On This Page – Quick Medical Summary
Seeing a value flagged “low” or “high” on a prenatal blood test can be frightening, especially when every result feels tied to your baby’s wellbeing. Here is the reassuring part: pregnancy changes your blood on purpose, so your complete blood count is read against pregnancy-specific ranges, not the standard adult ones.
Use this guide by your situation. If your flagged value is a low hemoglobin or hematocrit, the section on dilution versus true anemia is written for you. If it is a low platelet count, skip ahead to gestational thrombocytopenia. If it is a high white blood cell count, the section on why white cells rise will settle most worries. And if you only want to know which numbers actually warrant a call, that is covered near the end.
Most of these shifts are expected, and most reverse after delivery. If you want the bigger picture of the test itself, our guide to what a complete blood count actually measures and the National Library of Medicine’s overview of what a CBC test involves both help. Below are the trimester-by-trimester ranges and the specific values worth a conversation with your provider.
ℹ️ Medical Disclaimer: This article is educational. It does not diagnose anemia or any blood condition, interpret your specific results, or replace prenatal care. The reference ranges, anemia thresholds, iron guidance, and red-flag values described here are general information — your own results must be read in context by a board-certified obstetric provider (OB-GYN) or certified nurse-midwife, who may order iron studies or other tests before any treatment. Do not start, stop, or change iron or any medication based on this page.
Why your blood counts change when you’re pregnant
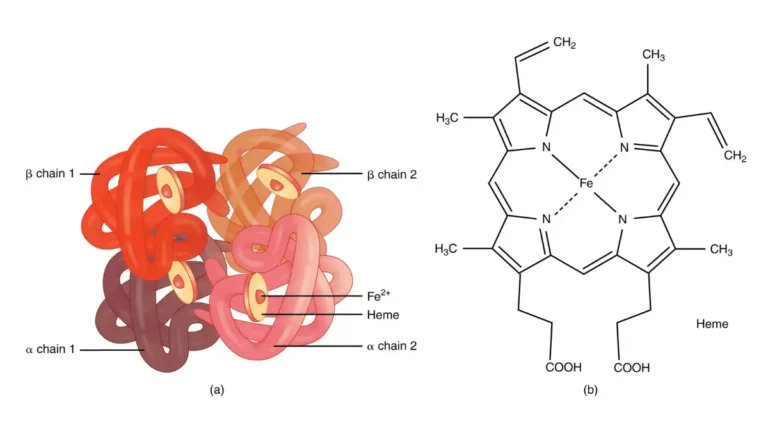
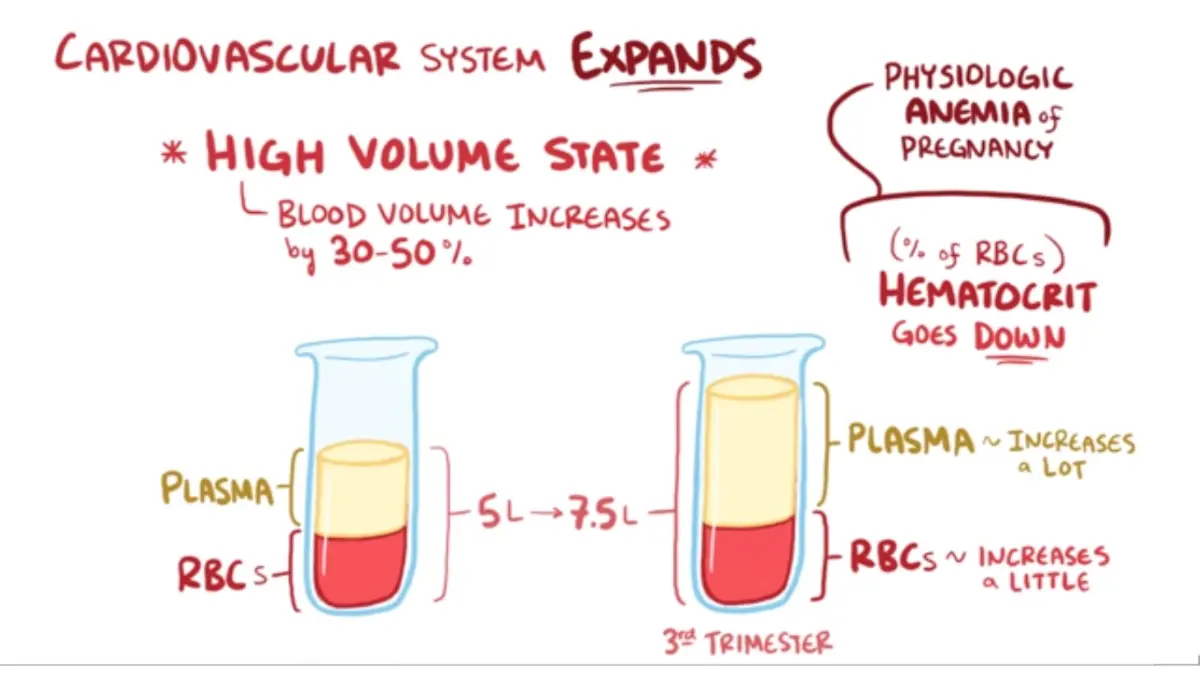
Almost every shift on a pregnancy CBC traces back to one change: your blood volume climbs, and the liquid part climbs faster than the cells. That single fact explains why hemoglobin, hematocrit, and platelets can all read lower without anything being wrong.
