On This Page – Quick Medical Summary
Being told you have localized prostate cancer and then asked to choose between surgery and radiation is one of the hardest decisions a person can face — both sound serious, and most people have no training to weigh them. That fear is normal. This guide explains how the choice between prostate cancer surgery vs. radiation actually works.
Start with where you are:
- Newly diagnosed and choosing your treatment: the survival and side-effect sections are written for your decision.
- A spouse, partner, or caregiver researching: the comparison table and question checklist will help most.
- Preparing for specialist appointments: jump to how doctors decide and what to ask.
The most reassuring fact belongs first. For cancer still confined to the prostate, long-term survival is nearly the same whether you choose radical prostatectomy (surgery) or radiation therapy. This is not a gamble with your life — it is a decision about which trade-offs fit your body and priorities. If you are still getting oriented, our overview of prostate cancer signs, stages, and treatment covers the fundamentals.
ℹ️ Medical Disclaimer: This article is educational and does not diagnose your condition or recommend treatment for your case. Decisions about prostate cancer surgery, radiation, medication, active surveillance, or insurance coverage belong with a board-certified urologist and radiation oncologist who can review your pathology and health. Seek urgent care for inability to pass urine, heavy bleeding, or fever after any procedure.
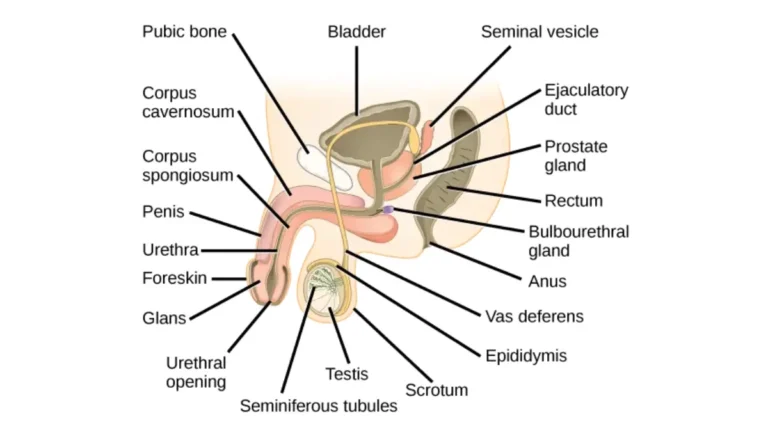
What surgery and radiation actually do
Surgery and radiation cure prostate cancer through different mechanisms, and that difference makes the rest of the decision clearer.
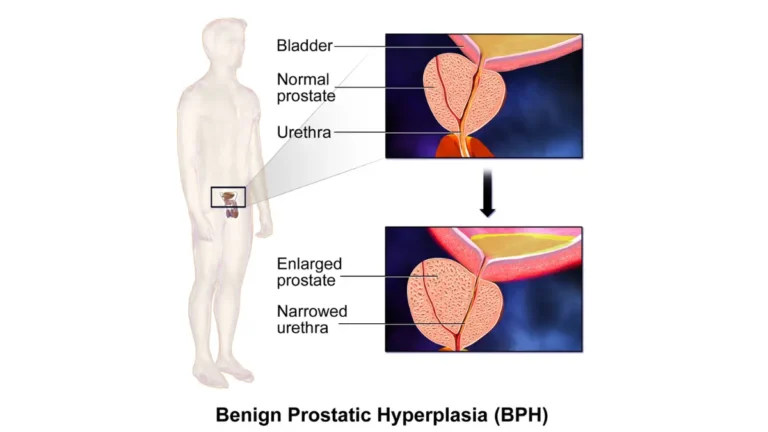
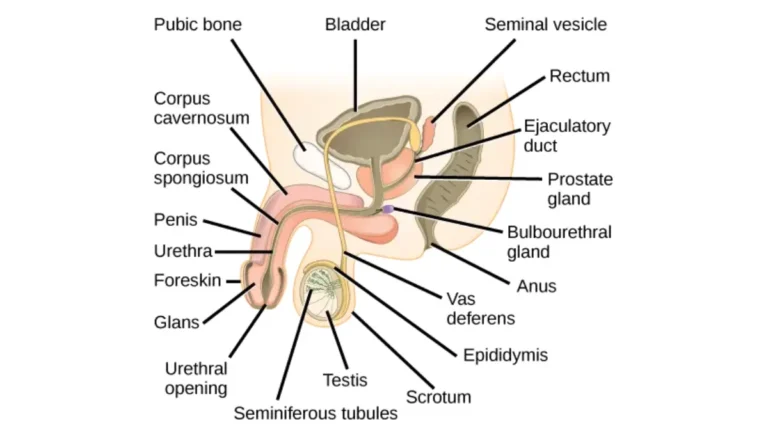
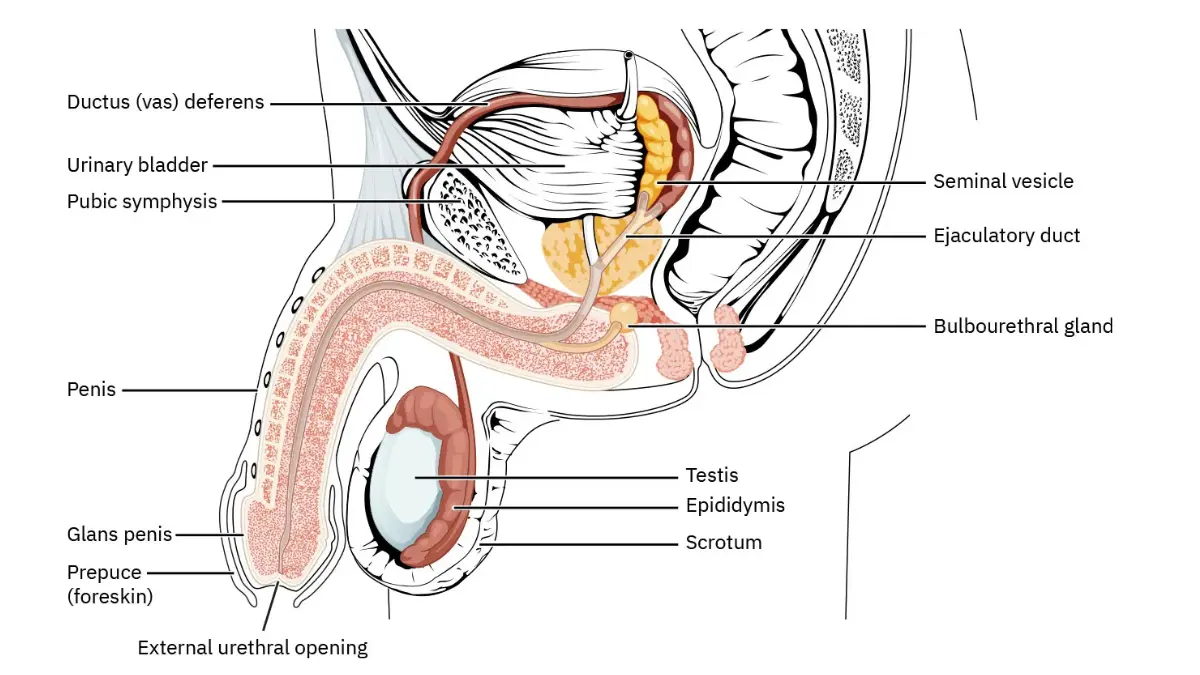
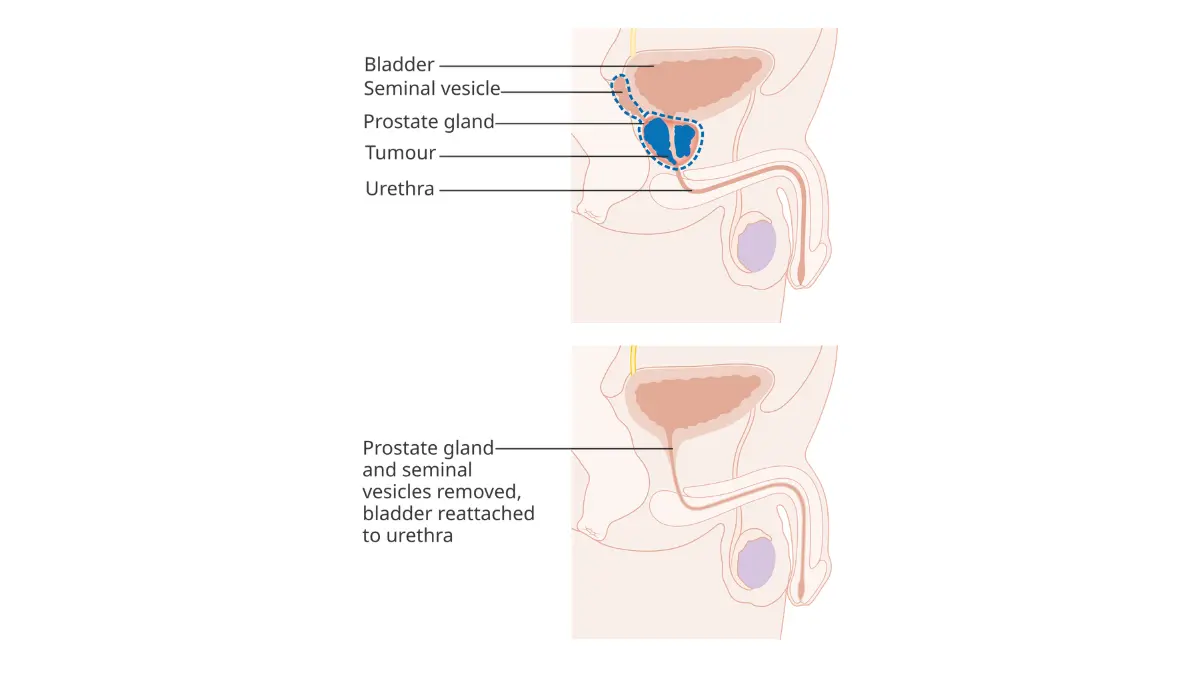
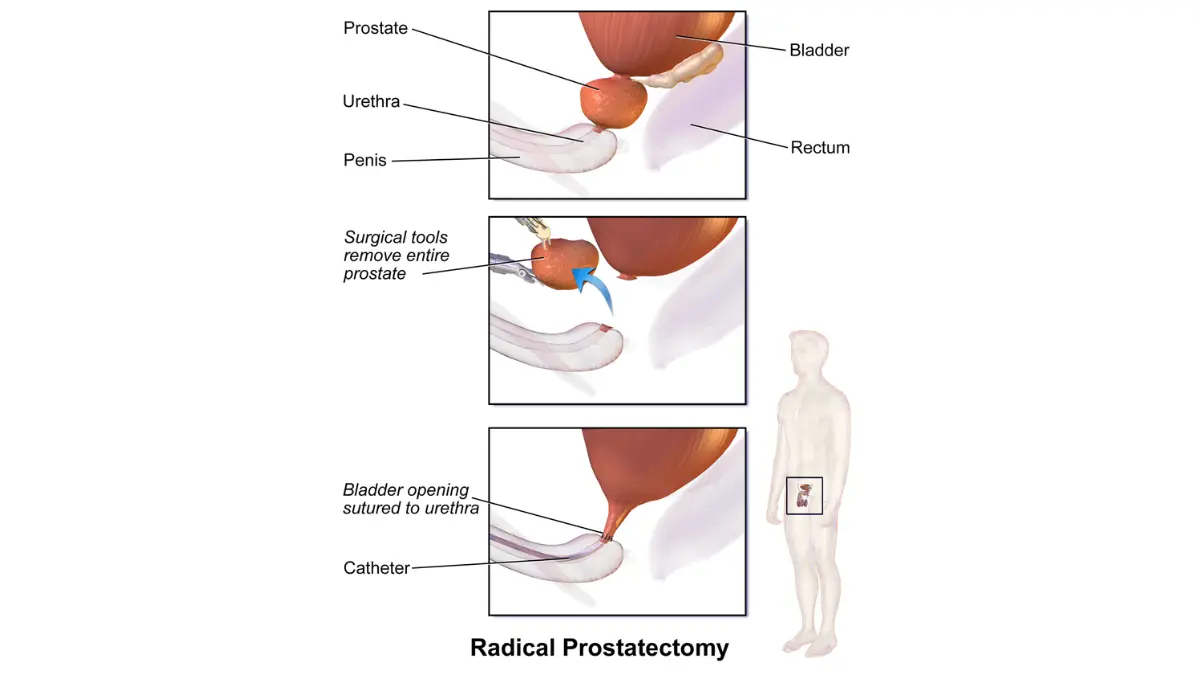
Radical prostatectomy: removing the prostate
A radical prostatectomy removes the entire prostate gland and the cancer inside it. Most are now done with robotic assistance through small incisions, though open surgery is still used. When the cancer’s location allows, surgeons attempt a nerve-sparing technique to preserve the nerves responsible for erections.
