On This Page – Quick Medical Summary
When James, a 58-year-old high school teacher from Ohio, heard the word “immunotherapy” at his oncology appointment, he felt two things simultaneously: hope and complete confusion. His oncologist had used terms like “checkpoint inhibitors” and “PD-L1 expression” without pausing to explain them. He left that appointment with more questions than answers.
If you’ve been in James’s position — or you’re a caregiver, a curious patient, or someone researching cancer treatment options — this guide is for you.
Immunotherapy is a medical treatment that activates or strengthens your body’s own immune system to identify, attack, and destroy disease — most commonly cancer cells — with far greater precision than traditional treatments like chemotherapy or radiation. Unlike drugs that poison cancer cells directly, immunotherapy teaches your immune system to do what it was always designed to do: eliminate threats.
It is also used outside of oncology. Allergen immunotherapy — commonly known as allergy shots or sublingual therapy — has helped millions of Americans reduce or eliminate their allergic reactions to pollen, pet dander, bee venom, and more. This guide covers both.
📌 Key Stat: The National Cancer Institute (NCI) reports that more than 150 FDA-approved immunotherapy treatments now exist across cancer types — with 17 new approvals granted in 2024 alone.
Not sure which symptoms led you here? Use our Symptom Checker as a helpful starting point before your next medical appointment.
What Is Immunotherapy? Your Immune System, Cancer’s Escape, and the Fix
Your Immune System — The Body’s Built-In Defense Force
Your immune system is a sophisticated, always-on surveillance network. It consists of:
- White blood cells (T cells, B cells, NK cells) — the soldiers that detect and destroy invaders
- The lymphatic system — the highways that transport immune cells throughout the body
- Antibodies — precision-targeted proteins that tag foreign threats for destruction
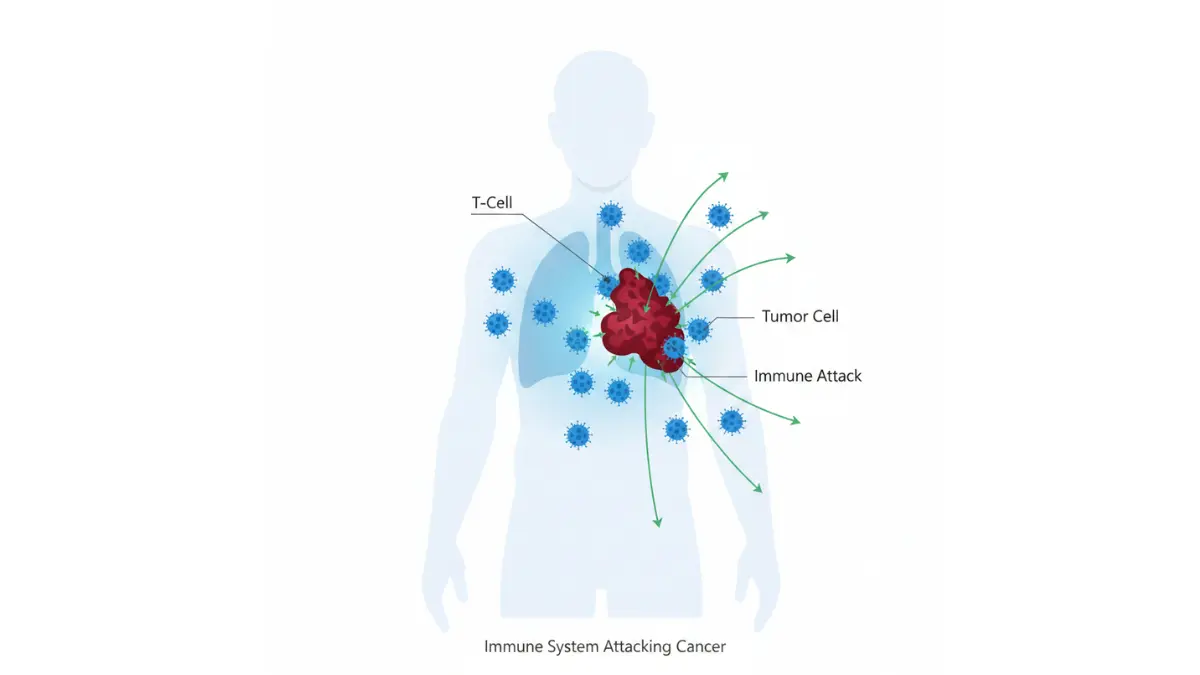
Under normal conditions, T cells patrol your body and destroy abnormal cells — including early-stage cancer cells — before they can grow. This process works silently, constantly, and mostly without you knowing.
Why Cancer Cells Escape Detection
Here is the uncomfortable truth that many competitors don’t explain clearly: cancer cells are not foreign invaders. They are your own cells — mutated.
