On This Page – Quick Medical Summary
Every 2.3 minutes, someone in the United States is diagnosed with lung cancer. That is not a statistic to scroll past. It is a reality that touches firefighters and teachers, marathon runners and lifelong non-smokers, mothers in their 40s and veterans in their 70s.
Lung cancer kills more Americans each year than colon, prostate, ovarian, and breast cancers combined. And yet — here is the part most people never hear — the five-year survival rate has nearly doubled in the past decade, rising from 17% in 2014 to 27% in 2026. For patients whose cancer is caught early, that survival figure climbs to 65%.
This is the guide that changes what you know about lung cancer. Not a generic overview. Not a list of symptoms copied from a pamphlet. A complete, clinically rigorous, patient-first resource — covering every type, every stage, every treatment option available in 2026, and every question you are afraid to ask out loud.
Whether you just received a diagnosis, are supporting a loved one, or are trying to understand your own risk, read every section. Knowledge is the first and most powerful treatment.
What Is Lung Cancer? — The Foundation Every Patient Needs
What Exactly Is Lung Cancer?
Lung cancer is a disease in which abnormal cells in the lung tissue begin to grow and multiply in an uncontrolled way, forming one or more tumors. Unlike healthy cells, which grow, divide, and die on a predictable schedule, cancer cells ignore the body’s stop signals. They keep multiplying.
Over time, these tumors can invade nearby lung tissue, crowd out healthy cells, and eventually spread through the bloodstream or lymphatic system to other organs — a process called metastasis. When lung cancer spreads to the brain, bones, or liver, the cancer cells are still lung cancer cells. They are treated as lung cancer, not as brain cancer or liver cancer.
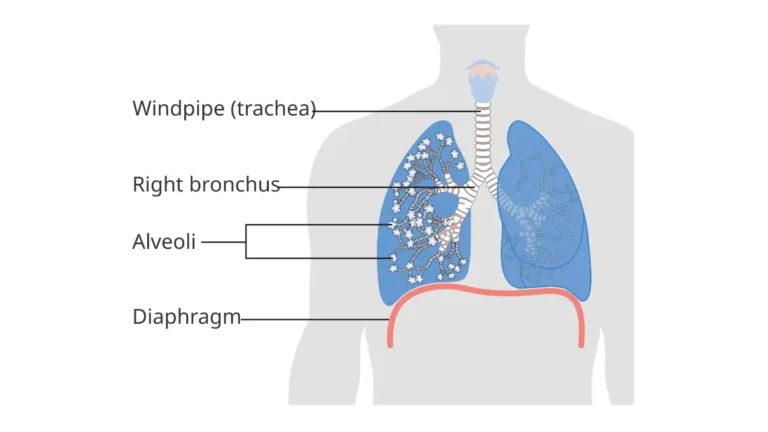
The lungs sit on either side of the chest, separated by a central space called the mediastinum. Every breath you take — roughly 20,000 per day — passes through a branching network of airways called bronchi, then bronchioles, and finally into tiny air sacs called alveoli, where oxygen and carbon dioxide are exchanged. Lung cancer almost always begins in the cells lining these airways or alveoli, and the specific cell type of origin determines which type of lung cancer you have — and crucially, how it behaves and how it is treated.
How Common Is Lung Cancer in 2026? The Numbers That Matter
According to the National Cancer Institute’s SEER database, an estimated 229,410 Americans will be diagnosed with lung cancer in 2026, and approximately 124,990 lives will be lost to the disease this year alone. Globally, the World Health Organization reports over 2.2 million new cases annually, making lung cancer the most diagnosed and most deadly cancer worldwide.
Despite these staggering numbers, there is meaningful progress. Consider:
- Death rates have been falling an average of 4.2% per year since 2014, driven by improved screening, earlier detection, and revolutionary new therapies.
- New case rates have declined 13% over the past five years, primarily because fewer Americans are smoking.
- The 5-year survival rate has nearly doubled — from 17% in 2014 to 27% today — the largest single-decade improvement in lung cancer history.
Lung cancer currently accounts for 11.1% of all new cancer cases in the United States and is responsible for 20.2% of all cancer deaths — or roughly 1 in every 5 cancer deaths. That makes it the most lethal cancer, by a significant margin, as reported by the National Cancer Institute.
The Survival Breakthrough Nobody Is Talking About
When oncologists compare the lung cancer landscape of 2016 to 2026, the change is nothing short of extraordinary. A decade ago, a Stage IV lung cancer diagnosis came with a median survival of around eight months. Today, patients with certain molecular profiles — particularly those with targetable genetic mutations — are routinely living three, four, and five or more years with advanced disease.
This transformation is not luck. It is the result of precision medicine: the ability to identify specific DNA-level mutations driving an individual tumor’s growth, and to deploy drugs engineered to shut those mutations down.
What this means for you: Surviving lung cancer in 2026 is increasingly possible — but it requires accessing the right testing, the right specialist, and the right treatment center. This guide will show you exactly how to do that.
Who Gets Lung Cancer? The Surprising 2026 Demographics
Lung cancer does not discriminate the way people assume. Here is what the 2025 American Cancer Society Cancer Facts and Figures reveals:
- Women under 50 are now being diagnosed with lung cancer at higher rates than men of the same age — a complete reversal of historical patterns.
- 20% of all lung cancer deaths occur in people who have never smoked a single cigarette in their lives, according to data from the World Health Organization.
- The average age at diagnosis remains 70 years, but this is shifting younger, particularly in women and in never-smoking populations.
- Lung cancer is more common in non-Hispanic Black men than in any other demographic group.
| Demographic | Key 2026 Data Point |
|---|---|
| Women under 50 | Higher incidence rate than men same age |
| Never-smokers | Account for 20% of lung cancer deaths |
| Average age at diagnosis | 70 years |
| Most at-risk male group | Non-Hispanic Black men |
| State with highest incidence | Kentucky |
| State with lowest incidence | Utah |
A Patient Story That Changes Everything
Marcus, a 52-year-old retired firefighter from Ohio, had never smoked. He was physically active, ate well, and had no family history of cancer. His only symptom was a dry cough that lingered for six weeks after a cold. His primary care physician ordered a chest CT scan. It revealed a 2.1 cm mass in the upper lobe of his right lung.
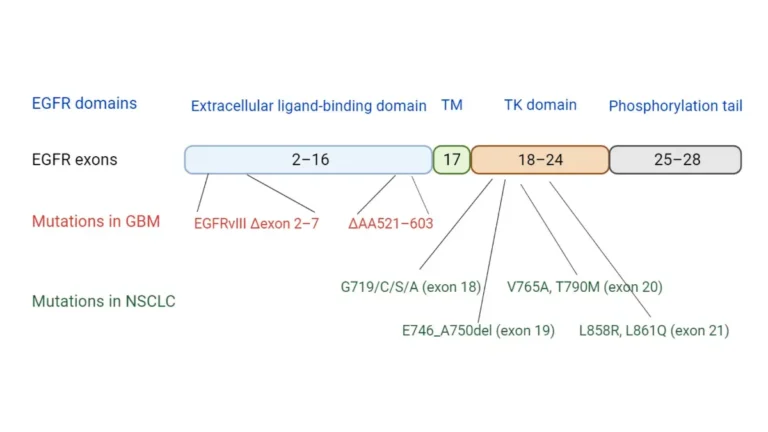
Biopsies confirmed adenocarcinoma — the most common subtype of lung cancer in non-smokers. Molecular testing identified an EGFR exon 19 deletion — one of the most targetable mutations in all of oncology. Marcus was started on osimertinib (Tagrisso). Within three months, his tumor had shrunk by 60%.
As of his last scan in early 2026, Marcus shows no evidence of active disease. He credits early detection — made possible because he used our Symptom Checker to assess his persistent cough and was prompted to consult his doctor immediately rather than waiting.
His story is not an outlier. It is what modern lung cancer medicine looks like when the system works.
A Brief History: From Rare Disease to Global Crisis — and Back
Before 1900, lung cancer was so rare that medical textbooks barely mentioned it. The explosion of cigarette manufacturing in the early 20th century — combined with the introduction of machine-rolled cigarettes, widespread advertising, and the distribution of cigarettes to soldiers in both World Wars — created a lung cancer epidemic that peaked in the 1980s.
By the 1950s and 1960s, landmark studies began linking tobacco and lung cancer. Governments and health authorities slowly adopted anti-tobacco policies. As smoking rates in the United States fell from over 40% of adults in the 1960s to approximately 12% in 2026, lung cancer rates began their long decline.
The modern era is defined by a new chapter: the molecular revolution. Since 2010, over 98 separate treatment approaches have been approved by the FDA for lung cancer. Eleven of those approvals came between 2024 and 2026 alone. Lung cancer medicine has changed more in the past decade than in the previous five decades combined.
Types of Lung Cancer — Every Category Explained Clearly
The Two Main Categories: NSCLC vs. SCLC
All lung cancers are divided into two primary categories based on how the cancer cells look under a microscope. This distinction is fundamental — it determines treatment strategy, prognosis, and which specialists you will work with most closely.
| Feature | Non-Small Cell Lung Cancer (NSCLC) | Small Cell Lung Cancer (SCLC) |
|---|---|---|
| Prevalence | ~85% of all lung cancers | ~13–15% of all lung cancers |
| Growth speed | Slower, more variable | Extremely rapid |
| Typical patient | Variable — smokers and non-smokers | Almost always heavy smokers |
| Metastasis at diagnosis | Often localized early, but not always | >66% already advanced at diagnosis |
| Primary treatment | Surgery, targeted therapy, immunotherapy, radiation, chemo | Chemotherapy + immunotherapy (surgery rare) |
| 5-year survival | Better than SCLC at all stages | Generally worse |
| Molecular testing value | Extremely high | Moderate |
Non-Small Cell Lung Cancer (NSCLC) — 85% of All Cases
NSCLC is not a single disease. It is a family of cancers that share the characteristic of having larger, more distinct-looking cells under the microscope. Within NSCLC, there are three major subtypes:
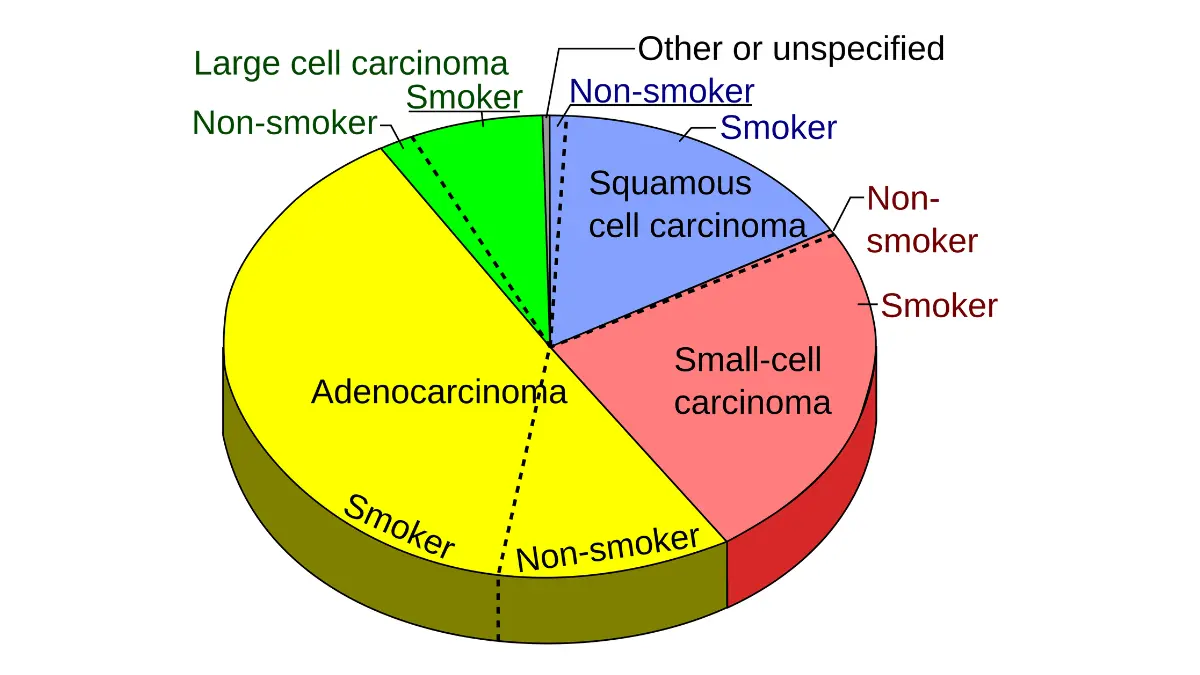
Adenocarcinoma — The Most Common Lung Cancer in 2026
Adenocarcinoma accounts for approximately 45% of all lung cancers — making it the single most common subtype worldwide. It originates in the mucus-producing glandular cells that line the outer edges of the lungs (the periphery).
