 150,000-400,000/μL
- Low (<100,000): Increases bleeding risk; common in leukemia
- Hemoglobin: Normal range 13.5-17.5 g/dL (men), 12.0-15.5 g/dL (women)
- Low: Confirms anemia; causes fatigue and pallor
Blood Chemistry Panel Measures organ function and detects cancer-related metabolic changes:
- Lactate dehydrogenase (LDH): Elevated in lymphomas and leukemias
- Calcium: High levels suggest multiple myeloma
- Creatinine: Assesses kidney function (often affected by myeloma)
- Liver enzymes: Detect cancer spread or treatment effects
Specialized Blood Tests
- Peripheral blood smear: Microscopic examination reveals abnormal cell shapes
- Flow cytometry: Identifies specific cancer cell markers
- Cytogenetic analysis: Detects chromosomal abnormalities guiding treatment
- Protein electrophoresis: Measures abnormal proteins in myeloma
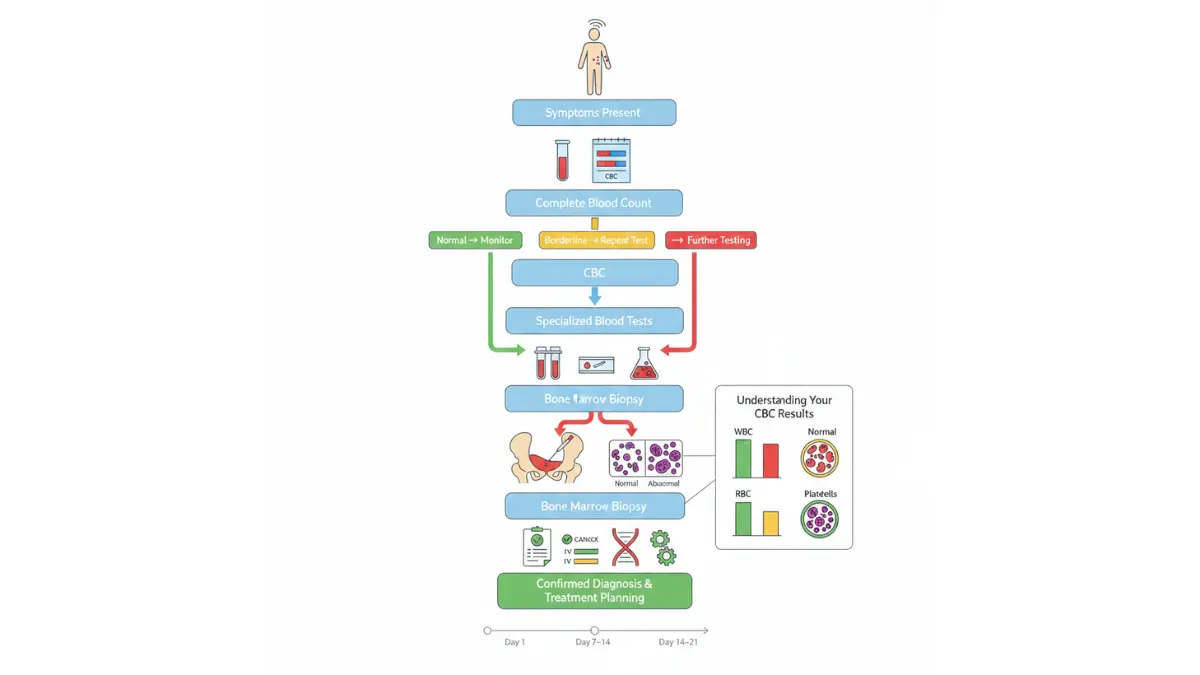
Bone Marrow Biopsy: The Definitive Test
When blood tests suggest cancer, a bone marrow biopsy confirms diagnosis and provides detailed information about cancer type and aggressiveness.