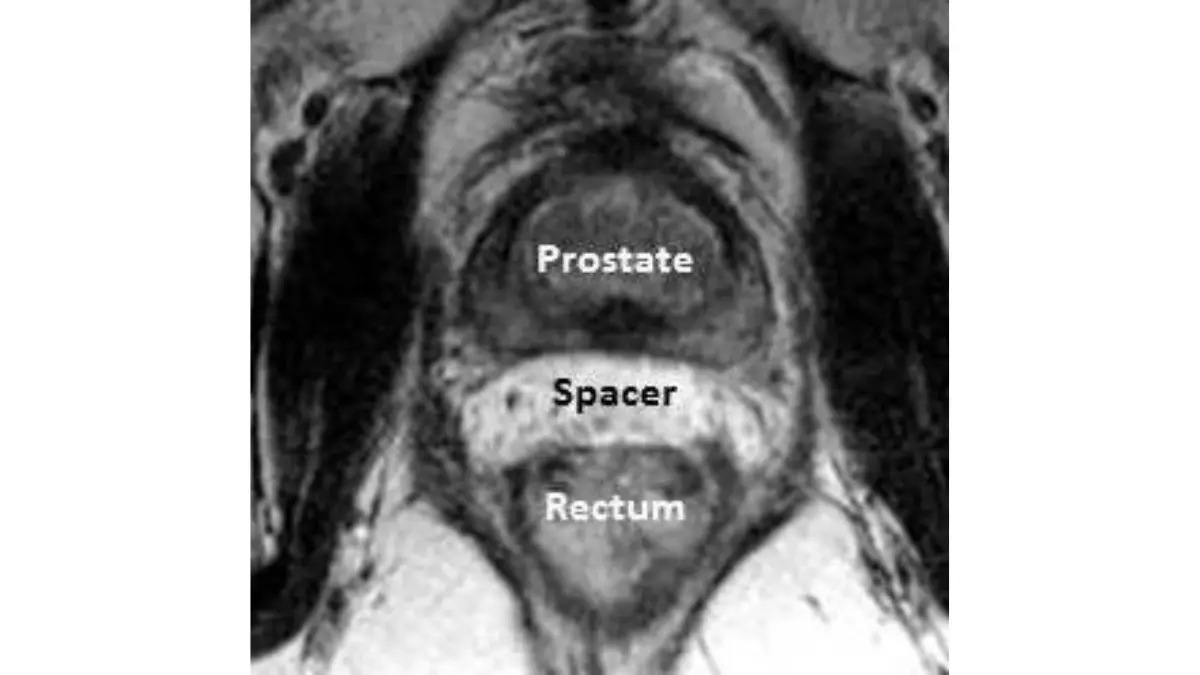
Radiation therapy: destroying cancer cells in place
Radiation therapy leaves the prostate in place and uses targeted radiation to damage cancer cells so they can no longer multiply. It comes in two main forms: external beam radiation, delivered from a machine over several weeks, and brachytherapy, in which radioactive seeds are placed inside the prostate.
🔬 How It Works: Surgery removes the organ that contains the cancer. Radiation damages the DNA inside cancer cells — they survive at first but die when they try to divide, which is why radiation’s full effect, and some side effects, appear gradually rather than at once.
The American Cancer Society’s overview of how prostate cancer is treated covers each option in more depth.
Does surgery or radiation give better survival?
For cancer confined to the prostate, long-term survival is nearly identical between surgery and radiation — the choice does not meaningfully change your odds of surviving the disease.
The strongest evidence is the ProtecT trial, which randomly assigned 1,643 men with localized prostate cancer to active monitoring, surgery, or radiation and followed them for a median of 15 years (New England Journal of Medicine, 2023).
📊 Clinical Data Point: At 15 years, prostate-cancer-specific survival was 97.2% after surgery and 97.7% after radiation, with no statistically significant difference between them (active monitoring was 96.6%). — Source: ProtecT trial, New England Journal of Medicine, 2023.
The chance of cancer spreading was also similar: about 4.7% after surgery and 5.0% after radiation by 15 years.
One caveat matters: most men in ProtecT had lower- or intermediate-risk cancer, so these findings apply most directly to that group rather than to high-risk disease.
✅ Patient Action: If your cancer is high-risk or higher-grade, ask your oncologist how the ProtecT survival data applies to your risk category, since the trial enrolled mostly lower-risk patients.
