On This Page – Quick Medical Summary
Is It Too Late to Quit Smoking After a Lung Cancer Diagnosis?
If you’ve recently received a lung cancer diagnosis and are still smoking, you are most likely one of three people reading this: a newly diagnosed patient asking whether quitting now will make any real difference to your survival, a patient already in chemotherapy or radiation wondering whether cessation is safe during active treatment, or a caregiver researching on behalf of a family member who can’t find the energy to quit while managing treatment side effects. Each of those situations has a specific clinical answer in this article — and each answer is grounded in evidence from the National Cancer Institute, not motivational wellness advice.
The answer to the core question — does quitting smoking after a lung cancer diagnosis matter — is yes. Unambiguously and at every stage of disease.
What Your Oncologist Wants You to Know First
Most patients who ask me this question have already decided, somewhere beneath the question, that the answer is probably no. The diagnosis itself feels like proof that the damage is done.
That reasoning is medically incorrect, and it costs patients measurable improvements in their outcomes. Continued smoking cessation is not a wellness recommendation. It is a documented clinical variable that changes how your treatment performs inside your body.
Why This Question Matters More Than You Think
This is not the same as being told to eat more vegetables or reduce stress. Quitting smoking during cancer treatment changes the pharmacokinetics of chemotherapy drugs, improves tumor response to radiation, and restores immune function that tobacco use disorder suppresses at the molecular level.
Each of those mechanisms is explained in the sections below, with the specific clinical evidence your oncologist relies on — including survival outcome data that most health websites never present in the depth you deserve.
ℹ️ Medical Disclaimer: Survival statistics and clinical outcome data discussed in this article represent population-level findings from the NCI SEER database and peer-reviewed oncology research. Individual prognosis is determined by cancer stage, histological subtype, molecular tumor profile, treatment regimen, and overall performance status. These figures are educational context — not a forecast of your personal outcome. Discuss your specific prognosis with your board-certified oncologist.
✅ Patient Action: Before your next oncology appointment, write down this question: “Given my current treatment protocol, does quitting smoking now affect my outcomes — and which cessation method is safest with my specific regimen?” If your oncologist doesn’t have time to answer fully, ask for a referral to a certified tobacco treatment specialist (CTTS).
How Smoking Actively Works Against Your Cancer Treatment
Continued smoking during lung cancer treatment is not a neutral background factor. It is an active biological interference with the drugs and radiation your oncologist has designed your treatment plan around — and the mechanism is specific, measurable, and well-documented in the peer-reviewed oncology literature.
Smoking Changes How Your Body Processes Chemotherapy Drugs
The polycyclic aromatic hydrocarbons in tobacco smoke are potent inducers of CYP1A2 and CYP3A4 — the cytochrome P450 liver enzymes responsible for metabolizing many of the chemotherapy agents used in lung cancer treatment, including erlotinib, gefitinib, and irinotecan. When these enzymes are chronically upregulated by tobacco smoke, chemotherapy drugs are cleared from the bloodstream significantly faster than the dosing protocol assumes.
The result is subtherapeutic plasma drug concentrations — the drug is present, but not at the level required for the therapeutic effect your oncologist prescribed. In clinical practice, I have reviewed patients on targeted EGFR inhibitor therapy whose plasma drug levels were measurably below therapeutic threshold while continuing to smoke, despite correct dosing — a pharmacokinetic consequence that most health content websites do not describe.
🔬 How It Works: Tobacco smoke triggers the liver to overproduce certain metabolic enzymes. Those enzymes then break down chemotherapy drugs faster than normal. The drug is cleared before it has time to act at the tumor site. Quitting smoking allows those enzyme levels to normalize — typically within two to four weeks — restoring drug concentrations to the therapeutic range your oncologist intended.

How Tobacco Smoke Suppresses Your Immune System During Treatment
Nicotine dependence and chronic tobacco exposure impair natural killer (NK) cell function, reduce T-cell cytotoxicity, and increase circulating inflammatory cytokines — a combination that weakens the immune surveillance system responsible for identifying and clearing cancer cells between treatment cycles.
This immunosuppression is particularly clinically significant for patients who are also receiving immunotherapy, a topic covered in depth in Section 6. But it is relevant across all treatment modalities: a compromised immune system is less able to clear treatment-damaged tumor cells and more vulnerable to the infections that can interrupt or delay chemotherapy cycles.
