On This Page – Quick Medical Summary
In 1977, reggae legend Bob Marley noticed a dark streak forming beneath his toenail. He assumed it was a soccer injury. It wasn’t.
It was acral lentiginous melanoma — one of the deadliest and most frequently overlooked forms of skin cancer. By the time it was correctly identified, it had already spread. Bob Marley died at 36.
This story isn’t rare. It’s happening right now, in 2026, to thousands of Americans.
Melanoma appears most commonly on the back, legs, and face — but in 2026, an estimated 112,000 Americans will be diagnosed with invasive melanoma, and a significant number of those cases will originate in spots most people — and even some clinicians — never think to check.
The survival rate when melanoma is caught early: 99%. The survival rate when it spreads to distant organs: 35%.
That gap is not a medical mystery. It is a detection failure — and it is entirely preventable.
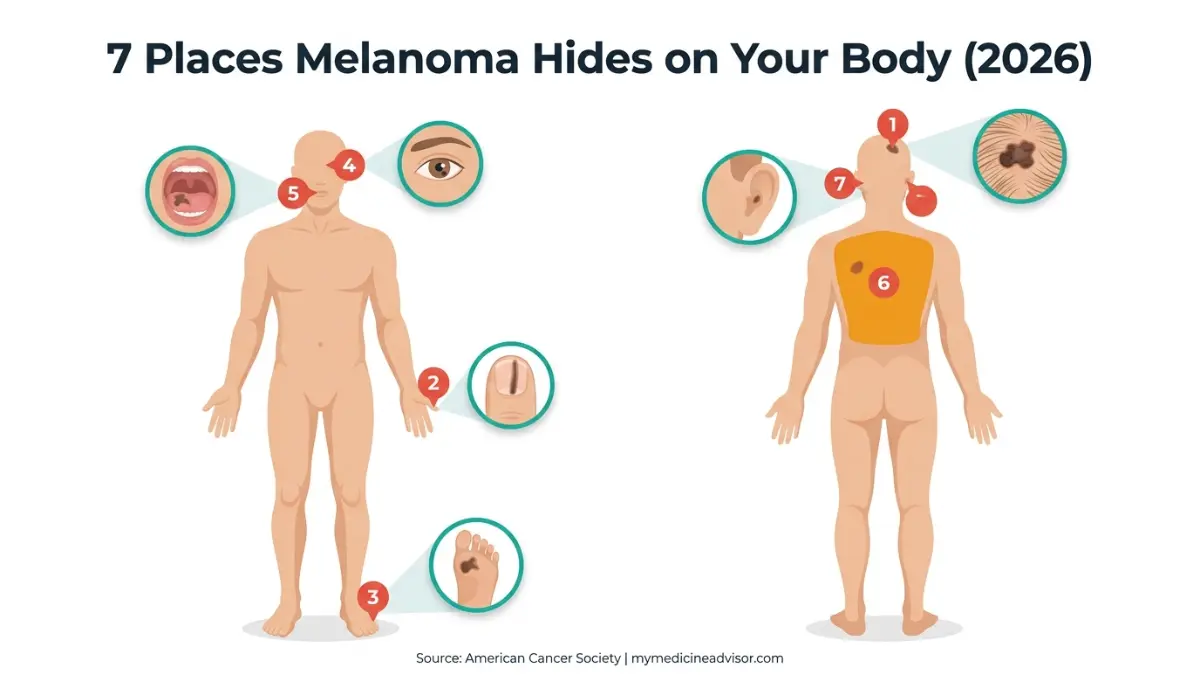
Here are the 7 body locations where melanoma appears and gets missed most dangerously in 2026.
The 7 Body Spots Where Melanoma Appears — And Gets Missed
1. The Scalp — Hidden Beneath Your Hair
Scalp melanoma accounts for fewer than 5% of all melanoma cases, but it carries disproportionately high mortality rates. The reason is simple: hair hides it.
By the time a scalp melanoma is discovered, it has often already advanced to a deeper stage. The scalp is also rich in blood vessels and lymphatic channels, giving melanoma cells a faster route to spread throughout the body, as Moffitt Cancer Center’s dermatology team explains.
What it looks like:
- A dark, asymmetric patch beneath parted hair
- A mole that bleeds when combing or brushing
- A raised, crusted lesion that doesn’t heal
Who is most at risk: Men over 50, people with thinning hair, and those who part their hair the same way for years — creating a chronic UV exposure line.