🔬 How It Works: During pregnancy your plasma volume — the fluid your blood cells float in — expands roughly 40% to 50%, while your red cell mass rises less, about 15% to 25%. More fluid dilutes the same red cells, so their measured concentration drops. This is hemodilution, and the mild fall it produces is the physiologic anemia of pregnancy, not blood loss.
Plasma rises faster than red cells
Your red cells are not disappearing; they are diluted. Because of that, a hemoglobin that would look low outside pregnancy can be entirely expected during it. Understanding how hematocrit and hemoglobin relate makes this easier, since both fall together for the same reason.
📊 Clinical Data Point: In pregnancy, plasma volume expands about 40–50% while red cell mass rises only about 15–25%, producing a physiologic dilutional anemia — Source: American Society of Hematology, 2023 Education Program (via NIH/PubMed Central).
Why the lowest readings usually land in the second trimester
Plasma expansion outpaces red-cell production most sharply in mid-pregnancy. So hemoglobin typically reaches its lowest point — its nadir — in the second trimester, then recovers somewhat in the third as red cell mass catches up.
CBC reference ranges by trimester
Normal pregnancy hemoglobin runs lower than the adult female range: roughly 11.3–14.3 g/dL in the first trimester, 10.1–13.3 in the second, and 10.1–14.1 in the third. The table sets the main CBC values against a typical non-pregnant range so you can locate your own result.
| CBC value | Non-pregnant (adult women) | First trimester | Second trimester | Third trimester |
|---|---|---|---|---|
| Hemoglobin (g/dL) | ~12.0–15.5 | 11.3–14.3 | 10.1–13.3 | 10.1–14.1 |
| Hematocrit (%) | ~35–45 | ~32–42 | ~30–40 | ~31–43 |
| White blood cells (×10⁹/L) | ~4.5–11.0 | 5.1–12.1 | 6.1–13.5 | 5.6–12.4 |
| Platelets (×10⁹/L) | 150–400 | 184–374 | 164–356 | 145–349 |
Source: trimester-specific reference intervals from a peer-reviewed pregnancy CBC study (reference intervals for CBC parameters in normal pregnancy, NIH/PubMed Central), corroborated by a second published dataset with matching hemoglobin, white-cell, and platelet bands. Hematocrit values are approximate and track hemoglobin. Reference ranges vary by laboratory, analyzer, altitude, and population — always compare against your own lab’s pregnancy ranges rather than the standard non-pregnant CBC chart.
Hemoglobin and hematocrit by trimester
Hematocrit falls in step with hemoglobin from the same dilution effect, which is why both often read low together. MCV, the average size of your red cells, changes very little in pregnancy — a small rise of a few femtoliters is normal and does not by itself signal a vitamin deficiency.
White blood cells and platelets by trimester
White cells rise across pregnancy, and platelets drift gently downward as the weeks pass. Both patterns are expected, and both are covered in the sections that follow.
📊 Clinical Data Point: In healthy pregnancy, platelet counts decline gradually, and the lower end of normal reaches about 145 ×10⁹/L by the third trimester — Source: peer-reviewed trimester reference-interval study (NIH/PubMed Central).
Physiologic dilution or real anemia? How the line is drawn
Anemia in pregnancy is defined by specific numbers. The CDC and ACOG set it at a hemoglobin below 11 g/dL (or hematocrit below 33%) in the first and third trimesters, and below 10.5 g/dL (hematocrit below 32%) in the second. Thresholds that once adjusted these cutoffs by race are no longer recommended, and the same standard now applies to everyone.
