On This Page – Quick Medical Summary
If you have a colonoscopy scheduled, the question on most people’s minds is simple: which of my usual medicines do I stop, and when? The reassuring answer is that most medications are continued — only a short, specific list needs adjusting.
This guide routes you to your situation. If you take a blood thinner like warfarin or Eliquis, start with the anticoagulant section. If you have diabetes and take insulin, an SGLT2 drug, or a GLP-1 medication such as Ozempic, the diabetes section is for you. If you take daily supplements like iron, fish oil, or fiber, see the supplements section. Caregivers can jump to the timing table and red-flag list near the end.
One rule sits above the rest and never changes: do not stop any prescribed medicine on your own. The clinician who prescribed each drug, with the team performing your colonoscopy, makes the final call on what to pause and when. For diet, cost, and results, see our complete colonoscopy prep guide.
ℹ️ Medical Disclaimer: This article is general health education, not medical advice. Decisions to stop, adjust, or continue any drug — including blood thinners, diabetes medications, and supplements — must be made with the clinician who prescribed it and the team performing your colonoscopy. If you have a recent heart stent, mechanical heart valve, recent blood clot, or insulin-dependent diabetes, contact them as early as possible, and seek urgent care for any concerning symptoms.
Why some medications are stopped before a colonoscopy
A colonoscopy is usually straightforward, but three things about it explain why a few medicines get paused.
Bleeding risk if a polyp is removed
Your gastroenterologist may remove a polyp — a small growth — or take a biopsy. A diagnostic colonoscopy, even with a biopsy, carries a low bleeding risk, but removing a polyp (a polypectomy) is a higher-bleeding-risk step. That is why blood-thinning medicines get the most attention.
Keeping the colon lining visible
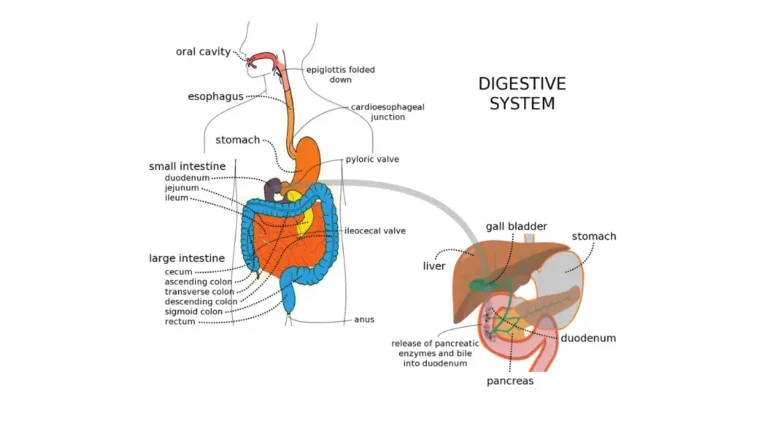
🔬 How It Works: Your doctor can only spot polyps if the colon lining (the mucosa) is clean and visible. Iron darkens stool and coats the lining, and undigested fiber leaves debris — clearing both is the purpose of bowel prep.
Staying safe under sedation and fasting
Prep means fasting and clear liquids for a day or more, which changes how some drugs behave. Diabetes medicines that lower blood sugar can push it too low, and certain newer drugs raise other risks under sedation. See our guide on how to prepare for a colonoscopy; the MedlinePlus colonoscopy overview also notes you may need to stop some medicines.
Blood thinners and antiplatelet medications
If you take a medicine that affects clotting, this is the most important section to discuss with your prescriber. The principle is a balance: the small risk of bleeding if a polyp is removed, weighed against the risk of a clot if you stop the drug.
⚠️ Clinical Warning: Never stop an anticoagulant or antiplatelet medicine on your own, especially with a recent heart stent, mechanical heart valve, or history of stroke or clots — stopping at the wrong time can trigger a dangerous clot. Your prescriber sets the timing and may keep the drug going if your clot risk is high.
Warfarin and DOACs (Eliquis, Xarelto, Pradaxa, Savaysa)
For a low-risk diagnostic colonoscopy, these are sometimes continued. When a polyp removal is likely, the prescriber may pause them for a drug-specific window, and some higher-clot-risk patients are “bridged” with another medicine. Many centers ask you to call one to two weeks ahead so there is time to plan.
Clopidogrel (Plavix) and other antiplatelets
Drugs like clopidogrel are often held for several days before a procedure where bleeding is more likely, but this decision frequently involves your cardiologist — particularly with a recent stent.
Low-dose aspirin: usually continued
The reassuring part for many readers: low-dose aspirin taken for the heart usually does not need to be stopped for a colonoscopy. Still, do not stop cardiac aspirin without asking the clinician who prescribed it.
✅ Patient Action: Ask the clinician who prescribed your blood thinner — and your cardiologist if you have a stent, mechanical valve, or recent clot: “Given my procedure and clot risk, do I continue, hold, or bridge this medication, and on which day?”
