On This Page – Quick Medical Summary
Melanoma is a type of skin cancer — but it is the deadliest one. While most non-melanoma skin cancers grow slowly and rarely spread, melanoma can silently invade your lymph nodes, lungs, and brain within weeks of going undetected. In 2026, an estimated 234,680 new melanoma cases will be diagnosed in the United States alone — and 8,510 Americans will die from it.
Understanding the difference between melanoma vs skin cancer is not just academic. It could save your life.
📋 This article is for educational purposes only and does not constitute medical advice. Always consult a qualified, board-certified dermatologist for diagnosis and treatment decisions.
What Is Skin Cancer? The 4 Types You Must Understand
Skin cancer is an abnormal, uncontrolled growth of skin cells — most commonly triggered by ultraviolet (UV) radiation from the sun or tanning beds. According to the American Academy of Dermatology, more people are diagnosed with skin cancer each year in the United States than all other cancers combined.
But “skin cancer” is not one disease. There are four major types — and they behave very differently.
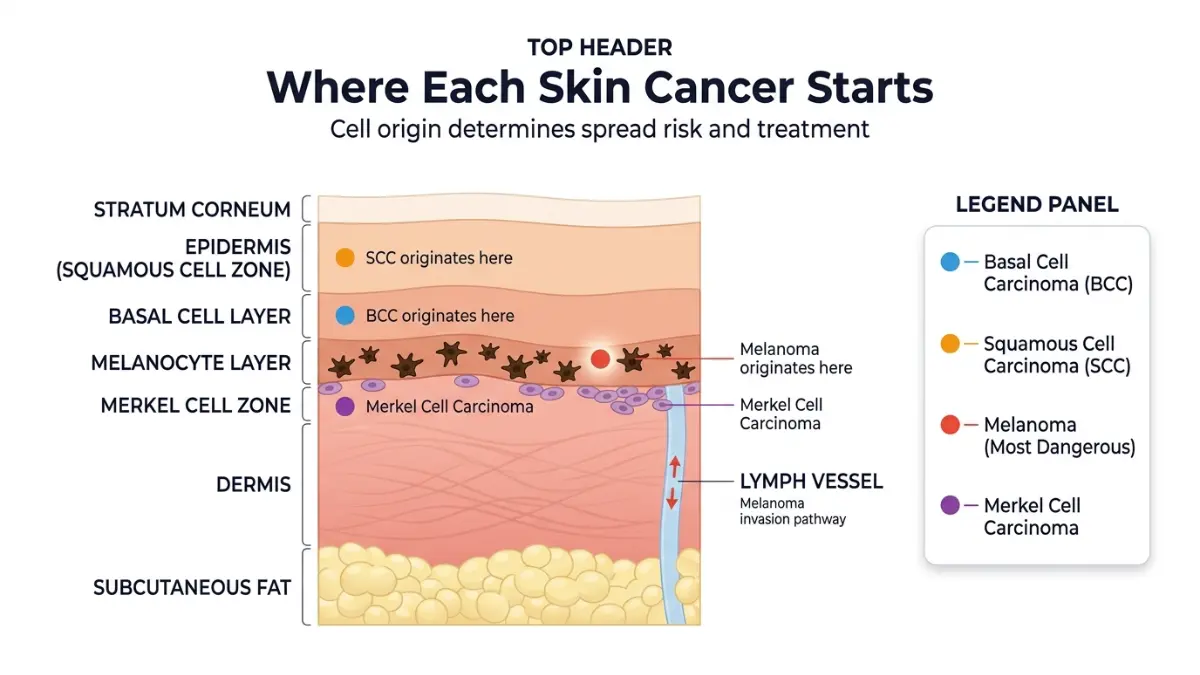
Basal Cell Carcinoma (BCC) — The Most Common
BCC is the most diagnosed cancer of any kind in the US, with over 4 million cases treated annually. It originates in the basal cells at the bottom of the epidermis. BCC is slow-growing, rarely spreads to other organs, and is nearly always curable with early treatment. It typically appears as a pearly bump or a flat, flesh-colored lesion on sun-exposed areas like the face, neck, or ears. You can read more about basal cell cancer cure rates and treatment options to understand what to expect after diagnosis.
Squamous Cell Carcinoma (SCC) — A Spreading Risk
SCC is the second most common skin cancer. It arises from the squamous cells in the outer layers of the skin. Unlike BCC, SCC can metastasize to the lymph nodes in certain high-risk situations — particularly when it is large, deep, or located on the ear or lip. The five-year survival rate for localized SCC exceeds 99%, but this drops significantly if left untreated.