✅ What This Means For You: Ask your hairdresser or barber to alert you to any unusual spots at every visit. Use a handheld mirror in bright light to check your scalp monthly.
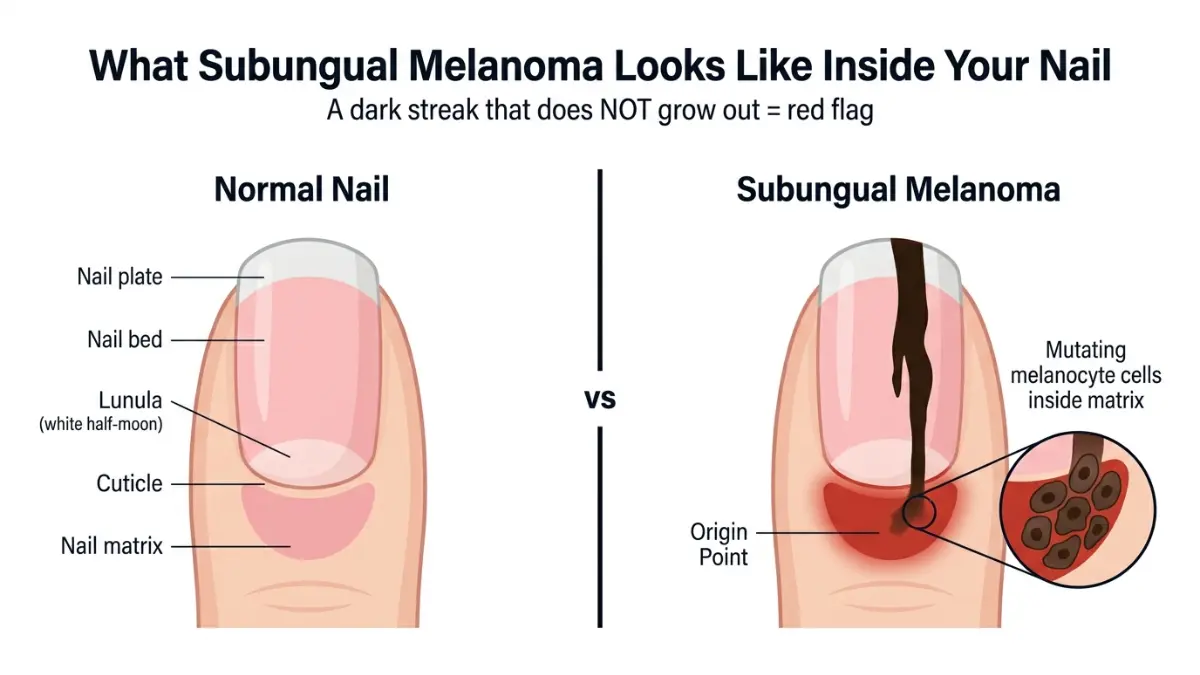
2. Under the Nails — Subungual Melanoma
This is the type that killed Bob Marley. Known as subungual melanoma, it appears beneath the fingernails or toenails as a brown or black vertical streak running from the base of the nail to the tip.
Unlike a bruise — which grows out with the nail — a melanoma streak stays in place. Unlike a fungal infection, it typically affects only one nail at a time.
The thumb and big toe are the most commonly affected areas, though it can appear under any nail. According to the American Academy of Dermatology, it is more prevalent in older adults and people with darker skin tones.
⚡ Exclusive 2026 Warning — Nail Salon UV Lamps: Gel nail curing lamps emit ultraviolet A radiation. While a single exposure is low-risk, years of repeated exposure may accumulate DNA damage in the nail matrix — a risk that virtually no mainstream health site currently warns patients about. If you regularly get gel manicures, apply a broad-spectrum SPF 30+ sunscreen to your hands before every session.
What to watch for:
- A dark band of color that does not grow out
- Darkening of the skin around the cuticle (a sign of advanced disease)
- Nail lifting from the nail bed or splitting vertically
If any of these signs concern you, use our Symptom Checker to log your findings before your dermatology appointment.
3. Soles of the Feet and Palms — Acral Lentiginous Melanoma
These surfaces receive almost zero direct sun exposure. Yet acral lentiginous melanoma (ALM) develops here with alarming regularity — and it is the most common form of melanoma diagnosed in people of color across the USA, UK, and Australia.
