On This Page – Quick Medical Summary
What Do Your Urine Test Results Really Mean?
Marcus, a 41-year-old software engineer, stared at his lab report showing “WBC: 12/HPF” and “protein: 1+” with mounting anxiety. Like millions of Americans who receive confusing urine test results each year, he had no idea whether these numbers signaled a minor issue or a serious health crisis.
Here’s what you need to know right now: Your urine test results reveal how well your kidneys filter waste, whether infection is present, and if metabolic conditions like diabetes are developing. Most abnormal results don’t indicate serious disease—but understanding what those numbers mean can help you know when to seek immediate care versus simple follow-up.
This 2026 guide decodes every parameter on your urinalysis report using the latest AMA and WHO reference ranges, updated in January 2026 to reflect new research on kidney function across different populations.
Why Your Results Look Confusing (And What We’re Fixing)
Medical laboratories report urine test results using abbreviations and units most people have never encountered:
- HPF (high-power field) = microscopic viewing area
- mg/dL (milligrams per deciliter) = concentration measurement
- Specific gravity = urine density compared to water
- 1+ or 2+ = semi-quantitative protein levels
The confusion stems from laboratories using medical terminology designed for physicians, not patients. According to the CDC’s clinical laboratory standards, over 65% of patients misinterpret at least one value on their urinalysis results.
What this guide delivers:
✅ Plain-English translation of every test parameter
✅ 2026 updated normal ranges by age and gender
✅ Clear “worry now vs. watch” decision framework
✅ Real patient case examples (anonymized)
✅ Medication and diet factors affecting results
Understanding your numbers reduces anxiety and helps you have more productive conversations with your healthcare provider. Similar to how our blood sugar converter helps clarify glucose readings, this guide transforms confusing lab data into actionable health insights.
2026 Normal Urine Test Results Reference Chart
The American Medical Association (AMA) and World Health Organization (WHO) released updated urinalysis reference ranges in January 2026, incorporating new data from diverse populations and modern lifestyle factors.
Why Ranges Vary: Age, Pregnancy, and Medications
Normal urine values aren’t one-size-fits-all. Your age, hydration status, medications, and whether you’re pregnant significantly impact what’s considered “normal” for you specifically.
According to NIDDK research on kidney function, reference ranges must account for physiologic variation across life stages.
Complete 2026 Normal Range Table
| Test Parameter | Normal Range (Adults) | What It Measures | Red Flag Values |
|---|---|---|---|
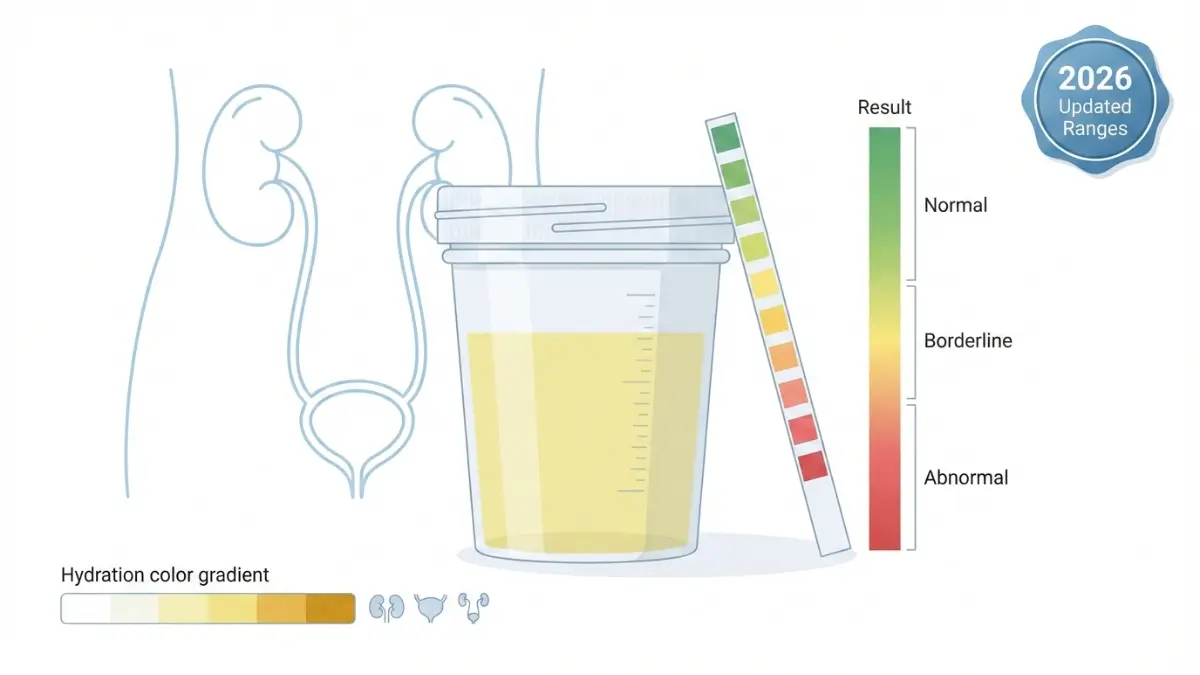