Merkel Cell Carcinoma — The Most Overlooked Type
Merkel cell carcinoma is rare but deeply aggressive. It forms in the Merkel cells deep within the top layer of skin and typically appears as a fast-growing, shiny pink or red lump. Nearly everyone who develops it is over 50. Most competitors don’t cover this type at all — yet it carries one of the highest recurrence rates of any skin cancer.
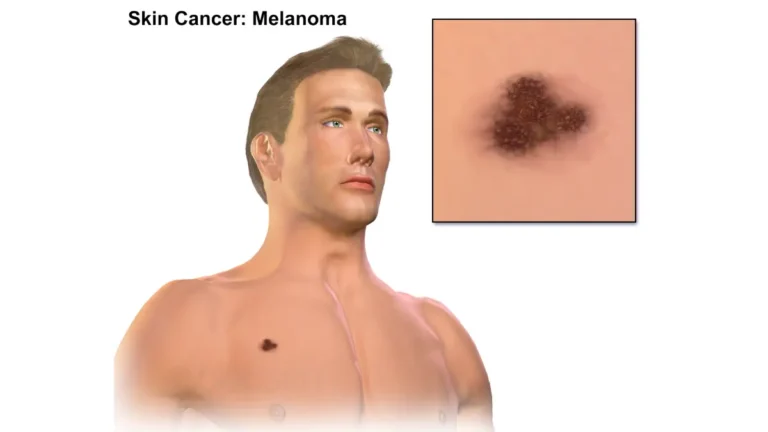
Melanoma — Why It Is Fundamentally Different
Melanoma arises from melanocytes, the pigment-producing cells that give your skin its color. It is significantly less common than BCC or SCC — but far more lethal. Unlike other skin cancers, melanoma spreads aggressively and early. According to the American Cancer Society, melanoma is responsible for the vast majority of skin cancer deaths despite representing only about 1% of total skin cancer cases.
If you have noticed any unusual skin changes, start by using our free Symptom Checker to log what you’re experiencing before your dermatologist appointment.
| Cancer Type | Cell Origin | Spread Risk | 5-Year Survival (Localized) |
|---|---|---|---|
| Basal Cell Carcinoma | Basal cells | Very rare | ~100% |
| Squamous Cell Carcinoma | Squamous cells | Low–moderate | ~99% |
| Merkel Cell Carcinoma | Merkel cells | High | ~76% |
| Melanoma | Melanocytes | High | ~99% (early) / 35% (metastatic) |
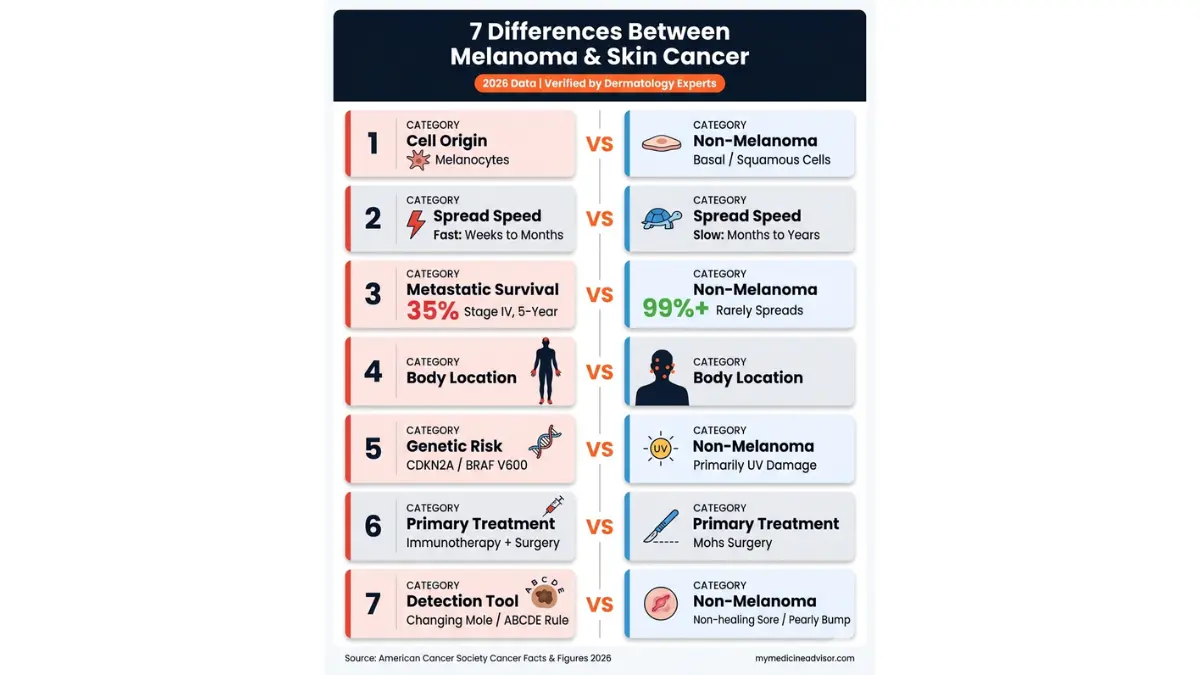
The 7 Deadly Differences — Melanoma vs Other Skin Cancers
This is the section no competitor delivers with precision. Here are the 7 clinically significant differences between melanoma and non-melanoma skin cancer — backed by 2026 data.
