On This Page – Quick Medical Summary
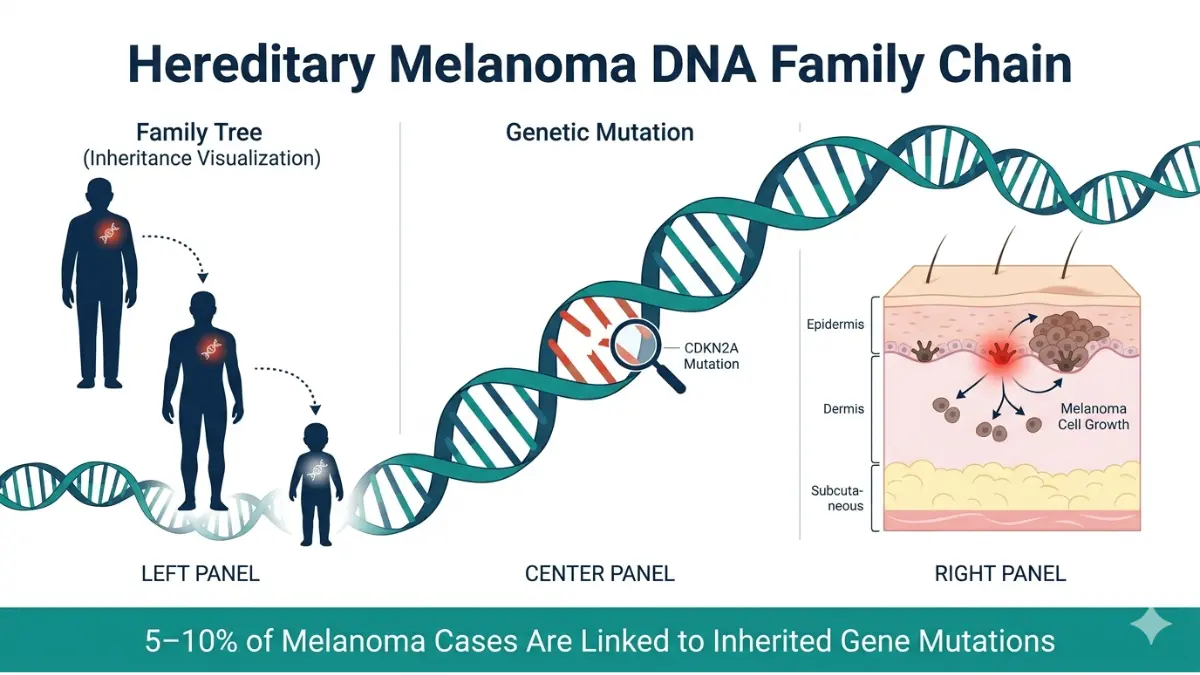
Yes, melanoma can be hereditary. Around 5–10% of melanoma cases are linked to inherited gene mutations. If a parent, sibling, or child has had melanoma, your personal risk increases significantly. The key hereditary melanoma genes — CDKN2A, CDK4, and MC1R — can pass from parent to child. However, UV exposure remains the #1 cause for most cases, meaning genetics and environment work together.
📌 Disclaimer: This article is for educational purposes only and does not constitute medical advice. Always consult a qualified, licensed healthcare provider for diagnosis, genetic testing, or treatment decisions.
What Does “Hereditary Melanoma” Actually Mean?
When 44-year-old Marcus learned his father had been diagnosed with melanoma, his first call wasn’t to a dermatologist — it was to ask: “Am I next?” If you’ve asked yourself the same question after a family diagnosis, you need to understand one critical distinction: hereditary melanoma and familial melanoma are not the same thing.