Surgery vs. radiation side effects: the real trade-off
Because survival is so similar, the decision usually comes down to side effects — and surgery and radiation affect different parts of the body.
In broad terms, radical prostatectomy tends to cause more urinary incontinence and erectile dysfunction, especially in the first months, while radiation therapy tends to cause more bowel problems that emerge later. The ProtecT trial measured these through patients’ own reports.
| Function | After surgery | After radiation | Key clinical detail |
|---|---|---|---|
| Urinary leakage | More common, often early, with partial recovery | Less common | Surgery’s urinary effects appear early; radiation’s build slowly |
| Erections | More affected early; ~17% firm enough for sex at 6 years | Less affected early; ~27% at 6 years | Both decline over years; the gap narrows |
| Bowel function | Rarely affected | Bloody stools (~5.6%) and fecal incontinence (~9.9%) at 6 years | Bowel problems are largely radiation-specific |
Source: patient-reported outcomes from the ProtecT trial (New England Journal of Medicine).
For the surgical side, our guide to what recovery after prostate surgery involves covers continence and healing; for the other path, see how prostate radiation is delivered.
✅ Patient Action: Before deciding, tell both specialists about your current urinary, sexual, and bowel function — your starting point strongly shapes which side effects you will notice most.
You can review the full data in the published ProtecT patient-reported outcomes study.
How your risk group and health shape the choice
Doctors don’t choose between surgery and radiation at random — they weigh a consistent set of factors, and seeing them helps you understand the recommendation.
The main considerations are:
- Your risk group — how aggressive the cancer looks, from your PSA, Grade Group or Gleason score, and stage.
- Your life expectancy and age — how many years of benefit a treatment can realistically provide.
- Your overall health — conditions that make surgery or anesthesia riskier.
- Your baseline function — your current urinary, sexual, and bowel health.
- Your personal priorities — which side effects you would least want to live with.
🩺 Physician Note: Current NCCN guidelines recommend active surveillance as the preferred option for very-low- and low-risk cancer when life expectancy is 10 years or more — so many men may not need surgery or radiation right away. For unfavorable intermediate-risk disease, both surgery and radiation are recommended.
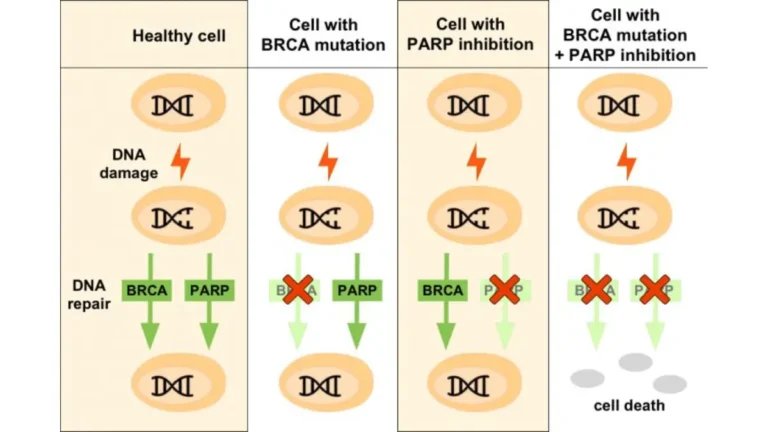
Broadly, younger, healthier men with longer life expectancy often lean surgical, partly for the pathology detail and flexibility afterward; older men or those with other serious health problems often lean toward radiation, which avoids an operation. Inherited risk matters too — a mutation such as BRCA2 may favor earlier treatment, and our hereditary risk assessment tool explains the factors.
✅ Patient Action: Ask for your exact risk group and an estimate of your life expectancy, and how each shapes your options — those two figures drive much of the recommendation.
The National Cancer Institute’s treatment-options summary for prostate cancer lays out the choices by stage.
Questions to ask before you choose
The most useful thing you can do is turn this information into a focused conversation with both specialists.
Before your surgery consult
Ask a urologist:
- What is my exact risk group, and why is surgery a good fit for it?
- How likely is nerve-sparing for me, and what are my expected continence and erection outcomes?
- If surgery shows the cancer is more advanced than expected, what happens next?
Before your radiation consult
Ask a radiation oncologist:
- Which type of radiation do you recommend for me, and why?
- What are my expected urinary and bowel side effects, and when might they appear?
- Will I also need hormone therapy, and for how long?
Why see both
Meeting both a urologist and a radiation oncologist before deciding is standard — each explains their option honestly, and the contrast helps you choose. A printable checklist of these questions is available to download for your appointments.