| Difference | Melanoma | Non-Melanoma (BCC/SCC) |
|---|---|---|
| 1. Cell Origin | Melanocytes (pigment cells) | Basal / Squamous / Merkel cells |
| 2. Spread Speed | Fast — lymph nodes and organs | Slow — stays local |
| 3. Survival (Metastatic) | 35% at 5 years | Rarely metastasizes |
| 4. Body Location | Anywhere, including non-sun areas | Predominantly sun-exposed areas |
| 5. Genetic Risk | CDKN2A / BRAF V600 mutations | Minimal genetic driver |
| 6. Treatment | Surgery + Immunotherapy + Targeted | Surgery / Mohs |
| 7. Detection Complexity | Can mimic normal moles | Usually a visible sore or bump |
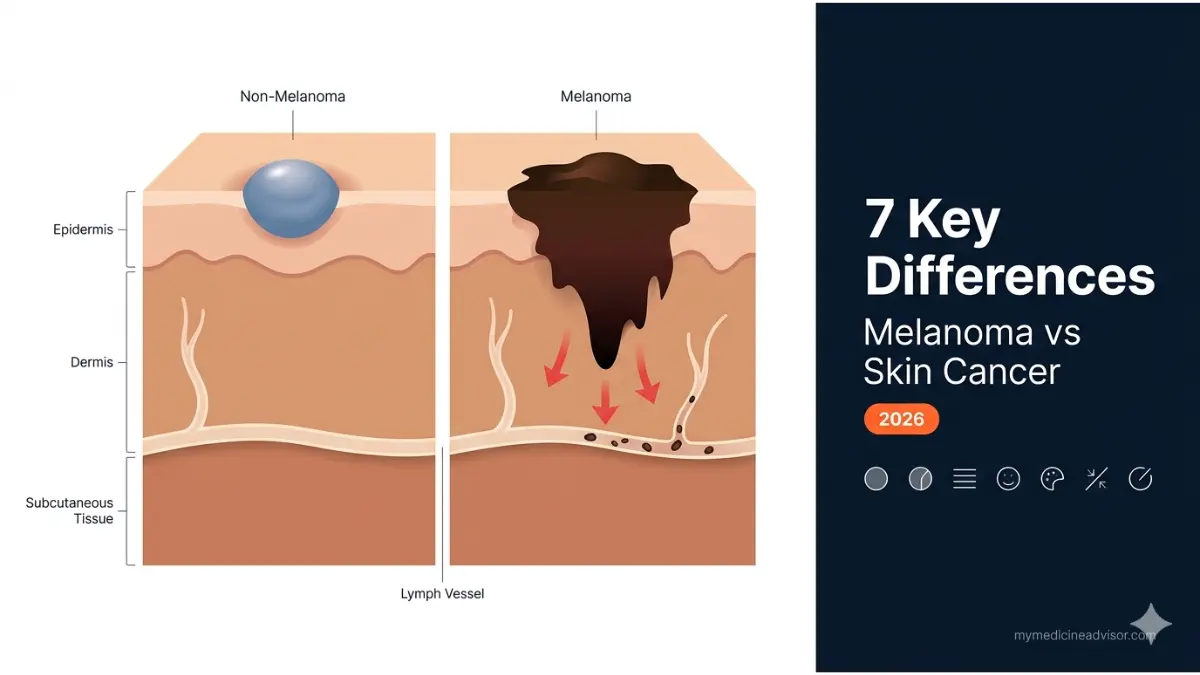
Difference #1 — Cell Origin: Why Melanoma Starts Deeper
Non-melanoma cancers originate in the upper keratinocyte layers of skin. Melanoma originates in melanocytes — pigment cells embedded in the lower epidermis. Because melanocytes are deeper and more mobile, melanoma has a biological head start when it comes to invasion. This cellular origin is why melanoma vs skin cancer is not an apples-to-apples comparison.