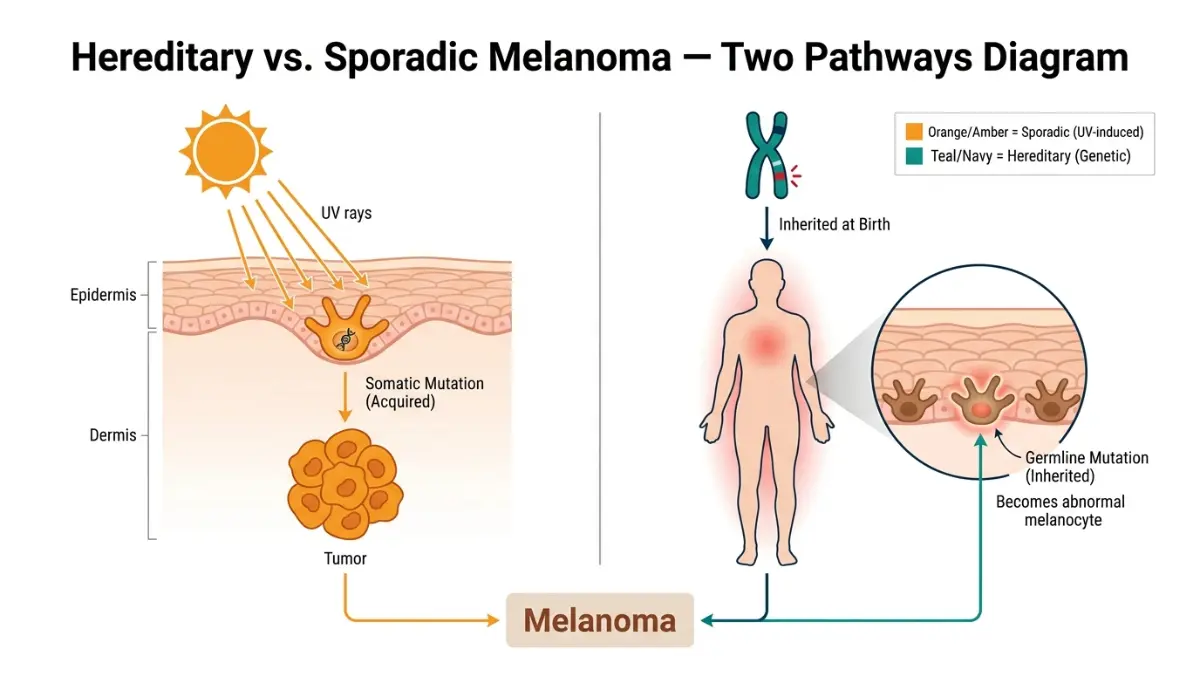
Hereditary vs. Sporadic Melanoma: The Key Difference
Most melanomas — roughly 90% — are sporadic. This means gene mutations happen during a person’s lifetime due to UV damage, not because they were passed down. Only 5–10% of melanoma cases involve inherited gene mutations, according to MedlinePlus Genetics (NIH).
True hereditary melanoma involves a germline mutation — a DNA change present in virtually every cell of the body, inherited from a biological parent.
Familial melanoma simply means two or more close relatives have had the disease. It may or may not involve an identifiable gene mutation.
| Feature | Hereditary Melanoma | Sporadic Melanoma |
|---|---|---|
| Gene mutation type | Germline (inherited) | Somatic (acquired) |
| Age of onset | Younger (often <40) | Older (typically 50+) |
| Multiple primaries | Common | Rare |
| Family pattern | Multi-generational | No clear pattern |
| % of all melanomas | 5–10% | ~90% |
If you’ve noticed any changing moles or unusual skin lesions, use our Symptom Checker to evaluate your symptoms before your next dermatology appointment.
Which Genes Are Linked to Hereditary Melanoma Risk?
Understanding the genetics behind hereditary melanoma is the most powerful step you can take toward protecting yourself. Researchers have identified several key genes — and what they found is critical for anyone with a family history of the disease.