Diabetes medications, including Ozempic and SGLT2 drugs
Fasting for prep changes how diabetes medications work. The right adjustments depend on which drugs you take and your blood sugar pattern, so your diabetes prescriber and the endoscopy team set the specifics.
Insulin, sulfonylureas, and metformin on prep day
Because you are eating little or nothing, doses that lower blood sugar are commonly reduced or held to prevent hypoglycemia (low blood sugar). A frequent pattern is a reduced dose the evening before and holding oral pills the procedure morning, while checking your blood sugar. These are general patterns, not instructions for your regimen — your prescriber sets your exact doses.
SGLT2 inhibitors (Jardiance, Farxiga, Invokana)
📊 Clinical Data Point: The FDA advises stopping canagliflozin, dapagliflozin, and empagliflozin at least 3 days before scheduled surgery, and ertugliflozin at least 4 days before, to lower the risk of ketoacidosis — Source: FDA, SGLT2 inhibitor labeling change. Because prep involves prolonged fasting, many endoscopy units apply a similar window; confirm yours.
🔬 How It Works: SGLT2 inhibitors — the “-flozin” drugs — make the kidneys clear glucose through urine. During fasting or stress, that can tip the body into euglycemic ketoacidosis, a dangerous acid buildup that can occur even when blood sugar looks normal.
GLP-1 drugs (Ozempic, Wegovy, Mounjaro): what changed
The advice here has genuinely shifted, so older “always stop it a week before” guidance is now out of date. In 2023, anesthesiology guidance suggested holding these drugs because they slow stomach emptying, raising aspiration risk under sedation. In 2024, updated multisociety guidance moved to a risk-based, shared-decision approach — many patients can continue, and for a low-risk diagnostic colonoscopy in someone without symptoms, the clear-liquid prep may be enough.
✅ Patient Action: Ask your diabetes prescriber and the endoscopy or anesthesia team: “How should I adjust my insulin or pills during prep, and do I need to hold my SGLT2 or GLP-1 medication — for how many days?”
Supplements and over-the-counter medications
The medicines easiest to forget are the ones you buy without a prescription. Several quietly affect either bleeding or how clearly your doctor can see the colon.
Iron supplements and multivitamins
Most centers ask you to stop iron supplements about 5 to 7 days before a colonoscopy, because iron darkens stool and coats the colon lining, hiding polyps from view. Plain multivitamins can usually be continued, but stop any that contain iron.
Fiber supplements, fish oil, and NSAIDs
Fiber and oil supplements such as fish oil are typically stopped about 4 to 7 days before, since fiber leaves residue and omega-3 oils can affect bleeding. NSAID pain relievers like ibuprofen and naproxen can often be continued, though some centers stop them several days before a higher-bleeding-risk procedure — little harm comes from pausing them aside from more aches. Pair this with our guide on what to eat before a colonoscopy, since dietary fiber matters too.
Anti-diarrheal medicines (Imodium)
Stop anti-diarrheal medicines like loperamide (Imodium) about 7 days before, because they slow the gut and work against the bowel prep.
🩺 Physician Note: A common point of confusion is treating “all supplements” the same. Prescribed iron for anemia differs from an optional multivitamin — if a clinician recommended a supplement, confirm timing with them rather than stopping it.
Colonoscopy medication timing at a glance
Use this table to draft your personal list — then confirm every line with your prescriber and the endoscopy unit, because your instructions override any general guide.
This table is a general reference, not personal medical instructions. Your endoscopy unit’s written instructions always take priority.
| Medication group | Typical stop-before window | Why | Key clinical detail |
|---|---|---|---|
| Anticoagulants / antiplatelets (warfarin, DOACs, clopidogrel) | Individualized; set by prescriber | Bleeding risk if a polyp is removed, vs. clot risk | Never stop on your own; cardiologist often involved |
| Low-dose aspirin (cardiac) | Usually continue | Continuing is generally safe for colonoscopy | Don’t stop without asking the prescriber |
| SGLT2 inhibitors (“-flozin” drugs) | At least 3 days (ertugliflozin 4) | Ketoacidosis risk during fasting | FDA labeling figure; confirm with your team |
| GLP-1 drugs (Ozempic, Wegovy, Mounjaro) | Risk-based; decide with care team | Slowed stomach emptying under sedation | Now individualized, not an automatic stop |
| Insulin / sulfonylureas | Adjusted on prep day | Fasting can cause low blood sugar | Prescriber sets exact dosing |
| Iron supplements | About 5–7 days | Darkens stool, hides polyps | Plain multivitamins usually fine |
| Fiber + fish oil supplements | About 4–7 days | Residue and bleeding effects | Confirm if clinician-recommended |
| Anti-diarrheals (Imodium) | About 7 days | Work against bowel prep | Slow gut motility |
| Blood-pressure & maintenance meds | Usually continue | Needed daily; safe with prep | Small sip of water on the day |
Sources: ASGE antithrombotic guidance (2016); FDA SGLT2 inhibitor labeling; AGA and multisociety GLP-1 guidance (2023–2024); MedlinePlus; and UCLA Health, VA, Boston Medical Center, and Penn Medicine prep protocols. Windows are typical ranges; your unit’s instructions take priority.