Difference #2 — How Fast Each Cancer Spreads
BCC grows so slowly that patients often don’t notice it for years. SCC may spread in certain anatomical locations, but the rate is still measured in months to years. Melanoma, however, can breach the dermis, enter the lymphatic system, and reach distant organs rapidly. The Skin Cancer Foundation confirms that melanoma’s metastatic potential is what separates it from all other common skin cancers.
Difference #3 — The Survival Rate Gap Is Shocking
When melanoma is caught at Stage I, the 5-year survival rate is approximately 99%. But once it reaches distant organs (Stage IV), that number collapses to just 35%, according to NCI SEER data. BCC and SCC virtually never reach this stage. This is the single most important number in the melanoma vs skin cancer conversation. Our dedicated guide to Stage 4 melanoma survival and therapy covers what to expect at advanced stages.
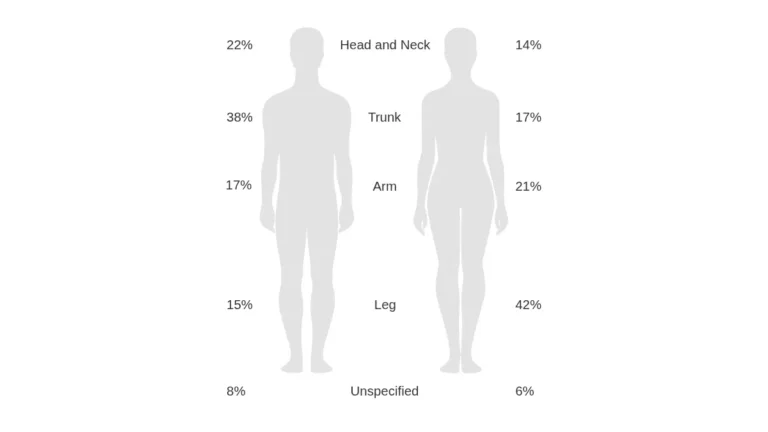
Difference #4 — Where on the Body They Appear
BCC and SCC appear almost exclusively on sun-exposed areas — face, ears, neck, forearms. Melanoma is different. Between 70% and 80% of melanomas arise on completely normal-looking skin, not existing moles. Additionally, melanoma can appear on the palms, soles of the feet, under the nails, and even inside the mouth — areas where many people never think to check.
Difference #5 — The Genetic Link Most Doctors Don’t Mention
Non-melanoma skin cancers are largely driven by cumulative UV damage — an environmental cause. Melanoma has a significant genetic dimension. The CDKN2A gene mutation and the BRAF V600 mutation are directly linked to melanoma risk and progression. If you have a family history of melanoma, consider using our free Genetic Risk Assessment Tool to understand your personal risk profile before your next dermatology visit.
Difference #6 — Treatment Pathways Are Completely Different
Mohs surgery is the gold standard for BCC and SCC — it removes the cancer layer by layer with very high precision. For melanoma, treatment depends on stage and can include wide local excision, sentinel lymph node biopsy, immunotherapy (pembrolizumab, nivolumab), BRAF-targeted therapy, and radiation. These treatments are explained further in our immunotherapy guide and chemotherapy side effects overview.
Difference #7 — Who Is at Highest Risk in 2026
This is the gap no competitor covers adequately. According to the Skin Cancer Foundation’s 2026 statistics, the five-year melanoma survival rate for Black patients is only 70%, compared to 95% for White patients. This 25-point gap exists primarily because melanoma in people with darker skin is diagnosed later — often on non-sun-exposed skin that goes unexamined. Every American, regardless of skin tone, needs annual skin checks.