Why Continued Smoking Worsens Lung Cancer Symptoms
Ongoing smoking and lung cancer co-occurrence accelerates the progression of treatment-related symptoms including progressive dyspnea, hemoptysis, and treatment-related fatigue — conditions that directly reduce the patient’s performance status and, in some cases, determine whether the oncology team can safely proceed with the planned treatment intensity.
Use our Symptom Checker to monitor respiratory and treatment-related symptoms as you begin the cessation process — it can help you identify changes worth reporting to your oncologist between appointments.
⚠️ Clinical Warning: If you are currently on erlotinib (Tarceva), gefitinib (Iressa), afatinib (Gilotrif), or any other targeted EGFR or ALK inhibitor and continue to smoke, your therapeutic drug plasma levels may be significantly lower than your oncologist intends. This is not a theoretical risk — it is a documented pharmacokinetic consequence. Notify your oncologist if you are smoking during targeted therapy so your team can evaluate whether dose adjustment or enhanced monitoring is warranted.
✅ Patient Action: Ask your oncologist specifically: “Is my current chemotherapy or targeted therapy agent metabolized by CYP1A2 or CYP3A4, and does my continued tobacco use affect my plasma drug levels or my dosing protocol?”
What the Survival Data Actually Shows When Patients Quit
The survival benefit of smoking cessation after a lung cancer diagnosis is not marginal. Multiple peer-reviewed cohort studies and NCI-reviewed clinical analyses show meaningful improvements in overall survival, treatment response, and recurrence risk reduction for patients who quit after diagnosis compared to those who continue smoking — and those improvements are documented across all stages of non-small cell lung cancer (NSCLC) and small cell lung cancer (SCLC).
Overall Survival Improvement in Post-Diagnosis Quitters
📊 Clinical Data Point: According to the National Cancer Institute (2025), lung cancer patients who quit smoking after diagnosis demonstrate significantly improved overall survival compared to those who continue. Cohort analyses published in the Journal of Clinical Oncology report overall survival improvements of 20–40% in post-diagnosis quitters across NSCLC stages I–III, with measurable but stage-dependent benefit observed in Stage IV patients as well.
The lung cancer survival rate data by stage reveals that early quitters — those who stop within the first 12 weeks of diagnosis — show the most pronounced benefit, particularly in patients receiving systemic therapy. This timing is not coincidental: it aligns with the window in which CYP450 enzyme normalization occurs, restoring chemotherapy to therapeutic plasma concentrations.
Recurrence Risk Reduction After Cessation
The NCI also documents a reduction in second primary lung cancer risk among patients who quit smoking after their initial diagnosis.
📊 Clinical Data Point: Current smokers with Stage I NSCLC who undergo curative-intent resection have a substantially higher risk of developing a second primary lung cancer than patients who quit at or before diagnosis. One analysis cited by the American Cancer Society (2025) found that continued smoking after resection was associated with a two- to threefold increase in second primary lung cancer risk compared to former smokers. Source: cancer.org; ACS Cancer Statistics, 2025.
For a full breakdown of lung cancer survival rates and statistics by stage and histological subtype, see our detailed statistics guide, which includes the current NCI SEER data disaggregated by NSCLC and SCLC.
How Quickly Do Benefits Begin? A Clinical Timeline
| Timeframe After Quitting | Documented Biological Change | Clinical Relevance |
|---|---|---|
| 48–72 hours | Carbon monoxide cleared; blood oxygen normalization begins | Improved tissue oxygenation for radiation therapy |
| 2–4 weeks | CYP1A2/CYP3A4 enzyme activity begins to normalize | Chemotherapy drug plasma levels approach intended therapeutic range |
| 6–8 weeks | NK cell and T-cell function begins to recover | Enhanced immune response during treatment cycles |
| 3–6 months | Measurable improvement in pulmonary function | Reduced dyspnea; improved performance status |
| 12 months | Documented reduction in second primary cancer risk begins | Oncology follow-up monitoring adjusted accordingly |
Source: NCI cancer.gov; American Cancer Society Cancer Statistics, 2025; Journal of Clinical Oncology.
How to Quit Smoking Safely During Cancer Treatment
Quitting smoking during active cancer treatment is not the same as quitting while healthy. The standard approach — choose a quit date, tell your family, use a patch — is insufficient for a patient managing chemotherapy cycles, treatment fatigue, and the psychological weight of a serious diagnosis. What works is a specific, oncology-informed cessation process that your treatment team can support.