📊 Clinical Data Point: Anemia in pregnancy is hemoglobin <11 g/dL (Hct <33%) in the 1st and 3rd trimesters and <10.5 g/dL (Hct <32%) in the 2nd — Source: CDC and ACOG trimester-based definition (2021 ACOG Practice Bulletin; CDC), as summarized in the American Society of Hematology’s 2023 review.
The CDC/ACOG cutoffs that define anemia in pregnancy
Mild dilutional anemia — often a hemoglobin around 10 to 11 g/dL — is common and expected. The clinical task is telling that harmless dilution apart from iron deficiency, which is the most common cause of true anemia in pregnancy and affects roughly 18% of US pregnancies, rising across the trimesters. Reading what a low hemoglobin result means in more depth can help you prepare questions.
The clue that points to iron deficiency (and why ferritin matters)
Dilution lowers your hemoglobin but not the size of your red cells; iron deficiency shrinks them. So a low MCV on the same CBC, or a low ferritin — your iron-store marker — points toward iron deficiency rather than simple dilution. Learning how iron studies are interpreted shows what your provider is looking for.
🩺 Physician Note: Current guidance treats ferritin as the key marker of iron stores in pregnancy, with a level under about 30 ng/mL indicating deficiency. Because pregnancy alters the blood, clinicians often confirm with iron studies rather than relying on hemoglobin alone.
✅ Patient Action: If your prenatal hemoglobin is below the cutoff for your trimester, ask your OB-GYN or midwife: “Can we check iron studies including ferritin to tell whether this is dilution or iron deficiency?” You can read more about anemia in pregnancy from the National Library of Medicine before that visit.
Why your white blood cell count goes up
A higher white blood cell count in pregnancy is usually expected, not a sign of infection. Pregnancy drives a normal rise in white cells that continues through the third trimester and peaks around delivery.
🔬 How It Works: The rise is a physiologic leukocytosis driven mainly by neutrophils, the white cells that respond first to threats. Pregnancy hormones prolong neutrophil survival and the body’s mild inflammatory state increases their production, so the total count climbs as a normal adaptation — not because an infection is present.
Physiologic leukocytosis — driven by neutrophils
This is why a white cell count in the low-teens can be normal during pregnancy when it might prompt questions otherwise. The count climbs highest during labor and the first days afterward, then settles back over the following weeks.
📊 Clinical Data Point: The upper limit of normal for white cells is about 36% higher in pregnancy (roughly up to 15 ×10⁹/L), and counts can briefly reach 20,000–30,000/µL during labor and the immediate postpartum period — Source: large pregnancy white-cell reference-interval studies (NIH/PubMed Central).
When a high count could still mean infection
A high count paired with symptoms is different from a high count alone. If a raised white cell count comes with fever, pain, or feeling unwell, it still deserves evaluation — the number alone cannot rule infection in or out. A deeper look at what a high white blood cell count can signal covers the non-pregnancy causes too.
Platelets that drift down: gestational thrombocytopenia
A gently falling platelet count is one of the most common CBC changes in pregnancy, and in most cases it is harmless. Platelets often dip below the non-pregnant floor of 150 ×10⁹/L as pregnancy advances.
🔬 How It Works: The decline comes mostly from the same hemodilution that lowers hemoglobin, plus a modest increase in how quickly platelets are cleared from the blood. The drop is usually mild, and the absolute count stays within a safe range for most people.
What gestational thrombocytopenia is (and how common)
Gestational thrombocytopenia is a benign, pregnancy-related fall in platelets below 150 ×10⁹/L, and it needs no treatment in most cases. It accounts for the large majority of low platelet counts in pregnancy and resolves on its own within weeks of delivery. Seeing the full list of causes behind a low platelet count can put your result in context.
📊 Clinical Data Point: Gestational thrombocytopenia (platelets below 150 ×10⁹/L) occurs in roughly 5–11% of pregnancies and accounts for about 75% of all thrombocytopenia in pregnancy — Source: New England Journal of Medicine platelet-in-pregnancy study and StatPearls (NIH/PubMed Central).
The platelet levels that warrant a closer look
Not every low platelet count is gestational thrombocytopenia. Counts rarely fall below about 70 ×10⁹/L in this benign pattern, so lower readings are evaluated for other causes such as immune thrombocytopenia or a hypertensive disorder of pregnancy.
⚠️ Clinical Warning: A platelet count below about 100 ×10⁹/L, or one accompanied by a severe headache, vision changes, or upper-abdominal pain, is not assumed to be harmless. These can signal preeclampsia, HELLP syndrome, or immune thrombocytopenia and need prompt evaluation by your obstetric provider. Ask specifically: “Do my platelets need a work-up for preeclampsia or another cause?”