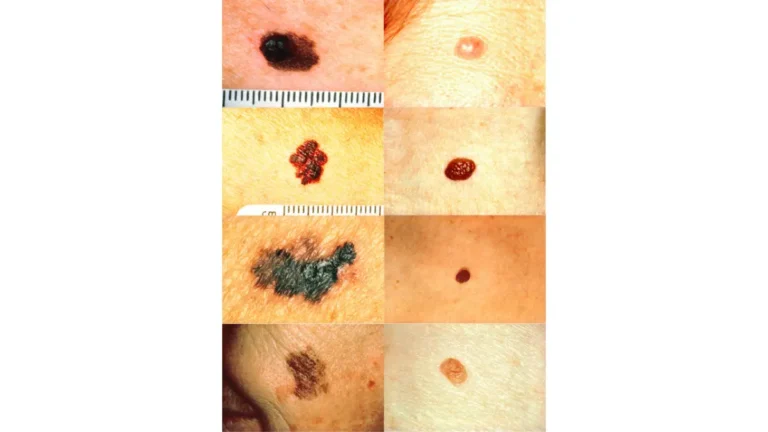
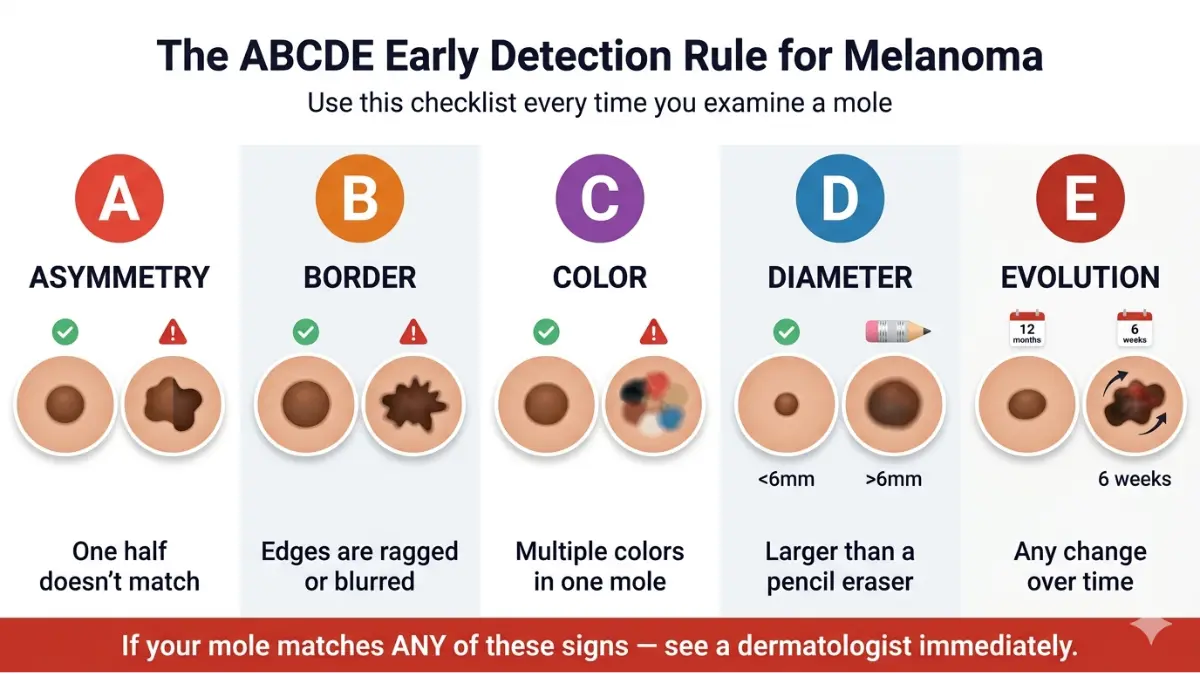
ABCDE Warning Signs — How to Spot Melanoma Before It Spreads
The ABCDE rule is a clinically validated early detection framework for identifying potentially cancerous moles and lesions. Every major health body — from the American Academy of Dermatology to the NCI — endorses it as the first-line screening tool.
For a comprehensive breakdown of all 12 warning signs of skin cancer, see our in-depth guide on skin cancer warning symptoms.
A — Asymmetry
If you draw a line through the middle of a mole and the two halves don’t match, that asymmetry is a warning sign. Normal moles are round and symmetrical.
B — Border Irregularity
Benign moles have smooth, well-defined borders. Melanoma lesions often have notched, ragged, or blurred edges that are difficult to clearly trace.
C — Color Variation
A normal mole is one shade of brown. A potential melanoma may contain multiple colors — shades of black, brown, tan, red, blue, or white — in a single lesion.