| Color | Pale yellow to amber | Hydration, liver function, bleeding | Dark brown, red/pink, orange |
| Clarity | Clear to slightly hazy | Infection, crystals, cells | Cloudy, turbid, murky |
| pH | 4.5-8.0 (optimal: 5.5-7.0) | Acid-base balance, diet, infection | <4.5 or >8.0 consistently |
| Specific Gravity | 1.005-1.030 | Kidney concentration ability | <1.003 or >1.035 |
| Protein | Negative (<10 mg/dL) | Kidney filtration integrity | 1+ (30 mg/dL) or higher |
| Glucose | Negative (<15 mg/dL) | Blood sugar control | Any positive (≥100 mg/dL) |
| Ketones | Negative | Fat metabolism, diabetic state | Moderate to large |
| Blood/RBC | 0-2 cells/HPF | Kidney stones, infection, trauma | >3 cells/HPF or visible blood |
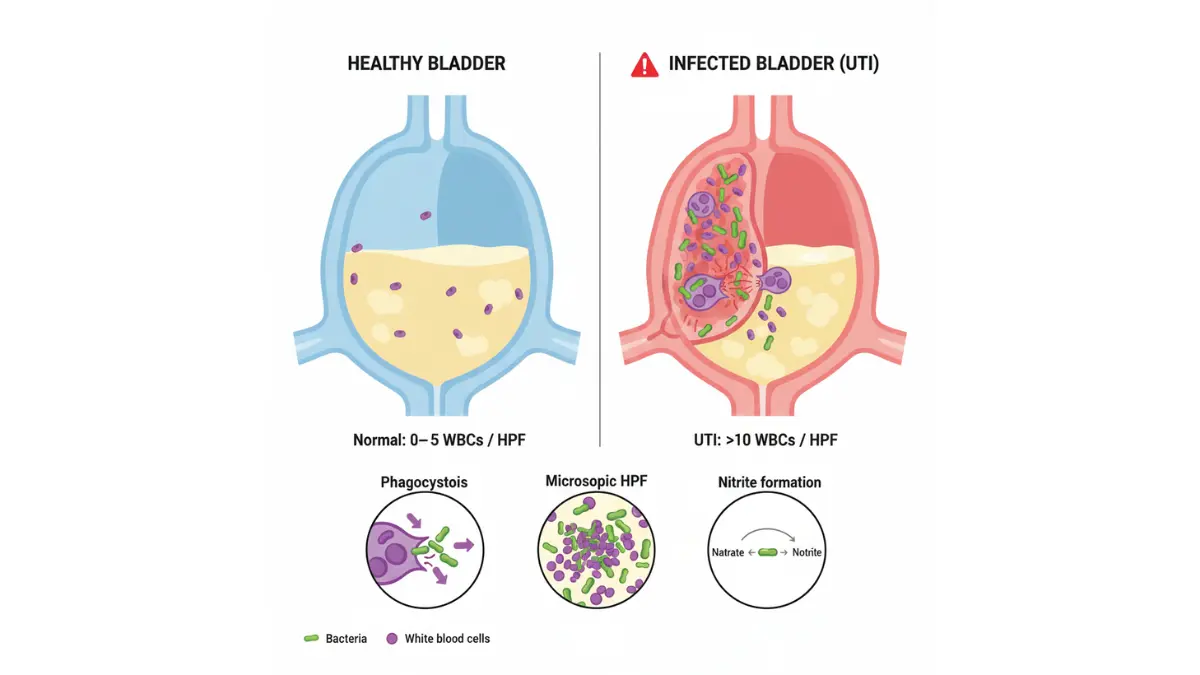
| WBC/Leukocytes | 0-5 cells/HPF | Infection, inflammation | >10 cells/HPF |
| Nitrites | Negative | Bacterial infection (UTI) | Positive |
| Bilirubin | Negative | Liver function, bile flow | Any positive |
| Urobilinogen | 0.1-1.0 mg/dL | Liver/hemolytic processes | >2.0 mg/dL |
| Epithelial Cells | Few (0-5/HPF) | Sample contamination | Numerous (>10/HPF) |
| Bacteria | None to rare | Infection risk | Moderate to many |
| Crystals | Occasional | Stone formation risk | Numerous specific types |
Source: American Medical Association 2026 Clinical Laboratory Standards
Age-Specific Normal Range Variations
Pediatric Ranges (Ages 2-12):
- WBC: 0-8/HPF (higher than adults due to immature immune systems)
- Specific gravity: 1.001-1.035 (wider range due to developing kidney concentration ability)
- Protein: Up to trace acceptable in very dilute urine
- pH: 5.0-7.0 (children’s diets affect this more than adults)
Adult Ranges (Ages 13-64):
- Standard ranges as listed in main table above
- Athletes may show temporary protein after intense exercise
Elderly Ranges (Ages 65+):
- Specific gravity: May trend lower (1.002-1.025) due to reduced kidney concentration
- Occasional epithelial cells more common
- Trace protein may be normal finding
- Kidney function naturally declines approximately 1% per year after age 40
Pregnancy-Specific Ranges (Updated 2026)
Pregnancy dramatically changes urinalysis normal values:
First Trimester (Weeks 1-13):
- Protein: Up to trace (30 mg/dL) acceptable
- Glucose: Slightly elevated threshold due to lowered renal glucose threshold
- Specific gravity: May be lower due to increased fluid intake
Second Trimester (Weeks 14-26):
- Protein: Up to 1+ may be normal if no other symptoms
- Glucose: Positive results require glucose tolerance testing
- Bacteria: Lower threshold for treatment (any bacteria = culture)
Third Trimester (Weeks 27-40):
- Protein: Closely monitored for preeclampsia (>2+ with high blood pressure = emergency)
- WBC: Up to 10/HPF may be acceptable
- Epithelial cells: More common due to vaginal contamination
Women can track pregnancy-related changes using our pregnancy due date calculator and pregnancy weight gain calculator.