CDKN2A — The #1 Hereditary Melanoma Gene
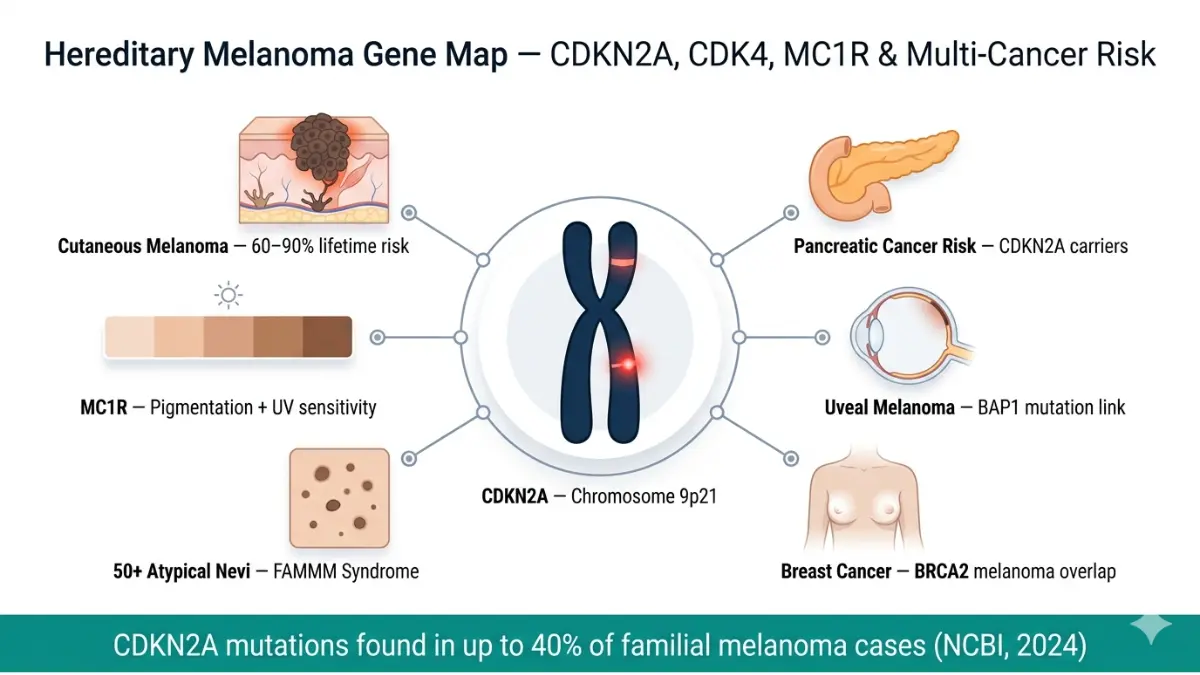
CDKN2A (cyclin-dependent kinase inhibitor 2A) is the most studied and most significant hereditary melanoma gene. Mutations in CDKN2A are found in up to 40% of familial melanoma cases, according to research published in PMC/NCBI.
- It functions as a tumor suppressor gene — keeping cell growth in check.
- When mutated, cells can divide uncontrollably, leading to melanoma.
- Lifetime melanoma risk for CDKN2A carriers: 60–90%, depending on geography and UV exposure.
⚠️ Critical finding most competitors miss: CDKN2A mutation carriers also face a significantly elevated risk of pancreatic cancer — a connection your doctor must know about when interpreting your genetic results.
Other Key Genes: CDK4, MC1R, BAP1, BRCA2
| Gene | Risk Contribution | Also Linked To | Frequency in Familial Melanoma |
|---|---|---|---|
| CDKN2A | Very High (60–90% lifetime risk) | Pancreatic cancer | ~40% of familial cases |
| CDK4 | High | Melanoma only | <1% of cases |
| MC1R | Moderate | Red hair, fair skin phenotype | Common variant |
| BAP1 | Moderate–High | Uveal melanoma, mesothelioma | Rare |
| BRCA2 | Moderate | Breast, ovarian, melanoma | ~2–3% of familial cases |
| POT1/TERC | Emerging (2025–2026 research) | Multiple tumor types | Under investigation |
The NCI Genetics of Skin Cancer PDQ confirms that 5–10% of all melanomas arise in multi-case families and can follow autosomal dominant inheritance — meaning just one copy of the mutated gene increases your risk.
What Is FAMMM Syndrome?