ALM on the soles of the feet is routinely misdiagnosed for 12 to 24 months. Patients are told they have a plantar wart, a bruise, or a fungal infection. By the time the correct diagnosis is made, the cancer has often penetrated deeper layers of tissue.
Researchers at Columbia University’s Herbert Irving Comprehensive Cancer Center confirm that more than 80% of all melanomas — including acral types — are first noticed by the patient or a family member, not a clinician.
What it looks like:
- A flat, dark brown or black irregular patch
- A spot that looks like a bruise but never fades
- An open sore on the sole that doesn’t heal properly
✅ What This Means For You: Check the entire surface of both feet — including between the toes — every time you shower. Remove nail polish periodically to inspect the nails beneath.
4. Inside the Eye — Uveal/Ocular Melanoma
Melanoma appears inside the eye more often than most people realize. Known as uveal or ocular melanoma, it develops in the middle layer of the eyeball — the uvea — which contains the iris and the muscles controlling it.
Most patients have no pain and no visible external symptoms in the early stages. The condition is often discovered accidentally during a routine eye exam when a dark spot is noticed on the iris or retina.
City of Hope Cancer Center notes that ocular melanoma is the most common primary intraocular malignancy in adults, and early eye screenings remain the most reliable detection method.
Warning signs:
- A dark spot growing within the colored part of the eye
- Sudden changes in vision or blurring
- Flashes of light or floating shapes (photopsia)
✅ What This Means For You: Don’t skip your annual eye exam. Take our free Eye Exam Tool as a basic screening supplement between clinical visits.
5. Mouth, Nose, and Genitals — Mucosal Melanoma
Mucosal melanoma develops in the mucous membranes lining the mouth, nasal cavity, throat, anus, and genitals. It represents roughly 1% of all melanoma diagnoses — but its outcomes are far worse than skin-based melanoma because it is almost always diagnosed at an advanced stage.
According to the American Cancer Society’s signs and symptoms page, mucosal melanoma may appear as dark, irregular spots or patches in these tissues — and it is uniquely resistant to standard therapies.
Warning signs to watch for:
- A dark or irregularly pigmented patch inside the mouth
- Persistent nosebleeds with no clear cause
- Nasal obstruction or loss of smell
- An unusual lesion on genital skin that doesn’t resolve
✅ What This Means For You: Your dentist can be your first line of defense. Ask them to inspect the inside of your mouth, lips, and gum line at every check-up — not just your teeth.
6. The Upper Back — The Blind Zone in Men
The upper back is the single most common location where melanoma appears in men under 50 in the United States, according to dermatological studies published on PubMed Central. Yet it is one of the hardest areas to self-examine.
You cannot see your own upper back without a mirror — and most men do not look. Melanoma in this region can grow and evolve for months or years before being noticed.
Risk profile:
- Men aged 30–55 who have had one or more blistering sunburns
- People who use tanning beds — which double melanoma risk over time
- Those with a family history of melanoma or multiple atypical moles
Learning to recognize the full spectrum of melanoma warning signs and symptoms is essential for this high-risk group.
✅ What This Means For You: Schedule a partner or family member to photograph your back every 3 months. Compare images side-by-side. Any new dark spot, growing mole, or changing lesion warrants a dermatologist visit within 2 weeks.
7. Behind the Ears and the Ear Canal
The outer ear and area directly behind it receive continuous sun exposure throughout a person’s lifetime — yet they are almost never included in a typical self-exam or sunscreen application.
As Nebraska Medicine’s dermatology team points out, melanoma and other skin cancers on the ears are often advanced by the time they are found simply because patients and even some primary care physicians overlook this area during routine checks.
What to look for:
- A scaly or crusted patch on the outer ear
- A dark or irregular mole on the ear lobe or behind the ear
- Any lesion that bleeds when touched
✅ What This Means For You: Include the back of both ears in every sunscreen application and monthly skin check — it takes 10 seconds and could save your life.