Which changes are routine and which mean call your provider
You can leave this page with a simple rule for reading your own result. Most of the shifts above are expected pregnancy physiology, and a short list of specific values or symptoms is what actually warrants a call.
Shifts that are usually just pregnancy:
- A hemoglobin or hematocrit that reads mildly low, especially around the second trimester, when dilution peaks.
- A white blood cell count that runs higher than the non-pregnant range without fever or other symptoms.
- A platelet count that dips modestly but stays above roughly 100 ×10⁹/L.
Values and symptoms worth a call to your provider:
- A hemoglobin below your trimester’s cutoff (11 g/dL in the first and third, 10.5 in the second), or symptoms of anemia such as marked fatigue, breathlessness, or dizziness.
- A platelet count below about 100 ×10⁹/L, or one with severe headache, vision changes, or upper-abdominal pain.
- A high white cell count together with fever, pain, or feeling unwell.
The reassuring bookend: most of these changes reverse after birth. Plasma volume begins falling within days of delivery and returns to non-pregnant levels by about six weeks, so hemoglobin and hematocrit climb back and gestational thrombocytopenia resolves within a few weeks.
Frequently asked questions about CBC ranges in pregnancy
1. What is a normal CBC in pregnancy?
A normal CBC in pregnancy looks different from the adult standard: hemoglobin, hematocrit, and platelets read lower while white blood cells read higher. Results are compared against trimester-specific pregnancy ranges rather than ordinary adult ranges, because these changes are expected physiology.
2. What hemoglobin level is too low in pregnancy?
The CDC and ACOG define anemia as a hemoglobin below 11 g/dL in the first and third trimesters and below 10.5 g/dL in the second. Below these cutoffs, ask your obstetric provider whether iron studies are needed to find the cause.
3. Is low hemoglobin in pregnancy dangerous?
A mild drop from dilution is normal and not dangerous. True anemia below the trimester cutoff is worth evaluating and treating, since iron-deficiency anemia is linked to poorer outcomes. Confirm the cause with your obstetric provider.
4. Why is my white blood cell count high in pregnancy?
Pregnancy causes a physiologic neutrophilic leukocytosis, so a high white blood cell count is usually a normal adaptation that peaks around labor. A high count alongside fever, pain, or feeling unwell still deserves evaluation for infection.
5. What platelet count is normal in pregnancy?
Platelets often dip below the non-pregnant floor of 150 ×10⁹/L, and a mild decline is usually gestational thrombocytopenia. A platelet count below about 100 ×10⁹/L should be evaluated by your provider.
6. What is gestational thrombocytopenia?
Gestational thrombocytopenia is a common, usually harmless drop in platelets below 150 ×10⁹/L during pregnancy. It affects roughly 5–11% of pregnancies, needs no treatment in most cases, and resolves within weeks after delivery.
7. Does hematocrit go down in pregnancy?
Yes. Hematocrit falls alongside hemoglobin because of the same hemodilution, typically reaching its lowest point in the second trimester before recovering somewhat in the third. It tracks your hemoglobin closely.
8. When in pregnancy is hemoglobin lowest?
Hemoglobin is usually lowest in the second trimester, when the expansion of plasma volume peaks relative to red cell mass. It typically rises again during the third trimester as red cell mass catches up.
9. How is anemia in pregnancy diagnosed?
Anemia is identified on a CBC, usually screened in the first trimester and again around 24–28 weeks. A low MCV or low ferritin points to iron deficiency, confirmed with iron studies. Ask your provider about testing.
10. Do CBC values return to normal after delivery?
Yes. Plasma volume falls within days of delivery and returns to non-pregnant levels by about six weeks, so hemoglobin and hematocrit climb back and gestational thrombocytopenia resolves within a few weeks.
11. What CBC changes mean I should call my provider?
Call your obstetric provider for a hemoglobin below your trimester’s cutoff, a platelet count below about 100 ×10⁹/L, or a high white blood cell count with fever, pain, or feeling unwell.
The bottom line
Your blood counts move during pregnancy because your body is doing exactly what it should — making more blood to support your baby. A flagged hemoglobin, platelet, or white cell value is common, and most of the time it reflects normal physiology rather than a problem.
The useful next step is simple: read your result against pregnancy ranges, not adult ones, and bring the specific values above to your prenatal visit. If a number crosses one of the lines here, message your provider before your next appointment. For a broader walkthrough of your results, see our guide to how to read your CBC results.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.