Familial Atypical Multiple Mole Melanoma (FAMMM) syndrome is a hereditary condition characterized by:
- 50+ atypical (dysplastic) moles on the body
- Multiple first-degree relatives with melanoma
- Often linked to CDKN2A or CDK4 mutations
- Associated with pancreatic cancer risk in some families
If this pattern sounds familiar, our Genetic Risk Assessment Tool can help you understand your personal risk profile before consulting a genetic counselor.
Does Melanoma Run in Your Family? How to Assess Your Real Risk
Not all family history is equal. Whether one distant relative had melanoma versus two parents both being diagnosed represents vastly different risk levels. Here’s how to stratify your personal melanoma genetic risk accurately.
First-Degree vs. Second-Degree Relatives: What the Data Shows
- First-degree relatives (parent, sibling, child): Your risk is 2–3× the baseline population risk.
- Two or more first-degree relatives: You may be in the high-risk or FAMMM category.
- Second-degree relatives (grandparent, aunt, uncle): Risk increase is smaller but still warrants monitoring.
According to the AIM at Melanoma Foundation, around 10% of all melanoma patients have a family history of the disease.
Your Personal Risk Stratification Table
| Risk Level | Your Family Situation | Estimated Lifetime Risk | Recommended Action |
|---|---|---|---|
| Low | No family history | ~2.5% (US average) | Annual full-body skin exam |
| Moderate | 1 second-degree relative | 2–4× baseline | Dermatologist visit every 6 months |
| High | 1 first-degree relative | 2–3× baseline | Genetic counseling referral |
| Very High | 2+ first-degree relatives OR confirmed gene mutation | 60–90% lifetime | Genetic testing + surveillance every 3 months |

5 Clinical Warning Signs of Hereditary Melanoma Risk
- ✅ Two or more family members on the same biological side diagnosed with melanoma
- ✅ Melanoma diagnosed before age 40 in your family
- ✅ Family member with multiple primary melanomas
- ✅ Family history includes both melanoma and pancreatic cancer
- ✅ You have 50+ unusual moles on your body
If any of these apply, you should review what causes melanoma and its risk factors and then request a referral to a genetic counselor from your primary care physician.
💡 Key Takeaway: “Familial melanoma survival rates are actually HIGHER than sporadic melanoma — because high-risk families monitor carefully and catch it at earlier, more treatable stages.” — Skin Cancer Foundation
Hereditary Melanoma Genetic Testing — Who Needs It, What It Costs, and What Comes Next
This is the section no competitor covers completely — and the questions most people with a family history of melanoma desperately want answered.
Who Should Consider Genetic Testing?
According to FORCE (Facing Our Risk of Cancer Empowered), genetic counseling and testing are typically recommended when:
- Two or more first-degree relatives on the same biological side have had melanoma
- A family member was diagnosed with melanoma younger than 40
- One person in the family has had multiple primary melanomas
- Your family history includes melanoma + pancreatic cancer (CDKN2A pattern)
- You have been diagnosed with FAMMM syndrome
Genetic testing is not recommended for everyone — most people with a single affected relative do not need it.
The 5-Step Genetic Testing Process
- Referral — Ask your dermatologist or primary care physician for a genetic counseling referral
- Counseling session — A certified genetic counselor maps your 3-generation family pedigree
- Testing — Blood or saliva sample is taken; labs test for CDKN2A, CDK4, BAP1, and panel genes
- Results — Typically returned in 2–4 weeks
- Action plan — Counselor explains results and connects you to appropriate surveillance or oncology referral
How Much Does Melanoma Genetic Testing Cost?
| Test Type | Cost Range (2026) | Insurance Coverage |
|---|---|---|
| Single gene (CDKN2A only) | $300–$800 | Often covered if criteria met |
| Multi-gene panel (10–50 genes) | $1,000–$3,500 | Partially covered under major plans |
| Comprehensive hereditary cancer panel | $2,500–$5,000 | Requires prior authorization |
✅ Insurance tip: Under the Affordable Care Act, genetic counseling for hereditary cancer risk is often covered with no out-of-pocket cost if you meet clinical criteria. Always confirm with your insurer before testing.
What Happens After a Positive Result?