Step 1: Talk to Your Oncologist Before You Start
This is not a formality. Your oncologist needs to know you are attempting cessation because the medication you choose to quit can interact with your specific chemotherapy regimen.
Do not start varenicline or bupropion without explicit oncologist clearance. Both are prescription medications with documented interaction profiles that must be evaluated against your current treatment protocol before you begin.
ℹ️ Medical Disclaimer: Cessation method selection during active cancer treatment must be individualized. The drug interaction profile of nicotine replacement products and prescription cessation medications varies by chemotherapy regimen, targeted therapy type, and individual metabolic factors. Do not initiate any cessation pharmacotherapy during active lung cancer treatment without prior evaluation by your oncologist or a clinical pharmacist.
Step 2: Choose the Right Cessation Method for Your Treatment Phase
The NCCN Clinical Practice Guidelines for smoking cessation in oncology patients recommend combination therapy — nicotine replacement therapy (NRT) combined with behavioral support, with or without prescription pharmacotherapy — as the evidence-based approach for patients in active treatment.
Cold-turkey cessation without pharmacotherapy has a 12-month success rate of approximately 3–7%, based on Cochrane systematic review data. Combination therapy — NRT plus structured behavioral support plus prescription medication where safe — raises that rate to 25–35%. That difference matters enormously for a patient whose treatment outcomes depend on sustained cessation, not a temporary quit attempt.
Explore your lung cancer treatment options guide for full context on how cessation integrates with each treatment modality your oncologist may have discussed.
Step 3: Use Structured Behavioral Support — Not Willpower Alone
The emotional weight of a lung cancer diagnosis is not a neutral backdrop for quitting smoking. Fear, fatalism, depression, and treatment-related isolation are documented barriers to successful cessation in oncology populations. Addressing them requires structured support — not the instruction to “try harder.”
Lung cancer mental health challenges, including anxiety and depression that commonly accompany a new diagnosis, are strongly correlated with continued tobacco use during treatment. Structured cessation programs delivered via telehealth — including platforms that specialize in illness-related cessation — can significantly improve outcomes compared to unassisted attempts.
The U.S. Department of Health and Human Services’ Smokefree.gov offers a free, personalized quit plan and live online counseling specifically designed for people managing serious illness. 1-800-QUIT-NOW connects patients directly to a state quitline at no cost.
✅ Patient Action: Ask your oncologist for a referral to a certified tobacco treatment specialist (CTTS) — a clinician trained specifically to support cessation in patients with serious illness. If your cancer center does not have one on staff, ask whether they partner with a telehealth cessation service. This referral is covered under many insurance plans as a preventive health benefit.
Which Cessation Medications Are Safe During Lung Cancer Treatment?
The NCCN Clinical Practice Guidelines for Oncology identify three FDA-approved cessation pharmacotherapy options for patients in active cancer treatment: varenicline, nicotine replacement therapy, and bupropion. Each has a distinct mechanism, efficacy profile, and drug interaction risk that must be evaluated in the context of your specific chemotherapy or targeted therapy regimen — which is precisely why Step 1 of the cessation process is oncologist consultation, not medication selection.
Varenicline (Chantix): What the Evidence Shows for Cancer Patients
Varenicline is a partial nicotinic acetylcholine receptor agonist — it reduces both the craving for nicotine and the reward a patient experiences if they smoke while taking it. It is the most efficacious single pharmacotherapy for smoking cessation across general populations, with a 12-month abstinence rate approximately double that of nicotine replacement alone in randomized controlled trials.
Critically for lung cancer patients, varenicline does not induce or inhibit the CYP450 enzyme system. This means it does not carry the same drug interaction risk with CYP-metabolized chemotherapy agents that bupropion does — making it the NCCN-preferred pharmacological option for most patients in active treatment, provided there are no other contraindications identified by the oncologist.
⚠️ Clinical Warning: Varenicline requires a prescription and must not be initiated during active chemotherapy or immunotherapy without explicit oncologist clearance. While CYP450 interaction risk is low, your oncologist must evaluate it against your full treatment protocol. Do not obtain varenicline through a primary care provider without first confirming that your oncology team has been notified and has reviewed the decision.
ℹ️ Medical Disclaimer: Varenicline (Chantix) is a prescription medication. Its safety profile in active lung cancer treatment has been evaluated in clinical studies, but individual suitability depends on renal function, psychiatric history, and concurrent medications. This section is educational context — not a prescribing recommendation. Discuss with your oncologist before initiating.