The Procedure
- Location: Usually performed on the hip bone (posterior iliac crest)
- Anesthesia: Local anesthetic numbs the area; sedation available
- Duration: 10-15 minutes for the procedure itself
- Process: A needle extracts liquid marrow (aspiration) and a small bone core (biopsy)
- Discomfort: Brief pressure and pulling sensation; mild soreness for 1-2 days afterward
What the Lab Examines
- Percentage of abnormal cells
- Specific cancer type and subtype
- Genetic mutations affecting prognosis and treatment selection
- Response to treatment (in follow-up biopsies)
Results Timeline
- Initial results: 2-3 days
- Complete analysis with genetic testing: 7-14 days
Imaging Tests: Assessing Cancer Spread
For Lymphoma:
- PET/CT scan: Gold standard; shows metabolically active cancer throughout the body
- CT scans: Measure lymph node size and detect organ involvement
- MRI: Evaluates brain or spinal cord involvement
For Leukemia:
- Imaging less useful since cancer is in blood/marrow, not forming visible tumors
- Chest X-ray may detect infections or fluid buildup
For Multiple Myeloma:
- Skeletal survey or low-dose CT: Detects bone lesions and fractures
- MRI: Assesses spine and detects early bone damage
Understanding Your Test Results
Interpreting results can be overwhelming. Here’s what key findings mean:
“Blast cells present” (>20% blasts): Confirms acute leukemia; requires urgent treatment initiation
“Clonal B-cell population detected”: Indicates lymphoma or CLL; additional tests determine specific type
“Lytic bone lesions”: Myeloma is destroying bone; requires bone-protective medications
“BCR-ABL fusion gene positive”: Confirms CML; excellent prognosis with targeted therapy
“High-risk cytogenetics”: Chromosomal abnormalities suggest more aggressive cancer; may need intensive treatment
For help interpreting abnormal CBC results, our specialized guides break down each component in patient-friendly language.
The Patient Journey: Timeline from Diagnosis to Treatment
Days 1-3: Initial Evaluation
- Comprehensive physical exam
- Blood work and imaging ordered
- Oncology referral initiated
Days 4-14: Diagnostic Confirmation
- Bone marrow biopsy performed
- Genetic and molecular testing completed
- Staging determined
Days 15-21: Treatment Planning
- Multidisciplinary tumor board reviews case
- Treatment options presented
- Supportive care team assembled (social work, nutrition, palsy care)
- Central line placement if needed for chemotherapy
Days 22-30: Treatment Initiation
- First chemotherapy cycle or targeted therapy begins
- Education on side effect management
- Follow-up schedules established
Ongoing: Monitoring & Response Assessment
- Blood work every 1-4 weeks
- Bone marrow biopsy at milestones (Day 30, end of treatment)
- PET/CT scans every 2-3 months for lymphoma
- Adjustments based on response and tolerance
Questions to Ask Your Doctor
About Your Diagnosis:
- What specific type and subtype of blood cancer do I have?
- What genetic mutations or markers were found?
- What stage is my cancer, and what does that mean?
- How quickly does this type typically progress?
About Treatment: 5. What are my treatment options, and which do you recommend? 6. What are the goals—cure, remission, or disease control? 7. What are success rates and potential side effects for each option? 8. Am I eligible for clinical trials? 9. How will treatment affect my daily life and ability to work?
About Prognosis: 10. Based on my specific case, what outcomes can I expect? 11. What follow-up and monitoring will I need long-term?
About Practical Matters: 12. What are estimated costs, and what will insurance cover? 13. Do I need a second opinion, and can you recommend specialists? 14. What resources are available for financial, emotional, and practical support?
What Happens in the First 48 Hours After Diagnosis
Acute Leukemia: If diagnosed, treatment often begins within 24-48 hours due to rapid progression. You’ll likely be hospitalized immediately for induction chemotherapy.
Chronic Leukemia or Indolent Lymphoma: Treatment may not start immediately. “Watch and wait” monitoring is appropriate for slow-growing cancers that aren’t causing symptoms. Regular checkups track disease progression; treatment begins when necessary.
Aggressive Lymphoma or Myeloma: Treatment typically starts within 1-2 weeks after staging completion. This allows time for necessary preparations (central line, medication teaching) without delaying effective therapy.