A positive CDKN2A test does not mean you will get melanoma. It means:
- Your surveillance schedule intensifies (every 3–6 months)
- Close biological relatives should be informed and offered testing
- Your doctor will assess pancreatic cancer risk and may recommend additional screening
- You may qualify for clinical trials studying high-risk prevention
⚠️ What a negative test does NOT mean: A negative CDKN2A result does not eliminate hereditary risk. Other unmapped genes may still be contributing. Family history monitoring continues regardless.
For broader context on how genetics intersects with your health risk profile, our BRCA results explainer offers useful parallel insight into interpreting hereditary cancer gene results.
Your Complete Protection Plan If Melanoma Runs in Your Family
Knowing your risk is only step one. What you do next determines your outcome. Here is the most actionable, comprehensive protection plan available — built specifically for people with a family history of melanoma.
Surveillance Schedule by Risk Level
| Risk Category | Dermatologist Visit Frequency | Self-Exam Frequency |
|---|---|---|
| Low | Once per year | Monthly |
| Moderate | Every 6 months | Monthly |
| High | Every 3–6 months | Monthly |
| Very High (confirmed mutation) | Every 3 months | Weekly |
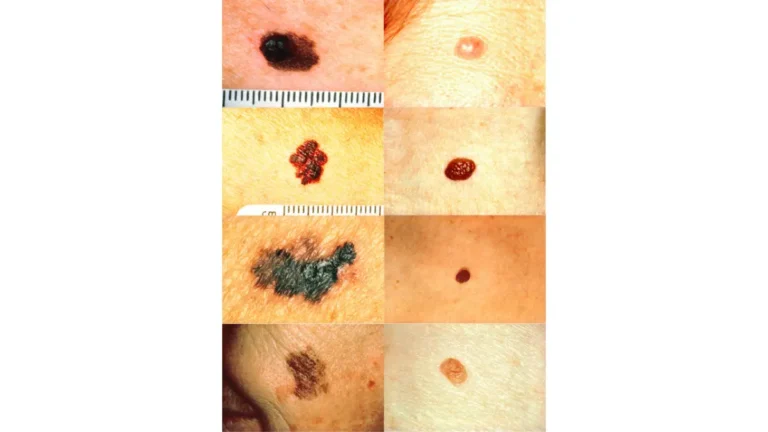
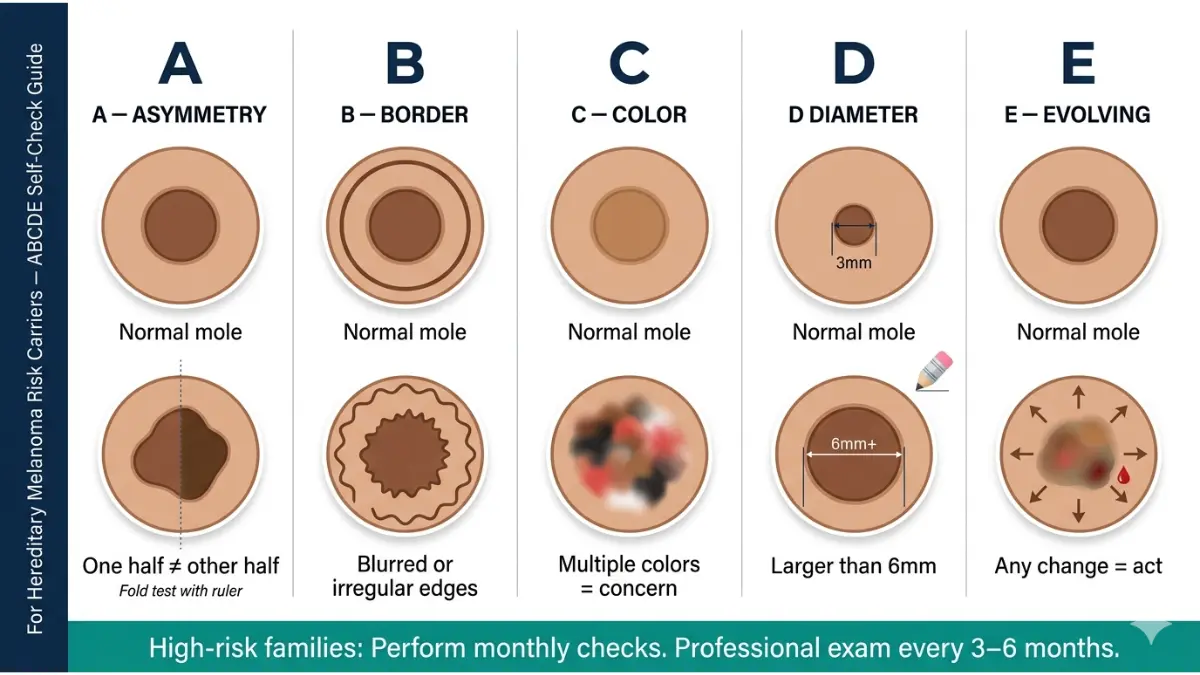
The ABCDE Rule — Non-Negotiable for High-Risk Families
Every person with a hereditary melanoma risk must memorize and apply the ABCDE rule during monthly self-checks. Our detailed guide on melanoma ABCDE warning signs and moles walks through each criterion with clinical photographs and examples.