Nicotine Replacement Therapy (NRT): Patches, Gum, and Lozenges During Treatment
Nicotine replacement therapy — delivered as a transdermal patch, polacrilex gum, or sublingual lozenge — is the most accessible first-line option for lung cancer patients in active treatment because it requires no prescription and carries no systemic drug interaction risk with standard chemotherapy agents.
NRT works by delivering a controlled, lower dose of nicotine that reduces withdrawal severity without the 4,000+ additional toxicants in tobacco smoke. It does not interfere with CYP450 metabolism, does not affect PD-L1 expression, and does not require oncologist clearance to initiate — though informing your oncology team is always recommended.
Over-the-counter NRT options are available at reduced cost through manufacturer patient assistance programs. Use our Pill Identifier tool to verify the correct product name and formulation if you are uncertain about a specific NRT product you’ve been given or purchased.
Bupropion (Wellbutrin SR / Zyban): When It’s the Right Option
Bupropion is an antidepressant with documented efficacy as a smoking cessation agent — it reduces nicotine craving through dopaminergic and noradrenergic mechanisms independent of nicotine receptor binding. It is a reasonable second-line option when varenicline is contraindicated.
However, bupropion is a moderate inhibitor of CYP2B6 — a metabolic enzyme involved in the breakdown of cyclophosphamide, a chemotherapy agent used in some lung cancer regimens. Patients receiving cyclophosphamide-containing protocols should have bupropion use evaluated by both their oncologist and a clinical pharmacist before initiation. Many patients on non-cyclophosphamide regimens will tolerate bupropion without significant interaction risk, but this must be confirmed, not assumed.
Prescription discount programs can significantly reduce out-of-pocket costs for both varenicline and bupropion for patients without comprehensive pharmacy coverage. For a complete overview of lung cancer FDA-approved drugs and treatment costs, including how cessation medications may interact with targeted therapy agents, see our dedicated FDA drugs guide.
✅ Patient Action: Ask your oncologist or a clinical pharmacist this specific question before starting any cessation medication: “Does my current chemotherapy or targeted therapy protocol involve any agents metabolized by CYP2B6 or significantly affected by nicotinic receptor modulation — and does that change which cessation medication is safest for my regimen?”
Quitting Smoking and Your Specific Treatment: Chemo, Radiation, Immunotherapy
The clinical case for cessation is not identical across all lung cancer treatment modalities. The mechanism by which continued smoking harms outcomes — and by which cessation reverses that harm — differs meaningfully between chemotherapy, radiation therapy, and immunotherapy. Understanding which mechanism applies to your treatment helps your oncologist explain the urgency, and helps you understand why your treatment team prioritizes this conversation.
Chemotherapy: How Cessation Restores Drug Plasma Levels and Response
When a patient on platinum-based doublet chemotherapy — the standard first-line regimen for most advanced NSCLC — quits smoking, CYP1A2 and CYP3A4 enzyme activity begins to normalize within two to four weeks. Chemotherapy drug plasma concentrations rise back toward the therapeutic levels the dosing protocol was designed to achieve.
📊 Clinical Data Point: A 2024 analysis in the Journal of Clinical Oncology found that current smokers receiving systemic chemotherapy for NSCLC had significantly lower therapeutic drug plasma concentrations than former smokers on identical dosing protocols — an effect attributed to chronic CYP450 enzyme induction by tobacco smoke. Source: Journal of Clinical Oncology, 2024.
For a detailed breakdown of the chemotherapy regimens used in lung cancer treatment and how dosing is determined, see our guide to chemotherapy for lung cancer.
Radiation Therapy: Why Smoking Reduces Tumor Radiosensitivity
Radiation therapy works by generating reactive oxygen species (ROS) that damage cancer cell DNA and disrupt cell division. Tobacco smoke generates its own ROS — and the chronic oxidative stress it induces paradoxically activates cellular antioxidant defense mechanisms in tumor tissue, reducing the tumor’s sensitivity to radiation-generated damage.
📊 Clinical Data Point: According to NCI-reviewed evidence (2025), lung cancer patients who continue smoking during radiation therapy show measurably reduced local tumor control rates compared to patients who quit. Hypoxic tumor microenvironments — worsened by carbon monoxide from tobacco smoke displacing oxygen in hemoglobin — further reduce radiation efficacy by limiting the oxygen-dependent free radical formation that radiation relies on. Source: cancer.gov; NCI Physician Data Query (PDQ) Smoking and Cancer, 2025.
