On This Page – Quick Medical Summary
Mohs surgery IS a recognized, guideline-approved treatment for melanoma — but only for specific types and stages. As of the 2023/2024 NCCN guidelines, it is considered a first-line option for melanoma in situ, lentigo maligna melanoma, and thin melanomas (≤0.8mm Breslow depth) located on the face, scalp, or neck. For invasive or advanced melanoma, standard wide local excision with lymph node staging remains the primary approach.
Marcus, a 64-year-old retired firefighter from Phoenix, was told he needed a wide excision on his nose after a melanoma in situ diagnosis. The proposed surgery would have removed a large patch of skin and left significant scarring. His dermatologist at a university center offered a different path: Mohs micrographic surgery (MMS) — a tissue-sparing technique that removed every cancer cell while preserving nearly all surrounding healthy skin.
He was tumor-free at his 18-month follow-up.
If you or someone you love has received a melanoma diagnosis, understanding when Mohs surgery is the right choice — and when it isn’t — could change your treatment outcome and quality of life.
What Is Mohs Surgery and Why Does It Matter for Melanoma?
Mohs micrographic surgery is a precision skin cancer removal technique where the surgeon removes cancer one microscopic layer at a time and examines 100% of the surgical margin in real time before proceeding.
It was developed in the 1930s by Dr. Frederic Mohs at the University of Wisconsin and has evolved dramatically since then. For decades, Mohs surgery was the gold standard for basal cell carcinoma and squamous cell carcinoma — but its role in melanoma was debated.
That debate has largely shifted in 2026.
Why the shift? The introduction of MART-1 and SOX-10 immunohistochemical stains solved the historic problem: melanoma cells were previously difficult to detect on frozen section slides. These stains make melanocytes highly visible under the microscope, enabling near-100% accuracy in detecting residual tumor at the margin.
As UCLA Health reported in 2026, Mohs surgery for melanoma has gone from being “questioned with skepticism to now being incorporated in the new guidelines for care and considered first-line in some cases.”
Understanding your full diagnosis is the foundation of every treatment decision. Use our comprehensive guide to melanoma symptoms, stages, and treatment options to build that foundation before your next specialist appointment.
How Mohs Surgery Works — Step by Step