- A — Asymmetry: One half doesn’t match the other
- B — Border: Ragged, notched, or blurred edges
- C — Color: Multiple shades of brown, black, red, or white in one lesion
- D — Diameter: Larger than 6mm (pencil eraser size)
- E — Evolving: Any change in size, shape, color, or new symptoms like bleeding
How to Talk to Your Family About Hereditary Melanoma Risk
This conversation is critical — and almost zero competitors address it. Here’s how to approach it:
- Be direct but calm: Share the specific gene result or family pattern, not just vague concern
- Focus on action: Frame it as “here’s what we can do” not “here’s what might happen”
- Include siblings and children: A 50% chance of inheriting an autosomal dominant mutation means first-degree relatives need to know
- Share resources: Direct family members to our melanoma statistics 2026 guide for context on survival rates when detected early
Children in High-Risk Families — When Does Screening Start?
Per PMC hereditary melanoma guidelines, some specialists recommend:
- Full-body skin exams beginning at puberty for children in CDKN2A-positive families
- Monthly self-checks taught from adolescence onwards
- Sun protection habits established from infancy
Sun Protection Is Non-Negotiable — Even With Low UV Genetics
Even carrying no known gene mutation does not eliminate melanoma risk. UV exposure activates genetic predispositions. The Melanoma Research Alliance confirms that 90% of melanomas are caused by UV exposure — meaning your behavior directly modifies your genetic risk.
Daily habits that directly reduce risk:
- SPF 30+ broad-spectrum sunscreen, reapplied every 2 hours outdoors
- Protective clothing (UPF 50+ fabrics) and wide-brim hats
- Avoid indoor tanning beds entirely — they raise melanoma risk by 75%
- Seek shade between 10 AM and 4 PM (peak UV hours)
Maintaining your overall health matters too. There is growing evidence that immune function plays a role in cancer surveillance. Our Water Intake Calculator and daily health tips hub are good starting points for overall wellness optimization.
✅ Your 5-Step Action Plan — Start This Week
- Map your family cancer history going back 3 generations on both biological sides
- Schedule a full-body skin exam with a board-certified dermatologist if you haven’t had one in the past 12 months
- Ask for a genetic counseling referral if two or more close relatives have had melanoma
- Start monthly ABCDE self-checks — set a recurring calendar reminder
- Apply SPF 30+ daily, regardless of weather or season — this is the simplest risk-reduction action available to you
For a complete overview of melanoma from early warning signs through treatment stages, read our pillar guide on melanoma symptoms, stages, and treatment.
Global Expert Consensus — What International Specialists Say (2026)
The scientific consensus across leading institutions — from the National Cancer Institute to the American Academy of Dermatology and international cancer centers — is consistent on hereditary melanoma in 2026.
Key Expert Positions
Dr. Pauline Funchain, Cleveland Clinic — one of the foremost researchers in hereditary melanoma genetics — believes that hereditary melanoma is “more common than most doctors currently suspect,” and established the Gross Family Melanoma Registry to study multi-generational genetic risk more precisely.