When the obvious choice may not be right
A few situations change the usual trade-offs, and knowing them protects you from a decision you might later regret.
When one option may not fit
Significant other health conditions can make surgery and anesthesia riskier, tilting the balance toward radiation. Certain bowel conditions or prior pelvic radiation can make radiation less suitable. High-risk cancer often calls for combined treatment — for example, radiation paired with hormone therapy — rather than one approach.
Salvage options if treatment doesn’t work
The two paths differ in what comes next if the cancer returns. Radiation after surgery (salvage radiation) is a well-established second option. Surgery after radiation is technically harder and less common — a real factor some men weigh.
⚠️ Clinical Warning: Do not assume a treatment can simply be repeated or reversed if it fails. The availability and difficulty of follow-up treatment differs by which option you choose first, so ask about it before you decide.
✅ Patient Action: Ask both specialists whether anything in your health history makes one option higher-risk for you, and what your salvage options would be if the first treatment does not fully work.
Frequently asked questions
1. Is surgery or radiation better for prostate cancer?
For localized prostate cancer, neither is clearly better for survival — the ProtecT trial found nearly identical 15-year survival for both. The right choice depends on your risk group, health, and which side effects you most want to avoid. Discuss both with a urologist and radiation oncologist.
2. Does surgery or radiation have fewer side effects?
Neither has fewer overall — they have different ones. Surgery more often causes urinary leakage and erectile dysfunction, especially early. Radiation more often causes bowel problems that appear later. Your starting urinary, sexual, and bowel function shapes which matters most.
3. How do doctors decide between surgery and radiation?
Doctors weigh five factors: risk group, life expectancy and age, overall health, baseline urinary and sexual function, and your priorities about side effects. Guidelines and shared decision-making guide the choice. Ask your specialist how each applies to you.
4. Is prostate removal surgery worth it?
Surgery can be worth it, especially for younger, healthy men with longer life expectancy, since it removes the cancer and gives detailed pathology. But it carries real risks of incontinence and erectile dysfunction. Whether it fits you depends on your risk group and priorities — discuss it with a urologist.
5. Can you have radiation after prostate surgery?
Yes. Radiation after surgery (salvage radiation) is well established if cancer returns or was not fully removed. This flexibility is one reason some men choose surgery first. Ask your urologist how salvage radiation would work for you.
6. Can you have surgery after radiation fails?
It is possible but uncommon. Surgery after radiation (salvage prostatectomy) is technically harder, with higher complication rates, because radiation changes the tissue. This difference is worth weighing before you choose. Ask both specialists about your salvage options with each path.
7. Which is better for older men, surgery or radiation?
Older men, or those with other health conditions, often lean toward radiation because it avoids surgery and anesthesia. For some, active surveillance fits better instead. There is no fixed age cutoff — life expectancy and overall health matter more than age. Discuss this with your specialist.
8. Does radiation cause erectile dysfunction like surgery?
Radiation can cause erectile dysfunction, but less often than surgery in the early years — in the ProtecT trial, more men kept erections firm enough for sex after radiation at six years. Over many years, rates rise in both groups and the gap narrows.
9. How long is recovery for prostate surgery versus radiation?
Surgery means a hospital stay and several weeks of recovery, with a catheter at first and gradual return of continence. Radiation needs no surgery but runs over several weeks of sessions, with side effects building over time. Our prostate surgery cost and recovery guide covers timelines.
10. Will I be incontinent after radiation?
Urinary incontinence is less common after radiation than after surgery, though radiation can cause urinary urgency and irritation that build over time. Most men do not become severely incontinent from radiation alone. Ask your radiation oncologist about your expected urinary side effects.
11. Should I get a second opinion before choosing?
Yes — seeing both a urologist and a radiation oncologist is standard before deciding, not a sign of distrust. Each explains their option honestly, and comparing them helps you choose with confidence. Bring your pathology report and a written list of questions.
Making your decision with confidence
The hardest part of this diagnosis is often feeling you must gamble with your life. The reassurance is real: for localized prostate cancer, surgery and radiation lead to nearly the same long-term survival. What differs is the side-effect trade-off, which you can weigh against your own life and values.
The single most useful next step is to meet with both a urologist and a radiation oncologist, bring your questions, and choose the path that fits you. For a plain-language overview to share with family, see MedlinePlus’s prostate cancer resource.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.