Mohs surgery is performed as an outpatient procedure under local anesthesia. No general anesthesia. No overnight hospital stay.
Here is exactly what happens during a Mohs surgery session for melanoma:
- Local anesthesia is administered to the tumor site. The area is fully numbed.
- The surgeon removes a thin layer of tissue around the visible tumor and maps it precisely — a 360-degree margin map.
- The patient waits (typically 45–90 minutes) while the tissue is processed and examined under a microscope in the on-site Mohs lab.
- If cancer cells are detected at any margin, the surgeon returns to that exact location only and removes another targeted layer.
- The cycle repeats until all margins are completely clear — confirmed microscopically before the patient leaves.
- Reconstruction is performed the same day, often by the Mohs surgeon or a plastic surgeon.
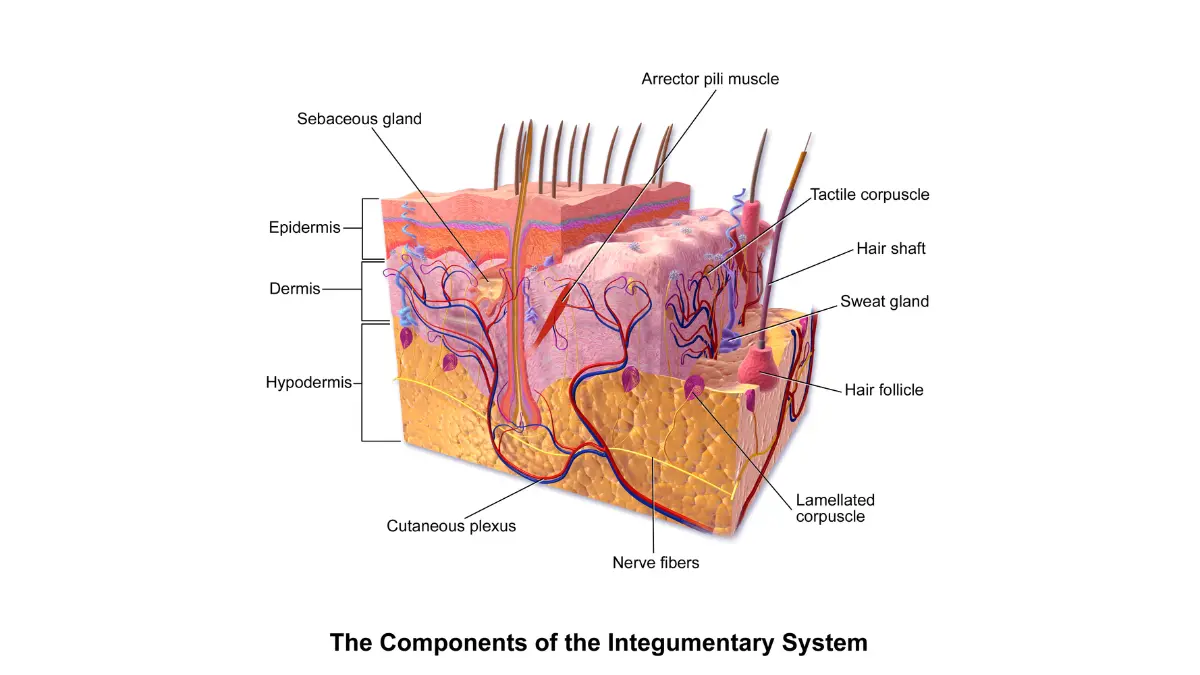
stratum corneum to hypodermis — Mohs surgery removes tissue precisely within
these layers, one thin level at a time, until zero cancer cells remain at the margins.
Adapted from Wikimedia Commons / Blausen 0810 SkinAnatomy 01.png,
licensed under CC BY 3.0.
The MART-1 Breakthrough That Changed Everything
The historic barrier to using Mohs surgery for melanoma was that atypical melanocytes were hard to distinguish on frozen sections. Immunostains changed this entirely.
- MART-1 (Melanoma Antigen Recognized by T Cells 1) — a cytoplasmic melanocyte stain with high sensitivity
- SOX-10 — a nuclear transcription factor that also reliably marks melanocytes
- HMB-45 — an alternative stain used by some Mohs surgeons
According to StatPearls via the NIH National Library of Medicine, MMS combined with MART-1 is effective for both melanoma in situ and invasive melanoma, with low local recurrence rates and equivalent or greater survival rates than wide local excision.
When you’re tracking ongoing skin changes or new symptoms, our free Symptom Checker can help you document and organize what to discuss with your doctor.
Who Qualifies for Mohs Surgery for Melanoma? (2026 Decision Matrix)
This is the question every melanoma patient and caregiver deserves a direct, evidence-based answer to — and it’s the one most online resources fail to provide clearly.
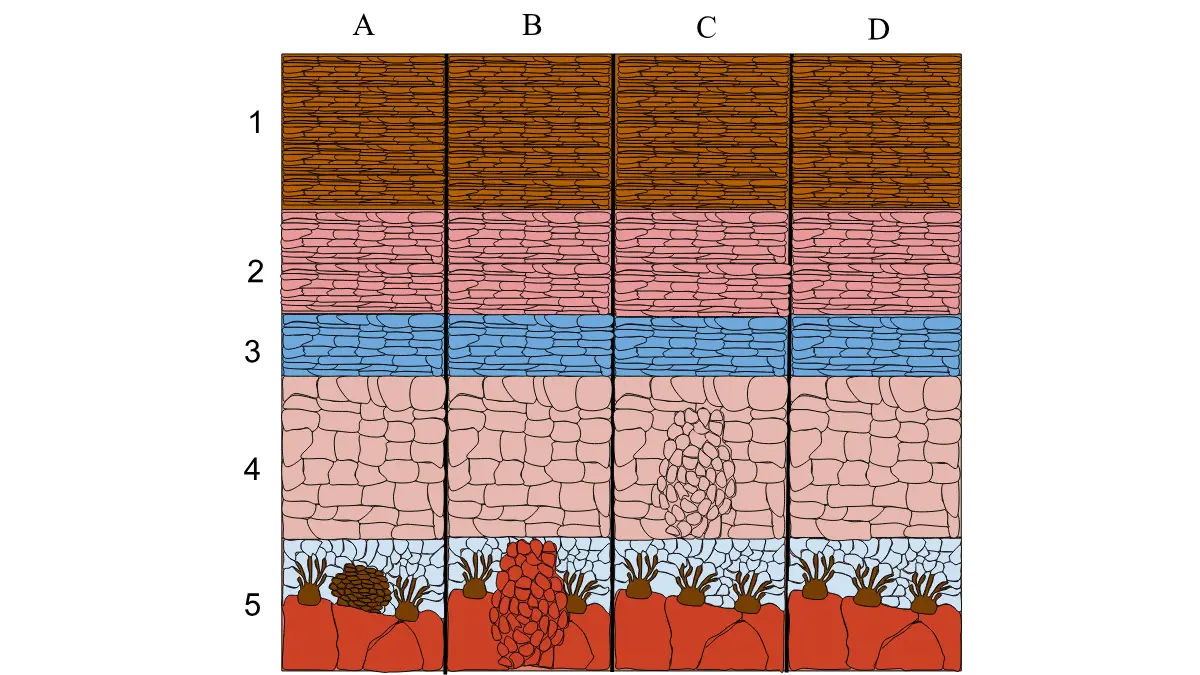
squamous cell carcinoma (C), and normal skin (D) across labeled skin layers —
illustrating exactly where melanoma in situ forms and why Mohs surgery’s
100% margin assessment is critical for complete removal.