What Changed in 2026 Clinical Guidelines
The January 2026 AMA update incorporated three major changes:
1. Protein Threshold for Diabetics
- Previous: >30 mg/dL considered abnormal
- 2026 Update: >15 mg/dL triggers microalbuminuria workup in diabetics
- Rationale: Earlier detection prevents diabetic kidney disease progression
2. Specific Gravity Interpretation
- Previous: Single range for all ages
- 2026 Update: Age-adjusted ranges (tighter for adults 20-50, wider for pediatric/elderly)
- Rationale: Reflects natural kidney concentration changes across lifespan
3. Ketone Levels for Low-Carb Dieters
- Previous: Any ketones flagged as abnormal
- 2026 Update: “Nutritional ketosis” category for non-diabetics (trace to small acceptable)
- Rationale: Popularity of ketogenic and low-carb diets (our keto calculator helps track macros for these diets)
These updates reflect modern understanding that one-size-fits-all reference ranges miss important clinical nuances in diverse patient populations.
Decoding Abnormal Results – What Each Number Means
Seeing “abnormal” on your urine test results doesn’t automatically mean disease. Many factors temporarily alter results, and understanding context is crucial.
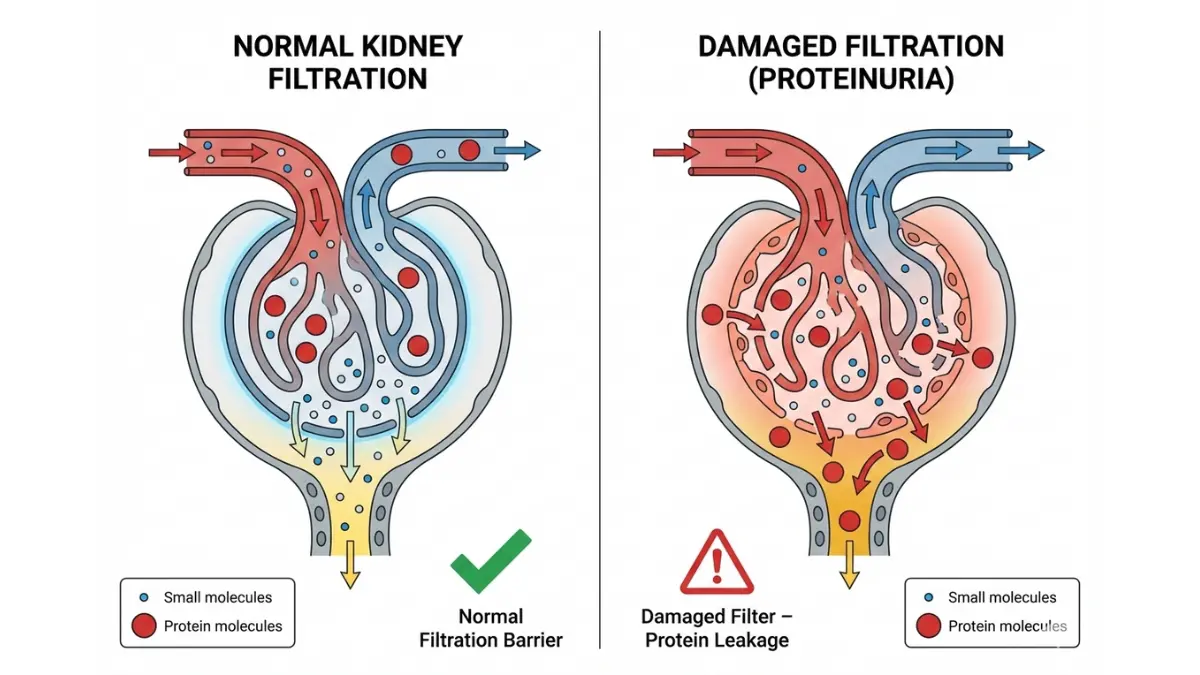
High Protein (Proteinuria): Causes & Action Steps
What elevated protein means:
Normally, your kidneys’ filtration system blocks large protein molecules from entering urine. Protein in urine signals the kidney filters (glomeruli) may be damaged or overworked.
Common causes of proteinuria:
Temporary/Benign (48-72 hours):
- Intense exercise (marathon running, weightlifting)
- Dehydration (concentrated urine)
- Fever or acute illness
- Prolonged standing (orthostatic proteinuria)
- Cold exposure
Chronic/Concerning:
- Diabetes-related kidney damage (diabetic nephropathy)
- High blood pressure damaging kidney blood vessels
- Preeclampsia during pregnancy
- Chronic kidney disease
- Autoimmune conditions (lupus, IgA nephropathy)
When to worry:
Persistent 2+ protein or higher across multiple tests indicates kidney filtration problems requiring investigation.
What This Means For You:
If you have diabetes and see 1+ protein consistently, request a urine albumin-to-creatinine ratio test. This specialized test (covered by most insurance) detects early diabetic kidney disease when interventions are most effective. According to the National Institute of Diabetes and Digestive and Kidney Diseases, catching albumin elevation early can preserve kidney function for decades.
Real example:
Michael, 56, with Type 2 diabetes for 8 years, noticed 1+ protein on routine urinalysis. His doctor ordered albumin-to-creatinine ratio testing, which showed early diabetic nephropathy (stage A2). Starting ACE inhibitor medication and improving blood sugar control (tracked using our blood sugar converter) stabilized his kidney function within 6 months.
Next steps:
- Repeat urinalysis in 2-4 weeks
- Request 24-hour urine protein collection if persistent
- Get kidney function panel (serum creatinine, GFR)
- Review blood pressure medications
Blood in Urine (Hematuria): Red Flags vs. Harmless
Blood in urine manifests two ways: visible (gross hematuria) or microscopic (only detected by testing).
