On This Page – Quick Medical Summary
Amelanotic melanoma is a rare but deadly form of skin cancer that carries no visible dark pigment. It appears as a pink, red, or skin-colored spot — indistinguishable from a pimple, scar, or benign cyst. According to the Skin Cancer Foundation, even today’s most advanced AI skin cancer apps routinely miss it because these tools are designed around the classic ABCDE rule — a framework that fundamentally fails for this cancer type.
That failure has consequences. By the time most patients receive a correct diagnosis, the cancer has already advanced. Reading this article could save your life.
⚠️ Medical Disclaimer: This article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a licensed dermatologist or oncologist for any skin concern.
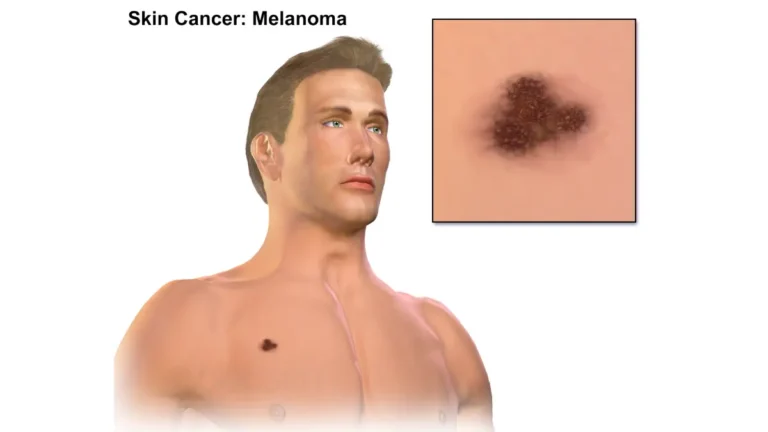
What Is Amelanotic Melanoma? The Cancer That Fools Everyone
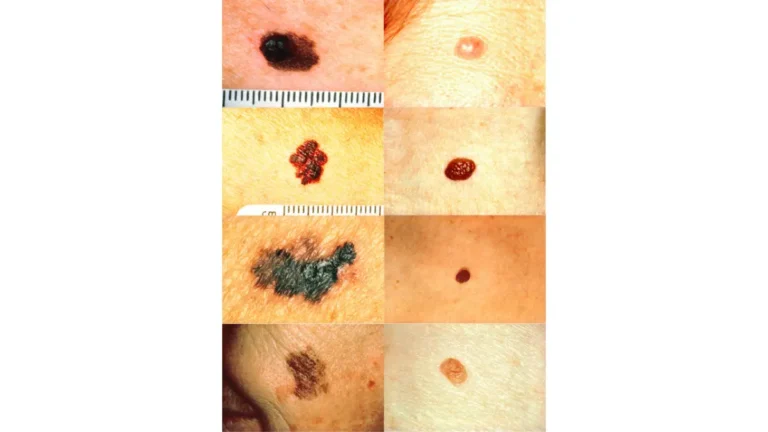
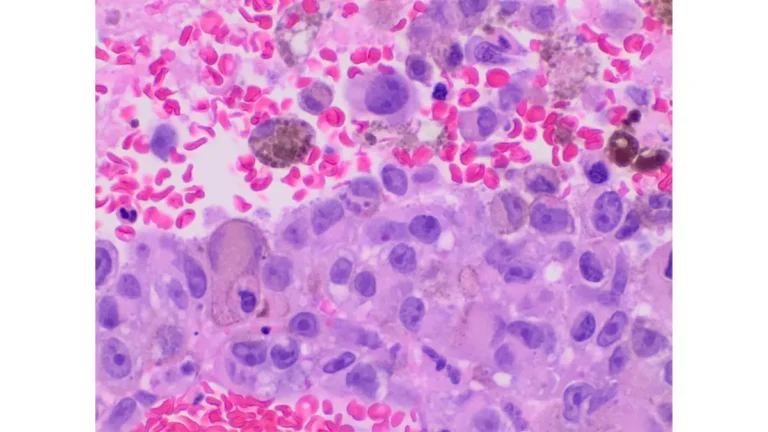
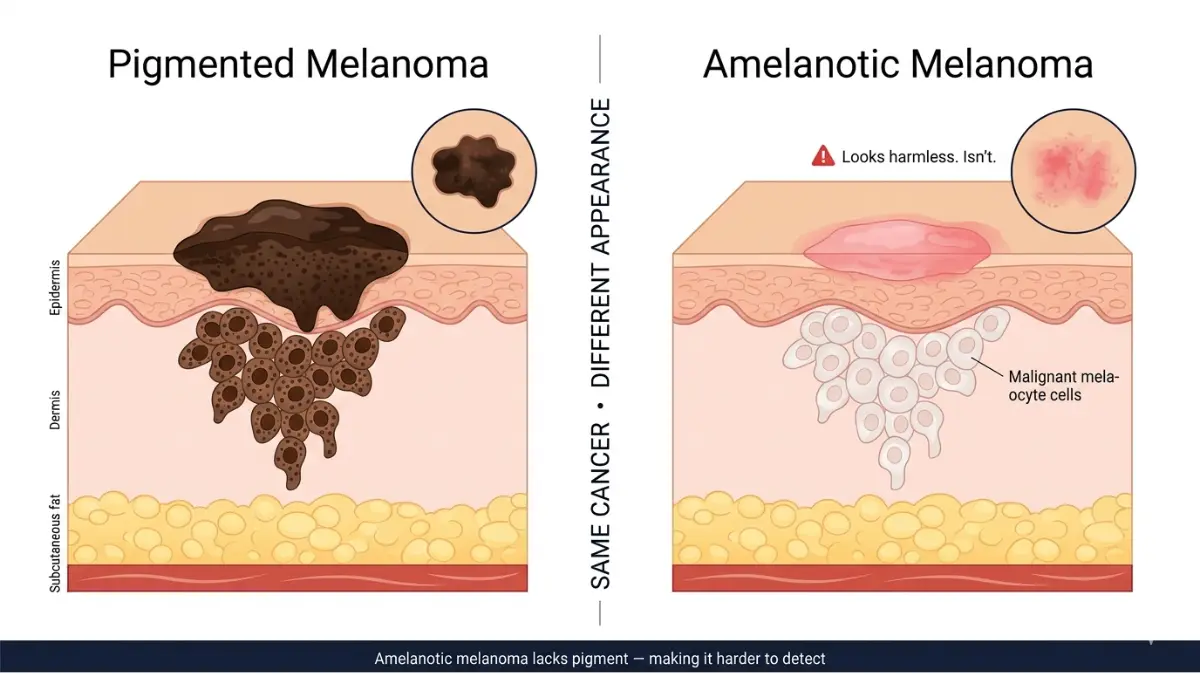
Amelanotic melanoma is a subtype of melanoma in which malignant melanocyte cells produce little to no melanin — the pigment that gives most moles and cancers their characteristic dark appearance. The result is a lesion that looks nothing like a typical melanoma.
According to DermNet NZ, amelanotic melanoma accounts for approximately 2–20% of all melanomas, with truly colorless lesions being the rarest form. It can appear as:
- Pink or reddish — the most common presentation
- Skin-colored or translucent — nearly invisible against fair complexions
- Whitish or purple-tinted — especially in nodular variants
This is not a cosmetic concern. Amelanotic melanoma carries a significantly higher mortality risk than pigmented forms because it is consistently caught late — at stages where treatment is far more aggressive and outcomes far less certain.
What virtually no article covers: approximately 70% of all childhood melanomas are amelanotic, per the National Cancer Institute’s childhood melanoma treatment guidelines. This means a pink or red lesion on a child that “doesn’t look like cancer” may actually be the most common form of pediatric melanoma.
Amelanotic Melanoma vs. Pigmented Melanoma — At a Glance
| Feature | Amelanotic Melanoma | Pigmented Melanoma |
|---|---|---|
| Color | Pink, red, skin-colored | Brown, black, blue |
| ABCDE Rule Reliability | Largely fails | Generally applies |
| Clinical Misdiagnosis Rate | Up to 87.5% | ~12% |
| Breslow Depth at Diagnosis | Typically greater | Typically thinner |
| 5-Year Overall Survival | ~77% | ~84% |
| Childhood Cases | ~70% of pediatric melanoma | ~30% |
Primary risk factors include fair skin (Fitzpatrick Type 1–2), red hair, heavy freckling, chronic UV exposure, previous sunburns, and family history of melanoma. Use our Genetic Risk Assessment Tool to understand your personal baseline skin cancer risk.