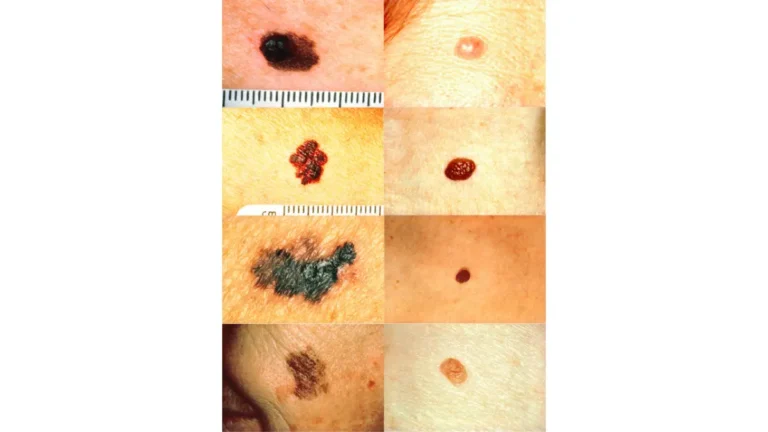
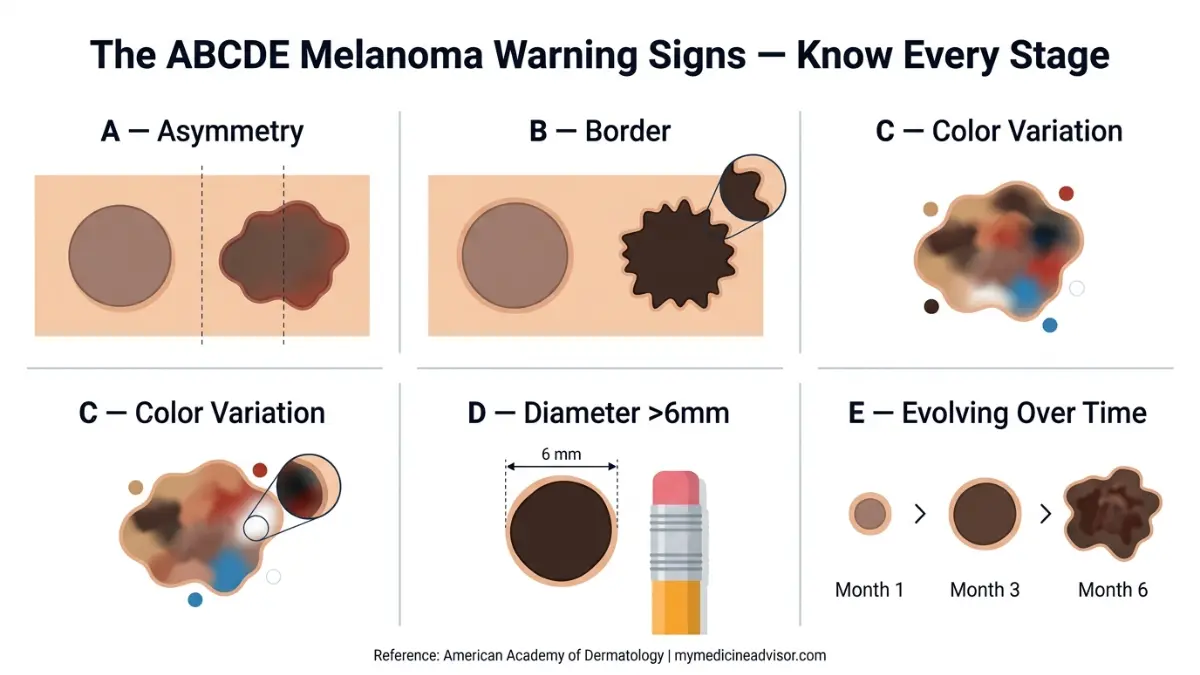
The ABCDE Rule + The Ugly Duckling Test
Understanding where melanoma appears is only half the battle. Knowing what to look for at each location is equally critical.
The ABCDE Rule — Your Screening Framework
| Letter | Meaning | What to Check |
|---|---|---|
| A | Asymmetry | One half doesn’t match the other |
| B | Border | Edges are ragged, notched, or blurred |
| C | Color | Multiple shades — brown, black, red, white, or blue |
| D | Diameter | Larger than 6mm (pencil eraser) — but size alone isn’t definitive |
| E | Evolving | Any change in size, shape, color, or new symptoms like bleeding |
The Skin Cancer Foundation’s warning signs guide emphasizes that not all melanomas follow the ABCDE rule — particularly amelanotic (colorless) melanomas, which can appear as pinkish, skin-toned lesions.