Why it matters most:
- It is the most common lung cancer in women, non-smokers, and younger adults.
- It is the subtype most likely to carry targetable genetic mutations (EGFR, ALK, KRAS, ROS1).
- Because it grows peripherally, it often produces no symptoms until advanced — making screening critically important.
- Survival outcomes with modern targeted therapy for adenocarcinoma with actionable mutations can be dramatically better than survival statistics suggest.
Squamous Cell Carcinoma (20–25% of Cases)
Squamous cell carcinoma arises from the flat cells lining the central airways (bronchi), near the center of the chest. It is strongly associated with tobacco smoking and tends to grow more centrally.
Key features:
- Earlier symptom onset than adenocarcinoma, because central tumors obstruct airways sooner.
- Coughing up blood (hemoptysis) is more common in this subtype.
- Less likely to carry targetable mutations, but PD-L1 immunotherapy is effective in many cases.
- Standard first-line chemotherapy: cisplatin + gemcitabine.
Large Cell Carcinoma (10–15% of Cases)
Large cell carcinoma is a less common, more aggressive subtype. It can arise anywhere in the lung — peripherally or centrally — and tends to grow and spread faster than adenocarcinoma or squamous cell carcinoma.
- Cells appear large with prominent nuclei under the microscope.
- Often diagnosed by exclusion — when a tumor lacks the features of the other two subtypes.
- Molecular testing is particularly critical here, as some large cell carcinomas carry targetable alterations.
Rare NSCLC Subtypes
- Carcinoid tumors (1–2% of lung cancers): Slow-growing neuroendocrine tumors, often discovered incidentally on imaging. Best prognosis of all lung cancer types.
- Sarcomatoid carcinomas: Aggressive, rare tumors requiring molecular profiling for proper classification and treatment selection.
- Pulmonary blastomas: Extremely rare, mixed tumors combining epithelial and mesenchymal elements.
Small Cell Lung Cancer (SCLC) — The Most Aggressive Subtype
SCLC is less common than NSCLC, but it is dramatically more aggressive. Tumor cells are small with poorly defined boundaries, rapid division cycles, and a tendency to spread through the body within weeks of reaching critical mass.
Key clinical realities:
- Over two-thirds of SCLC patients are already at an advanced stage when first diagnosed.
- SCLC is almost exclusively caused by tobacco smoking — it is exceptionally rare in never-smokers.
- Surgery is seldom used because the cancer is typically widespread by the time it is found.
- SCLC is initially sensitive to chemotherapy — often dramatically so — but almost universally develops resistance within months, leading to relapse.
- After relapse, median survival is typically 3–4 months, making initial treatment response the critical window.
For a detailed breakdown of small cell lung cancer outcomes and treatment costs, our guide on SCLC survival rates and treatment options provides comprehensive clinical data.
SCLC Staging uses a simplified two-stage system (unlike the detailed TNM system used for NSCLC):
- Limited Stage: Cancer confined to one side of the chest and regional lymph nodes, small enough to be covered by a single radiation field.
- Extensive Stage: Cancer has spread beyond one side of the chest, including the other lung, distant lymph nodes, and distant organs.
The New Era: Diagnosing by Molecular Profile
Here is what the top-ranking lung cancer websites almost universally fail to explain at a patient level: two patients with “lung cancer” may have completely different diseases at the molecular level, require completely different treatments, and have dramatically different outcomes.
The molecular revolution has created a new classification system that sits on top of the traditional NSCLC/SCLC division. Today, oncologists look for actionable genomic alterations (AGAs) — specific mutations in tumor DNA that can be targeted by precision drugs.
The most important mutations currently targeted in NSCLC:
| Mutation | Prevalence in NSCLC | Key FDA-Approved Drugs |
|---|---|---|
| EGFR (exon 19 del / L858R) | 10–15% overall; 30–50% in never-smokers | Osimertinib, Erlotinib |
| ALK rearrangement | 3–7% | Alectinib, Brigatinib, Lorlatinib |
| KRAS G12C | 12–15% | Sotorasib, Adagrasib |
| ROS1 rearrangement | 1–2% | Crizotinib, Lorlatinib |
| MET exon 14 skipping | 3–4% | Tepotinib, Capmatinib |
| RET fusion | 1–2% | Selpercatinib, Pralsetinib |
| NTRK fusion | <1% | Larotrectinib |
| BRAF V600E | 1–3% | Dabrafenib + Trametinib |
| EGFR Exon 20 insertion | 2–3% | Sunvozertinib (FDA accelerated approval, 2025) |
Why this table matters to you: Before starting any treatment for NSCLC, you should have comprehensive molecular testing. If your oncologist does not recommend it, ask for it. This single decision can be the difference between a drug that works and one that doesn’t.
To understand your own genetic risk factors before or after a diagnosis, use our Genetic Risk Assessment Tool — a validated resource that helps identify hereditary risk patterns based on family history and personal health data.
For patients wondering about the differences between lung cancer and mesothelioma — two diseases that are often confused — our detailed comparison guide on mesothelioma vs. lung cancer explains everything clearly.
Lung Cancer Causes, Risk Factors & the Never-Smoker Crisis
What Causes Lung Cancer? The Biological Mechanism
Lung cancer begins with DNA damage. Every cell in your body carries a complete copy of your genetic code. When certain genes that control cell growth — called proto-oncogenes and tumor suppressor genes — sustain mutations, the delicate balance between cell growth and cell death breaks down.
Under normal circumstances, the body has multiple repair mechanisms and immune surveillance systems that detect and eliminate damaged cells. Lung cancer develops when:
- DNA damage occurs faster than repair mechanisms can correct it.
- Mutations accumulate over time in specific growth-regulating genes.
- The immune system fails to recognize and destroy the abnormal cells.
- A clone of abnormal cells gains the ability to grow indefinitely, invade neighboring tissue, and eventually spread.
This process typically takes years to decades — which is why lung cancer most often appears in older adults and why early intervention is so powerful.
Tobacco Smoking — Still the Leading Cause
Smoking remains the most significant risk factor for lung cancer. Tobacco smoke contains over 7,000 chemical compounds, at least 70 of which are known human carcinogens. These chemicals — including nitrosamines, benzene, and polycyclic aromatic hydrocarbons — directly damage the DNA of lung cells with every inhalation.
Key facts about smoking and lung cancer risk:
- Smoking accounts for approximately 80–90% of all lung cancer deaths in the United States, according to the Centers for Disease Control and Prevention.
- Risk scales directly with pack-years (packs smoked per day × years of smoking): someone who smoked two packs per day for 20 years (40 pack-years) faces a substantially higher risk than someone with 20 pack-years.
- Second-hand smoke is also a confirmed carcinogen — non-smokers living with smokers have a 20–30% higher risk of lung cancer than those in smoke-free homes, according to the American Cancer Society.
- People who quit smoking reduce their lung cancer risk by approximately 39.1% within five years of quitting, per data cited in the American Family Physician.
- Quitting smoking after a diagnosis significantly reduces the risk of developing a second primary cancer — by up to 3.5 times compared to continuing to smoke.
On vaping and e-cigarettes: As of 2026, vaping is too new to have complete long-term epidemiological data. However, many vaping liquids contain known carcinogens, nicotine (which promotes tumor survival), and chemicals that cause significant lung inflammation. Current evidence from pulmonology experts strongly suggests vaping is not safe for lung health, even if its precise cancer risk remains under study.
Radon Gas — The Invisible Killer in Your Home
Radon is a naturally occurring, colorless, odorless radioactive gas produced by the breakdown of uranium in soil and rock. It seeps through cracks in building foundations and can accumulate to dangerous concentrations indoors — particularly in basements.
Radon is the second leading cause of lung cancer in the United States, responsible for approximately 21,000 deaths annually. It is the leading cause of lung cancer in people who have never smoked.
What you need to know:
- The U.S. Environmental Protection Agency (EPA) and the Surgeon General recommend taking action to reduce radon in homes when measured levels exceed 4 pCi/L (picocuries per liter).
- The World Health Organization recommends action at 3 pCi/L or higher.
- One in fifteen U.S. homes is estimated to have radon levels at or above EPA’s action level.
- Radon test kits cost $10–$30 and are available online and at hardware stores. Professional mitigation systems typically cost $800–$2,500.
- Smokers exposed to elevated radon face a nearly 100-fold increased risk of lung cancer compared to non-exposed non-smokers — the combination is especially dangerous.
Actionable step: Test your home for radon. If you smoke and live in a high-radon home, quitting smoking and mitigating radon together may be the two most impactful things you can do to reduce your lung cancer risk.
Occupational Exposures and Air Pollution
Certain workplace environments and environmental conditions significantly elevate lung cancer risk:
High-risk occupational carcinogens:
- Asbestos: The most clinically significant occupational lung carcinogen. Asbestos exposure accounts for over 34,000 lung cancer deaths in the U.S. annually — roughly 27% of all lung cancer fatalities. Occupations historically at highest risk include construction workers, shipyard workers, electricians, plumbers, and military veterans.
- For those dealing with asbestos-related respiratory conditions, our article on asbestosis symptoms and what patients miss provides critical context.
- Arsenic, chromium VI, and nickel: Found in certain industrial processes.
- Diesel engine exhaust: Classified as a Group 1 carcinogen by the International Agency for Research on Cancer (IARC).
- Crystalline silica: Dust from cutting concrete, stone, or brick.
- Beryllium, cadmium, and coal dust: Additional confirmed occupational carcinogens.
Outdoor and indoor air pollution:
- Outdoor air pollution (fine particulate matter, PM2.5) was classified as a Group 1 lung carcinogen by the IARC in 2013. The American Lung Association’s 2026 “Something in the Air” report highlights ongoing concerns about air quality in major U.S. cities — particularly for individuals with chronic respiratory conditions.
- Indoor cooking fumes — particularly from high-heat cooking methods (wok cooking, stir-frying) using certain oils — have been linked to elevated lung cancer rates in non-smoking Asian women globally. This exposure is often overlooked in Western medical discussions.
States with highest lung cancer death rates (American Lung Association, 2025): West Virginia, Kentucky, Arkansas, Oklahoma, and Mississippi — all states with historically elevated smoking rates and significant occupational chemical exposure.
The Never-Smoker Lung Cancer Crisis
This is the section that all major competing lung cancer guides skip, minimize, or bury in a footnote. It deserves its own headline.
People who have never smoked account for approximately 20% of all lung cancer deaths in the United States — according to 2024 data from the Centers for Disease Control and Prevention. In absolute terms, that represents roughly 25,000 deaths per year. If never-smoker lung cancer were classified as its own cancer, it would rank among the top ten most deadly cancers in the country.
Never-smoker lung cancer is increasingly recognized as a biologically distinct disease from tobacco-driven lung cancer:
- It is predominantly adenocarcinoma.
- It is far more likely to carry targetable genetic mutations — particularly EGFR and ALK mutations — which can be treated with precision oral medications.
- It is disproportionately diagnosed in women and in younger patients (under 50).
- It is rising most rapidly among young women globally, particularly in East Asian countries, though the trend is now visible in the U.S. as well.
Causes of lung cancer in never-smokers:
- Radon gas (leading environmental cause)
- Second-hand smoke exposure
- Outdoor and indoor air pollution
- Inherited genetic predisposition (EGFR germline variants, other loci)
- Viral infection (human papillomavirus has been studied as a potential co-factor in some populations)
- High-heat cooking fumes
The most important clinical implication: never-smokers should not assume they are safe from lung cancer. If you have a persistent respiratory symptom and you have never smoked, do not let a clinician dismiss it based solely on your smoking history.
| Never-Smoker Lung Cancer Profile | Details |
|---|---|
| Share of all lung cancer deaths | ~20% |
| Most common subtype | Adenocarcinoma |
| Most common mutations | EGFR, ALK |
| Most affected population | Women, younger adults |
| Primary environmental cause | Radon gas |
| Clinical implication | Targetable mutations → precision therapy eligible |
Genetic and Family History Risk Factors
Lung cancer has a hereditary component that is frequently underappreciated:
- Having a first-degree relative (parent, sibling, child) with lung cancer increases your personal risk, independent of smoking status.