Causes breakdown by prevalence:
| Cause | Prevalence | Typical Presentation |
|---|---|---|
| Urinary tract infection (UTI) | 40% | Burning, frequency, urgency |
| Kidney stones | 25% | Severe flank pain, nausea |
| Exercise-induced | 15% | After intense workout, resolves in 48 hours |
| Menstrual contamination | 10% | Females during menstruation |
| Prostate enlargement | 5% | Males over 50, weak urine stream |
| Bladder/kidney cancer | 3-5% | Painless visible blood, smokers, over 50 |
| Glomerulonephritis | 2% | Protein also elevated, swelling |
Urgency Decision Matrix:
| Blood Level | Symptoms | Action Needed | Timeline |
|---|---|---|---|
| Trace (2-3 RBCs) | None | Repeat test, increase hydration | Recheck in 2-3 weeks |
| 5-10 RBCs/HPF | Mild burning | Schedule doctor visit, possible UTI | Within 3-5 days |
| >10 RBCs/HPF | Burning, fever, back pain | Urgent care evaluation, likely infection | Same day or next day |
| Visible blood | Flank pain, unable to pass urine | Emergency department | Immediate (possible stone/obstruction) |
| Visible blood + clots | Severe pain, fever, confusion | Call 911 or go to ER | Immediate emergency |
False positives for blood:
The dipstick test detects heme (iron-containing compound in blood), which also appears in:
- Menstrual blood contamination
- Myoglobin from extreme muscle breakdown (rhabdomyolysis)
- Certain foods (beets, berries) causing red urine
- Medications (rifampin, phenazopyridine)
According to CDC infection control guidelines, blood in urine combined with nitrites strongly suggests bacterial urinary tract infection requiring antibiotics.
Glucose in Urine: Diabetes or Something Else?
Normally, kidneys reabsorb 100% of filtered glucose. Glucose appears in urine when blood glucose exceeds the “renal threshold” (typically 180 mg/dL).
Causes of glucosuria:
Diabetes-related:
- Undiagnosed Type 1 or Type 2 diabetes
- Poorly controlled known diabetes
- Gestational diabetes during pregnancy
Non-diabetes causes:
- Pregnancy (lowered renal threshold, normal phenomenon)
- Fanconi syndrome (genetic kidney tubule disorder)
- Some medications (SGLT2 inhibitors like empagliflozin—intentionally cause glucose loss)
- Rare: renal glycosuria (benign genetic variation)
What to do:
Any positive glucose in non-diabetic individuals requires blood glucose testing. Request:
- Fasting blood glucose
- Hemoglobin A1c (3-month average blood sugar)
- Glucose tolerance test if pregnant
False positives/negatives:
Large doses of vitamin C (>500 mg) can cause false-negative glucose results. Conversely, certain antibiotics may cause false positives.
White Blood Cells (WBCs): Infection Indicators
Elevated white blood cells in urine (pyuria) indicates inflammation or infection in the urinary tract.
Interpretation guide:
- 0-5 WBCs/HPF: Normal
- 6-10 WBCs/HPF: Borderline, possible early infection or contamination
- 11-25 WBCs/HPF: Likely urinary tract infection
- >25 WBCs/HPF: Significant infection, possibly kidney involvement (pyelonephritis)
When WBCs don’t mean infection:
Our symptom checker helps differentiate infection from other causes:
- Kidney stones causing irritation
- Interstitial cystitis (chronic bladder inflammation)
- Sample contamination (vaginal discharge, poor collection technique)
- Post-procedure inflammation (recent catheterization)
UTI vs. Kidney Infection:
| Feature | Bladder Infection (Cystitis) | Kidney Infection (Pyelonephritis) |
|---|---|---|
| WBC count | 10-30/HPF | >50/HPF |
| Symptoms | Burning, frequency, urgency | Fever, flank pain, nausea |
| Nitrites | Usually positive | Usually positive |
| Bacteria | Moderate | Many |
| Treatment setting | Outpatient (oral antibiotics) | May require IV antibiotics/hospitalization |
Ketones: Keto Diet vs. Diabetic Emergency
Ketones result from fat metabolism when glucose isn’t available for energy.
2026 interpretation for keto dieters (NEW):
The updated AMA guidelines distinguish “nutritional ketosis” from diabetic ketoacidosis:
Nutritional Ketosis (Safe):
- Ketones: Trace to small (15-40 mg/dL)
- Blood glucose: Normal (70-120 mg/dL)
- No acidosis symptoms
- Person following ketogenic or very low-carb diet
Diabetic Ketoacidosis (Medical Emergency):
- Ketones: Moderate to large (>80 mg/dL)
- Blood glucose: Very high (>250 mg/dL) OR normal (in rare euglycemic DKA)
- Symptoms: Confusion, fruity breath, rapid breathing, severe abdominal pain
- Requires immediate ER evaluation
Research from Johns Hopkins Medicine shows ketogenic diets can safely produce trace to moderate ketones without health risks in non-diabetics. However, pregnant women should avoid ketogenic diets as ketones may affect fetal brain development.
pH Abnormalities: Acidic vs. Alkaline Urine
Urine pH varies based on diet, medications, and body acid-base balance.