The Ugly Duckling Test
This method works on a simple principle: most of your moles look like each other. A melanoma looks different — it stands out from the crowd like an ugly duckling.
Look for any spot that is notably larger, smaller, darker, lighter, or differently shaped compared to your surrounding moles. Isolated spots with no neighboring moles for comparison are also considered red flags.
For a deeper breakdown, review our complete guide to melanoma ABCDE signs and moles.
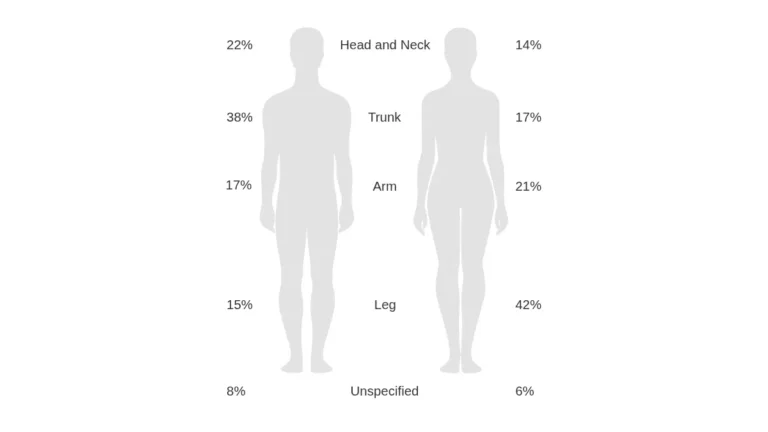
Where Melanoma Appears Most — By Age, Gender, and Skin Tone
Location patterns for melanoma differ significantly based on demographic factors. Understanding your personal risk profile helps prioritize which areas to examine most carefully.
| Group | Most Common Location | Relative Risk Level |
|---|---|---|
| Men under 50 | Upper back and chest | High |
| Women under 50 | Legs (especially calves) | High |
| Men and women over 60 | Head, neck, and face | Very High |
| People with darker skin tones | Palms, soles, and nails (ALM) | High — often late-diagnosed |
| Fair-skinned individuals | Torso, arms, and face | High |
| Outdoor workers | Face, scalp, and forearms | Very High |
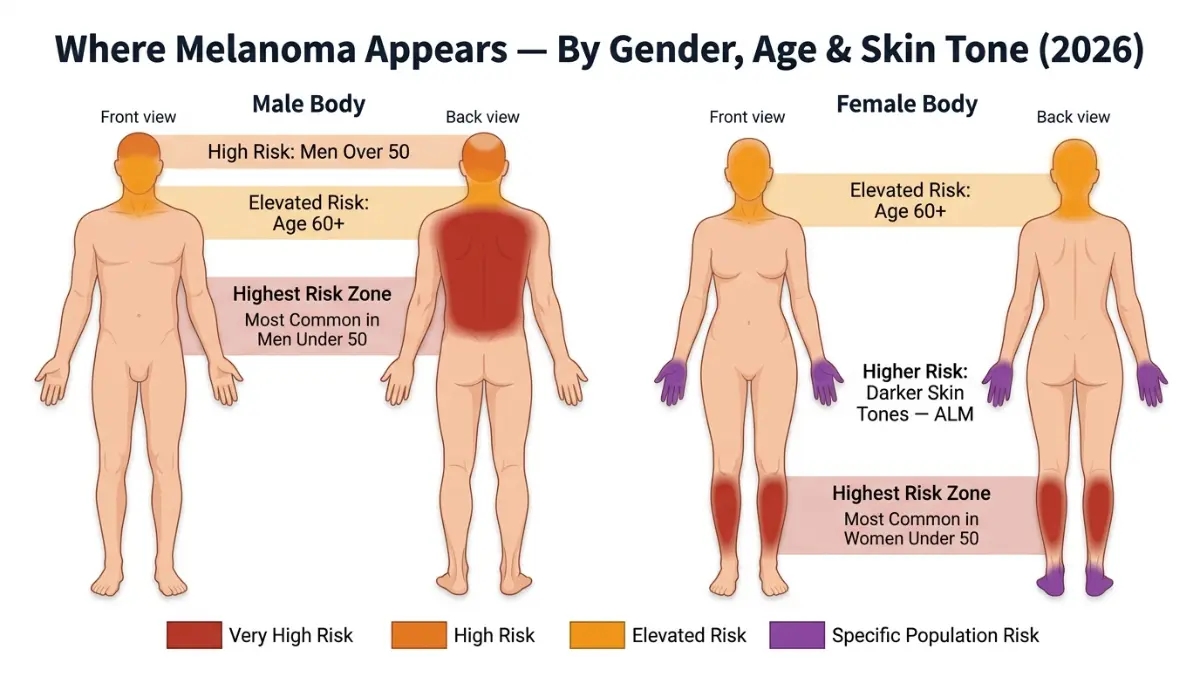
Research analyzing over 360 melanoma patients across two oncology centers found that women showed statistically significant central-body melanoma patterns, while men’s lesions occurred more frequently in peripheral areas — with head and neck lesions more common on the left side, potentially linked to driver-side UV exposure in left-hand traffic countries like the USA.