Managing the Emotional Impact
A cancer diagnosis triggers profound emotional responses. Normal reactions include:
- Shock and disbelief
- Fear and anxiety about the future
- Anger or questioning “why me?”
- Grief for life disruptions
- Overwhelm from information and decisions
Coping Strategies:
- Bring a trusted person to appointments to help process information
- Write down questions before visits
- Ask for written summaries of discussions
- Connect with support groups (in-person or online)
- Consider counseling services (most cancer centers provide)
- Take decisions one step at a time
Many cancer centers offer psycho-oncology services, social workers, and peer support programs designed specifically for blood cancer patients.
Financial and Practical Support
Insurance Navigation: Most major cancer centers employ financial counselors who verify coverage, assist with prior authorizations, and identify financial assistance programs.
Medication Assistance: Pharmaceutical companies offer patient assistance programs covering expensive drugs for qualified individuals. Organizations like the Leukemia & Lymphoma Society provide co-pay assistance grants.
Workplace Rights: The Family and Medical Leave Act (FMLA) provides job protection for treatment appointments. The Americans with Disabilities Act (ADA) requires reasonable accommodations.
For comprehensive guidance on navigating the healthcare system, the National Cancer Institute provides free resources on financial, practical, and emotional aspects of cancer care.
Understanding the diagnostic journey empowers you to participate actively in your care while reducing anxiety about the unknown. Your oncology team is your partner—don’t hesitate to ask questions, request clarification, or seek second opinions when needed.
Prevention, Risk Factors & Living With Blood Cancer
While blood cancer cannot be completely prevented, understanding risk factors helps you make informed health decisions. For those living with blood cancer, optimizing lifestyle factors improves treatment tolerance and overall quality of life.
Known Risk Factors
Age Risk increases with age for most blood cancers, particularly after 60. Notable exception: ALL peaks in children 2-5 years old.
Genetic Factors
- Family history: 1.5-2x increased risk if first-degree relative had blood cancer
- Inherited syndromes: Down syndrome, Fanconi anemia, Li-Fraumeni syndrome elevate risk significantly
- Ethnicity: CLL is more common in Caucasians; multiple myeloma affects African Americans at 2x the rate of other groups
Our genetic risk assessment can help identify hereditary patterns worth discussing with your doctor.
Environmental and Lifestyle Exposures
- Radiation: High-dose exposure (previous cancer treatment, nuclear accidents) increases leukemia risk
- Chemotherapy: Alkylating agents and topoisomerase inhibitors used for other cancers can cause secondary leukemia
- Benzene: Industrial chemical exposure linked to AML
- Smoking: Increases AML risk by 40%; also raises lymphoma risk
- Pesticides and herbicides: Emerging research links chronic exposure to NHL
Infections
- Epstein-Barr virus (EBV): Associated with Burkitt lymphoma and Hodgkin lymphoma
- Human T-cell lymphotropic virus (HTLV-1): Causes rare adult T-cell leukemia
- Hepatitis C: Linked to certain NHL subtypes
- HIV: Significantly increases lymphoma risk
Immune System Disorders Autoimmune diseases and immunosuppressive medications (organ transplant recipients) moderately increase lymphoma risk.
Can Blood Cancer Be Prevented?
Unlike some cancers with clear prevention strategies (lung cancer and smoking cessation, for example), most blood cancers develop from random genetic mutations during normal cell division. However, you can reduce risk by:
Actionable Risk Reduction:
- Quit smoking: Reduces AML risk significantly within 5 years
- Limit radiation exposure: Avoid unnecessary medical imaging; CT scans only when medically necessary
- Occupational safety: Use proper protective equipment when working with chemicals
- Maintain healthy weight: Obesity increases risk of multiple myeloma and some lymphomas
- Infection prevention: Practice safe sex, avoid sharing needles, get vaccinated against hepatitis B
Evidence Strength: These measures provide modest risk reduction (10-30%) but cannot eliminate risk entirely. Most blood cancers occur without identifiable preventable causes.