- Genome-wide association studies (GWAS) have identified several genetic loci — including CHRNA3/5 (nicotinic acetylcholine receptor genes), TERT-CLPTM1L, and CHEK2 — that confer increased susceptibility to lung cancer.
- Lung cancer survivors face elevated risk of developing a second primary lung cancer — particularly if they continue or resume smoking.
Additional Risk Factors: A Complete Reference
| Risk Factor | Relative Risk Increase | Modifiable? |
|---|---|---|
| Current smoker (heavy, long-term) | 15–30× | Yes — quit |
| Former smoker | Still elevated vs. never-smoker | Yes — risk declines after quitting |
| Radon exposure (>4 pCi/L) | 2–3× | Yes — test and mitigate |
| Asbestos exposure | 5–7× (non-smoker); ~100× (smoker) | Partially — avoid further exposure |
| Air pollution (long-term PM2.5) | 1.3–1.5× | Partially |
| First-degree family history | 1.5–2× | No |
| COPD diagnosis | 2–6× | Partially (quitting, treatment) |
| Prior chest radiation | Elevated | No |
| HIV/immunosuppression | Elevated | Partially |
Lung Cancer Symptoms — From Early Warning Signs to Advanced Disease
Why Lung Cancer Is Called “The Silent Disease”
Lung cancer is one of the most lethal cancers precisely because it is one of the stealthiest. In the majority of patients, early-stage lung cancer produces no symptoms whatsoever. The tumor may grow for months or years before the patient notices anything wrong.
By the time symptoms appear, the cancer has often already spread beyond the lung. According to the American Lung Association’s 2025 State of Lung Cancer report, only 28.1% of lung cancers are diagnosed at an early stage nationally. A full 43% are not detected until the cancer has spread to distant organs — when the five-year survival rate drops to just 10%.
This is not a reason for despair. It is the single strongest argument for lung cancer screening (covered comprehensively in Section 9).
Early-Stage Lung Cancer Symptoms: Know These First
The symptoms of early lung cancer are easily mistaken for ordinary respiratory problems. This is why they are so often missed — by patients and, sometimes, by clinicians. Here is what to watch for, presented as a clinical reference table:
| Symptom | Description | When to Act |
|---|---|---|
| Persistent cough | Cough that does not go away after 2–3 weeks, or worsens over time | See your doctor if cough persists >3 weeks |
| Recurring pneumonia or bronchitis | Same area of lung repeatedly infected | Always warrants investigation |
| Shortness of breath (dyspnea) | Breathlessness with activities that previously caused none | Consult a physician promptly |
| Chest pain or discomfort | Dull, persistent ache in the chest, shoulder, or back | Medical evaluation needed |
| Hoarseness | Voice changes not explained by cold or laryngitis | See a physician if lasting >2 weeks |
| Unexplained fatigue | Persistent tiredness that rest does not resolve | Worth discussing with your doctor |
⚠️ Key Point: These symptoms, taken alone, are far more likely to represent benign conditions than lung cancer. But when they persist, worsen, or occur in combination — especially in anyone with known risk factors — medical evaluation is essential.
For a comprehensive symptom guide with risk stratification, explore our article on lung cancer signs and early warnings for a deeper clinical breakdown.
Symptoms as Lung Cancer Advances
As lung cancer grows and spreads, symptoms become more prominent and more varied:
Respiratory symptoms:
- Coughing up blood (hemoptysis): Even a small amount of blood in phlegm requires immediate medical evaluation. Never dismiss it.
- Wheezing: A high-pitched breathing sound caused by airway narrowing or obstruction.
- Stridor: A harsh, high-pitched breathing sound caused by upper airway obstruction.
Systemic symptoms:
- Unexplained weight loss: Losing 10+ pounds without intentional diet or exercise changes is a red flag for malignancy.
- Loss of appetite: Frequently co-occurs with weight loss.
- Severe fatigue: Fatigue in advanced lung cancer is qualitatively different from ordinary tiredness — it does not respond to rest.
Structural symptoms:
- Pancoast tumor (superior sulcus tumor): A tumor growing at the very top (apex) of the lung that presses on nearby nerves and structures. It causes a distinctive pattern of symptoms that is frequently misattributed to cervical spine problems:
- Shoulder pain radiating down the inner arm
- Weakness or atrophy in hand and forearm muscles
- Horner’s syndrome (see below)
- This clinical pattern, when properly recognized, is often a diagnosable presentation of lung cancer. It is unfortunately often misdiagnosed as rotator cuff injury or cervical radiculopathy for months before the correct diagnosis is made.
- Superior Vena Cava (SVC) Syndrome: When a tumor or enlarged lymph node compresses the superior vena cava — the large vein returning blood from the upper body to the heart — it causes characteristic swelling of the face, neck, arms, and upper chest, often with a purplish discoloration. This is a medical emergency in severe cases.
- Horner’s Syndrome: A constellation of three findings — a smaller pupil (miosis), drooping upper eyelid (ptosis), and reduced or absent sweating on one side of the face — caused by compression of the sympathetic nerve chain in the chest. When occurring on the same side as a lung tumor, Horner’s syndrome should immediately raise suspicion for a Pancoast tumor.
When Lung Cancer Spreads: Symptoms by Metastatic Location
Lung cancer preferentially spreads to specific organs. Understanding where it spreads — and what symptoms result — helps both patients and clinicians recognize progression early.
| Metastatic Site | Symptoms Produced |
|---|---|
| Brain | Persistent headaches, nausea, seizures, weakness on one side of the body, personality or behavioral changes, vision problems, balance difficulties |
| Bone | Deep, aching bone pain (often worse at night); spontaneous or low-trauma fractures (particularly in the spine, ribs, or hip); elevated calcium (hypercalcemia) causing confusion, constipation, nausea |
| Liver | Jaundice (yellowing of skin and eyes), right-sided abdominal pain or fullness, unexplained elevated liver enzymes on blood tests |
| Adrenal glands | Often symptom-free; large adrenal metastases may cause abdominal pain |
| Lymph nodes | Palpable swollen nodes in the neck or above the collarbone (supraclavicular region) |
Paraneoplastic Syndromes: The Symptoms That Don’t Seem Related to Your Lungs
This is one of the most clinically important — and most underexplained — aspects of lung cancer. Paraneoplastic syndromes are conditions caused not by the tumor itself physically invading tissue, but by hormones or proteins secreted by the tumor, or by the immune system responding to the tumor in ways that damage normal tissue.
SCLC is particularly prone to causing paraneoplastic syndromes, but NSCLC can cause them too.
The most important paraneoplastic syndromes in lung cancer:
- SIADH (Syndrome of Inappropriate Antidiuretic Hormone): The tumor secretes ADH, causing the kidneys to retain too much water, diluting sodium in the blood. Symptoms include fatigue, nausea, vomiting, muscle weakness, confusion, and in severe cases, seizures and coma. Especially common in SCLC.
- Cushing Syndrome (Ectopic ACTH Syndrome): The tumor secretes ACTH, overstimulating cortisol production by the adrenal glands. Symptoms include rapid weight gain (particularly in the face and trunk), muscle weakness, high blood sugar, high blood pressure, and easy bruising.
- Hypercalcemia of Malignancy: More common with squamous cell carcinoma. The tumor produces a parathyroid hormone-related protein (PTHrP) that raises blood calcium. Symptoms include confusion, excessive thirst, frequent urination, constipation, muscle weakness, and cardiac arrhythmias.
- Lambert-Eaton Myasthenic Syndrome (LEMS): The immune system, triggered by the tumor, attacks the neuromuscular junctions (the connections between nerves and muscles). Patients develop progressive proximal muscle weakness — particularly in the hips and thighs — difficulty walking, and autonomic symptoms (dry mouth, constipation, impotence). LEMS is almost always associated with SCLC.
- Paraneoplastic Limbic Encephalitis: The immune system attacks the limbic system — the brain region governing memory, emotions, and behavior. Patients develop memory loss, personality changes, mood disturbances, and seizures. This can precede the lung cancer diagnosis by weeks or months.
Clinical Insight: If you or someone you know develops unexplained neurological symptoms, electrolyte abnormalities, or a Cushing-like appearance — especially in someone with a smoking history — paraneoplastic syndrome from an occult lung cancer should be considered. These conditions are often investigated by specialists who never consider lung cancer as the underlying cause, leading to diagnostic delays of months.
The MedlinePlus lung cancer resource provides additional information on the systemic effects of lung cancer that many patients find helpful as an introductory reference.
Lung Cancer Symptoms in Women: Why They Are Missed More Often
The gender gap in lung cancer diagnosis is a documented and growing problem. There are several reasons women’s lung cancer symptoms are missed more often:
- Women are more likely to develop adenocarcinoma — the peripheral, often silent subtype — rather than the central tumors that produce earlier, more obvious symptoms.
- Women’s symptoms are more likely to be attributed to anxiety, GERD, musculoskeletal causes, or stress by both patients and clinicians.
- Women are less likely to be asked about smoking history in the context of respiratory symptoms (despite the fact that 20% of women with lung cancer never smoked).
- The ACS 2025 finding that women under 50 are now diagnosed at higher rates than men of the same age has not yet changed clinical screening patterns.
What you can do: If you are a woman with persistent respiratory symptoms and your concerns are being dismissed, request imaging. You are your own best advocate. Use our Symptom Checker to document your symptoms over time and bring that record to your next appointment.
For an MD Anderson expert-level overview of lung cancer symptoms, the MD Anderson lung cancer resource provides a rigorous clinical framework.
How Lung Cancer Is Diagnosed — Tests, Biomarkers & Liquid Biopsy
The Diagnostic Journey: What to Expect, Step by Step
Receiving a lung cancer diagnosis is almost never a single moment. It is a multi-step process that can take days to weeks. Understanding each step — before you experience it — reduces anxiety and helps you ask the right questions.
“Getting a diagnosis is one of the most stressful experiences a patient can face. The process feels overwhelming. But it is a process with a clear sequence, and understanding it gives you some control back.” — A common sentiment expressed by lung cancer patients across major support communities.
Step 1: Your First Appointment
The diagnostic journey typically begins when a persistent symptom prompts a visit to a primary care physician. During this appointment:
- Your physician will take a complete medical history: smoking history (pack-years), occupational exposures, family history, and a detailed symptom timeline.
- A physical examination follows, including listening to breath sounds (auscultation), checking lymph nodes in the neck and collarbone area, and assessing your overall health status.
- Blood tests may be ordered to evaluate general health, organ function, and inflammatory markers.
Questions to ask at this appointment:
- “Given my symptoms, should I have imaging of my chest?”
- “What are you looking for with these blood tests?”
- “How long should we wait before the next step if symptoms continue?”
- “Should I see a pulmonologist or a thoracic specialist?”
Step 2: Imaging Tests
Imaging is the cornerstone of initial lung cancer evaluation. Here is how each test is used:
Chest X-Ray
The simplest and most accessible imaging test. A chest X-ray can identify large masses, significant fluid around the lungs, and major structural changes. However, it misses small or early-stage tumors reliably — it is not sensitive enough to be used as a screening tool.
CT Scan (Computed Tomography)
The gold standard for lung evaluation. A chest CT produces detailed cross-sectional images and can detect tumors as small as a few millimeters. It also shows:
- Tumor size, shape, and location within the lung
- Enlarged lymph nodes in the chest
- Evidence of spread to nearby structures
- Pleural effusion (fluid around the lungs)
PET Scan (Positron Emission Tomography)
A PET scan uses a radioactive glucose tracer to identify cells with abnormally high metabolic activity — which cancer cells characteristically display. It is particularly valuable for:
- Determining whether abnormalities seen on CT are metabolically active (likely cancer) or dormant (less likely)
- Identifying lymph node involvement
- Detecting distant metastases not visible on CT
PET-CT (Combined Scan)
The most powerful staging tool. A combined PET-CT overlays metabolic data from the PET scan onto the anatomical detail of the CT, giving oncologists a comprehensive picture of the cancer’s extent throughout the body.