To assess your personal hereditary and lifestyle risk factors, use our free Genetic Risk Assessment Tool — it takes under 3 minutes and flags your highest-risk categories instantly.
For a full statistical breakdown of diagnosis rates and demographic trends, explore our Melanoma Statistics 2026 report.
The 7-Step Monthly Self-Exam — Head to Toe
According to the Cleveland Clinic’s melanoma care guide, more than 80% of melanomas are first identified by the patient, a partner, or a family member — not a physician. A monthly self-exam is your most powerful early-detection tool.
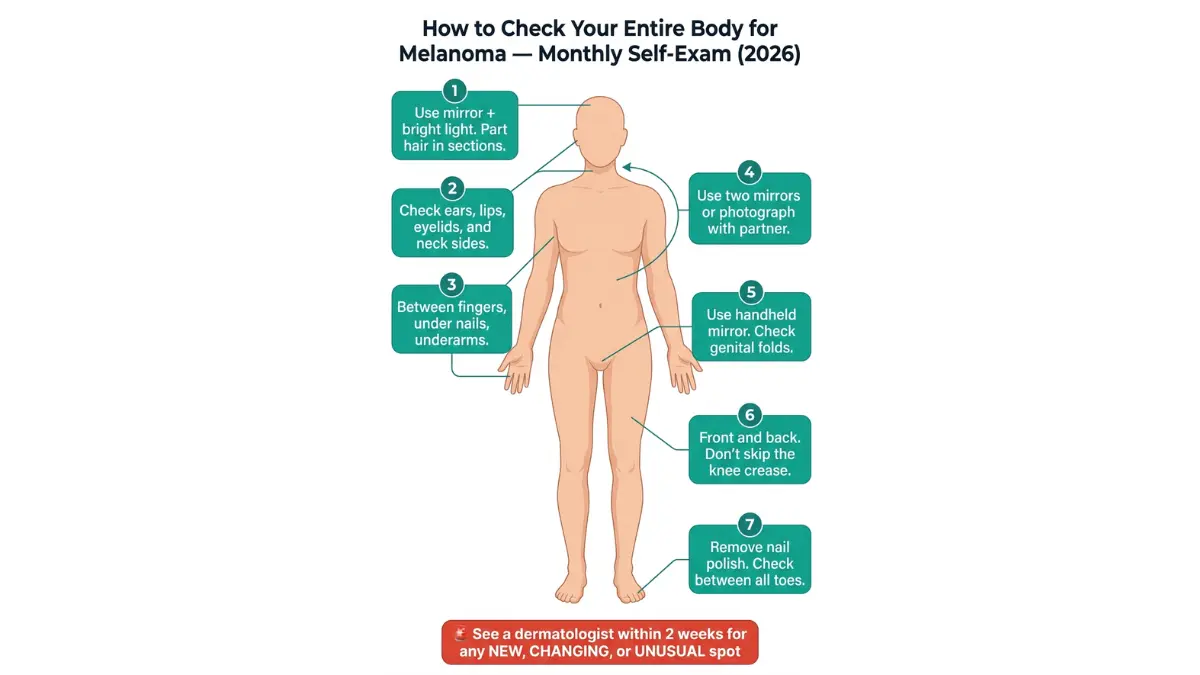
How to perform a complete self-exam:
- Face and Scalp — Use a handheld mirror in bright natural light. Part your hair in multiple sections. Check your ears, lips, and eyelids.
- Neck and Chest — Examine the front, sides, and back of your neck. Check the entire chest and upper torso.