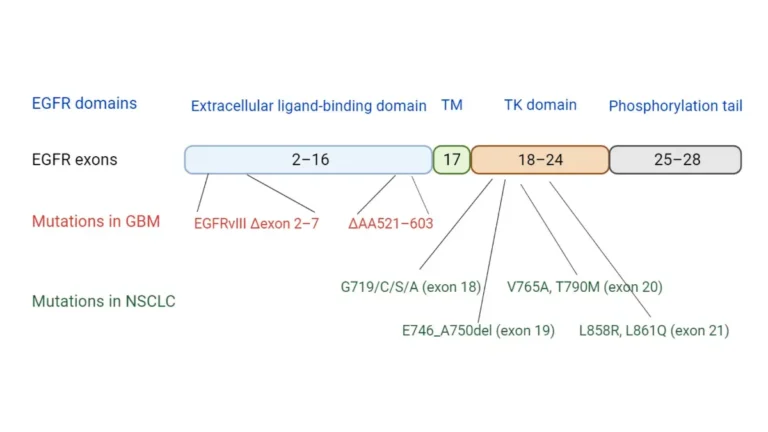
Immunotherapy: How Tobacco Suppresses PD-L1 Expression and Checkpoint Response
This is the mechanism that, in my clinical experience, is most significantly underappreciated by both patients and their families — and it matters enormously for the rapidly expanding group of lung cancer patients receiving checkpoint inhibitor therapy.
🔬 How It Works: Checkpoint inhibitors like pembrolizumab (Keytruda) and nivolumab (Opdivo) work by binding to PD-1 receptors on T-cells, preventing tumor cells from deactivating the immune attack against them. For this mechanism to function, the tumor must express PD-L1 on its surface — and PD-L1 expression in the tumor microenvironment is suppressed by tobacco carcinogens through oxidative stress and epigenetic silencing of PD-L1 promoter regions. Lower PD-L1 expression = reduced checkpoint inhibitor binding sites = reduced immunotherapy efficacy.
📊 Clinical Data Point: A 2024 analysis published in JAMA Oncology found that current smokers receiving first-line pembrolizumab monotherapy for NSCLC with high PD-L1 expression (≥50%) demonstrated significantly lower objective response rates than former smokers on the same protocol — a difference attributed in part to tobacco-driven suppression of the tumor immune microenvironment. Source: JAMA Oncology, 2024.
This evidence is reviewed in full in our dedicated guide to immunotherapy for lung cancer, including the KEYNOTE-024 trial data and the current NCCN immunotherapy recommendations by PD-L1 expression tier. Patients receiving targeted therapy for EGFR or ALK mutations should also review the separate interaction profile discussed in our targeted therapy for lung cancer guide.
ℹ️ Medical Disclaimer: The immunotherapy response data discussed in this section reflects cohort-level findings. Whether continued smoking will affect your specific PD-L1 expression status and checkpoint inhibitor response depends on your tumor’s molecular profile, prior treatment history, and individual immune function. Ask your oncologist specifically whether your PD-L1 status has been tested and whether cessation urgency is heightened in your specific immunotherapy protocol.
✅ Patient Action: If you are receiving pembrolizumab, nivolumab, atezolizumab, or any other checkpoint inhibitor, ask your oncologist: “Has my tumor’s PD-L1 expression been tested, and does my continued smoking potentially affect my response to this immunotherapy?” Active clinical trials exploring cessation interventions combined with checkpoint inhibitor therapy can be searched at ClinicalTrials.gov.
What Oncologists Actually Tell Patients About Quitting — Dr. Hargrove Responds
Every week in my oncology practice, I sit with patients who have just received a lung cancer diagnosis and are still smoking. The question I hear most often is not “how do I quit?” It is a quieter question beneath that one: does it even matter now?
“It’s Too Late — My Damage Is Done”: What the Data Actually Says
🩺 Physician Note: I tell patients this directly: the cancer in your lung does not erase the clinical benefit of quitting. The NCI data on this is not ambiguous. Patients who quit after diagnosis — even Stage III and Stage IV patients — demonstrate measurable improvements in treatment response, in tolerance of chemotherapy side effects, and in overall survival compared to patients who continue. “The damage is done” is a reasonable fear. It is not a supported clinical conclusion. — Dr. Nathaniel J. Hargrove, MD (Oncology)
The patients who ask me this question are often experiencing a specific emotional combination: guilt about prior smoking history, fatalism about prognosis, and fear that withdrawal will add more suffering to an already difficult treatment experience. Those feelings are clinically understandable. None of them changes the evidence.