Brain MRI
Lung cancer has a strong predilection for spreading to the brain — especially SCLC and certain NSCLC subtypes. Brain MRI is recommended at diagnosis for:
- All patients with SCLC
- NSCLC patients with Stage II or higher disease (recommended at IIA; considered at IB)
- Any patient with neurological symptoms
Low-Dose CT (LDCT) for Screening
This is distinct from a diagnostic CT. LDCT uses significantly less radiation and is specifically designed for screening in high-risk individuals with no symptoms. See Section 9 for full details on screening eligibility.
| Imaging Test | What It Shows | When It’s Used |
|---|---|---|
| Chest X-ray | Large masses, major changes | Initial evaluation, limited sensitivity |
| CT scan | Tumors >3mm, nodal involvement, structure | Primary diagnostic and staging tool |
| PET scan | Metabolic activity, spread | Staging, treatment response monitoring |
| Brain MRI | Brain metastases | At diagnosis for SCLC; selected NSCLC |
| LDCT | Small early nodules | Annual screening in high-risk individuals |
Step 3: Biopsy — The Definitive Diagnosis
A biopsy — the removal and microscopic examination of tumor tissue — is the only way to definitively diagnose lung cancer and determine its specific type and molecular characteristics. There is no blood test that diagnoses lung cancer definitively on its own (though liquid biopsy, discussed below, is advancing rapidly).
Methods of obtaining a lung biopsy:
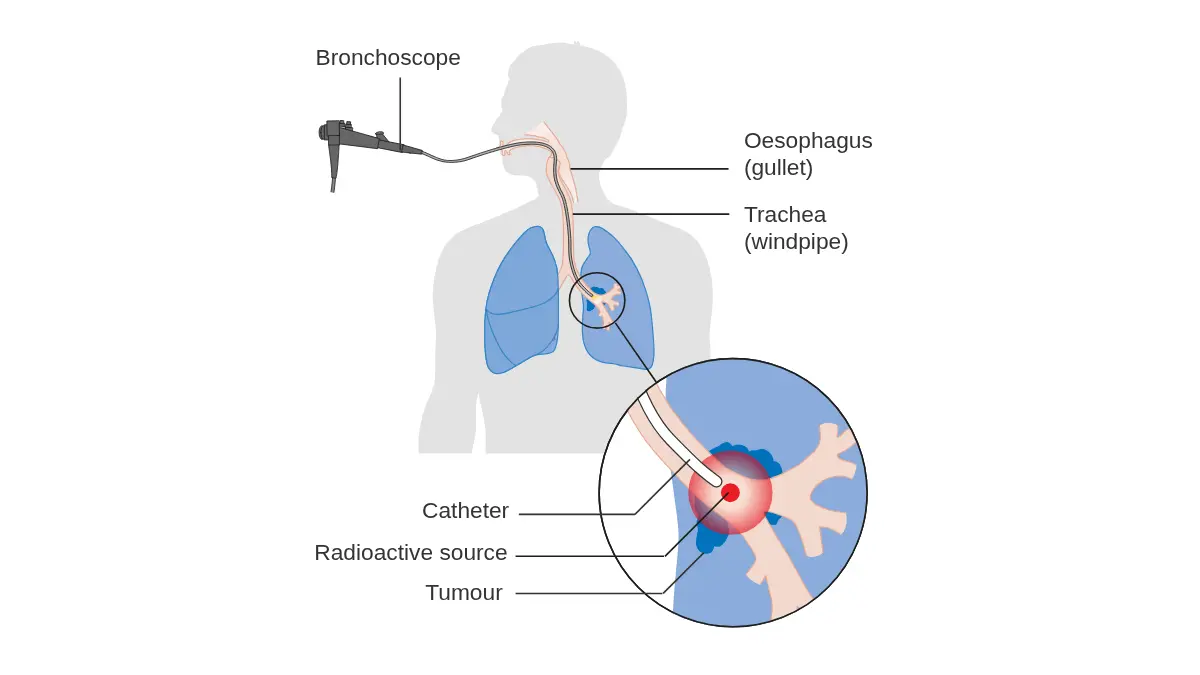
Bronchoscopy: A flexible tube (bronchoscope) is passed through the mouth or nose, down the throat, through the vocal cords, and into the airways. The pulmonologist can directly visualize central tumors and obtain tissue samples. Modern bronchoscopes include:
- Endobronchial Ultrasound (EBUS): Allows real-time ultrasound imaging through the bronchoscope to guide biopsy of lymph nodes or tumors adjacent to central airways. EBUS has largely replaced mediastinoscopy for lymph node staging in many centers.
- Navigational bronchoscopy: GPS-like technology that guides the bronchoscope to peripheral lesions not accessible by standard bronchoscopy.
CT-Guided Needle Biopsy (Percutaneous biopsy): For peripheral tumors, a radiologist uses CT imaging to guide a fine needle through the chest wall and into the tumor. This is done under local anesthesia and sedation. Complications include a small risk of pneumothorax (collapsed lung).
Surgical biopsy (VATS — Video-Assisted Thoracoscopic Surgery): When less invasive methods cannot obtain adequate tissue, minimally invasive chest surgery is used. The surgeon inserts a camera and instruments through small incisions between the ribs.
Sputum cytology: Examination of cells shed into mucus coughed up from the lungs. This is a non-invasive test, but it has significant limitations in sensitivity and is typically reserved for situations where other biopsy methods are not feasible.
Thoracentesis: When fluid has accumulated around the lungs (pleural effusion), a sample can be drained and tested for cancer cells. This is both diagnostic and therapeutic (relieving breathlessness caused by the fluid).
Understanding your biopsy results is critically important. Our detailed guide on how to interpret biopsy results and timelines walks you through each component of a pathology report in patient-friendly language.
Biomarker Testing: The Most Important Test You May Not Know About
Here is a gap that all three top-ranking competitors fail to adequately address for patients: comprehensive biomarker (molecular) testing is not optional for NSCLC patients — it is essential.
Biomarker testing analyzes the DNA of your tumor tissue to identify specific mutations that drive tumor growth. Why does this matter? Because certain mutations can be specifically targeted by precision drugs — converting what would otherwise be a difficult-to-treat cancer into one that responds powerfully to an oral medication taken at home.
Who should get comprehensive biomarker testing?
- All patients with non-squamous NSCLC (adenocarcinoma, large cell carcinoma)
- All patients with squamous cell NSCLC (increasingly recommended, as targetable alterations are found in a subset)
- Any SCLC patient where specific testing may guide clinical trial eligibility
What is tested in a comprehensive biomarker panel? A modern comprehensive molecular profile typically includes:
- DNA sequencing for point mutations and insertions/deletions (EGFR, KRAS, BRAF, MET)
- Gene rearrangement testing (ALK, ROS1, RET, NTRK)
- Copy number analysis (MET amplification, ERBB2 amplification)
- PD-L1 expression (by immunohistochemistry — determines immunotherapy eligibility and dose selection)
- TMB (Tumor Mutational Burden) — predicts immunotherapy response
The 2025–2026 coverage gap: The American Lung Association’s 2025 State of Lung Cancer report flagged that comprehensive biomarker testing is still not universally available or covered — a major inequality in lung cancer care, particularly in rural areas and states with lower screening and testing rates.
What This Means For You: At your first oncology appointment, ask: “Has comprehensive molecular profiling been ordered for my tumor? Will I be tested for all FDA-recognized actionable alterations?” Do not assume this is being done automatically.
Liquid Biopsy: The Future of Lung Cancer Diagnosis Is Already Here
Liquid biopsy is one of the most significant diagnostic advances in lung cancer medicine — and one of the most poorly explained to patients by mainstream health websites.
What is a liquid biopsy?
A liquid biopsy is a simple blood draw that detects and analyzes fragments of tumor DNA circulating in the bloodstream — called circulating tumor DNA (ctDNA). When cancer cells die, they release snippets of their DNA into the blood. A liquid biopsy isolates these fragments and sequences them for cancer-driving mutations.
How is liquid biopsy used in lung cancer in 2026?
- When tissue biopsy is not possible or not safe (e.g., tumor location makes surgical biopsy too risky)
- For molecular profiling when tissue biopsy yields insufficient material
- Monitoring treatment response: Rising ctDNA levels can predict relapse before it shows on imaging
- Detecting acquired resistance mutations when a targeted therapy stops working (the tumor DNA in the blood often reveals the new mutation driving resistance)
- Emerging role in early detection: Research is actively evaluating liquid biopsy as a future screening tool for high-risk populations
Current limitations:
- Sensitivity is lower than tissue biopsy (can miss mutations present in small quantities)
- A negative liquid biopsy does not rule out lung cancer — it may mean ctDNA levels are too low to detect
- Not yet approved or validated as a standalone primary screening method
The Multidisciplinary Tumor Board
One of the most important — and most frequently overlooked — aspects of lung cancer diagnosis and treatment planning is the multidisciplinary tumor board (MDT). This is a formal meeting of specialists from multiple disciplines who review each patient’s case together to develop a coordinated, consensus treatment plan.
A typical lung cancer tumor board includes:
- Pulmonologist
- Thoracic surgeon
- Radiation oncologist
- Medical oncologist
- Pathologist
- Radiologist (diagnostic imaging specialist)
- Palliative care physician (ideally)
- Oncology nurse navigator
- Social worker
Why it matters to you: A tumor board catches errors, prevents over- or under-treatment, and ensures you receive the benefit of multiple expert perspectives simultaneously. Studies consistently show that patients discussed at tumor boards receive treatment more aligned with current guidelines.
What to do: Ask your care team: “Will my case be reviewed by a multidisciplinary tumor board before treatment begins?” At any major cancer center, the answer should be yes. If it is not offered, ask for it or consider a second opinion at a center that provides this standard of care.
The AAFP clinical reference on lung cancer provides family physician-level guidance on when and how to refer patients to multidisciplinary teams.
Lung Cancer Staging — What Every Stage Really Means for Your Treatment
Why Staging Matters More Than Any Other Single Factor
Staging is the process of determining how far lung cancer has spread within the body. It is the single most important factor in determining treatment options and is a primary driver of prognosis. Two patients with the same type of lung cancer but different stages will often receive completely different treatments — and have dramatically different outcomes.
However, staging is not destiny. A growing number of patients with Stage IV lung cancer are living far beyond what historical statistics would predict, thanks to targeted therapy. Your stage tells you what is, not necessarily what will be.
The TNM Staging System for NSCLC
NSCLC is staged using the TNM system — the international standard from the American Joint Committee on Cancer (AJCC), 8th edition:
- T (Tumor): Describes the primary tumor — its size, location, and whether it has invaded nearby structures.
- N (Nodes): Describes lymph node involvement — which lymph nodes, if any, contain cancer.
- M (Metastasis): Describes whether the cancer has spread to distant organs.
T Score Reference:
| T Score | Tumor Characteristics | Real-World Size Comparison |
|---|---|---|
| T1a | ≤1 cm, no invasion | Smaller than a large blueberry |
| T1b | 1–2 cm | Roughly the size of a grape |
| T1c | 2–3 cm | About the size of a large grape |
| T2a | 3–4 cm, or specific invasion | Roughly the size of a walnut |
| T2b | >4–5 cm | Approaching the size of a golf ball (4.3 cm) |
| T3 | >5–7 cm, or invasion of chest wall/diaphragm | Larger than a golf ball |
| T4 | >7 cm, or invasion of heart/great vessels/trachea | Major local invasion |
NSCLC Stages: A Patient-Centered Breakdown
Stage 0 (Occult / In Situ)
Cancer cells are detectable in mucus or liquid biopsy specimens, but no tumor is visible on imaging or biopsy. This is extremely rare — sometimes called “occult” carcinoma. When a tumor is visible on imaging but too small to have invaded surrounding tissue, it is classified as Stage 0 in situ.
Stage I: Localized — The Most Curable Stage
Stage I lung cancer is confined to the lung, with no lymph node involvement and no distant spread.
- Stage IA (T1, N0, M0): Tumor ≤3 cm, within the lung, no lymph node involvement.
- Stage IB (T2a, N0, M0): Tumor 3–4 cm, or with specific local features, no lymph node involvement.
Treatment: Surgery is the preferred treatment for most Stage I NSCLC patients. Specifically:
- Lobectomy (removal of the affected lung lobe) remains the gold standard.
- For patients with limited lung function, segmentectomy or wedge resection are alternatives.
- Adjuvant targeted therapy (post-surgery) is now standard for certain patients with EGFR or ALK mutations in Stage IB tumors >4 cm.
For detailed information about Stage I outcomes, our guide on Stage 1 lung cancer survival rates provides the latest survival data with stage-by-stage breakdowns.
5-year survival: 64–92% (varies by substage and treatment received).
Stage II: Locally Advanced — Still Highly Treatable
Stage II involves either a larger tumor or spread to a limited number of nearby lymph nodes — but no distant metastasis.
- Stage IIA: T2b, N0, M0 — tumor 4–5 cm, no lymph node involvement.
- Stage IIB: T3, N0 or T1–2, N1, M0 — larger tumor OR spread to lymph nodes in the same lung.