D — Diameter
Most melanomas are larger than 6mm (roughly the size of a pencil eraser) when first detected. However, some are found earlier and smaller — which is why size alone is not a reliable indicator.
E — Evolving
This is the single most critical warning sign. Any mole or spot that changes in size, shape, color, or begins bleeding, itching, or crusting over time warrants immediate evaluation. Normal moles don’t change.
🔴 What This Means For You: Research from the Skin Cancer Foundation shows that patients who wait more than 119 days after biopsy to begin melanoma treatment face a 41% higher risk of death compared to those treated within 30 days. Do not delay.
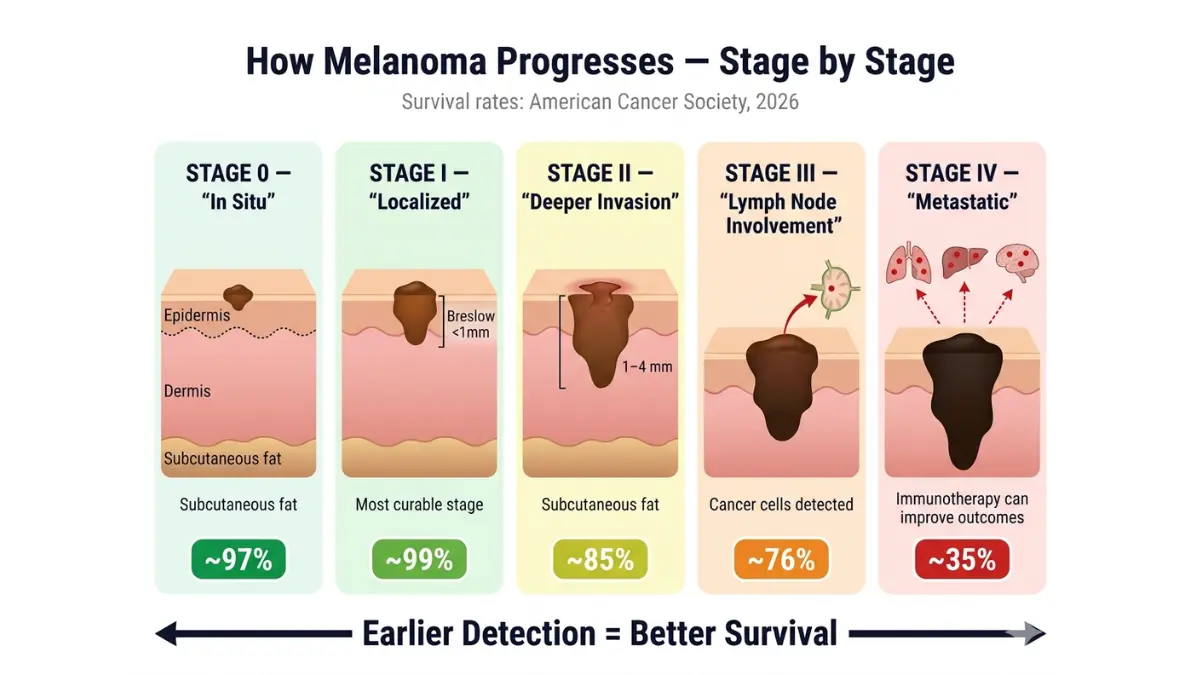
Melanoma Survival Rates 2026 — Stage-by-Stage Breakdown
Survival statistics provide context — not predictions. They are population-level estimates, not individual outcomes. That said, understanding these numbers is essential for informed decision-making.
According to American Cancer Society Cancer Facts & Figures 2026:
| Melanoma Stage | Description | 5-Year Survival Rate |
|---|---|---|
| Stage 0 (In Situ) | Confined to outer skin layer | ~97% |
| Stage I | Thin, localized | ~99% |
| Stage II | Thicker, still localized | ~85% |
| Stage III | Spread to nearby lymph nodes | ~76% |
| Stage IV | Metastasized to distant organs | ~35% |
For a detailed breakdown of what each stage means clinically, visit our guide on melanoma symptoms, stages, and treatment.
Stage III–IV: What 35% Really Means
A 35% five-year survival rate for Stage IV melanoma means that 65 out of 100 patients with metastatic melanoma will not survive five years with standard treatment. However, 2026 immunotherapy data changes this picture significantly. According to Cancer Research UK, combination immunotherapy with nivolumab and ipilimumab shows over 55% survival at 6.5 years in Stage III/IV patients — a dramatic improvement over chemotherapy-only outcomes.