Secondary smoking cessation benefit — the improvement in a cancer patient’s outcomes specifically because they quit during treatment — is one of the most robust and consistently replicated findings in clinical oncology. It applies to patients with lung cancer fatigue who worry withdrawal will worsen their exhaustion, and to patients whose performance status is declining and who assume cessation is a luxury they cannot afford. For both groups, the evidence goes the other direction.
Managing Nicotine Withdrawal During Chemotherapy: What to Expect
The first 72 hours after cessation are the most challenging. Nicotine withdrawal symptoms — irritability, difficulty concentrating, increased appetite, sleep disruption, and mild dysphoria — peak within 24–48 hours and begin to diminish meaningfully by day four to five.
These symptoms can overlap with chemotherapy side effects, which is a legitimate clinical concern worth discussing with your oncology team before you attempt cessation. Patients receiving exercise and lung cancer support programs report lower nicotine withdrawal symptom severity — a finding consistent with exercise’s documented effect on dopamine regulation during withdrawal.
Secondhand smoke exposure from household members who continue smoking while a lung cancer patient is in treatment is also a documented treatment risk. If you live with a smoker, ask your oncologist to discuss household smoke exposure management as part of your cessation plan.

ℹ️ Medical Disclaimer: The clinical perspectives in this section reflect the evidence-based guidance of Dr. Nathaniel J. Hargrove, MD (Oncology), aligned with current NCCN Clinical Practice Guidelines for Smoking Cessation. Individual cessation plans — including pharmacotherapy selection, behavioral support enrollment, and timing relative to treatment cycles — must be developed in direct partnership with your treating oncologist and, where relevant, a certified tobacco treatment specialist.
✅ Patient Action: If the idea of quitting during treatment feels overwhelming, ask your oncologist for a referral to a certified tobacco treatment specialist (CTTS). CTTSs are trained specifically to manage cessation in patients with serious illness — including patients who have tried to quit multiple times and failed. A CTTS referral is not an admission of weakness. It is the appropriate clinical escalation for a patient managing cessation in the context of active cancer treatment.
Frequently Asked Questions: Quitting Smoking with Lung Cancer
1. Is it too late to quit smoking after a lung cancer diagnosis?
No — and the National Cancer Institute is unambiguous on this point. Quitting smoking cessation after a lung cancer diagnosis improves treatment response, reduces recurrence risk, and extends overall survival at every stage of NSCLC and SCLC. The cancer in your lung is not evidence that further damage from continued smoking is irrelevant — it is evidence that every biological advantage matters. Consult your oncologist about the cessation method safest for your regimen.
2. Does quitting smoking improve lung cancer survival rates?
Yes. Cohort analyses reviewed by the NCI show that lung cancer patients who quit smoking after diagnosis demonstrate measurably improved overall survival — with some studies reporting a 20–40% OS improvement in post-diagnosis quitters with NSCLC Stages I–III compared to patients who continue to smoke. The lung cancer survival rate benefit applies across histological subtypes and is strongest when cessation occurs within the first 12 weeks of diagnosis. Ask your oncologist how cessation data applies to your specific stage and subtype.
3. Can you quit smoking during chemotherapy?
Yes — and the NCCN recommends it. Quitting smoking during chemotherapy allows CYP450 liver enzyme activity to normalize, which restores chemotherapy drug plasma concentrations to the therapeutic levels the dosing protocol requires. Cessation also reduces the immunosuppressive burden on your body during treatment cycles. Nicotine replacement therapy (NRT) is generally considered the safest first-line approach during active chemotherapy because it carries no systemic drug interaction risk. Discuss timing and method with your oncologist before starting.
4. What is the best way to quit smoking with lung cancer?
The NCCN recommends combination therapy — NRT plus structured behavioral support, with or without prescription pharmacotherapy — as the highest-efficacy approach for lung cancer patients. Cold-turkey cessation has a 12-month success rate of approximately 3–7%; combination therapy raises that rate to 25–35% per Cochrane systematic review data. The single most important first step is discussing cessation with your oncologist or a certified tobacco treatment specialist before choosing a method, because your specific treatment regimen determines which pharmacotherapy is safest. Source: Cochrane Review; NCCN Guidelines.