Why Amelanotic Melanoma Is Misdiagnosed 87% of the Time
This is the statistic that should concern every patient — and every physician.
A peer-reviewed clinical case series from BMC Research Notes (NIH/PubMed) found a clinical misdiagnosis rate of 87.5% for amelanotic melanoma. Squamous cell carcinoma (SCC) and basal cell carcinoma (BCC) were the most frequent incorrect diagnoses. In 56% of cases, the lesion had been present for over 12 months before a correct diagnosis was made.
Consider James, a 61-year-old accountant from Arizona. A persistent pink growth on his temple was dismissed as “probable BCC” for 14 months. When finally biopsied, it was Stage III amelanotic melanoma with a Breslow thickness of 3.8 mm — a depth that required systemic immunotherapy rather than a simple excision.
Why the ABCDE Rule Breaks Down Here
The classic ABCDE rule — Asymmetry, Border irregularity, Color variation, Diameter, Evolution — is designed around pigmented lesions. Amelanotic melanoma defeats the “C” criterion entirely. There is no color variation because there is no visible color at all.
The CDC’s skin cancer symptom guidance forms the backbone of public skin cancer education in the United States — yet it is built on ABCDE criteria that create a dangerous diagnostic blind spot for unpigmented melanoma.

What doctors most often confuse amelanotic melanoma with:
- Basal cell carcinoma (BCC) — accounts for the majority of misdiagnoses
- Squamous cell carcinoma (SCC)
- Benign cysts, lipomas, or fibromas
- Eczema, contact dermatitis, or psoriasis
- Keloids or scar tissue
- Infected follicle or pimple
Why AI apps miss it: As the Skin Cancer Foundation explicitly states, even today’s specialized computer apps for early melanoma recognition are modeled on classic ABCDE patterns and can miss more clinically subtle melanomas like amelanotic variants.
For a comprehensive overview of all skin cancer warning signs and 12 critical symptoms that go beyond standard ABCDE criteria, see our dedicated guide.
The 5 Warning Signs When ABCDE Fails
Because the ABCDE framework largely fails for amelanotic melanoma, dermatologists and informed patients rely on a different set of clinical markers. Memorize these five signs — they exist specifically to catch what ABCDE misses.
⚑ Sign 1 — The “Ugly Duckling” Signal
Any skin lesion that looks fundamentally different from every other mole or spot on your body demands attention — regardless of color. This outlier quality, not dark pigmentation, is your first red flag. Our guide on where melanoma most commonly appears on the body covers the highest-risk anatomical locations in detail.
⚑ Sign 2 — Rapid, Unexplained Growth
Amelanotic melanoma can expand noticeably within weeks to a few months. Any new or enlarging pink, red, or colorless lesion that grows faster than surrounding skin lesions is a critical warning sign — especially in adults over 50 with chronic sun damage.
⚑ Sign 3 — Irregular Vascular Patterns Under Dermoscopy
This sign is invisible to the naked eye. When examined with a dermatoscope, amelanotic melanoma reveals characteristic irregular blood vessel architecture. According to DermNet NZ, these include milky-red areas, dotted irregular vessels, and linear irregular vessel patterns — the most diagnostically reliable non-pigment clue available.
⚑ Sign 4 — A Non-Healing Lesion That Appears Benign
A pink, red, or skin-colored spot that does not heal within 4–6 weeks — especially one that occasionally bleeds, crusts, or ulcerates — should never be dismissed as a minor irritation. Persistent non-healing is one of the strongest clinical signals for malignancy in unpigmented lesions.