The Racial Survival Gap in 2026
This data point is absent from virtually every competitor article. The five-year survival rate for Black melanoma patients is approximately 70%, compared to 95% for White patients — a 25-point disparity driven almost entirely by late-stage diagnosis. Melanoma in darker-skinned individuals most often appears on palms, soles, and nail beds — locations where self-examination rarely occurs.
⚡ Key Takeaway: Early detection is the single most powerful variable in melanoma outcomes. Annual full-body skin exams with a dermatologist are non-negotiable for high-risk individuals.
You can also explore our article on AI-powered melanoma screening in 2026 to understand how new technology is improving detection rates.
Treatment Differences — Melanoma vs Non-Melanoma Skin Cancer
Treatment selection is driven entirely by cancer type, stage, and depth. The gap between how BCC/SCC is treated versus how melanoma is managed is vast.
Treating BCC and SCC
For most basal cell and squamous cell carcinomas, surgical removal is curative:
- Mohs Micrographic Surgery — Gold standard for high-risk BCC/SCC. Removes tissue in precise layers, verifying cancer-free margins in real time. Cure rates exceed 99% for primary BCC.
- Excision — Standard surgical removal with clear margins.
- Cryotherapy — Freezing small, superficial lesions.
- Radiation therapy — Used when surgery is not possible or for elderly patients. See our overview of radiation therapy for how this works in practice.
According to the American Society for Mohs Surgery, Mohs surgery preserves the maximum amount of healthy tissue while achieving the highest cure rates for non-melanoma cancers.
How Melanoma Treatment Is Fundamentally Different
Melanoma treatment is staged-dependent and often multi-modal:
| Treatment | Used For | Notes |
|---|---|---|
| Wide Local Excision | All stages | Removes tumor with clear margins |
| Sentinel Lymph Node Biopsy | Stage I–III | Maps lymph node involvement |
| Immunotherapy | Stage III–IV | Pembrolizumab, Nivolumab |
| BRAF/MEK Targeted Therapy | BRAF+ Stage III–IV | Dabrafenib + Trametinib |
| Adjuvant Radiation | High-risk Stage II–III | Reduces recurrence risk |
| Chemotherapy | Advanced/refractory cases | Less common since immunotherapy |
The 2026 Immunotherapy Revolution
The emergence of checkpoint inhibitors (anti-PD-1 and anti-CTLA-4 drugs) has fundamentally changed Stage IV melanoma treatment. According to NCBI StatPearls, pembrolizumab and nivolumab have produced durable responses in patients who previously had very limited options. Ask your oncologist specifically about BRAF V600 mutation testing — it determines whether targeted therapy is an option for you.
🔵 What This Means For You: If you’ve been given a biopsy and are waiting on results, understanding what your biopsy results mean can help you have a more productive conversation with your care team.
Prevention, Risk Reduction & When to See a Doctor
The best melanoma outcome is the one that never happens. Evidence-based prevention is highly effective — and most Americans are not doing enough.
7 Evidence-Based Prevention Steps for 2026
- Apply SPF 30+ broad-spectrum sunscreen daily — even on cloudy days and in winter months.
- Avoid peak UV hours (10am–4pm) — UV index is highest during this window.
- Never use tanning beds — Women under 30 who use indoor tanning beds are six times more likely to develop melanoma, per the Skin Cancer Foundation.
- Wear protective clothing — UPF-rated fabric, wide-brim hats, and UV-blocking sunglasses.
- Get a full-body skin exam annually — A board-certified dermatologist can detect lesions invisible to the untrained eye.
- Perform monthly self-exams — Use a full-length mirror and a hand mirror. Check your scalp, between toes, palms, soles, and under nails.
- Know your genetic risk — If a first-degree relative has had melanoma, your risk is significantly elevated. Use our Genetic Risk Assessment Tool to map your family risk profile.
High-Risk Groups Who Should Get Screened Now
You are at elevated risk if you:
- Have 50 or more moles, or any atypical (dysplastic) nevi
- Have a personal or family history of melanoma or skin cancer
- Have fair skin, light eyes, or red/blond hair
- Have a history of blistering sunburns — especially before age 18
- Work outdoors regularly or live at high altitude
- Have a weakened immune system or are on immunosuppressive medications
When Exactly Should You See a Dermatologist?