- Arms and Hands — Check between the fingers, under the nails, and the underarm area.
- Back and Buttocks — Use two mirrors or ask a partner to photograph the entire back surface. Don’t skip the gluteal fold.
- Genitals and Groin — Use a mirror. Look for any irregular pigmented patches or lesions that don’t resolve.
- Legs and Calves — Sit on the edge of a chair. Examine from the thigh to the ankle — front and back. Check the back of the knee.
- Feet and Soles — Remove all nail polish. Examine the entire sole, between each toe, and beneath every nail.
🚨 When to See a Dermatologist Immediately: Any spot that is new, changing, or unusual — regardless of its location — warrants a dermatologist review within 2 weeks. Do not wait for your annual physical.
Use our Symptom Checker to document and track any suspicious changes before your appointment.
For a detailed understanding of what happens if a lesion is flagged, read our comprehensive guide on melanoma symptoms, stages, and treatment.
2026 Melanoma Statistics and What Experts Want You to Know
The data this year is sobering — but also deeply motivating.
2026 U.S. Melanoma Statistics (American Cancer Society):
| Metric | 2026 Figure |
|---|---|
| Total estimated diagnoses | 234,680 |
| Invasive melanoma cases | 112,000 |
| In situ (non-invasive) cases | 122,680 |
| Estimated deaths | 8,510 |
| 5-year survival (localized) | 99% |
| 5-year survival (regional spread) | 74% |
| 5-year survival (distant organs) | 35% |
Source: American Cancer Society, Key Statistics for Melanoma Skin Cancer 2026
What leading dermatologists say:
Dr. Adam Sutton, double board-certified dermatologist and Mohs surgeon at Nebraska Medicine, states that when melanoma is diagnosed early, it is highly curable — and that full-body skin exams by board-certified dermatologists remain the gold standard for catching it before it advances.
The National Cancer Institute’s melanoma treatment overview confirms that surgical excision of localized melanoma under local anesthesia is highly effective — but only when the melanoma has not yet penetrated the dermis.
The single most important prevention action in 2026: Annual full-body skin screening with a board-certified dermatologist. If you have multiple moles, a family history of melanoma, or a history of tanning bed use, schedule a screening every 6 months.
For the latest on AI-assisted early detection technology now being deployed in US dermatology clinics, read our Melanoma 2026: AI Screening and Survival feature.
Reducing Your Risk — No Matter Where Melanoma Appears
Sun protection is the most evidence-based strategy for reducing melanoma risk — but it must cover the spots that most people miss.
Sun Protection by Body Zone
| Body Zone | Common Error | Correct Action |
|---|---|---|
| Scalp | Not applying SPF spray under parted hair | Use SPF 50 scalp spray; wear a wide-brim hat |
| Ears | Never applied SPF behind ears | Apply SPF to entire ear + back with every use |
| Nails / Hands | Skipped before gel nail UV lamp | Apply SPF 30 to hands before every salon visit |
| Eyes | No UV-blocking sunglasses | Wear wraparound UV400 certified lenses daily |
| Feet / Soles | Missed during sunscreen application | Apply SPF to tops and soles when exposed |
| Back | Partner not involved in application | Designate a back-application partner or use a back-spray SPF |
Additional Risk-Reduction Steps
- Avoid tanning beds entirely. UV lamps in tanning beds emit UV-A radiation that penetrates deeper than UV-B sunlight — and tanning bed use before age 35 increases melanoma risk by approximately 75%, according to the Skin Cancer Foundation.
- Reapply sunscreen every 2 hours outdoors — and after swimming or sweating.
- Perform a monthly self-exam. It takes 10 minutes and could mean the difference between a 99% and a 35% survival rate.
- Know your genetic history. If a first-degree relative has had melanoma, your personal risk is significantly elevated. Use our Genetic Risk Assessment Tool to understand your baseline risk and discuss targeted screening intervals with your dermatologist.
For the complete picture on how melanoma differs from other skin cancers and why early intervention changes everything, explore our full skin cancer hub.
If you or a loved one has already received a diagnosis, our dedicated guide on Stage 4 melanoma survival and therapy options provides a comprehensive, evidence-based overview of current treatment pathways.
⚕️ Medical Disclaimer: This article is for educational and informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a board-certified dermatologist or licensed healthcare provider regarding any changes to your skin or personal health concerns.