Low pH (<5.0) – Acidic Urine:
Causes:
- High-protein diet (meat, eggs)
- Diabetic ketoacidosis
- Starvation or severe calorie restriction
- Chronic diarrhea
- Certain medications (methionine, ammonium chloride)
Clinical significance:
Chronically acidic urine increases risk of uric acid kidney stones. If pH consistently <5.5, discuss alkalinizing agents (potassium citrate) with your doctor.
High pH (>7.5) – Alkaline Urine:
Causes:
- Urinary tract infection with urease-producing bacteria (Proteus, Klebsiella)
- Vegetarian/vegan diet rich in fruits and vegetables
- Vomiting or nasogastric suctioning
- Renal tubular acidosis (kidney tubules can’t acidify urine properly)
- Old/contaminated urine sample (bacteria break down urea → ammonia)
Clinical significance:
Alkaline urine promotes calcium phosphate and struvite stone formation. Persistent pH >7.5 with positive nitrites strongly suggests UTI.
Maintaining optimal hydration (use our water intake calculator) helps maintain normal urine pH and prevents stone formation.
When To Worry – Action Decision Matrix
Not every abnormal result requires immediate action. This evidence-based framework helps you decide your next steps based on test results and symptoms.
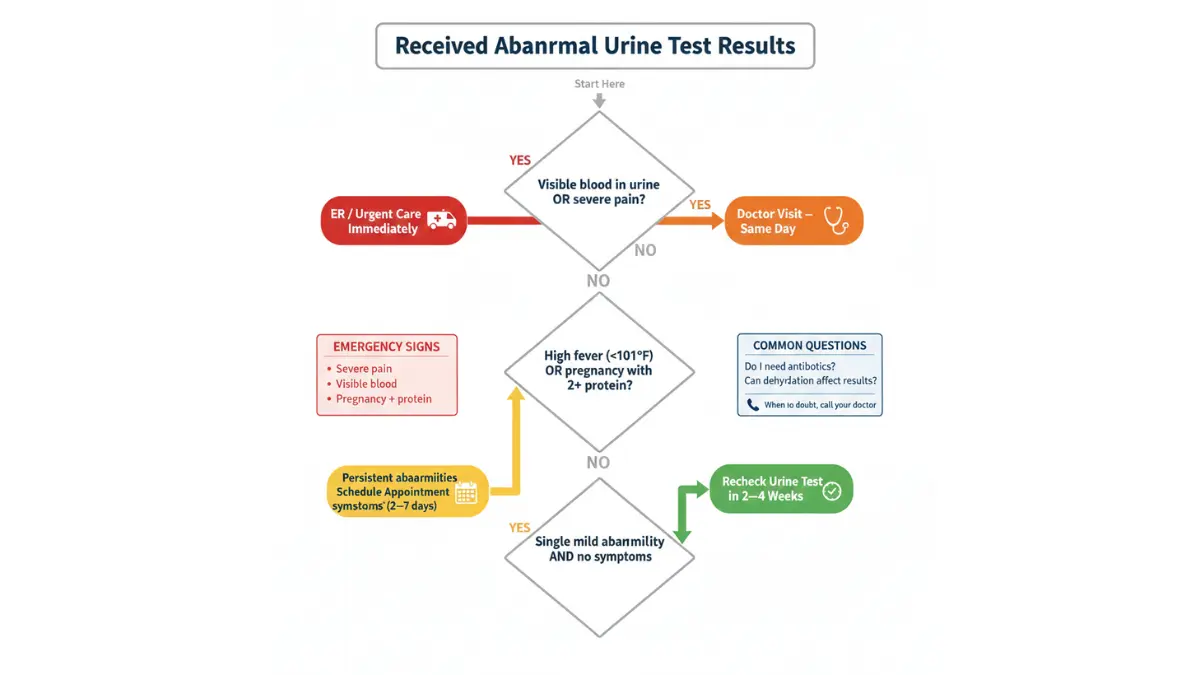
The 3-Tier Urgency System
TIER 1: NON-URGENT (Recheck in 2-4 Weeks)
Results in this category:
- Trace protein with no symptoms, no diabetes/hypertension
- pH slightly outside range (4.3-4.5 or 8.0-8.2) on single test
- 1-3 RBCs without visible blood or pain
- 3-6 WBCs without burning or frequency
- Specific gravity <1.005 or >1.025 (likely hydration-related)
What to do:
- Increase water intake to 8-10 glasses daily
- Avoid intense exercise for 48 hours before repeat test
- Repeat urinalysis in 2-4 weeks
- Keep symptom diary
- No treatment needed unless results persist
Example scenario:
Linda, 34, had trace protein on routine physical exam urinalysis. No diabetes, normal blood pressure, no symptoms. Repeat testing 3 weeks later after avoiding exercise for 2 days showed completely normal results. Diagnosis: Benign transient proteinuria from her marathon training.
TIER 2: SCHEDULE DOCTOR VISIT (Within 2-7 Days)
Results in this category:
- Persistent 1+ protein across two tests
- Any positive glucose (if not known diabetic)
- 5-15 WBCs with mild burning or frequency
- Trace to moderate ketones in non-keto dieter
- Positive nitrites without severe symptoms
- pH consistently <4.5 or >8.0 across multiple tests
- 3-10 RBCs with intermittent mild flank discomfort
What to do:
- Call primary care physician for appointment within week
- Bring all previous lab results
- List all medications (including supplements)
- Note any symptoms: burning, frequency, blood, pain, fever
- Request urine culture if infection suspected
Questions to ask your doctor:
- Do my symptoms match urinary tract infection?
- Should we do a urine culture before starting antibiotics?
- Do I need imaging (ultrasound, CT) to check for stones?
- Could any of my medications cause these results?
- Do I need 24-hour urine collection for protein quantification?