Treatment: Surgery remains the cornerstone, often combined with:
- Adjuvant chemotherapy (for larger tumors)
- Adjuvant targeted therapy (for EGFR/ALK-positive tumors)
- Radiation if surgery is not possible
5-year survival: 36–53% (depending on substage and treatment).
Stage III: Locally Advanced — Complex, But Often Treatable
Stage III is the most clinically diverse and nuanced category in NSCLC staging. It encompasses a wide spectrum — from patients who are candidates for potentially curative surgery to those requiring definitive chemoradiation.
- Stage IIIA: Cancer has spread to ipsilateral mediastinal lymph nodes or to limited contralateral nodes. Some Stage IIIA tumors are resectable.
- Stage IIIB: Cancer has spread to contralateral mediastinal nodes or supraclavicular nodes. Typically not resectable.
- Stage IIIC: Extensive mediastinal lymph node involvement. Typically treated with definitive chemoradiation.
Treatment: The standard approach for most Stage III NSCLC is:
- Concurrent chemoradiation (simultaneous chemotherapy + radiation)
- Followed by durvalumab (Imfinzi) immunotherapy consolidation — a practice-changing 2018 approval that extended median progression-free survival from 5.6 months to 16.8 months (PACIFIC trial)
- For selected Stage IIIA patients: surgery may be possible after induction therapy
5-year survival: 10–36% (broad range due to substage heterogeneity).
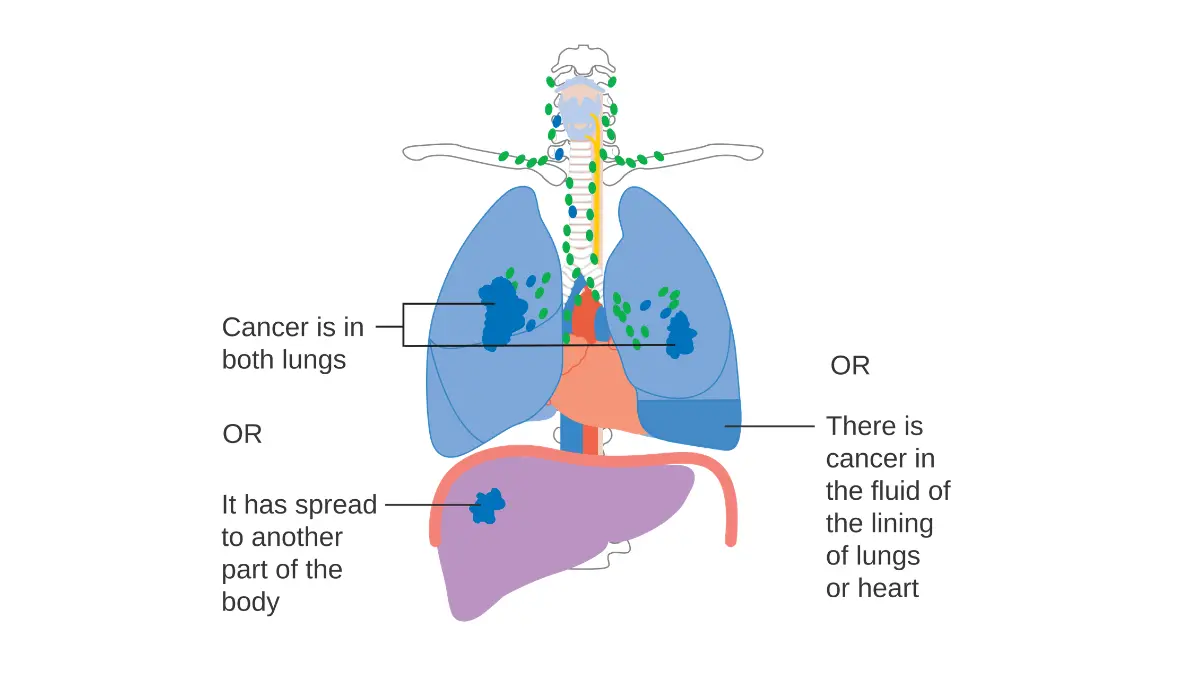
Stage IV: Metastatic Lung Cancer — Manageable More Often Than You Think
Stage IV means lung cancer has spread to the other lung, the fluid around the lungs (pleural or pericardial effusion), or to distant organs.
- Stage IVA: Single distant site involved.
- Stage IVB: Multiple distant metastatic sites.
The critical nuance most competitors miss: The overall Stage IV 5-year survival of approximately 9% is a population-wide average that includes patients diagnosed before the modern era of targeted therapy. In 2026, the picture for specific molecular subtypes looks dramatically different:
- Patients with EGFR-mutant NSCLC treated with osimertinib: median overall survival of 38.6 months (FLAURA trial), with many patients surviving 4–5+ years.
- Patients with ALK-rearranged NSCLC treated with alectinib: median PFS >34 months in some trials.
- Patients with high PD-L1 expression (≥50%) treated with pembrolizumab: median overall survival of 26.3 months (KEYNOTE-024).
These are not cherry-picked outliers. They are the treatment outcomes that are now achievable for specific molecular subgroups.
| Stage | TNM | 5-Yr Survival (All Comers) | Potential With Targeted Therapy |
|---|---|---|---|
| IA1–IA3 | T1, N0, M0 | 77–92% | N/A (surgery curative in most |
| IB | T2a, N0, M0 | 64% | N/A (adjuvant therapy added |
| IIA | T2b, N0, M0 | 53% | Adjuvant osimertinib if EGFR+ |
| IIB | T3, N0 or T1-2, N1, M0 | 36% | Adjuvant therapy benefits |
| IIIA–C | Various N2-3 | 10–36% | Chemorad + immunotherapy |
| IVA | Single mets | ~15–20% | 38+ months median OS if EGFR+ |
| IVB | Multiple mets | ~7–9% | Substantial improvement with molecular matching |
Small Cell Lung Cancer Staging
SCLC does not use the same detailed TNM system routinely. Instead, the classic two-stage system is used clinically:
- Limited Stage: One side of the chest, treatable within one radiation field. About one-third of SCLC diagnoses are limited stage.
- Extensive Stage: Spread beyond the chest or involving the opposite lung. About two-thirds of SCLC patients present at extensive stage.
Our dedicated guide on small cell lung cancer survival rates provides detailed prognosis data for both limited and extensive-stage SCLC.
“I Just Got Staged — Now What?”
Receiving a stage can feel like receiving a sentence. It is not. Here are the most important immediate steps:
- Request a written copy of your staging report. You have the legal right to your medical records.
- Ask for a full explanation of what your specific T, N, and M classification means.
- Request a multidisciplinary tumor board review before any treatment begins.
- Consider seeking a second opinion at an NCI-designated cancer center — this is universally encouraged in oncology and will not delay your care.
- Ask about clinical trial eligibility. Even at early stages, clinical trials may offer you access to next-generation therapies.
- Begin palliative care consultation regardless of stage. More on this in Section 7.
Remember: Your stage describes the extent of your cancer today. It is not a fixed prediction of your future.
Lung Cancer Treatment — Every Option Explained (2026 Updated)
The Treatment Revolution: 98 FDA-Approved Therapies and Counting
As of August 2025, the FDA has approved 98 different treatment approaches for lung cancer — a number that reflects the extraordinary pace of innovation in this field, according to data from LUNGevity Foundation. Eleven of those approvals occurred between 2024 and 2026 alone, establishing NSCLC as one of the most actively developing areas in oncology.
This proliferation of options is genuinely good news. But it also means that treatment selection requires true expertise — ideally the combined input of a multidisciplinary team experienced specifically in thoracic oncology.
Treatment in 2026 is determined by:
- Cancer type (NSCLC vs. SCLC, and subtype within NSCLC)
- Stage (local vs. regional vs. metastatic)
- Molecular profile (targetable mutations present or absent)
- PD-L1 expression level (immunotherapy eligibility)
- Performance status (your overall health and functional capacity)
- Comorbidities (other health conditions)
- Patient preferences (quality of life priorities, tolerance for specific side effects)
For a comprehensive guide to FDA-approved lung cancer drugs updated through 2026, our resource on lung cancer FDA-approved treatment drugs provides a full clinical reference.
Surgery: The Cornerstone of Early-Stage Treatment
Surgery offers the best chance of cure for early-stage NSCLC. The goal is to remove the tumor with adequate margins of healthy tissue, minimizing the chance that any cancer cells remain.
Types of lung surgery, from most conservative to most extensive:
| Surgery Type | Tissue Removed | When Used | Recovery Time |
|---|---|---|---|
| Wedge resection | Tumor + small wedge of surrounding lung | Small peripheral tumors; poor lung function | 2–4 weeks |
| Segmentectomy | One segment of a lobe | Small tumors in patients with limited reserve | 3–5 weeks |
| Lobectomy | One entire lobe (most common) | Standard of care for resectable Stage I–II | 4–6 weeks |
| Sleeve resection | Section of airway + adjacent lobe | Central tumors involving airway | 4–8 weeks |
| Pneumonectomy | Entire lung | Advanced local disease; last resort | 6–12 weeks |
Minimally invasive surgery — specifically Video-Assisted Thoracoscopic Surgery (VATS) and Robotic-Assisted Thoracic Surgery (RATS) — allows surgeons to perform lobectomies and segmentectomies through small incisions using cameras and robotic instruments. These approaches result in:
- Less postoperative pain
- Shorter hospital stays (typically 2–4 days vs. 5–7 days for open surgery)
- Faster return to normal activity
- Lower complication rates in experienced hands
Neoadjuvant therapy (treatment given before surgery to shrink the tumor) is increasingly standard for Stage II and selected Stage III patients. In 2024–2026, neoadjuvant chemotherapy plus nivolumab (immunotherapy) became a standard approach for resectable Stage II–IIIA NSCLC, based on the CheckMate 816 trial showing a pathologic complete response rate of 24% — meaning nearly 1 in 4 patients had no detectable cancer at surgery.
Adjuvant therapy (treatment after surgery to reduce recurrence risk) represents another major 2025–2026 advancement:
- Osimertinib (Tagrisso) for EGFR-mutant NSCLC after complete resection: shown to reduce recurrence risk by 83% vs. placebo (ADAURA trial)
- Alectinib for ALK-positive NSCLC after complete resection: shown to dramatically reduce recurrence
- Adjuvant atezolizumab (immunotherapy) for PD-L1-positive resected NSCLC
Radiation Therapy: Precise, Powerful, and Increasingly Curative
Radiation therapy uses high-energy beams to damage the DNA of cancer cells, preventing them from dividing. In 2026, radiation oncology for lung cancer has advanced dramatically from the broad-field treatments of prior decades.
For detailed information on how radiation is used in cancer treatment generally, our comprehensive overview of radiation therapy approaches provides additional context.
Key radiation approaches for lung cancer:
Conventional Radiation (External Beam Radiation Therapy, EBRT): Delivered in daily fractions over 5–7 weeks. Used primarily for Stage III unresectable NSCLC in combination with chemotherapy (chemoradiation).
Stereotactic Body Radiation Therapy (SBRT) / SABR: A major advancement for patients with early-stage NSCLC who cannot tolerate surgery (due to poor lung function, advanced age, or comorbidities). SBRT delivers very high doses of precisely focused radiation in just 3–5 sessions — compared to 25–35 sessions for conventional radiation. Studies show local control rates of 85–95% at 3 years for Stage I NSCLC treated with SBRT — comparable to surgical outcomes in selected patients.
Prophylactic Cranial Irradiation (PCI): For limited-stage SCLC patients who achieve complete remission with chemotherapy, PCI to the brain reduces the risk of brain metastasis development and improves long-term survival.
Palliative Radiation: Even when cure is not the goal, radiation is extraordinarily effective for:
- Relieving bone pain from metastases (often within days)
- Treating brain metastases (either whole-brain or SRS — stereotactic radiosurgery — for 1–4 brain mets)
- Relieving SVC syndrome
- Reducing hemoptysis
Chemotherapy: Still Essential, Now Often Combined
Chemotherapy uses drugs that target rapidly dividing cells — killing cancer cells but also affecting some normal tissues, which accounts for side effects.
For a thorough review of what to expect during treatment and how to manage side effects, our in-depth guide to chemotherapy in 2026 is an essential read.
Standard chemotherapy regimens in lung cancer:
- Non-squamous NSCLC: Cisplatin (or carboplatin) + pemetrexed — the most widely used doublet for advanced adenocarcinoma.
- Squamous NSCLC: Cisplatin + gemcitabine, or carboplatin + paclitaxel.
- SCLC (both stages): Cisplatin (or carboplatin) + etoposide — delivered in cycles every 3 weeks.