FREQUENTLY ASKED QUESTIONS
Q1. Where does melanoma most commonly appear on the body?
In men, melanoma most commonly appears on the upper back and chest. In women, it most frequently develops on the legs, particularly the calves. After age 60, head and neck sites — especially the face — become the most common location for both sexes.
Q2. Can melanoma appear where the sun doesn’t shine?
Yes. Melanoma can appear in areas with zero sun exposure — including the soles of the feet, under the nails, inside the mouth, in the genital region, and even inside the eye. UV radiation is a trigger, not a requirement.
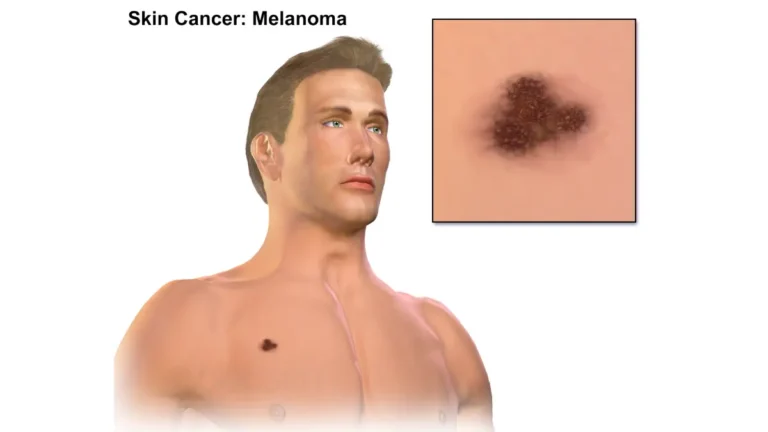
Q3. What does melanoma look like when it first appears?
Early melanoma often appears as a flat or slightly raised discolored patch. It may look like a new mole, a changing freckle, or a dark streak beneath a nail. Some melanomas (amelanotic) appear pink or skin-toned with no pigmentation.
Q4. Can melanoma appear under your fingernails?
Yes. Subungual melanoma appears as a brown or black vertical streak beneath the nail that does not grow out over time. It most commonly affects the thumbnail or big toenail and is frequently misidentified as a bruise or fungal infection.
Q5. Where does melanoma appear in people with darker skin?
In people with darker skin tones, melanoma most commonly appears on the palms of the hands, soles of the feet, and under the nails — a subtype called acral lentiginous melanoma (ALM). It is frequently diagnosed at a later stage in this population due to lower clinical awareness.
Q6. Can melanoma appear in the eye?
Yes. Uveal or ocular melanoma develops inside the eyeball, most often in the uvea — the layer containing the iris. It typically causes no pain in early stages and is most often detected during a routine eye examination.
Q7. How quickly does melanoma appear and spread?
Superficial spreading melanoma — the most common type — grows slowly outward on the skin surface for months before penetrating deeper layers. Nodular melanoma, however, is aggressive and can penetrate deeply within weeks. Early detection dramatically changes outcomes.
Q8. Does melanoma always appear as a dark spot?
No. Amelanotic melanoma has little to no pigment and appears as a pink, red, or skin-colored lesion. This makes it particularly dangerous — it doesn’t trigger alarm because it doesn’t look like the stereotypical dark mole.
Q9. Where does melanoma appear differently in men vs. women?
Men are significantly more likely to develop melanoma on the back, scalp, and torso. Women are more likely to develop it on the lower legs and calves. After age 60, both groups share the head and neck as primary risk zones.
Q10. Can melanoma appear inside the mouth or nose?
Yes. Mucosal melanoma develops in the mucous membranes lining the mouth, nose, throat, and genitals. It accounts for approximately 1% of diagnoses but carries a significantly worse prognosis than skin melanoma due to late detection.
Q11. How do I check where melanoma might appear on my back?
Stand in a well-lit room and use two mirrors — one wall-mounted, one handheld. Photograph your entire back every 3 months and compare images. Alternatively, ask a trusted partner or family member to inspect the full back surface, using the ABCDE criteria as a guide. An annual full-body skin check by a board-certified dermatologist is the gold standard.
📌 Related Reading:
- Melanoma Warning Signs and Symptoms — Full Guide
- Melanoma vs. Skin Cancer — Key Differences Explained
- Skin Cancer Signs: 12 Warning Symptoms You Should Never Ignore
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.