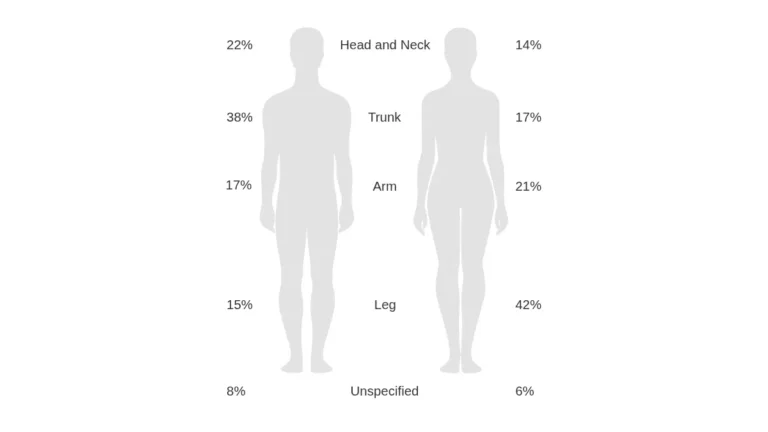
⚑ Sign 5 — High-Risk Anatomical Location
Acral amelanotic melanoma — affecting the palms, soles, fingers, and nail beds — is among the most dangerously underdiagnosed variants. A 2024 systematic review published in MDPI (NIH) found that 53.8% of acral amelanotic melanomas arise on the foot, and that these were initially misdiagnosed as non-healing ulcers, traumatic injuries, or fungal infections in the overwhelming majority of cases.
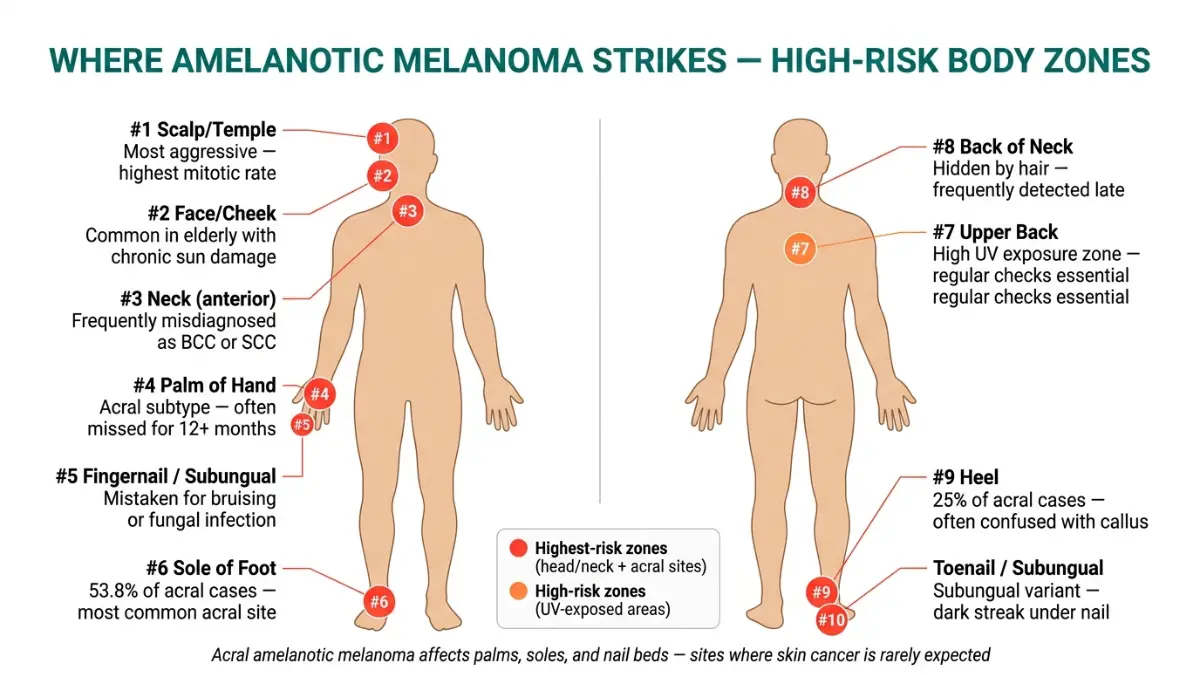
Highest-risk body locations include:
- Scalp and back of neck (highest average mitotic rates)
- Sole of foot, especially the heel
- Under fingernails or toenails (subungual)
- Palms of the hands
- Mucosal surfaces (lips, oral cavity)
⚡ Act now: Conduct a full-body self-check today. Photograph and date any suspicious pink, red, or colorless spots. Use our Symptom Checker to document your findings before your dermatology appointment.
How Amelanotic Melanoma Is Diagnosed — From Suspicion to Confirmation
No photograph, app, or visual inspection can definitively diagnose amelanotic melanoma. A biopsy is not optional — it is the only reliable diagnostic tool. Here is the step-by-step clinical journey.