- Should we check kidney function with blood tests (creatinine, GFR)?
- When should I repeat the urinalysis?
- What symptoms would prompt me to go to urgent care before my appointment?
TIER 3: URGENT/EMERGENCY CARE (Same Day or ER)
Results requiring immediate evaluation:
- Visible blood (red or brown urine) with severe pain
- 2+ or 3+ protein with facial/leg swelling
- Large ketones with confusion, rapid breathing, or abdominal pain (diabetics)
- 20 WBCs with fever >101°F (38.3°C)
- Dark urine (tea/cola colored) with yellow skin or eyes (jaundice)
- Any abnormal results with inability to urinate despite urge
- Blood in urine + fever + flank pain (possible kidney infection)
- Pregnant with 2+ protein + headache + vision changes (preeclampsia warning)
Where to go:
- Emergency Department: Severe pain, high fever (>102°F/38.9°C), visible blood with clots, pregnant with protein + headache, diabetic with large ketones + confusion
- Urgent Care: Moderate symptoms, fever 100-102°F, blood without severe pain, significant WBCs with burning
What to bring:
- All medications (bring bottles)
- Recent lab results
- List of allergies
- Insurance card and ID
- Summary of symptoms including when they started
Red Flags Requiring Immediate Attention
Call 911 or go to ER immediately for:
- Visible blood in urine + inability to urinate + severe abdominal pain (possible obstruction)
- Diabetic with large ketones + confusion + fruity breath odor (diabetic ketoacidosis)
- High fever (>103°F/39.4°C) + severe flank pain + vomiting (sepsis risk from kidney infection)
- Pregnant beyond 20 weeks with 2+ protein + severe headache + visual disturbances (eclampsia risk)
Real emergency scenario:
David, 58, experienced sudden severe right flank pain radiating to groin, visible blood in urine, and nausea. Urinalysis at ER showed >50 RBCs/HPF. CT scan revealed 7mm kidney stone causing obstruction. He received IV pain medication and underwent same-day ureteroscopy to remove the stone. Delay could have caused permanent kidney damage.
Understanding these tiers empowers you to respond appropriately without either ignoring concerning findings or panicking over benign temporary abnormalities.
Factors Affecting Your Urine Test Results
Many substances and conditions alter urine test results without indicating disease. Knowing these factors prevents unnecessary worry and repeat testing.
Medications That Change Results (100+ Drug Database)
Over 100 commonly prescribed medications affect urinalysis results. Always inform your healthcare provider about ALL medications before testing.
Most Common Medication Effects:
| Medication Class | Affected Parameters | How Results Change |
|---|---|---|
| Antibiotics (ciprofloxacin, nitrofurantoin) | Protein, glucose, pH | False positive protein, altered pH |
| NSAIDs (ibuprofen, naproxen) | Protein, blood | May cause actual kidney damage → protein |
| Phenazopyridine (AZO, Pyridium) | Color, all parameters | Orange color, interferes with dipstick readings |
| Vitamin C (>500 mg/day) | Glucose, blood | False negative for both |
| Diuretics (furosemide, HCTZ) | Specific gravity, glucose | Diluted urine, may show glucose |
| Levodopa (Parkinson’s medication) | Color, ketones | Dark urine, false positive ketones |
| Rifampin (tuberculosis treatment) | Color | Orange-red urine (normal effect) |
| Metformin (diabetes medication) | Ketones, lactate | May show ketones during illness |
What to do:
Don’t stop medications before urine testing unless specifically instructed by your physician. Instead, inform the lab about all medications so they can interpret results appropriately.
According to research from the National Institutes of Health, medication interference accounts for 15-20% of false positive urinalysis results.
Food & Supplement Impact on Urine Tests
Foods causing color changes (not actual blood):
- Beets, berries, rhubarb: Pink to red urine (mimics blood)
- Asparagus: Strong odor, greenish tint
- Carrots, vitamin A: Orange urine
- Fava beans: Dark brown urine
- Food dyes (artificial colors in candy, sports drinks): Various colors
Dietary effects on test parameters:
High-Protein Diet:
- Increased specific gravity
- Possible temporary protein spillage after very high intake (>200g protein/day)
- More acidic pH (<5.5)
- Increased urea nitrogen
Vegetarian/Vegan Diet:
- More alkaline pH (6.5-8.0)
- Lower specific gravity
- Less concentrated urine
Supplements causing abnormalities:
- B-vitamins: Bright yellow/neon color (harmless riboflavin)
- Vitamin C (>1000 mg): False negative blood and glucose
- Iron supplements: Dark urine, possible false positive blood
- Calcium supplements: Increased calcium crystals
Timing & Collection Errors
Improper urine collection is the #1 cause of inaccurate results.
First morning vs. random sample:
First Morning Urine (Most Accurate):
- Most concentrated (best for detecting small abnormalities)
- Preferred for protein evaluation
- Required for pregnancy tests
- Recommended for microscopic examination
Random Urine:
- Acceptable for most screening tests
- May be too diluted if collected after drinking large amounts of water
- Influenced by recent meals, exercise, medications
Common collection errors:
Contamination Problems:
- Menstrual blood mixing with urine (false positive blood, high WBCs)
- Vaginal discharge contamination (increased epithelial cells, bacteria)
- Fecal contamination (bacteria, increased WBCs)
- Skin bacteria from inadequate cleansing
How to collect proper “clean catch” midstream sample:
- Wash hands thoroughly with soap and water
- Cleanse genital area:
- Females: Separate labia, wipe front to back with provided wipe
- Males: Retract foreskin (if uncircumcised), cleanse tip of penis
- Start urinating into toilet (flush initial urine)
- Midstream collection: Move cup into stream, collect 1-2 ounces
- Finish urinating into toilet
- Seal cup immediately and deliver to lab within 1 hour if possible
Sample degradation:
Urine begins changing chemically within 30 minutes at room temperature:
- Bacteria multiply (false positive infection)
- pH increases (bacteria break down urea → ammonia)
- Glucose decreases (bacteria consume it)
- Cells disintegrate
- Crystals dissolve or form artifactually
Refrigerate samples if testing delayed >2 hours. Never freeze urine for standard urinalysis.