For more pointers, see our colonoscopy prep tips and bowel prep options.
What to keep taking and when to call your doctor
After all the “stop” rules, here is the relief: most of your regular medicines stay exactly as they are.
Medicines you usually keep taking
Blood-pressure, thyroid, seizure, and most other daily maintenance medicines are normally continued right up to the procedure. On the morning of your colonoscopy, you can usually take them with a small sip of water a couple of hours beforehand — your unit will confirm the timing.
Situations that need a call before you change anything
A few situations deserve an early phone call rather than wait-and-see:
- A recent heart stent, acute coronary syndrome, or mechanical heart valve — do not stop antithrombotic drugs without cardiology input, and the procedure may be rescheduled.
- A recent blood clot (deep vein thrombosis or pulmonary embolism) while on anticoagulation.
- Insulin-dependent or hard-to-control diabetes, where prep-day dosing should be planned in advance.
✅ Patient Action: If any of these apply, call both the prescribing clinician and the endoscopy unit as soon as you are scheduled — ideally one to two weeks ahead — and ask exactly how to handle each medicine.
Frequently asked questions about medications before a colonoscopy
1. What medications should I stop before a colonoscopy?
The medications most often paused before a colonoscopy are blood thinners and antiplatelets, certain diabetes drugs (SGLT2 and sometimes GLP-1 medicines), iron supplements, fiber and fish oil supplements, and anti-diarrheals. Most other daily medicines continue. Follow your endoscopy unit’s written list and confirm each medicine with your prescriber.
2. How many days before a colonoscopy do I stop blood thinners?
There is no single number — timing depends on the drug, why you take it, and your clot risk, so your prescriber sets it. Some blood thinners continue for a diagnostic colonoscopy; others pause for a drug-specific window. Never stop one on your own.
3. Can I take my blood pressure medication before a colonoscopy?
Yes, blood-pressure medicines are usually continued before a colonoscopy. On the procedure morning, you can typically take them with a small sip of water a couple of hours beforehand. Your endoscopy unit confirms the exact timing, so follow your prep sheet.
4. Do I stop Ozempic or Wegovy before a colonoscopy?
Not automatically. Guidance shifted in 2024 toward a risk-based, shared decision rather than every patient stopping these GLP-1 drugs. For a low-risk colonoscopy without symptoms, the clear-liquid prep may suffice. Decide with your diabetes prescriber and the endoscopy team.
5. When do I stop iron supplements before a colonoscopy?
Most centers ask you to stop iron supplements about 5 to 7 days before a colonoscopy, because iron darkens stool and coats the colon lining, hiding polyps. Plain multivitamins usually continue, but stop iron-containing ones. If iron was prescribed for anemia, confirm timing with your prescriber.
6. Should I stop aspirin before a colonoscopy?
Low-dose aspirin taken for the heart usually does not need to be stopped before a colonoscopy, and continuing it is generally considered safe. Do not stop cardiac aspirin on your own, though — ask the clinician who prescribed it whether to continue.
7. What about diabetes pills and insulin on the day of prep?
Because fasting can lower blood sugar, insulin and many diabetes pills are commonly reduced or held during prep — often a reduced dose the evening before and holding oral pills the procedure morning, with blood-sugar checks. Your prescriber sets your exact doses.
8. Can I take ibuprofen before a colonoscopy?
Often, yes — NSAID pain relievers like ibuprofen can usually be continued for a colonoscopy. Some centers stop them several days before if a polyp removal is likely, since they affect bleeding; acetaminophen is an alternative. Check your prep sheet if unsure.
9. Do I stop fish oil or fiber supplements before a colonoscopy?
Fiber supplements and fish oil are typically stopped about 4 to 7 days before a colonoscopy — fiber leaves residue that blurs the view, and fish oil can affect bleeding. Pausing these is usually low-risk, but confirm timing if a clinician recommended them.
10. What medications can I keep taking before a colonoscopy?
Most daily maintenance medicines — blood-pressure, thyroid, and seizure medicines — are usually continued before a colonoscopy, along with low-dose cardiac aspirin and plain multivitamins. On the day, take them with a small sip of water beforehand. Your prep sheet lists what to continue.
11. What if I forgot to stop a medication before my colonoscopy?
Call your endoscopy unit as soon as you realize. Do not assume the procedure is canceled — the team decides whether to proceed or reschedule, based on the medicine and timing. Have your medication list ready when you call.
Putting your colonoscopy medication plan together
Most of your medicines will stay the same — the work is in handling the short list that doesn’t. Use the timing table to draft your personal stop-list, then confirm every item on your pre-procedure call so nothing is missed. The one rule that never changes: don’t stop a prescribed medicine on your own.
A colonoscopy is one of the most effective colorectal cancer screening tests available, and the CDC recommends screening for adults ages 45 to 75. If you are weighing your options or your risk, you can assess your colorectal cancer risk or review what your colonoscopy results mean once the test is done.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.