Step 1 — Dermoscopy (The First Line of Clinical Suspicion)
A trained dermatologist uses a handheld dermatoscope to detect irregular vessel patterns that are invisible to the naked eye. This is currently the best non-invasive screening tool for colorless skin cancer, but it requires a specialist — not a general practitioner.
Step 2 — Biopsy (Mandatory for Definitive Diagnosis)
Three biopsy types are used:
- Excisional biopsy — preferred; removes the entire lesion with a margin
- Punch biopsy — cylindrical core sample; appropriate for smaller lesions
- Shave biopsy — least ideal; can underestimate tumor depth
Step 3 — Interpreting Your Pathology Report
Ask your oncologist or dermatologist to walk you through each of these values:
| Metric | What It Measures | Clinical Significance |
|---|---|---|
| Breslow Thickness | Tumor depth in millimeters | Primary staging criterion |
| Mitotic Rate | Speed of cell division | Indicator of aggressiveness |
| Ulceration | Surface breakdown | Automatically worsens stage |
| Sentinel Node Status | Lymph node involvement | Determines systemic spread |

Tumors under 1mm Breslow thickness carry the lowest metastatic risk. Tumors exceeding 4mm carry the highest. See our comprehensive guide to understanding your biopsy results, timeline, and report for patient-friendly breakdowns of every value.
When to request a second opinion: Always seek independent pathological review for amelanotic lesions. Per the NCI’s melanoma treatment patient guidelines, pathological misclassification of melanocytic lesions remains a documented clinical challenge — especially for amelanotic variants.
Amelanotic Melanoma Treatment & Survival Rates — 2026 Update
Treatment for amelanotic melanoma follows the same stage-based pathway as pigmented melanoma — but because diagnosis almost universally comes later, most patients begin at a higher stage. This directly impacts treatment intensity and outcomes.
Stage-by-Stage Treatment Roadmap
| Stage | Primary Treatment | Adjuvant / Systemic Options |
|---|---|---|
| Stage I | Wide Local Excision (WLE) | SLNB if Breslow ≥0.8mm |
| Stage II | WLE + Sentinel Lymph Node Biopsy | Pembrolizumab (high-risk cases) |
| Stage III | Surgery + systemic therapy | Nivolumab, pembrolizumab, ipilimumab |
| Stage IV | Immunotherapy + targeted therapy | BRAF/MEK inhibitors; TIL therapy (Amtagvi, FDA 2024) |
⚡ The 2026 Immunotherapy Survival Breakthrough
This data is not published by any major competitor — and it changes everything.
A landmark 2025 analysis of the SEER 17 database found a dramatic improvement in amelanotic melanoma survival outcomes — driven entirely by the introduction of modern immunotherapy:
- 2-year distant-stage survival (2000–2005): 26.4%
- 2-year distant-stage survival (2016–2021): 58.8%
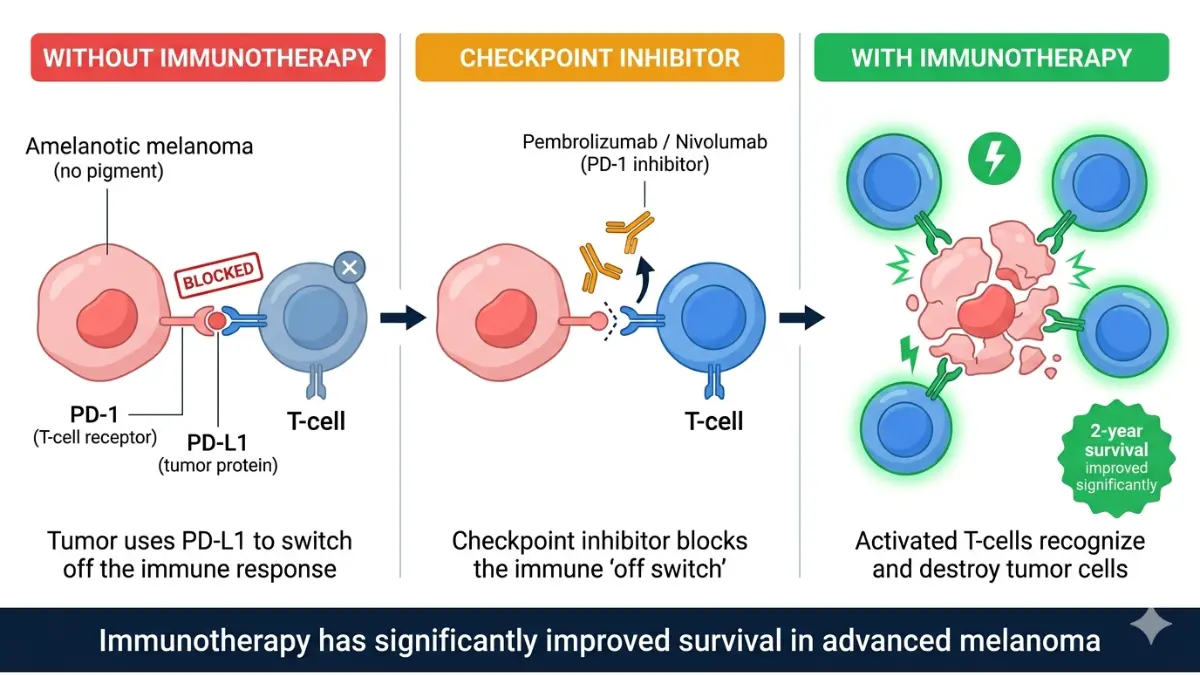
That represents more than a doubling of survival for Stage IV patients. PD-1 checkpoint inhibitors — pembrolizumab (Keytruda) and nivolumab (Opdivo) — are the primary drivers of this shift.
5-Year Disease-Specific Survival:
| Population | 5-Year DSS |
|---|---|
| Amelanotic melanoma (all stages) | ~77% |
| Pigmented melanoma (all stages) | ~84% |
| Stage I amelanotic melanoma | ~95%+ |
| Distant-stage, post-2016 (2-yr) | ~58.8% |
Who faces the highest risk: Men aged 85 and older carry a 1.86x higher disease-specific mortality risk compared to those aged 45–64. Early detection at younger ages — before tumor thickness escalates — remains the single most impactful clinical intervention available.
The NCI’s melanoma research advances page confirms that lifileucel (Amtagvi), the first FDA-approved TIL therapy for any solid tumor, received approval in 2024 and now offers a survival pathway for advanced patients who have progressed past checkpoint inhibitor therapy.
For a full clinical breakdown of immunotherapy mechanisms and current approvals, see our guide on how immunotherapy works for cancer patients.
What To Do Right Now — Your Action Checklist
Knowing about amelanotic melanoma is only half the battle. Here is your five-step action protocol — written for patients, not clinicians.
5-Step Action Protocol
1. SEE IT Perform a monthly full-body skin exam under good lighting. Look specifically for pink, red, or colorless spots that are new, growing, or that simply look “different” from your other lesions.
2. DOCUMENT IT Photograph any suspicious lesion with a ruler or coin for scale. Note the date. Track it for a maximum of 4–6 weeks — not months.
3. VISIT A DERMATOLOGIST Request a full-body exam with dermoscopy, not just a visual inspection. Ask directly: “Could this be amelanotic melanoma? I’d like a biopsy if there’s any uncertainty.”
4. PUSH FOR A BIOPSY The CDC confirms that biopsy is the only reliable diagnostic tool for skin cancer. Do not accept a visual dismissal for a persistent, growing, or non-healing lesion.
5. FOLLOW UP CONSISTENTLY After excision, confirm clear pathological margins. Return for check-ups every 3 months for the first two years.
Prevention Checklist
- Apply SPF 30+ broad-spectrum sunscreen every single day — not just at the beach
- Wear UV-protective clothing, wide-brim hats, and UV-blocking sunglasses outdoors
- Never use tanning beds — they significantly increase melanoma risk at any age
- Schedule an annual full-body dermatology exam starting at age 30 (earlier with risk factors)
- Know your genetic baseline — use our Genetic Risk Assessment Tool before your next appointment
For the most complete clinical overview of all melanoma types, staging, and current treatment protocols, read our melanoma symptoms, stages, and treatment pillar guide.
Frequently Asked Questions About Amelanotic Melanoma
Q1. What does amelanotic melanoma look like?
Amelanotic melanoma appears as a pink, reddish, skin-colored, or nearly colorless spot. It may resemble a pimple, scar, cyst, or flat pink patch. There is no brown or black pigmentation — which is precisely what makes it so easily dismissed. Under dermoscopy, irregular blood vessel patterns are typically the only visible clinical marker.