Hydration Status Impact
Water intake dramatically affects urine concentration and test results.
Dehydrated (Dark yellow/amber urine):
- High specific gravity (>1.025)
- Falsely elevated protein concentration
- All substances appear more concentrated
- May trigger false positive results
Over-hydrated (Nearly clear urine):
- Low specific gravity (<1.010)
- Diluted results may miss abnormalities
- Glucose and protein may fall below detection threshold despite being present
Optimal hydration for accurate testing:
Clear to pale yellow urine indicates proper hydration. Aim for 8-10 glasses (64-80 ounces) daily, adjusting for activity level, climate, and body size. Calculate your specific needs using our water intake calculator.
Exercise & Physical Activity Effects
Intense or prolonged exercise temporarily alters multiple urine parameters.
Exercise-induced changes:
Protein (Exercise Proteinuria):
- Affects up to 70% of athletes after intense workouts
- Usually resolves within 24-48 hours
- Mechanism: Temporary increase in glomerular permeability
- Not harmful, doesn’t indicate kidney disease
Blood (Exercise Hematuria):
- Occurs in 10-15% of endurance athletes
- Caused by: Bladder trauma (empty bladder bouncing), kidney trauma, hemolysis (red blood cell breakdown)
- Usually trace to small amounts
- Resolves with rest
Myoglobin:
- Released from muscle breakdown during extreme exertion
- Causes positive dipstick “blood” without actual RBCs
- Dangerous if severe (rhabdomyolysis) → kidney failure risk
Recommendation:
Avoid intense exercise 48 hours before routine urinalysis for most accurate results. If recent intense activity, inform your doctor—they may repeat testing after rest period rather than pursuing extensive workup.
Pregnancy-Specific Changes
Normal physiological changes during pregnancy alter urinalysis results.
Expected pregnancy changes:
Protein:
- Up to 1+ (30 mg/dL) considered normal in late pregnancy
- 1+ with high blood pressure or swelling requires immediate evaluation (preeclampsia)
Glucose:
- Renal threshold decreases during pregnancy
- Glucose may appear in urine with normal blood sugar
- Any positive glucose requires glucose tolerance testing to rule out gestational diabetes
pH:
- May be slightly more alkaline due to dietary changes
- Increased risk of UTIs due to urinary stasis
Bacteria:
- Pregnancy increases UTI risk 2-4 fold
- Even asymptomatic bacteriuria requires treatment (unlike non-pregnant women)
- Untreated UTIs can cause preterm labor
White blood cells:
- Slightly higher acceptable range (up to 10/HPF)
- Vaginal discharge contamination more common
Track pregnancy health metrics comprehensively using our pregnancy weight gain calculator and fetal growth percentile calculator.
Next Steps & Follow-up Testing
Abnormal urinalysis results often trigger additional testing to pinpoint the underlying cause and guide treatment.
Common Follow-Up Tests Explained
24-Hour Urine Collection:
When ordered:
- Persistent protein to quantify exact amount
- Kidney stone risk assessment
- Hormone evaluation (cortisol, metanephrines)
- Creatinine clearance (kidney function assessment)
How to collect:
- Discard first morning urine on Day 1
- Collect ALL urine for next 24 hours in provided container
- Refrigerate container between collections
- Include first morning urine on Day 2
- Return to lab promptly
What it measures:
Total protein, creatinine, calcium, uric acid, oxalate, citrate, sodium, and other substances over 24 hours. More accurate than spot urine for quantifying abnormalities.
Cost: $50-$150 without insurance; usually covered with copay if medically indicated.
Urine Culture & Sensitivity:
When ordered:
- Suspected UTI with positive nitrites or high WBCs
- Treatment failure after antibiotics
- Recurrent UTIs (>2 per year)
- Pregnant women with any bacteria
- Complicated UTIs (males, catheters, immunocompromised)
How it works:
- Lab grows bacteria from urine sample (48-72 hours)
- Identifies specific organism (E. coli, Klebsiella, etc.)
- Tests which antibiotics kill the bacteria (sensitivity testing)
Results timeline: 48-72 hours for preliminary results; full sensitivity panel may take 3-5 days.
Cost: $30-$80 without insurance; typically covered by insurance with medical necessity.
Kidney Function Panel (Blood Test):
Complements urine testing to assess overall kidney health.
Tests included:
- Serum creatinine (waste product kidneys filter)
- Blood Urea Nitrogen (BUN)
- Estimated GFR (glomerular filtration rate)
- Electrolytes (sodium, potassium, chloride, CO2)
- Calcium and phosphorus
Interpretation:
- GFR >60 mL/min/1.73m²: Normal kidney function
- GFR 30-59: Moderate kidney disease (Stage 3 CKD)
- GFR 15-29: Severe kidney disease (Stage 4 CKD)
- GFR <15: Kidney failure (Stage 5 CKD)
According to NIDDK kidney disease research, catching kidney disease at Stage 3 and implementing treatment can prevent progression to dialysis in many patients.