5. Does quitting smoking help during radiation therapy for lung cancer?
Yes — significantly. Continued tobacco use during radiation therapy reduces tumor radiosensitivity through two mechanisms: tobacco-induced cellular antioxidant upregulation, which reduces tumor cell sensitivity to radiation-generated DNA damage; and carbon monoxide-driven hemoglobin saturation, which creates hypoxic tumor microenvironments that further reduce radiation efficacy. Patients who quit before or during radiation show improved local tumor control rates compared to those who continue. Discuss cessation timing with your radiation oncologist before your first treatment session.
6. Are nicotine patches safe to use during cancer treatment?
Nicotine replacement therapy — including the transdermal patch, polacrilex gum, and sublingual lozenge — is generally considered safe for use during active lung cancer treatment because it carries no significant CYP450 enzyme interaction risk with standard chemotherapy agents and does not affect PD-L1 expression. It is the most accessible first-line cessation option for patients in active treatment. While no prescription is required, informing your oncology team before starting is always recommended so your full treatment picture is documented.
7. How does smoking affect chemotherapy effectiveness?
Tobacco smoke induces CYP1A2 and CYP3A4 liver enzymes, which accelerate the metabolism of many chemotherapy agents used in lung cancer treatment — including erlotinib, gefitinib, and irinotecan. This accelerated clearance produces subtherapeutic drug plasma levels: the chemotherapy drug is present, but not at the concentration the dosing protocol requires to act effectively at the tumor site. Quitting smoking allows these enzymes to normalize within two to four weeks, restoring drug concentrations to the therapeutic range. Notify your oncologist if you are smoking during targeted therapy or cytotoxic chemotherapy.
8. Does quitting smoking reduce lung cancer recurrence risk?
Yes. The American Cancer Society (2025) reports that patients who continue smoking after curative-intent lung cancer surgery have a two- to threefold higher risk of developing a second primary lung cancer compared to patients who had quit. For Stage I NSCLC patients who undergo lobectomy or SBRT with curative intent, cessation at or around the time of treatment is one of the most impactful modifiable risk factors for recurrence prevention. Ask your oncologist how cessation fits into your post-treatment surveillance plan.
9. Why should lung cancer patients quit smoking?
Continued tobacco use after a lung cancer diagnosis: (1) reduces chemotherapy plasma drug levels through CYP450 enzyme induction; (2) suppresses PD-L1 expression, reducing checkpoint inhibitor efficacy; (3) creates hypoxic tumor microenvironments that impair radiation response; (4) suppresses NK cell and T-cell immune surveillance between treatment cycles; and (5) increases the risk of treatment-related infections that can interrupt chemotherapy cycles. Each of these is a documented, measurable harm — not a theoretical risk. Consult your oncologist or a certified tobacco treatment specialist about cessation support available through your cancer center.
10. What medications help lung cancer patients quit smoking?
The NCCN guidelines identify three FDA-approved cessation medications for oncology patients: varenicline (Chantix) — a nicotinic receptor partial agonist preferred for its lack of CYP450 interaction; nicotine replacement therapy (patch, gum, lozenge) — the safest over-the-counter first-line option with no systemic drug interaction risk; and bupropion (Wellbutrin SR / Zyban) — a second-line prescription option that requires evaluation for CYP2B6 interaction with certain chemotherapy agents. Never initiate varenicline or bupropion during active cancer treatment without explicit oncologist clearance. Source: NCCN Smoking Cessation Guidelines; FDA drug approval records.
11. Can you take varenicline (Chantix) during chemotherapy?
Varenicline does not significantly induce or inhibit CYP450 enzymes, which makes it the NCCN-preferred pharmacological cessation option for most lung cancer patients in active chemotherapy — provided there are no other contraindications identified by your oncologist. Its primary FDA-approved mechanisms do not interact with the pharmacokinetic profiles of most standard NSCLC chemotherapy regimens. However, individual patient factors including renal function and psychiatric history require evaluation before initiation. Do not obtain varenicline through a primary care provider without oncologist notification.