Chemotherapy may be used:
- Neoadjuvant (before surgery) to shrink tumors
- Concurrent with radiation (chemoradiation) for Stage III disease
- Adjuvant (after surgery) to reduce recurrence risk
- First-line or later-line for advanced/metastatic disease without targetable mutations
A critical 2026 point: For most patients with advanced NSCLC who have targetable mutations, targeted therapy — not chemotherapy — is now the preferred first-line treatment. Chemotherapy’s role is being increasingly reserved for patients without targetable alterations, or combined with immunotherapy.
Targeted Therapy: Precision Medicine at Its Most Powerful
This is where lung cancer treatment has made its most dramatic strides. Targeted therapies are designed to block specific molecular pathways that drive tumor growth in individual patients. They are generally taken as daily oral pills or capsules — a major quality-of-life advantage over IV chemotherapy.
Key targeted therapies approved through 2026:
EGFR-Mutant NSCLC (the most common targetable subtype):
- Osimertinib (Tagrisso) — the current gold standard for EGFR exon 19 deletion or L858R mutation. Third-generation EGFR inhibitor; crosses the blood-brain barrier (important for preventing/treating brain metastases). Now approved in both metastatic and adjuvant (post-surgery) settings.
- Amivantamab + Lazertinib (MARIPOSA trial): A combination of a bispecific antibody and a third-generation EGFR TKI, showing improved progression-free survival vs. osimertinib alone. Approved 2024.
- Sunvozertinib: FDA accelerated approval July 2025 — specifically for EGFR Exon 20 insertion mutations, a subtype previously without a strong targeted option.
ALK-Rearranged NSCLC:
- Alectinib (Alecensa): Second-generation ALK inhibitor; median PFS >34 months in the first-line setting. Now also approved as adjuvant therapy.
- Brigatinib (Alunbrig): Active even after alectinib resistance in some cases.
- Lorlatinib (Lorbrena): Third-generation; most potent activity against resistant disease and brain metastases.
KRAS-Mutant NSCLC:
- Sotorasib (Lumakras): First approved KRAS inhibitor (KRAS G12C mutation).
- Adagrasib (Krazati): Second approved KRAS G12C inhibitor, with strong intracranial activity.
- 2026 Frontier: Zoldonrasib (KRAS G12D inhibitor) showed “durable clinical efficacy” in AACR 2026 — the first agent targeting the most common KRAS mutation subtype.
For a complete reference on these and other agents, the NCI’s comprehensive NSCLC treatment PDQ provides the most current clinical guidance.
The recent 2025 review published in PMC on NSCLC management updates provides an excellent overview of how the treatment landscape has transformed since 2024.
Immunotherapy: Teaching Your Immune System to Fight
Immunotherapy has transformed the treatment of lung cancer in patients without targetable mutations — and is now being evaluated in combination with targeted therapy for patients who do have mutations.
For a thorough explanation of how immunotherapy works in cancer treatment, our guide on how immunotherapy works provides a patient-friendly and scientifically rigorous explanation.
How checkpoint inhibitors work:
Cancer cells evade immune destruction by expressing proteins — particularly PD-L1 — that bind to receptors on immune T-cells and essentially tell them: “Don’t attack me.” Checkpoint inhibitors block this interaction, allowing T-cells to recognize and destroy cancer cells.
Key approved immunotherapy agents for lung cancer:
| Drug | Target | Key Approval(s) |
|---|---|---|
| Pembrolizumab (Keytruda) | PD-1 | First-line Stage IV NSCLC (PD-L1 ≥1%); monotherapy if PD-L1 ≥50% |
| Nivolumab (Opdivo) | PD-1 | Second-line NSCLC; neoadjuvant + adjuvant |
| Atezolizumab (Tecentriq) | PD-L1 | NSCLC (combination); extensive-stage SCLC |
| Durvalumab (Imfinzi) | PD-L1 | Stage III NSCLC consolidation after chemoradiation |
| Nivolumab + Ipilimumab | PD-1 + CTLA-4 | First-line advanced NSCLC (PD-L1 ≥1%) |
Side effects of immunotherapy differ fundamentally from chemotherapy. Because they activate the immune system, they can cause inflammation in virtually any organ:
- Pneumonitis (lung inflammation): Can be severe; requires prompt steroid treatment.
- Colitis: Diarrhea, abdominal cramping.
- Endocrinopathies: Thyroid dysfunction, adrenal insufficiency, pituitary problems.
- Hepatitis: Elevated liver enzymes.
- Skin reactions: Rash, vitiligo-like depigmentation.
These side effects, called immune-related adverse events (irAEs), can be serious but are manageable when caught early. Report any new or changing symptoms to your oncology team promptly.
Emerging Treatments: The 2026 Frontier
Several new classes of drugs are either newly approved or in advanced trials in 2026:
Antibody-Drug Conjugates (ADCs): Engineered antibodies that carry a chemotherapy payload directly to cancer cells expressing a specific surface protein. The antibody finds the cancer cell; the chemotherapy payload kills it — with far less collateral damage to normal tissue than traditional chemotherapy. Early ADC data in lung cancer (including telisotuzumab vedotin for MET-overexpressing NSCLC) is promising.
Bispecific Antibodies: Amivantamab (RYBREVANT) targets both EGFR and MET simultaneously — the first bispecific antibody approved for lung cancer. A subcutaneous (under-skin injection) formulation was approved in February 2026, dramatically improving convenience.
Next-generation KRAS inhibitors: Elisrasib, a next-generation KRAS G12C inhibitor, showed “robust and durable efficacy” in advanced NSCLC at AACR 2026 — representing the next wave of precision KRAS targeting.
Clinical trials offer access to these and other cutting-edge treatments before they receive full approval. There is no fee to enroll in a clinical trial — in fact, the cost of experimental treatment is covered by the trial sponsor. You can search all open lung cancer trials at ClinicalTrials.gov.
Palliative Care: The Most Misunderstood Treatment in Oncology
Almost every lung cancer website frames palliative care as an end-of-life option. This framing is clinically wrong — and it causes real harm, because it prevents patients from accessing a powerful form of care that improves both quality and quantity of life.
What palliative care actually is:
Palliative care is specialized medical care focused on symptom management, emotional support, and quality of life for patients with serious illness — at any stage of disease. It is provided alongside curative or life-prolonging treatment, not instead of it.
The landmark evidence: A 2010 study published in the New England Journal of Medicine (Temel et al.) found that patients with advanced NSCLC who received early palliative care integration alongside standard oncologic treatment:
- Had better quality of life
- Had fewer aggressive interventions near the end of life
- And — counterintuitively — lived an average of 2.7 months longer than those who received standard care alone
This study fundamentally changed oncology guidelines. ASCO and NCCN now recommend palliative care integration from the time of diagnosis for any patient with advanced lung cancer.
What a palliative care team can help with:
- Breathlessness management (pursed-lip breathing, fans, opioids at specific doses, oxygen)
- Pain from bone metastases, chest wall invasion, or Pancoast tumors
- Nausea and appetite loss from chemotherapy
- Fatigue management
- Psychological distress, anxiety, and depression
- Advance care planning (living wills, healthcare proxy designation)
- Family and caregiver support
What This Means For You: At your first oncology appointment, say these words: “I would like a referral to palliative care.” It is not giving up. It is accessing a proven, evidence-based service that makes treatment more tolerable and your life better.
Lung Cancer Prognosis, Survival Rates & Life After Diagnosis
Understanding Survival Statistics: What They Mean — and What They Don’t
Survival statistics are population averages. They describe what happened to groups of people diagnosed with similar cancers in the past — often 5–10 years ago, before many of today’s treatments existed. They do not, and cannot, predict what will happen to you as an individual.
The 5-year relative survival rate means: of all people diagnosed with this type and stage of lung cancer, what percentage were still alive 5 years later, compared to the general population? It explicitly does not mean that 5 years is a ceiling. Many patients live 10, 15, or 20+ years after a lung cancer diagnosis.
Three reasons the statistics are more optimistic than they appear:
- They lag current treatment by 5–10 years. Data published in 2026 reflects outcomes of patients diagnosed in 2016–2021 — before the most transformative targeted therapy approvals.
- They do not separate patients by molecular subtype. The average includes patients without targetable mutations whose outcomes are worse, which pulls down the numbers for those with excellent molecular profiles.
- Survival at specialized cancer centers consistently outperforms national averages.
Current Lung Cancer Survival Rates by Stage (2026 Data)
According to SEER Cancer Statistics and the American Lung Association’s 2025 State of Lung Cancer report:
- Overall 5-year survival (all stages combined): 27% — nearly double the 15% seen in 1997.
- Localized (Stage I) disease: 65% — rising to 92% for the smallest Stage I tumors.
- Regional (Stage II–III) disease: 36%.
- Distant (Stage IV) disease: 9% overall; substantially higher for specific molecular subtypes.
- American Lung Association 2025 national average: 29.7%.
State-by-state variation is striking:
- Best outcomes: Rhode Island (37.6% 5-year survival)
- Worst outcomes: Alabama (22.7% 5-year survival)
This near-15 percentage point gap between states reflects differences in access to comprehensive biomarker testing, early diagnosis rates, availability of specialized oncology centers, and smoking cessation resources — not differences in the biology of the disease.
With modern targeted therapy, the picture for specific molecular subgroups is dramatically better:
| Molecular Subtype | Treatment | Median Overall Survival |
|---|---|---|
| EGFR exon 19 del / L858R | Osimertinib (FLAURA trial) | 38.6 months |
| ALK rearrangement | Alectinib (ALEX trial) | Not reached at 5 years in many analyses |
| KRAS G12C | Sotorasib or Adagrasib | ~12–15 months (improving) |
| PD-L1 ≥50% (no mutation) | Pembrolizumab (KEYNOTE-024) | 26.3 months |
| PD-L1 <1% (no mutation) | Chemo + immunotherapy | ~14–16 months |
| SCLC limited stage | Chemo + radiation | 12–20 months (long-term remission in ~10%) |
| SCLC extensive stage | Chemo + immunotherapy | ~12 months |
Factors That Improve Lung Cancer Prognosis
The following factors are consistently associated with better outcomes — and several are within your control:
Strongest predictors of better outcomes:
- Early stage at diagnosis (the single biggest factor — screened populations have dramatically better survival)
- Presence of an actionable genomic alteration with a matched targeted therapy
- High PD-L1 expression (≥50%) in patients without targetable mutations
- Good performance status (overall health and physical function)
- Care at an NCI-designated cancer center or high-volume thoracic oncology program
- Comprehensive biomarker testing and access to all approved treatments
- Early integration of palliative care (proven survival benefit)
Lifestyle factors that support treatment outcomes:
- Smoking cessation after diagnosis: reduces risk of second primary cancer by 3.5-fold; may improve response to immunotherapy
- Maintaining adequate nutrition: critical during treatment
- Physical activity (within safe limits): reduces fatigue, depression, and may improve treatment response
- Sleep quality: treatment-related fatigue and anxiety are worsened by poor sleep. Use our Sleep Calculator to help identify your optimal sleep windows and circadian timing during treatment.
- Maintaining healthy body weight: use our BMI Calculator to monitor your weight status; unintentional weight loss during treatment is a clinical concern that should be reported to your care team.
- Hydration: chemotherapy requires adequate fluid intake to protect kidneys. Our Water Intake Calculator can help you calculate your daily hydration goals based on your body weight and treatment status.
Mental Health and Lung Cancer: The Gap Everybody Ignores
This section does not exist in any major competing lung cancer guide. That absence is a failure of patient care.
The mental health reality of lung cancer:
- Anxiety and depression are 2–3 times more prevalent in lung cancer patients than in the general population.
- Scanxiety — the intense psychological distress experienced before and after follow-up imaging — is a near-universal experience that significantly diminishes quality of life.
- Lung cancer patients face a unique stigma: the assumption that they “caused” their own disease by smoking. This guilt and shame — even in never-smokers who face it from others — is a documented contributor to delayed care-seeking and psychological distress.
- AACR 2026 presented dedicated research on mental health needs in patients with EGFR-mutated NSCLC, highlighting that even patients with the “best-prognosis” molecular subtype experience significant psychological burden.
Practical mental health support:
- Ask for a mental health referral at diagnosis — ideally to a psycho-oncologist (a specialist in the psychological care of cancer patients).
- Cognitive-behavioral therapy (CBT) has strong evidence for anxiety and depression in cancer patients.
- Support groups (both in-person and online) reduce isolation and provide practical wisdom from patients who have navigated similar experiences.