Imaging Studies:
Kidney/Bladder Ultrasound:
- Non-invasive, no radiation
- Detects stones, masses, cysts, structural abnormalities
- Cannot see inside ureters well
- Cost: $200-$500 without insurance
CT Scan (Non-Contrast for Stones):
- Gold standard for kidney stone detection (>95% sensitivity)
- Detects stones as small as 1-2mm
- Evaluates kidney structure, ureters, bladder
- Radiation exposure (equivalent to 6 months background radiation)
- Cost: $500-$3,000 without insurance
Cystoscopy:
- Camera inserted through urethra into bladder
- Directly visualizes bladder lining
- Can detect tumors, inflammation, stones
- Done in urology clinic under local anesthesia
- Cost: $1,500-$4,500 without insurance
Cost Transparency & Insurance Navigation
Typical costs for common urine tests (2026):
| Test | Without Insurance | With Insurance (Copay) | Medicare Coverage |
|---|---|---|---|
| Basic urinalysis | $25-$75 | $10-$25 | Covered (80%) |
| Urine culture | $30-$80 | $15-$30 | Covered (80%) |
| 24-hour urine collection | $50-$150 | $20-$50 | Covered with medical necessity |
| Kidney function panel | $40-$100 | $10-$30 | Covered (80%) |
| Kidney ultrasound | $200-$500 | $50-$150 | Covered (80%) |
| CT scan (abdomen/pelvis) | $500-$3,000 | $100-$500 | Covered (80%) |
Insurance tips:
- Request pre-authorization for imaging studies
- Use in-network labs and facilities
- Ask about payment plans if uninsured
- Many hospital systems offer financial assistance (apply before testing)
Prevention: Keeping Your Results Normal
Hydration strategies:
- Drink 64-80 ounces (8-10 glasses) water daily
- Increase to 80-100 ounces in hot weather or with exercise
- Urine should be pale yellow (if dark, drink more)
Dietary recommendations:
- Balanced diet with moderate protein (0.8-1.0g per kg body weight)
- Limit sodium (<2,300 mg daily) to reduce kidney stress
- Adequate calcium (1,000-1,200 mg daily) prevents oxalate stones
- Reduce oxalate-rich foods if prone to kidney stones (spinach, nuts, chocolate)
When to retest:
- Abnormal results: Repeat in 2-4 weeks
- Diabetes or hypertension: Annual screening
- Kidney disease: Every 3-6 months
- Recurrent UTIs: After each episode
- Pregnancy: Every prenatal visit
Maintain overall health by tracking metrics like BMI and following evidence-based wellness strategies on our health tips page.
Frequently Asked Questions About Urine Test Results
1. What does “trace” mean on my urine test?
Trace indicates the substance is barely detectable—present in very small amounts just above the detection threshold. Trace protein or blood often resolves without treatment and may be normal variation.
2. Can a urine test detect pregnancy?
Yes. Urine pregnancy tests detect hCG (human chorionic gonadotropin) hormone. Home tests work 1-2 weeks after missed period; lab tests detect pregnancy earlier (6-8 days after conception).
3. Why is my urine cloudy but the test shows no infection?
Cloudy urine without infection may result from phosphate crystals (benign, common in alkaline urine), concentrated urine, or vaginal discharge contamination. Increased hydration often clears this.
4. What does “HPF” mean in urine test results?
HPF stands for “high-power field”—the viewing area when lab technicians examine urine under a microscope at high magnification. Results report how many cells (RBCs, WBCs) appear per HPF.
5. Can dehydration cause abnormal urine test results?
Absolutely. Dehydration concentrates urine, making all substances appear elevated. Protein, specific gravity, and even glucose may test abnormally high simply from dehydration. Retest after proper hydration.
6. How long do urine test results take?
Basic urinalysis: 30 minutes to 24 hours. Urine culture: 48-72 hours for preliminary results, 3-5 days for complete sensitivity testing. Some hospital labs provide rapid results within hours.
7. What does 1+ or 2+ protein mean?
These are semi-quantitative measurements: 1+ = approximately 30 mg/dL, 2+ = 100 mg/dL, 3+ = 300 mg/dL, 4+ = >1000 mg/dL. Higher numbers indicate more protein in urine. Persistent 1+ or higher requires investigation.
8. Can I eat before a urine test?
Yes, eating before urinalysis is fine for most tests. However, avoid high-protein meals immediately before if testing for protein. First morning urine (before eating/drinking) provides most accurate results.
9. Why do I need to provide midstream urine?
The first portion of urine flushes bacteria from the urethra. Midstream collection avoids this contamination, providing cleaner sample that better represents bladder contents. This reduces false positive infection results.
10. What does specific gravity measure?
Specific gravity measures urine density compared to water (1.000). It indicates kidney concentration ability and hydration status. Higher values (>1.020) = concentrated/dehydrated; lower (<1.010) = dilute/over-hydrated.
11. Can stress affect urine test results?
Acute stress doesn’t directly alter urinalysis results, but stress-related behaviors do. Stress may increase blood pressure (affecting protein), cause dehydration (concentrated urine), or trigger urinary frequency mimicking infection symptoms.
Key Takeaway: Understanding your urine test results empowers you to make informed health decisions. While this guide provides comprehensive interpretation, always consult your healthcare provider about your specific results. Early detection of kidney disease, diabetes, and urinary tract problems through routine urinalysis saves lives and preserves kidney function.
For related diagnostic test interpretation, explore our guides on CBC test results, liver function tests, and HbA1c levels.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.