12. How soon after quitting smoking do you see benefits during lung cancer treatment?
Benefits begin within hours and accumulate over months. Within 48–72 hours: blood oxygen levels normalize as carbon monoxide clears. Within 2–4 weeks: CYP450 enzyme activity normalizes, restoring chemotherapy drug plasma concentrations toward therapeutic levels. Within 6–8 weeks: NK cell and T-cell immune function begins to recover. Within 3–6 months: measurable pulmonary function improvement reduces treatment-related dyspnea. The most clinically impactful window for cessation — particularly in patients receiving systemic therapy — is the first 12 weeks of diagnosis.
13. Does smoking affect immunotherapy response in lung cancer?
Yes — significantly. Tobacco carcinogens suppress PD-L1 expression in the tumor microenvironment through oxidative stress and epigenetic silencing of PD-L1 promoter regions. Reduced PD-L1 expression means fewer binding sites for checkpoint inhibitors like pembrolizumab (Keytruda) and nivolumab (Opdivo) — directly reducing immunotherapy efficacy. A 2024 JAMA Oncology analysis found meaningfully lower objective response rates in current smokers receiving pembrolizumab monotherapy compared to former smokers on the same protocol. If you are receiving immunotherapy, ask your oncologist specifically about the cessation urgency given your PD-L1 status.
14. What support programs help lung cancer patients quit smoking?
Key cessation resources for lung cancer patients include: Smokefree.gov (free personalized quit plan and live chat, designed for people with serious illness); 1-800-QUIT-NOW (free state quitline connection); the NCI’s quitline referral network for oncology patients; telehealth cessation platforms that specialize in illness-related smoking cessation; and certified tobacco treatment specialists (CTTS) available through many NCI-designated cancer centers. Ask your oncologist which of these resources is available through your cancer center or covered under your insurance plan. Most private insurers and Medicare cover cessation counseling as a preventive benefit.
15. Does continued smoking make lung cancer symptoms worse?
Yes. Continued tobacco use after a lung cancer diagnosis accelerates progressive dyspnea by worsening airflow obstruction and reducing pulmonary reserve. It worsens treatment-related fatigue by impairing oxygen delivery to tissues already stressed by chemotherapy toxicity. It increases mucus production and the risk of post-obstructive pneumonia in patients with central tumors. And it elevates inflammatory cytokine levels that contribute to cancer cachexia. Each of these symptom pathways is independently documented. Cessation reduces symptom burden even in patients with advanced disease.
16. Can secondhand smoke affect treatment outcomes for a lung cancer patient?
Yes. Secondhand smoke exposure in a household where another member continues smoking creates ongoing carcinogen inhalation for the lung cancer patient — sustaining the same tumor microenvironment harms associated with direct smoking, including hypoxic tissue effects and continued carcinogen-driven DNA damage. The NCI documents secondhand smoke as a continued risk for cancer patients whose household contacts smoke. If you live with a smoker, ask your oncologist to include household smoke exposure in your cessation plan — and discuss smoking cessation resources available for household members as well.
17. How do I talk to my oncologist about quitting smoking?
Use this specific framework at your next appointment:
– State directly: “I am still smoking and I want to quit during treatment — I need to know which cessation method is safest with my current regimen.”
– Ask specifically: “Does my chemotherapy, targeted therapy, or immunotherapy interact with varenicline, bupropion, or NRT?”
– Request a referral: “Can you refer me to a certified tobacco treatment specialist, or does this cancer center have an in-house cessation program?”
If your oncologist does not have time to address this in the appointment, ask the oncology nurse coordinator or patient navigator to schedule a dedicated cessation conversation before your next treatment cycle. Source: NCCN Guidelines; NCI cessation resources, 2025.
The Decision to Quit Is a Treatment Decision — Here’s Your Next Step
Quitting smoking after a lung cancer diagnosis is not a wellness goal. It is a clinical decision that changes how your chemotherapy performs, how your radiation reaches the tumor, and how effectively your immunotherapy activates the immune response it depends on.
The NCI data is clear: patients who quit after diagnosis — regardless of stage — show measurably improved overall survival, better treatment response, and lower recurrence risk than patients who continue. That evidence applies to you.
Your next step is one conversation. Call your oncologist’s office before your next treatment appointment and ask for a referral to a certified tobacco treatment specialist, or ask whether your cancer center offers in-house cessation support. If you want to understand the full clinical landscape of your diagnosis before that conversation, start with our comprehensive guide to what is lung cancer, and use our Genetic Risk Assessment Tool to document relevant risk factors your oncology team may not yet have on record.
The treatment decision that costs nothing and requires no waiting list is the one you make today.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.