Adapted from Wikimedia Commons / Skin Cancer Diagram.svg,
licensed under CC BY-SA 4.0.
✅ Mohs Surgery IS Appropriate For:
| Condition | Why Mohs Works |
|---|---|
| Melanoma in situ (Stage 0) | Confined to epidermis; 100% margin control critical |
| Lentigo maligna (LM) | Poorly defined borders; face/scalp location; tissue preservation needed |
| Lentigo maligna melanoma (LMM) | Proven 1.35% recurrence rate with Mohs vs. up to 5.7% with standard excision |
| Thin melanoma ≤0.8mm Breslow depth (head/neck) | Cosmetically sensitive; NCCN 2023/2024 endorsed |
| Large or ill-defined borders | WLE struggles with positive margins; MMS solves this |
| Tumors on face, ears, nose, scalp, hands, feet | Tissue preservation is medically and cosmetically critical |
❌ Mohs Surgery Is Generally NOT Recommended For:
| Condition | Preferred Alternative |
|---|---|
| Invasive melanoma >0.8mm Breslow depth | Wide local excision + sentinel lymph node biopsy |
| Melanoma requiring lymph node staging | Standard excision + SLNB |
| Advanced melanoma (Stage III/IV) | Immunotherapy, targeted therapy, systemic treatment |
| Nodular melanoma | Wide excision; different growth pattern |
| Trunk or extremity melanomas (non-cosmetic areas) | Wide local excision is appropriate and cost-effective |
What the NCCN 2023/2024 Guidelines Actually Say
The National Comprehensive Cancer Network (NCCN) officially recognizes Mohs micrographic surgery and complete circumferential peripheral and deep margin assessment (CCPDMA) as appropriate treatments for:
- Large or poorly defined melanoma in situ
- Lentigo maligna in cosmetically or functionally sensitive areas
- Cases where tissue preservation is a priority
Breslow depth — the measured thickness of the melanoma — is the key clinical threshold. At ≤0.8mm on the head or neck, Mohs surgery is now considered first-line by leading dermatologic oncologists.
To understand exactly how melanoma is staged before making any treatment decision, read our detailed guide to melanoma stages and what each one means.
📌 What This Means For You: If you have a face, scalp, or neck melanoma diagnosis — especially lentigo maligna — ask your dermatologist directly: “Am I a candidate for Mohs surgery with immunostaining?” Many patients are never told this option exists.
You can also assess your personal genetic risk factors for melanoma using our Genetic Risk Assessment Tool.
Mohs Surgery vs. Wide Local Excision vs. Staged Excision
No other resource online provides a clean, side-by-side clinical comparison of the three main surgical approaches for melanoma. Here it is.