- GO2 Foundation, LUNGevity, and the American Lung Association all offer structured peer support programs.
For a comprehensive guide to managing depression, including evidence-based strategies and when to seek professional help, our resource on depression and mental health provides clinical context.
Physical Activity During and After Lung Cancer Treatment
Exercise has moved from “be gentle with yourself” advice to an evidence-based intervention in cancer care. Research consistently shows that regular, appropriate-intensity physical activity during cancer treatment:
- Reduces treatment-related fatigue (the most common cancer treatment side effect)
- Improves psychological well-being and reduces depression and anxiety
- Maintains muscle mass and physical function
- May improve immunotherapy response (emerging data)
- Reduces risk of second malignancy
Guidelines: The American College of Sports Medicine Cancer Guidelines recommend:
- At least 150 minutes of moderate-intensity aerobic activity per week for cancer survivors
- 2–3 sessions of resistance training per week
Always consult your oncologist before beginning or intensifying exercise during active treatment. To identify safe exercise intensity zones during treatment or recovery, our Heart Rate Zone Calculator helps you determine aerobic training zones based on your age and resting heart rate.
Nutrition During Lung Cancer Treatment
Adequate nutrition is not optional during lung cancer treatment — it is a clinical necessity. Malnutrition during treatment is associated with:
- Increased treatment toxicity
- Reduced ability to complete planned treatment courses
- Higher rates of infection
- Worse survival outcomes
Key nutritional priorities during treatment:
- Adequate protein intake to preserve muscle mass during chemotherapy-related catabolism. Our Protein Intake Calculator can help calculate your personalized daily protein targets.
- Calorie sufficiency: Unintentional weight loss of >5% during treatment is a red flag that should prompt referral to an oncology dietitian.
- Managing treatment-related eating challenges: Nausea, taste changes, mouth sores, and early satiety are all manageable with targeted interventions — ask your care team for a dietitian referral.
Monitoring After Treatment: What Follow-Up Looks Like
After completing primary treatment for lung cancer, you will enter a structured surveillance program designed to detect recurrence early:
Typical follow-up schedule:
- First 2 years: CT scan every 3–6 months (frequency depends on stage and treatment received)
- Years 2–5: CT scan every 6 months
- Beyond 5 years: Annual chest CT
- Brain MRI: More frequent monitoring if brain metastases were present or resected
What you are watching for:
- New or growing pulmonary nodules
- New symptoms (bone pain, headaches, weight loss)
- Rising tumor markers (where applicable)
- Second primary lung cancer (especially in former or current smokers)
Liquid biopsy for monitoring: Emerging research supports the use of ctDNA monitoring to detect molecular recurrence weeks to months before imaging-detectable relapse. Ask your oncologist about this option.
Prevention, Screening, Caregiver Guide & Financial Toolkit
Can Lung Cancer Be Prevented? Evidence-Based Strategies That Work
Lung cancer cannot be completely prevented, but the evidence is overwhelming that specific, actionable steps can dramatically reduce risk.
What works — with strong evidence:
1. Smoking Cessation (highest impact)
- Tobacco smoking drives 80–90% of U.S. lung cancer deaths.
- Quitting at any age reduces risk, with benefits beginning within months.
- Risk reduction of 39.1% within 5 years of quitting (AAFP data).
- Most effective cessation strategy: combination of pharmacotherapy + behavioral counseling (doubles success rate vs. either alone).
- Approved medications: Varenicline (Chantix/Champix), nicotine replacement therapy (patch, gum, lozenge, inhaler), bupropion.
- FDA-approved cessation support: 1-800-QUIT-NOW (free coaching in all 50 states).
2. Radon Testing and Mitigation
- Test your home — the EPA provides guidance at epa.gov/radon.
- EPA-certified test kits: $10–$30 from hardware stores or online.
- If levels exceed 4 pCi/L, hire an EPA-listed mitigation contractor.
- Cost of mitigation: $800–$2,500 for a radon reduction system.
- This is one of the most cost-effective cancer-prevention investments available.
3. Occupational Safety
- Know your occupational carcinogen risks. Employers are required to provide MSDS (Material Safety Data Sheets) for chemical exposures.
- Use appropriate respiratory protection consistently.
- Report suspected workplace carcinogen exposures to OSHA.
- Former asbestos workers should disclose this history to their physician and discuss monitoring options.
4. Air Quality Management
- Monitor local air quality using AirNow.gov or a reliable air quality app.
- On high-pollution days (AQI >150), reduce outdoor exercise and keep windows closed.
- Use high-efficiency air filtration (HEPA filters) in sleeping areas.
- Ensure adequate kitchen ventilation, especially if using high-heat cooking methods.
Prevention Summary Checklist:
- ☐ Not smoking (or actively quitting)
- ☐ Home tested for radon
- ☐ Radon mitigated if >4 pCi/L
- ☐ Occupational carcinogen exposures minimized
- ☐ Air quality monitored on high-pollution days
- ☐ Annual lung cancer screening (if eligible — see below)
Lung Cancer Screening: Who Qualifies, What to Expect, and Why It Saves Lives
Lung cancer screening with Low-Dose CT (LDCT) is the only screening modality proven to reduce lung cancer mortality. It works because LDCT can detect lung tumors when they are still small and localized — before they cause symptoms and before they spread.
The key trial: The National Lung Screening Trial (NLST) demonstrated that annual LDCT screening in high-risk individuals reduces lung cancer mortality by up to 20% compared to standard chest X-ray screening.
Despite this evidence, only 18.2% of eligible Americans are currently being screened nationally (ALA 2025 State of Lung Cancer). This represents one of the largest gaps between evidence and practice in American medicine.
2025 USPSTF Screening Criteria — Updated (Most Competitors Still Show Old Data)
The U.S. Preventive Services Task Force updated its lung cancer screening recommendations in 2021, with the key change being a significantly expanded eligible population compared to the prior 2013 guideline:
Current USPSTF screening criteria (you must meet ALL three):
- Age 50–80 years (lowered from 55)
- 20 pack-year smoking history or more (reduced from 30 pack-years)
- Currently smoking OR quit within the past 15 years
Why this matters: The updated criteria expanded screening eligibility by approximately 5 million additional Americans, including younger smokers and those who quit more recently. If you or a loved one is between 50–54 with a 20 pack-year history, you now qualify — but many primary care clinicians are still not routinely offering screening to this newly eligible group.
What LDCT screening involves:
- 10-minute scan; no injection, no contrast dye
- Very low radiation dose (roughly equivalent to natural background radiation received in a few months)
- No claustrophobia (open, short scanner)
- Results interpreted on the Lung-RADS scoring system (1–4), which guides follow-up recommendations
If a lung nodule is found:
- Most lung nodules are not cancer — the vast majority are benign scars from old infections, lymph nodes, or other benign lesions.
- The Lung-RADS system determines follow-up: from annual continued screening (for very small stable nodules) to 6-month repeat CT (for intermediate nodules) to biopsy or PET scan (for suspicious nodules).
- Finding a nodule is not a diagnosis of cancer. It is an indication to continue monitoring.
Is LDCT screening covered?
- Medicare: Covers annual LDCT for eligible beneficiaries with a clinician order.
- Private insurance: Required to cover LDCT screening without cost-sharing under the Affordable Care Act for eligible patients.
- Medicaid: Coverage varies by state — check with your plan.
Global screening programs:
| Country | Screening Program Status |
|---|---|
| United States | Annual LDCT — USPSTF recommended for eligible individuals |
| United Kingdom | NHS Targeted Lung Health Check program (rolling out nationally) |
| Canada | Provincial programs in various stages; national recommendations pending |
| Australia | Pilot programs underway; national program recommendations under development |
The American Lung Association and Lung Cancer Research Foundation both provide patient-facing resources to help find screening programs in your area.
The Caregiver’s Complete Guide: For Families and Friends
Every major lung cancer guide is written entirely for the patient. This section is for the person beside the patient — the spouse, the adult child, the friend, the colleague who becomes a caregiver overnight without training, preparation, or a road map.
The reality of lung cancer caregiving:
Caring for someone with lung cancer is one of the most demanding experiences a person can face. Caregivers manage:
- Appointment scheduling, transportation, and medication management
- Insurance navigation, prior authorizations, and billing disputes
- Emotional support during scans, results, and bad news
- Physical care during treatment side effects
- The weight of their own fear, grief, and exhaustion — often suppressed to “be strong”
Studies consistently show that lung cancer caregivers experience rates of anxiety, depression, and burnout comparable to those of patients themselves.
Practical caregiving guidance:
Before appointments:
- Write down all questions in advance — both the patient’s and your own.
- Bring a notebook or phone to record answers (with the patient’s permission to record).
- Know the patient’s current medication list, including supplements.
- Ask the oncology team for a copy of all test results and notes.
During treatment:
- Help track symptoms, side effects, and medication timing — a simple daily log is invaluable.
- Know the signs of treatment emergencies: fever >38°C (100.4°F) during chemotherapy is a potential neutropenic emergency requiring immediate evaluation.
- Manage nutrition challenges: small, frequent, calorie-dense meals; identify what the patient can tolerate; consult an oncology dietitian.
Emotional support:
- Be present. Listening is more valuable than advice.
- Avoid toxic positivity (“Stay positive!” “You’ll beat this!”). It minimizes real feelings.
- Ask: “How are you feeling right now?” rather than assuming.
- Allow the patient to have bad days. Not every day needs to be “a fight.”
Caregiver self-care — not optional:
- You cannot pour from an empty cup. Your health matters too.
- Accept offers of help from family and friends. Be specific: “Can you bring dinner on Tuesday?”
- Join a caregiver support group — LUNGevity CareLine (1-800-298-2436) offers free peer support for both patients and caregivers.
- Ask your employer about Family and Medical Leave Act (FMLA) protections.
Having hard conversations:
- Encourage the patient to document their wishes in an Advance Directive (living will) and designate a healthcare proxy (healthcare power of attorney).
- These conversations are not about giving up — they are about ensuring the patient’s values guide their care regardless of what happens.
Financial Toxicity: The Practical Survival Guide Nobody Provides
“Financial toxicity” is the medical term for the economic burden of cancer treatment — and it is real, measurable, and linked to worse health outcomes. Studies show that lung cancer patients who experience severe financial distress are more likely to skip doses of medication, delay follow-up visits, and have worse survival.
What lung cancer treatment costs in 2026:
- Average annual out-of-pocket costs for lung cancer patients: $8,000–$15,000+ even with insurance.
- Targeted therapies (like osimertinib) have a list price of ~$19,000–$22,000 per month before insurance negotiation or assistance.
- Immunotherapy infusions: $10,000–$20,000+ per infusion at list price.
Insurance essentials:
- Prior authorization: Many targeted therapies and immunotherapy agents require prior authorization before insurance covers them. This can delay treatment. Your oncology team’s prior authorization team should handle this — ask if there is any delay.
- Step therapy: Some plans require trying and failing an older, cheaper drug before approving the most effective first-line agent. If this is happening, your oncologist can file a medical necessity exception.
- Appeals: If coverage is denied, appeal. A written appeal with supporting clinical documentation from your oncologist has a meaningful success rate.
- Clinical trial costs: Under the Affordable Care Act, insurance is required to cover routine patient care costs even during clinical trial participation.
Financial assistance programs:
- Patient Advocate Foundation (patientadvocate.org): Free case management and copay assistance.
- NeedyMeds (needymeds.org): Database of prescription assistance programs.
- Manufacturer patient assistance programs: Every major targeted therapy manufacturer (AstraZeneca, Genentech, Bristol Myers Squibb, Merck) offers a patient assistance program for patients who cannot afford their drugs.
- HealthWell Foundation (healthwellfoundation.org): Grants for insurance premiums, copays, and travel.
- CancerCare (cancercare.org): Limited financial grants and free professional support services.
- Social Security Disability Insurance (SSDI): Advanced-stage lung cancer qualifies for the Social Security Compassionate Allowances program — an expedited disability review process that can approve benefits within weeks rather than months.
Questions to ask your hospital’s financial counselor at your first visit:
- “What financial assistance programs does this hospital offer for cancer patients?”
- “Do you have a financial navigator or social worker who specializes in cancer care?”
- “Are there any free or reduced-cost programs for my specific medications?”
- “Can we discuss a payment plan if I have a large out-of-pocket balance?”
Clinical Trials: Your Hidden Treatment Option
Clinical trials are not a last resort. They are a legitimate, often superior treatment option — and they are systematically underutilized, particularly by patients outside major academic medical centers.