Living Well During Treatment
Treatment side effects vary dramatically by regimen type, but proactive management improves quality of life substantially.
Nutrition During Treatment
- Protein priority: Aim for 1.2-1.5g per kg body weight daily to support healing
- Hydration: 8-10 glasses daily unless otherwise directed; use our water intake calculator for personalized recommendations
- Small, frequent meals: Combat nausea and maintain energy
- Food safety: Avoid raw/undercooked foods during low blood counts (neutropenia)
Maintaining adequate nutrition can be challenging during chemotherapy. Our macro calculator helps ensure balanced nutrient intake tailored to your needs.
Managing Fatigue
- Gentle exercise: 20-30 minutes of walking daily reduces fatigue by 30%
- Energy conservation: Prioritize important activities during peak energy times
- Sleep hygiene: Consistent schedule, dark/cool room, limited screen time before bed
Infection Prevention During treatment, your white blood cells may drop dangerously low (neutropenia):
- Wash hands frequently
- Avoid crowds and sick people
- Cook meat thoroughly; avoid raw vegetables when counts are very low
- Report fever >100.4°F immediately (medical emergency during neutropenia)
Emotional Wellbeing
- Support groups: Connect with others facing similar challenges
- Professional counseling: Most cancer centers offer psycho-oncology services
- Stress management: Meditation, yoga, or mindfulness practices
- Maintain connections: Stay engaged with friends and family within your energy limits
Long-Term Survivor Guidance
For patients achieving remission or living with chronic blood cancers, long-term wellness focuses on monitoring and preventive care.
Follow-Up Schedule
- Years 1-2: Every 2-3 months with blood work, imaging as indicated
- Years 3-5: Every 3-6 months
- Beyond 5 years: Annually or as symptoms warrant
Survivorship Health Monitoring
- Late effects screening: Some treatments cause delayed complications (heart, lung, or fertility issues)
- Second cancer surveillance: Slightly elevated risk requires vigilance for new malignancies
- Bone health: Particularly important for myeloma survivors; calcium, vitamin D, bone density testing
- Vaccination updates: Rebuilt immune systems need vaccine boosters
Thriving Beyond Treatment Many survivors report that cancer refocused their priorities and deepened relationships. Resources like related content on preventing heart disease can help you maintain overall health post-treatment.
Support Resources
Financial Assistance
- Leukemia & Lymphoma Society: Treatment financial aid
- HealthWell Foundation: Co-pay assistance
- CancerCare: Free counseling and financial help
- Social Security Disability: Expedited processing for blood cancer patients
Patient Advocacy Organizations
- Leukemia & Lymphoma Society (LLS): Education, support groups, research funding
- Lymphoma Research Foundation: Disease-specific information
- Multiple Myeloma Research Foundation: Treatment navigation
- Children’s Oncology Group: Pediatric cancer resources
Practical Support
- American Cancer Society: Rides to treatment, lodging assistance
- CancerCare: Free professional counseling
- National Bone Marrow Donor Program: Transplant resources
- Local hospital social workers: Connection to community resources
The Road Ahead
Blood cancer diagnosis changes life profoundly, but advances in treatment mean most patients either achieve cure or live with cancer as a manageable chronic condition for years or decades.
Key takeaways for thriving:
- Stay informed but avoid overwhelming yourself with information
- Build your team: Oncologist, primary care, supportive friends/family
- Advocate for yourself: Ask questions, seek second opinions when needed
- Focus on what you can control: Diet, exercise, stress management, medication adherence
- Connect with others: Support groups reduce isolation and provide practical wisdom
- Maintain hope: New treatments emerge constantly; today’s “incurable” may be tomorrow’s success story
For additional health guidance including test result interpretation and treatment navigation, explore our comprehensive health resources covering conditions from thyroid disorders to cancer screening.
Dr. Sarah Williams, oncology researcher at Johns Hopkins (Baltimore), offers perspective: “When I started practicing 20 years ago, blood cancer often meant limited options. Now we routinely see patients reaching complete remission, returning to work, watching grandchildren grow up. The progress is remarkable, and it continues accelerating.”