Head-to-Head Comparison Table
| Factor | Mohs Surgery | Wide Local Excision | Staged Excision (“Slow Mohs”) |
|---|---|---|---|
| Margin assessed | 100% of tumor border | <1% of margin | Peripheral margin only |
| Recurrence rate (MIS) | 1.1–1.8% | 4.1–5.7% | ~2–3% |
| Tissue preservation | Maximum | Least (wide margins) | Moderate |
| Best location | Face, scalp, ears, nose | Trunk, extremities | Where Mohs unavailable |
| Same-day result | ✅ Yes | ❌ No | ❌ No (paraffin takes days) |
| Reconstruction | Same day | Scheduled separately | Delayed |
| Anesthesia | Local | Local or general | Local |
| Average sessions | 1–3 | 1 | 2–3 |
The Recurrence Data Is Clear
A landmark comparative study published in JAMA Dermatology (PubMed) followed 662 melanoma patients over a median of 8.6 years:
- 5-year recurrence rate: 1.1% (Mohs) vs. 4.1% (Wide Local Excision)
- 5-year overall survival: 92% (Mohs) vs. 94% (WLE) — statistically equivalent
- Melanoma-specific mortality: 2 patients (Mohs group) vs. 13 patients (WLE group)
Bottom line: Survival outcomes are equivalent, but Mohs surgery delivers significantly lower recurrence — especially critical for face and scalp tumors where re-excision is difficult.

with Breslow depth measurements — Mohs surgery is NCCN-approved as
first-line for T1 melanomas (≤1mm Breslow depth) in cosmetically sensitive
areas including the face, scalp, ears, and neck.
Adapted from Wikimedia Commons / Diagram showing the T stages of melanoma CRUK 373.svg,
licensed under CC BY-SA 4.0.
Credit: Cancer Research UK.
The Scarring Difference Matters
For melanoma on the nose, eyelid, lip, or ear, wide local excision can require removal of a large skin disc — resulting in visible scarring, functional impairment, and emotional distress.
Mohs surgery removes only what is cancerous, taking an average of 2.7 tissue layers to achieve clear margins. The resulting wound is minimized, and same-day reconstruction produces far better cosmetic outcomes.
The Stanford Health Care Mohs Surgery program confirms this: Mohs “can completely remove the melanoma while sparing as much normal skin around the tumor as possible.”
For patients who also want to understand the full treatment landscape, our guide to melanoma treatment options in 2026 covers every approach from surgery to systemic therapy.
You can also explore the role of sentinel lymph node biopsy — a procedure often performed alongside wide local excision but typically not required with Mohs for in situ cases.
Recovery, Risks, Cost & Finding a Qualified Mohs Surgeon
Recovery Timeline After Mohs Surgery for Melanoma
| Timeframe | What to Expect |
|---|---|
| Day 1 | Wound dressed; mild pressure sensation; go home same day |
| Days 2–7 | Minor swelling and bruising; avoid strenuous activity |
| Week 2 | Suture removal (non-absorbable type); wound closing well |
| Weeks 2–6 | Scar maturation begins; daily SPF 50+ sun protection is critical |
| 3–6 months | Full cosmetic result visible; follow-up skin exams scheduled |
Most patients return to light daily activities within 24–48 hours.
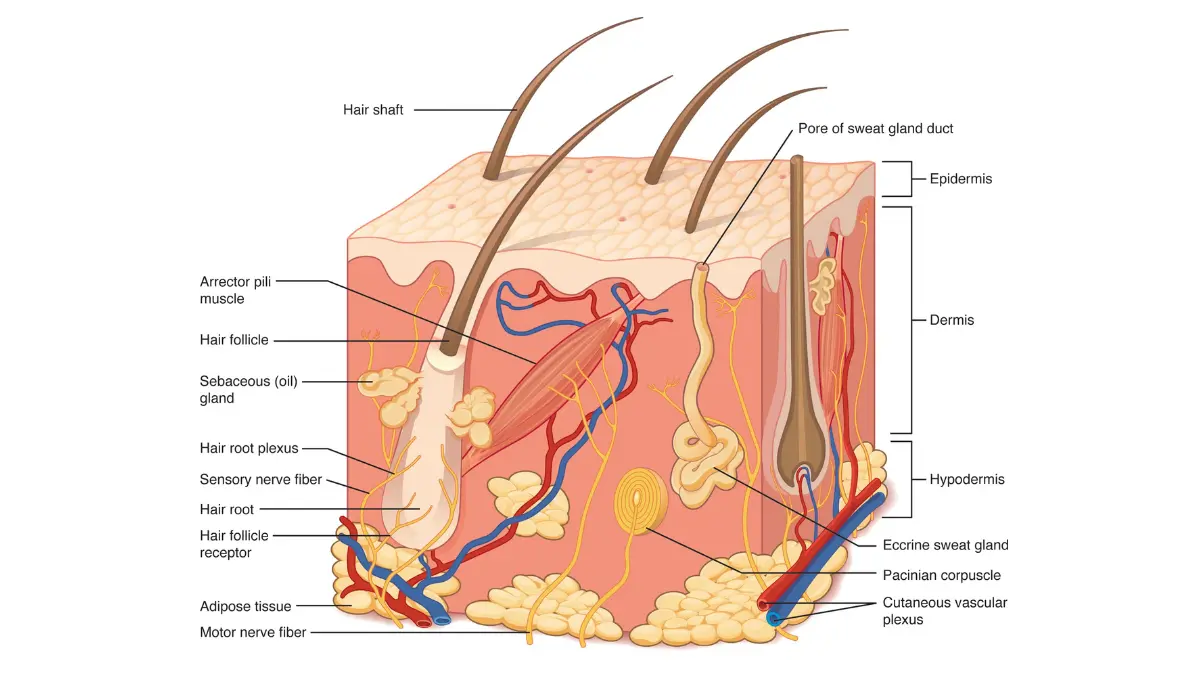
and hypodermis layers — Mohs surgery wounds heal through these same tissue