What clinical trials are:
- Research studies evaluating new treatments (new drugs, new drug combinations, new surgical or radiation techniques) in real patients.
- Divided into phases: Phase I (safety and dosing), Phase II (efficacy and side effects), Phase III (comparison to current standard of care).
- By the time a drug enters Phase III, it has already shown meaningful activity.
Why to consider a clinical trial:
- Access to next-generation therapies years before they receive FDA approval.
- Closely monitored, high-quality care.
- Often, you receive the experimental treatment plus the standard of care (not instead of it).
- No enrollment fee — the pharmaceutical sponsor covers the cost of experimental treatment.
The placebo myth, debunked: In lung cancer trials, patients in the “control arm” almost always receive the current best standard of care — not a placebo. True placebo-only controls are ethically permissible only when no effective standard treatment exists.
How to find trials:
- ClinicalTrials.gov: The official registry of all U.S. clinical trials. You can search by cancer type, stage, mutation, and location.
- GO2 Foundation’s Trial Finder: Tailored for lung cancer patients.
- Your oncologist should assess your trial eligibility at every appointment.
Questions to ask before joining a trial:
- “What phase is this trial?”
- “What is the probability I receive the experimental treatment vs. the control?”
- “What additional time commitment does the trial require?”
- “Are there travel or lodging stipends if I need to visit a distant trial site?”
Global Support Organizations
United States:
- American Lung Association: lung.org (1-800-LUNGUSA)
- LUNGevity Foundation: lungevity.org (CareLine: 1-800-298-2436)
- GO2 Foundation for Lung Cancer: go2foundation.org
- Lung Cancer Research Foundation: lungcancerresearchfoundation.org
United Kingdom:
- Roy Castle Lung Cancer Foundation: roycastle.org
- Macmillan Cancer Support: macmillan.org.uk
Australia:
- Lung Foundation Australia: lungfoundation.com.au
- Cancer Council: cancer.org.au
Canada:
- Lung Cancer Canada: lungcancercanada.ca
Your 10-Step Action Plan After a Lung Cancer Diagnosis
If you or someone you love has just been diagnosed, here are the ten most important actions to take in the days and weeks ahead:
Step 1: Request a complete copy of all imaging reports, biopsy results, and pathology reports.
Step 2: Ask whether comprehensive molecular/biomarker testing has been ordered or is pending.
Step 3: Ask for a referral to a multidisciplinary tumor board before treatment begins.
Step 4: Consider seeking a second opinion at an NCI-designated cancer center — this is standard practice in oncology.
Step 5: Request a palliative care consultation — not because you are giving up, but because it will make everything else better.
Step 6: Ask for a referral to an oncology social worker and a financial counselor on your first visit.
Step 7: Ask your oncologist about clinical trial eligibility.
Step 8: Connect with a lung cancer support community (LUNGevity, GO2 Foundation, or a local cancer center’s support program).
Step 9: If you smoke, seek help to quit now — cessation improves treatment outcomes and reduces risk of a second cancer.
Step 10: Take care of your own mental health. Ask for a referral to a psycho-oncologist or counselor. Your emotional health is part of your treatment.
Most Frequently Asked Questions about Lung Cancer
1: Can you survive lung cancer?
Yes — and survival outcomes have improved dramatically. The overall 5-year survival rate for lung cancer has nearly doubled since 2014, rising from 17% to 27% in 2026. For patients diagnosed at an early local stage, the 5-year survival rate reaches 65%. Patients with specific targetable molecular mutations — such as EGFR or ALK alterations — can achieve median survival of 3–5+ years even with Stage IV metastatic disease using precision oral targeted therapies. Long-term survivors are no longer rare: many patients live 10, 15, and even 20 years after diagnosis. The most important survival predictor is access to early detection, comprehensive molecular testing, and treatment at a high-volume, specialized cancer center.
2: What is the first sign of lung cancer most people miss?
The most commonly missed early sign is a cough that persists beyond three weeks. Most people attribute a prolonged cough to allergies, post-nasal drip, acid reflux, or a lingering cold — all of which are far more common. The cough of early lung cancer is typically dry, persistent, and unresponsive to ordinary treatments. Recurring pneumonia or bronchitis in the same area of the lung — treated with antibiotics but returning — is another early sign frequently dismissed. Because early lung cancer rarely causes pain and often grows in peripheral areas of the lung where it doesn’t immediately obstruct airways, it can be entirely symptom-free for a long period.
3: Can you get lung cancer if you have never smoked?
Absolutely — and this is far more common than most people realize. Approximately 20% of all lung cancer deaths in the United States occur in people who have never smoked, totaling an estimated 25,000 deaths annually. The most common causes of lung cancer in never-smokers include radon gas exposure (the leading environmental cause), second-hand smoke, outdoor and indoor air pollution, occupational exposures (asbestos, diesel exhaust), and inherited genetic mutations. Never-smoker lung cancer is predominantly adenocarcinoma and is significantly more likely to carry targetable molecular mutations (particularly EGFR and ALK), making it often more amenable to precision treatment than smoking-related lung cancers.
4: How fast does lung cancer spread?
It depends entirely on the type of lung cancer. Small cell lung cancer (SCLC) is one of the fastest-spreading cancers known — it can progress from diagnosis to widespread metastatic disease in a matter of weeks to months. Non-small cell lung cancer (NSCLC) grows and spreads more slowly, but the pace varies by subtype: large cell carcinoma tends to grow more rapidly; adenocarcinoma and squamous cell carcinoma are generally slower. Many lung cancers grow undetected for years before causing symptoms. Doubling time — the time for a lung cancer tumor to double in volume — ranges from as short as a few weeks (for SCLC) to months or even years (for slow-growing adenocarcinoma).
5: What is the difference between NSCLC and SCLC?
Non-small cell lung cancer (NSCLC) and small cell lung cancer (SCLC) differ fundamentally in their cell of origin, growth pattern, treatment approach, and prognosis. NSCLC accounts for approximately 85% of all lung cancers and includes three main subtypes: adenocarcinoma, squamous cell carcinoma, and large cell carcinoma. It tends to grow more slowly and has increasingly effective treatment options through targeted therapy, immunotherapy, and surgery. SCLC accounts for 13–15% of lung cancers, is almost exclusively associated with tobacco smoking, grows and spreads with extraordinary speed, and is rarely treated with surgery because it is almost always systemic at diagnosis. SCLC responds well to initial chemotherapy but almost always relapses.
6: What percentage of smokers actually get lung cancer?
Approximately 10–15% of lifetime smokers develop lung cancer. This often surprises both heavy smokers (“only 10–15%?”) and non-smokers (“only 10–15%?”). It does not mean smoking is safe — even if the majority of smokers do not develop lung cancer, smoking still causes 80–90% of all lung cancer deaths. The risk is cumulative and increases with every year of continued smoking and every additional cigarette per day. Additionally, smoking dramatically increases the risk of numerous other serious conditions: chronic obstructive pulmonary disease (COPD), cardiovascular disease, stroke, and multiple other cancers. Former smokers who have quit retain an elevated risk for decades, though their risk gradually declines with each year after quitting.
7: Is lung cancer hereditary?
Lung cancer has a hereditary component, though it is not as strongly hereditary as breast or colon cancer. Having a first-degree relative (parent, sibling, or child) with lung cancer approximately doubles your personal risk of developing lung cancer, even after controlling for smoking status. Genome-wide association studies have identified several genetic loci that increase lung cancer susceptibility — including variants in the CHRNA3/5 gene region (nicotinic acetylcholine receptor genes) and the TERT-CLPTM1L region. These genetic risk factors interact with environmental exposures like tobacco smoke and radon, making genetic background one of multiple contributors to risk rather than a single determinant. If you have a strong family history, using our Genetic Risk Assessment Tool can help you understand your personalized risk profile before speaking with a physician.
8: Does lung cancer hurt?
Early-stage lung cancer typically causes no pain. This is one of its most dangerous characteristics. As the cancer advances, pain can develop through several mechanisms: direct chest wall or rib invasion by the tumor, bone metastases causing deep aching or sharp localized pain, spinal cord or nerve compression, and pleural disease causing a constant chest pressure or ache that worsens with breathing. Pancoast tumors — located at the apex of the lung — cause a distinctive syndrome of shoulder and inner arm pain that frequently leads to months of misdiagnosis as cervical spine or rotator cuff disease. Importantly, even when lung cancer causes significant pain, modern palliative medicine has highly effective strategies for managing it — including opioid medications, nerve blocks, targeted radiation to painful bone lesions, and other interventions.
9: Can lung cancer be cured if caught early?
Yes — early-stage lung cancer has a genuinely high cure rate. Stage IA1 lung cancer (the smallest early tumors) has a 5-year survival rate of approximately 92% — meaning the vast majority of patients treated at this stage are alive and well five years later. Stage I lung cancer overall has a 5-year survival of 64–92% depending on exact substage. Surgery is typically the primary treatment for early-stage NSCLC, and for appropriate patients, it can achieve permanent remission. For patients who cannot tolerate surgery, stereotactic body radiation therapy (SBRT) achieves local control rates of 85–95% at 3 years. This is precisely why the 2025 USPSTF screening recommendations expand annual low-dose CT screening to all Americans between 50–80 with a 20 pack-year smoking history — because catching lung cancer early, when cure is achievable, is now an attainable goal.
10: What new lung cancer treatments were approved in 2025 and 2026?
2025–2026 has been an extraordinarily productive period for lung cancer drug approvals. Key approvals and developments include: Sunvozertinib received FDA accelerated approval in July 2025 for EGFR Exon 20 insertion mutations — a subtype previously without a strong first-line targeted option. The subcutaneous formulation of amivantamab (RYBREVANT FASPRO) was approved in February 2026, allowing EGFR-mutant lung cancer patients to receive this bispecific antibody as a quick injection rather than a lengthy IV infusion. Zoldonrasib, a first-in-class KRAS G12D inhibitor, demonstrated durable clinical efficacy in advanced NSCLC at the AACR 2026 meeting — potentially opening a new targeted therapy pathway for a major mutation subset. AACR 2026 also featured elisrasib, a next-generation KRAS G12C inhibitor showing robust and durable efficacy. As of August 2025, a total of 98 treatment approaches have been FDA-approved for lung cancer.
11: How do I know if I qualify for lung cancer screening?
You qualify for annual low-dose CT (LDCT) lung cancer screening under current USPSTF guidelines if you meet ALL three criteria: you are between 50 and 80 years old; you have a smoking history of 20 pack-years or more; and you currently smoke or quit within the past 15 years. A pack-year is calculated by multiplying the number of packs of cigarettes smoked per day by the number of years you smoked (e.g., 1 pack per day for 20 years = 20 pack-years; 2 packs per day for 10 years = also 20 pack-years). If you meet these criteria, speak to your primary care physician about a referral for LDCT screening — it is covered by Medicare and required to be covered by private insurance without cost-sharing. If you are unsure whether your symptoms might warrant earlier evaluation regardless of screening status, our Symptom Checker can help you assess your situation and prepare for a conversation with your doctor.
Final Summary: What You Need to Remember
Lung cancer is the most lethal cancer in America — but it is no longer the hopeless disease it was even a decade ago. Here is what this guide has shown:
- Lung cancer survival has nearly doubled since 2014, and precision medicine is driving it higher every year.
- Never-smokers account for 20% of deaths — this disease does not belong exclusively to people who smoked.
- Molecular testing before treatment is non-negotiable — it is the single most important decision point in your treatment journey.
- Early detection through screening saves lives — 65% of stage I patients survive 5 years, vs. 9% at stage IV.
- Palliative care from diagnosis improves survival — not just quality of life.
- Financial and caregiver support exists — you do not have to navigate this alone.
Use every tool in this guide. Bring this knowledge to your appointments. Ask for what you need. And know that the science behind lung cancer treatment has never been more powerful than it is in 2026.
This article was prepared with input from the mymedicineadvisor.com Global Medical Advisory Board. All statistics are sourced from peer-reviewed literature, government health databases, and major oncology organizations as cited throughout. This article is for educational and informational purposes only. It does not constitute medical advice and should not be used as a substitute for professional medical consultation, diagnosis, or treatment. If you are experiencing symptoms that concern you, please consult a qualified healthcare professional promptly.
External sources cited in this article include the National Cancer Institute, the World Health Organization, the American Lung Association, the U.S. Preventive Services Task Force, the U.S. Environmental Protection Agency, the American Academy of Family Physicians, the American Cancer Society, PubMed Central, and MD Anderson Cancer Center. All external links were verified at time of publication.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.