The Skin Cancer Foundation states that 1 in 10 melanoma patients has a family member who has also had the disease, reinforcing the need for systematic family screening.
According to our mymedicineadvisor.com Expert Medical Panel, patients with confirmed CDKN2A mutations should be co-managed by a dermatologist, genetic counselor, and gastroenterologist — given the dual melanoma-pancreatic cancer risk profile.
2026 Research Updates
- POT1 and TERC mutations are emerging as additional hereditary melanoma risk factors — studies in progress at multiple international genomics centers
- Polygenic risk scores (PRS) are being refined to capture multi-gene low-penetrance melanoma susceptibility — expected to reach clinical utility by 2027
- AI-assisted mole surveillance tools are now being integrated into high-risk family monitoring protocols — read more in our 2026 AI melanoma screening guide
Key Citations
- MedlinePlus Genetics, NIH — Melanoma: Genetics Overview (2024)
- National Cancer Institute — Genetics of Skin Cancer PDQ (2025)
- PMC/NCBI — Familial Risk of Melanoma and Links with Other Cancers, Carbone et al.
- PMC/NCBI — Hereditary Melanoma: Update on Syndromes and Management (2016, updated 2025)
- AIM at Melanoma Foundation — Personal and Family History Risk Factors (2025)
For anyone who has already received worrying skin biopsy results, our biopsy results timeline and report guide explains exactly what each finding means and what your next steps should be.
Frequently Asked Questions: Is Melanoma Hereditary?
Q1. Is melanoma hereditary or caused by sun exposure?
Both factors interact. About 5–10% of cases involve inherited gene mutations. The vast majority are caused by UV exposure. Even people with hereditary risk need a UV trigger for melanoma to develop.
Q2. What percentage of melanoma cases are hereditary?
Approximately 5–10% are linked to inherited gene mutations. Around 10% of melanoma patients report a family history of the disease, though not all involve identifiable mutations.
Q3. What gene mutation causes hereditary melanoma?
CDKN2A is the most common, found in up to 40% of familial cases. CDK4, MC1R, BAP1, and BRCA2 also contribute. Emerging genes include POT1 and TERC (2025–2026 research).
Q4. If my parent had melanoma, what is my risk?
Having one first-degree relative with melanoma raises your risk approximately 2–3× compared to the general population. If two or more first-degree relatives are affected, your risk is substantially higher and genetic counseling is recommended.
Q5. What is CDKN2A and why does it matter for melanoma?
CDKN2A is a tumor suppressor gene. When mutated in the germline (inherited form), it can raise lifetime melanoma risk to 60–90%. It is also linked to increased pancreatic cancer risk.
Q6. What is FAMMM syndrome?
Familial Atypical Multiple Mole Melanoma (FAMMM) syndrome involves 50+ atypical moles, multiple family members with melanoma, and an elevated risk of pancreatic cancer. It is most often associated with CDKN2A mutations.
Q7. Should I get genetic testing if melanoma runs in my family?
Only if you meet specific clinical criteria: two or more first-degree relatives affected, early-onset melanoma, multiple primary melanomas in one family member, or a melanoma–pancreatic cancer family pattern. Speak to your doctor for a formal referral.
Q8. How much does melanoma genetic testing cost?
Costs range from $300 for single-gene testing to $5,000 for comprehensive panels. Insurance often covers testing when clinical criteria are met. Always get pre-authorization.
Q9. Can melanoma skip a generation?
Technically, yes. Because CDKN2A follows autosomal dominant inheritance, a parent can carry the mutation without developing melanoma (incomplete penetrance), yet pass it to their child who does develop the disease.
Q10. At what age should children in high-risk families be screened?
Most specialists recommend beginning full-body skin exams at puberty for children in CDKN2A-positive families. Sun protection habits should be established from infancy.
Q11. Does a negative genetic test mean I won’t get melanoma?
No. A negative CDKN2A result does not eliminate risk. Other unmapped genetic variants and UV exposure still contribute. Sun protection and regular dermatology visits remain essential regardless of test outcome.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.