See a dermatologist immediately if you notice:
- Any mole that is changing in size, shape, or color
- A new dark spot on your skin — even if it doesn’t itch or bleed
- A sore that has not healed within 3–4 weeks
- A shiny, pearly bump that bleeds easily
- Dark streaks under a fingernail or toenail that you cannot explain
- Any spot that fits the ABCDE criteria described in Section 3
If you are unsure whether your symptoms are worth reporting, start with our free Symptom Checker to document your findings before your appointment.
🟢 For a comprehensive deep-dive on everything melanoma — from early detection to AI-assisted screening tools in 2026 — read our full melanoma symptoms, stages, and treatment guide.
Frequently Asked Questions — Melanoma vs Skin Cancer
1. Is melanoma the same as skin cancer?
Melanoma is a type of skin cancer, but not all skin cancers are melanoma. Melanoma originates in melanocytes (pigment cells) and is significantly more aggressive than basal cell or squamous cell carcinoma.
2. Can non-melanoma skin cancer turn into melanoma?
No. BCC cannot transform into melanoma — they arise from entirely different cell types. However, having a history of non-melanoma skin cancer does increase your overall risk of developing melanoma.
3. What does early melanoma look like?
Early melanoma often resembles a changing or irregularly shaped mole. It may show multiple colors, have uneven borders, or be growing larger. Between 70–80% of melanomas appear on normal-looking skin — not pre-existing moles.
4. How fast does melanoma spread?
This varies by subtype. Nodular melanoma can penetrate deep skin layers within weeks. Superficial spreading melanoma may grow radially for months before invasive spread. Speed of spread is directly related to Breslow thickness (depth of invasion).
5. What is the survival rate for melanoma in 2026?
When detected early (Stage I), the five-year survival rate is approximately 99%. At Stage IV (metastatic), it drops to around 35% with standard treatment — though new immunotherapy combinations are showing 55%+ survival at 6.5 years in clinical trials.
6. Is basal cell carcinoma dangerous?
BCC is rarely life-threatening when treated early. However, if left untreated for years, it can grow large, destroy surrounding tissue, and in rare cases spread to lymph nodes. Early treatment carries a cure rate of nearly 100%.
7. What is the ABCDE rule for melanoma?
ABCDE stands for Asymmetry, Border irregularity, Color variation, Diameter greater than 6mm, and Evolving (changing over time). Any lesion meeting one or more of these criteria should be evaluated by a dermatologist.
8. Can dark-skinned people get melanoma?
Yes. While the incidence is lower in people with darker skin tones, melanoma in these individuals is often diagnosed later and in more dangerous locations — under nails, on palms, and on soles of feet. Black patients have a significantly lower five-year survival rate (70%) compared to White patients (95%), primarily due to late diagnosis.
9. What is the deadliest type of skin cancer?
Melanoma is the deadliest common skin cancer. It accounts for only about 1% of skin cancer cases but causes the overwhelming majority of skin cancer deaths in the United States.
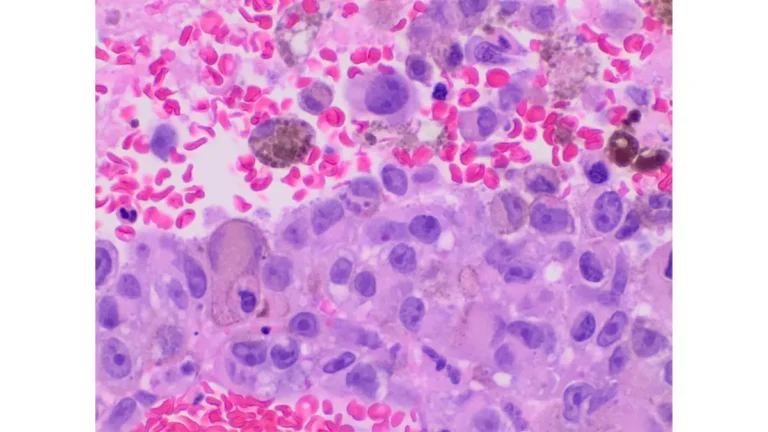
10. How is melanoma diagnosed?
Diagnosis begins with a clinical skin examination using dermoscopy. Any suspicious lesion is removed by excisional biopsy and examined by a pathologist. Staging involves Breslow thickness measurement, sentinel lymph node biopsy, and imaging for advanced cases.
11. Can melanoma be cured if caught early?
Yes. When melanoma is detected at Stage I, the five-year survival rate exceeds 99%. Early detection through regular self-exams and annual dermatologist visits is the single most effective strategy for surviving melanoma.
📌 Related Reading:
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.