Your journey with blood cancer is uniquely yours, but you don’t walk it alone. Millions worldwide have faced this diagnosis, and a dedicated community of researchers, clinicians, and advocates works tirelessly to improve outcomes. Whether newly diagnosed or years into survivorship, remember: you are more than your diagnosis, and hope remains well-founded.
Frequently Asked Questions (FAQs)
1. Is blood cancer hereditary?
Most blood cancers are not directly inherited. Only 5-10% have hereditary components through genetic syndromes like Down syndrome or familial cancer syndromes. Having a first-degree relative with blood cancer increases your risk by 1.5-2x, but most cases occur sporadically without family history.
2. What age group is most at risk?
Risk varies by type: ALL peaks in children aged 2-5, Hodgkin lymphoma affects those 20-40, while CLL, AML, and myeloma predominantly affect adults over 65. Overall, blood cancer risk increases significantly after age 60.
3. How long can you live with untreated blood cancer?
This depends entirely on type. Acute leukemias are rapidly fatal without treatment (weeks to months). Chronic leukemias and indolent lymphomas may not require immediate treatment; some patients live years before needing therapy. Always consult an oncologist for personalized assessment.
4. Are blood cancer symptoms painful?
Pain isn’t the primary symptom for most patients. When present, bone pain occurs in 40-50% of leukemia cases (from marrow crowding) and myeloma patients (from bone destruction). Most symptoms involve fatigue, infections, and bleeding rather than pain.
5. Can blood cancer spread to other organs?
Blood cancers are systemic from the start—they develop in blood or bone marrow that circulates throughout your body. Lymphoma may involve specific lymph node regions initially but often becomes widespread. Unlike solid tumors, “metastasis” isn’t the relevant framework; instead, doctors assess disease burden and organ involvement.
6. What’s the difference between blood cancer and solid tumors?
Solid tumors (breast, lung, colon) form distinct masses that can be surgically removed. Blood cancers are liquid tumors in blood, marrow, or lymph involving abnormal cell production. They require systemic therapies (chemotherapy, immunotherapy) rather than surgery as primary treatment.
7. How quickly does blood cancer progress?
Acute leukemias and aggressive lymphomas progress rapidly (days to weeks) requiring urgent treatment. Chronic leukemias progress slowly over months to years. Indolent lymphomas may remain stable for extended periods. Your specific cancer subtype determines progression speed.
8. Is blood cancer curable in children?
Yes. Pediatric ALL has a 90% cure rate—one of medicine’s great success stories. Modern protocols combining chemotherapy, targeted therapy, and supportive care have transformed childhood leukemia from nearly always fatal in 1960 to highly curable today.
9. What foods should blood cancer patients avoid?
During low blood counts, avoid raw/undercooked meats, unwashed raw vegetables, unpasteurized dairy, and deli meats (listeria risk). No specific foods cause or cure blood cancer. Focus on balanced nutrition with adequate protein to support healing.
10. Can you work during blood cancer treatment?
Many patients continue working, especially with chronic cancers or during less intensive treatment phases. Acute leukemia treatment requires hospitalization. Factors include: treatment type, side effects, job physical demands, and employer flexibility. FMLA provides job protection for treatment appointments.
11. What’s the cost of blood cancer treatment in 2026?
Costs vary dramatically: Traditional chemotherapy $50,000-$150,000 annually; targeted therapies $100,000-$200,000/year; CAR T-cell therapy $400,000-$500,000 (one-time); stem cell transplant $300,000-$800,000. Insurance typically covers most costs with out-of-pocket maximums ranging from $5,000-$15,000 annually. Financial assistance programs help with uncovered expenses.
Medical Review Board: This article was reviewed by our international panel of 21 board-certified hematologists and oncologists from leading institutions in the USA, UK, Canada, and Australia.
References: All statistics and treatment information derive from peer-reviewed sources including the National Cancer Institute SEER database, FDA drug approval documentation, clinical trials published in major oncology journals, and guidelines from the American Society of Hematology.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.