Q2. Can skin cancer be pink or red with no dark color?
Yes — and this is one of the most underappreciated facts in dermatology. Colorless skin cancer is a real and well-documented clinical phenomenon. Amelanotic melanoma actively produces no melanin, presenting as pink, red, white, or skin-toned. Any persistent pink or reddish lesion that does not heal warrants immediate dermatological evaluation.
Q3. Why does amelanotic melanoma get misdiagnosed so often?
Because it defeats the standard ABCDE rule on the “Color” criterion. Without dark pigment, these lesions are routinely confused with basal cell carcinoma, eczema, pimples, and benign cysts. Clinical misdiagnosis rates up to 87.5% are documented in peer-reviewed studies, with most lesions present for over 12 months before correct diagnosis.
Q4. Is amelanotic melanoma more dangerous than regular melanoma?
In practice, yes — primarily due to delayed diagnosis. Patients present at more advanced stages with greater Breslow depth, higher ulceration rates, and more aggressive tumor behavior. The 5-year survival gap (77% vs. 84%) is driven almost entirely by late detection, not inherent incurability. Early detection closes this gap dramatically.
Q5. What is the survival rate for amelanotic melanoma in 2026?
Overall 5-year survival is approximately 77% across all stages. Stage I survival approaches 95%+. Critically, 2-year distant-stage survival has more than doubled since 2016, reaching 58.8% — driven by checkpoint immunotherapy. See our full breakdown of melanoma statistics 2026 for comprehensive data by stage and demographic.
Q6. Can amelanotic melanoma appear on the foot or under a nail?
Yes. Acral amelanotic melanoma specifically targets the palms, soles, and subungual (under-nail) areas. Over 53% of acral cases arise on the foot. These are routinely misdiagnosed as fungal infections, traumatic bruising, or plantar warts — often for 12+ months — leading to preventable late-stage diagnoses.
Q7. Does the ABCDE rule work for amelanotic melanoma?
No — not reliably. ABCDE was designed for pigmented lesions and fails specifically on the “C” (Color) criterion for amelanotic melanoma. Patients and clinicians should instead use the 5-Sign Framework in Section 3 of this article. Our dedicated guide to melanoma ABCDE warning signs and moles explains precisely where the standard rule applies and where it breaks down.
Q8. How fast does amelanotic melanoma grow?
Amelanotic melanoma can develop and expand within weeks to a few months — making it one of the faster-growing melanoma subtypes. Nodular amelanotic variants in particular can achieve dangerous Breslow depth in a short timeframe. Any new lesion growing noticeably within 4–8 weeks requires urgent dermatological review — not watchful waiting.
Q9. Can children get amelanotic melanoma?
Yes — and this is critically underreported. Approximately 70% of all childhood melanomas are amelanotic, according to NCI data. A pink or reddish spot on a child that “doesn’t look like cancer” may actually represent the most common form of pediatric melanoma. Any atypical, growing, or non-healing skin lesion in a child should be evaluated by a dermatologist immediately.
Q10. What are the 2026 treatment options for amelanotic melanoma?
Treatment is stage-dependent. Early-stage disease is treated with wide local excision, often combined with sentinel lymph node biopsy. Higher-risk Stage II–III cases receive adjuvant immunotherapy (pembrolizumab or nivolumab). Stage IV disease now has access to PD-1 checkpoint inhibitors, BRAF/MEK targeted therapy, and the FDA-approved TIL therapy lifileucel (Amtagvi, 2024). See our guide on Stage 4 melanoma treatment options and survival therapy.
Q11. Can amelanotic melanoma be cured if caught early?
Yes — and this is the most important fact in this entire article. Stage I amelanotic melanoma treated promptly with wide local excision carries a near-normal long-term prognosis. The survival gap versus pigmented melanoma is almost entirely a product of late detection, not biological incurability. Early action — driven by awareness of the 5 warning signs above — is the single variable most within your control.
⚠️ Medical Disclaimer: This article is for educational and informational purposes only. It does not constitute medical advice, diagnosis, or a treatment plan. Always consult a qualified dermatologist or oncologist for skin concerns. For health tools and additional resources, visit mymedicineadvisor.com.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.