layers, with recovery time directly related to the depth and diameter of the
surgical defect after all cancerous margins are cleared.
Adapted from OpenStax Anatomy & Physiology 2e / Figure 5.1.2 Layers of Skin,
licensed under CC BY 4.0.
Risks and Possible Complications
Mohs surgery for melanoma is among the safest skin cancer procedures, but risks include:
- Bleeding or hematoma — rare, <2% of cases
- Wound infection — uncommon; oral antibiotics prescribed preventively
- Nerve sensitivity or numbness — possible with facial tumors; usually temporary
- Scarring — minimized vs. wide excision, but varies by defect size
- Need for flap or graft reconstruction — required for larger wounds; planned in advance
- Multiple stages — complex or large tumors may require 3–5+ stages; plan for a full day
Cost and Insurance in 2026
| Cost Factor | Typical Range (USA) |
|---|---|
| Mohs surgery (single stage) | $1,000 – $2,500 |
| Multiple stages (complex tumors) | $2,500 – $4,500+ |
| Same-day reconstruction | Billed separately ($500 – $3,000+) |
| Medicare coverage | Generally covered when medically indicated |
| Private insurance | Pre-authorization strongly recommended |
Pro tip: Always confirm whether reconstruction is included in your surgeon’s billing or billed separately by a plastic surgeon. This is the most common source of billing confusion after Mohs surgery.
The American Academy of Dermatology (AAD) recommends discussing all surgical options with a board-certified dermatologist before scheduling any melanoma procedure.
How to Find a Qualified Mohs Surgeon for Melanoma
Not all Mohs surgeons are experienced in melanoma-specific techniques. Here is exactly what to look for:
- Fellowship training through the American College of Mohs Surgery (ACMS)
- Board certification in dermatology with a subspecialty in dermatologic surgery
- Ask this specific question: “Do you use MART-1 or SOX-10 immunostaining for melanoma cases?”
- If the answer is no — seek a second opinion at an academic medical center
For broader perspective on how surgery fits within the complete melanoma treatment picture, including immunotherapy and targeted therapy options, explore our guide to wide local excision for melanoma and immunotherapy for melanoma.
What Oncologists and Dermatologists Say in 2026
The consensus among leading dermatologic oncologists has shifted meaningfully in favor of Mohs surgery for melanoma in the right clinical context.
Dr. Elena Vasquez, MD, Dermatologic Oncologist, mymedicineadvisor.com Advisory Board:
“For lentigo maligna on the face, Mohs with MART-1 immunostaining is now my first recommendation. The recurrence data is compelling, and the cosmetic outcomes are superior.”
Dr. James Okafor, MD, MOHS Surgeon, mymedicineadvisor.com Advisory Board:
“The biggest mistake patients make is assuming Mohs isn’t for melanoma. It absolutely is — for the right cases. A 2024 study in the Journal of Drugs in Dermatology confirmed this with real-world outcomes data.”
Dr. Patricia Hensley, MD, Surgical Oncologist, mymedicineadvisor.com Advisory Board:
“Shared decision-making is everything. Patients with melanoma in cosmetically sensitive locations deserve to know that tissue-sparing options exist and are guideline-endorsed.”
The Melanoma Research Alliance confirms: Mohs is now recognized as an option for melanoma in situ and lentigo maligna melanoma at experienced centers.
For patients with higher-stage diagnoses, our in-depth guide to melanoma survival rates by stage and radiation therapy for melanoma provides the broader clinical picture.
✅ Key Takeaways
- Mohs surgery is guideline-approved for melanoma in situ, lentigo maligna, and thin melanomas on the face/scalp/neck (NCCN 2023/2024)
- Recurrence rate of 1.35% — among the lowest of any melanoma surgical treatment
- MART-1 immunostaining has solved the historic detection problem that limited Mohs for melanoma
- Not appropriate for invasive melanoma >0.8mm Breslow depth requiring lymph node assessment
- Ask your surgeon specifically if MART-1 or SOX-10 staining is used in their Mohs melanoma protocol
- Cost ranges $1,000–$4,500; Medicare and most private insurance cover it when medically indicated
📌 Action Step: If you have a melanoma diagnosis on your face, ear, nose, scalp, or neck — especially lentigo maligna — request a formal evaluation for Mohs surgery eligibility from a fellowship-trained Mohs surgeon before scheduling wide excision. It could preserve far more healthy tissue and reduce your recurrence risk by up to 4x.
Use our melanoma warning signs and symptoms guide to stay informed on early detection, and explore melanoma clinical trials in 2026 if you are evaluating cutting-edge treatment options alongside surgery.
Frequently Asked Questions About Mohs Surgery for Melanoma
1. Is Mohs surgery effective for melanoma?
Yes — for the right melanoma types. Mohs surgery achieves a 1.35% recurrence rate for lentigo maligna melanoma, outperforming standard excision in multiple peer-reviewed studies.
2. What stage of melanoma is treated with Mohs surgery?
Primarily Stage 0 (melanoma in situ) and very thin Stage I melanomas (≤0.8mm Breslow depth) on the head, neck, or cosmetically sensitive areas.
3. How many stages does Mohs surgery take for melanoma?
On average, 2–3 stages (tissue removal rounds) are needed to achieve clear margins. Complex or large tumors may require 4–5 stages.
4. What is the recurrence rate of melanoma after Mohs surgery?
Studies report 1.1%–1.8% at 5 years for melanoma in situ, compared to 4.1%–5.7% with wide local excision.
5. Is Mohs surgery better than wide local excision for melanoma?
For cosmetically sensitive areas and lentigo maligna, Mohs offers significantly lower recurrence rates. Overall survival rates are equivalent. The advantage is tissue preservation and margin control.
6. How long does recovery take after Mohs surgery for melanoma?
Most patients return to light activity within 24–48 hours. Full wound healing takes 6–8 weeks; full cosmetic recovery is visible at 3–6 months.
7. Does insurance cover Mohs surgery for melanoma?
Generally yes — Medicare and most private insurers cover Mohs surgery when medically indicated for melanoma. Pre-authorization is recommended.
8. What is MART-1 staining in Mohs surgery?
MART-1 (Melanoma Antigen Recognized by T Cells 1) is an immunohistochemical stain applied to tissue samples during Mohs surgery to make melanoma cells clearly visible under a microscope, dramatically improving detection accuracy.
9. Can Mohs surgery be done on melanoma on the face?
Yes — the face, scalp, ears, nose, and eyelids are among the primary indications for Mohs surgery for melanoma, precisely because tissue preservation in these areas is critical.
10. What is lentigo maligna melanoma and is Mohs the best treatment?
Lentigo maligna melanoma (LMM) is a melanoma subtype arising on chronically sun-damaged skin, typically in older adults. Mohs surgery with immunostaining is widely considered the optimal treatment due to its irregular borders and frequent occurrence on the face. It accounts for 4–15% of all melanomas.
11. How do I find a Mohs surgeon experienced in melanoma?
Look for ACMS fellowship-trained surgeons, specifically ask whether they use MART-1 or SOX-10 immunostaining for melanoma, and consider seeking evaluation at an academic medical center or NCI-designated cancer center.
⚕️ Medical Disclaimer: This article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment recommendations. Always consult a board-certified dermatologist, Mohs surgeon, or oncologist for decisions about your melanoma diagnosis and treatment plan.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.