Because they originate from your own tissue, cancer cells learn to “speak” the immune system’s language. Specifically:
- They display a protein called PD-L1 on their surface
- PD-L1 binds to PD-1 receptors on T cells, sending a signal: “Don’t attack me — I’m one of you”
- Your T cells receive this false signal, stand down, and allow the cancer to grow unchecked
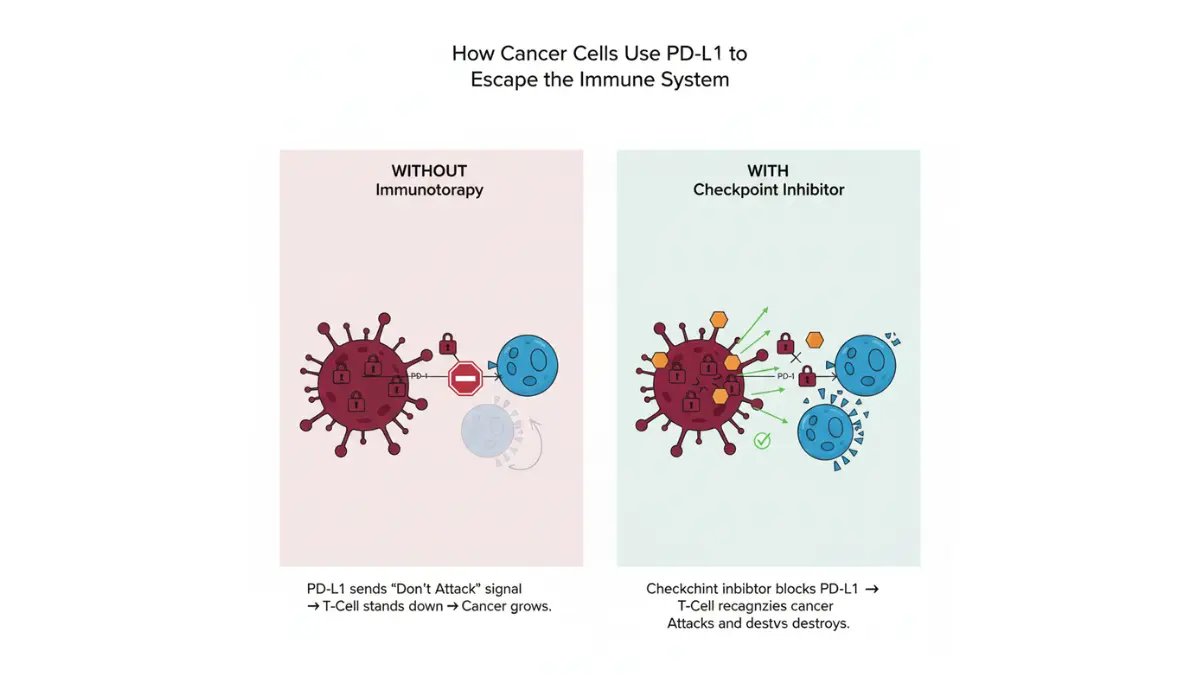
Think of it this way: cancer cells are like criminals wearing police uniforms. Your immune system can’t tell them apart from healthy cells, so it lets them walk right past.
How Immunotherapy Unmasks and Destroys Cancer
Immunotherapy interrupts this deception. Depending on the type used, it either:
- Blocks the PD-L1/PD-1 “disguise” so T cells can recognize and attack the cancer
- Engineers T cells to identify cancer with complete precision
- Marks cancer cells with antibodies so immune cells can find them
- Gradually desensitizes the immune system to specific allergens (in allergy treatment)
💡 Key Takeaway: Unlike chemotherapy, immunotherapy doesn’t attack cells directly. It trains your immune system to find and destroy cancer — and the immune system can remember, providing protection even years after treatment ends.
For patients with cancer, understanding your genetic risk profile is a powerful first step. Our Genetic Risk Assessment Tool can help you explore hereditary health factors worth discussing with your doctor.
7 Types of Immunotherapy — The Complete 2026 Guide
No single competitor covers all seven types in one article. Here they are, clearly explained.

1. Immune Checkpoint Inhibitors — The Most Widely Used Type
Checkpoint inhibitors are the backbone of modern cancer immunotherapy. They work by blocking the PD-1, PD-L1, or CTLA-4 “off switch” that cancer cells use to hide from immune cells.
FDA-approved checkpoint inhibitor drugs include:
- Pembrolizumab (Keytruda) — approved for 30+ cancer types
- Nivolumab (Opdivo) — melanoma, lung, kidney, bladder, and others
- Ipilimumab (Yervoy) — melanoma, often combined with nivolumab
📊 2026 Data: Checkpoint inhibitors account for 81% of all immunotherapy treatments used clinically, according to data from the Cancer Research Institute’s 2025 Insights + Impact Report.
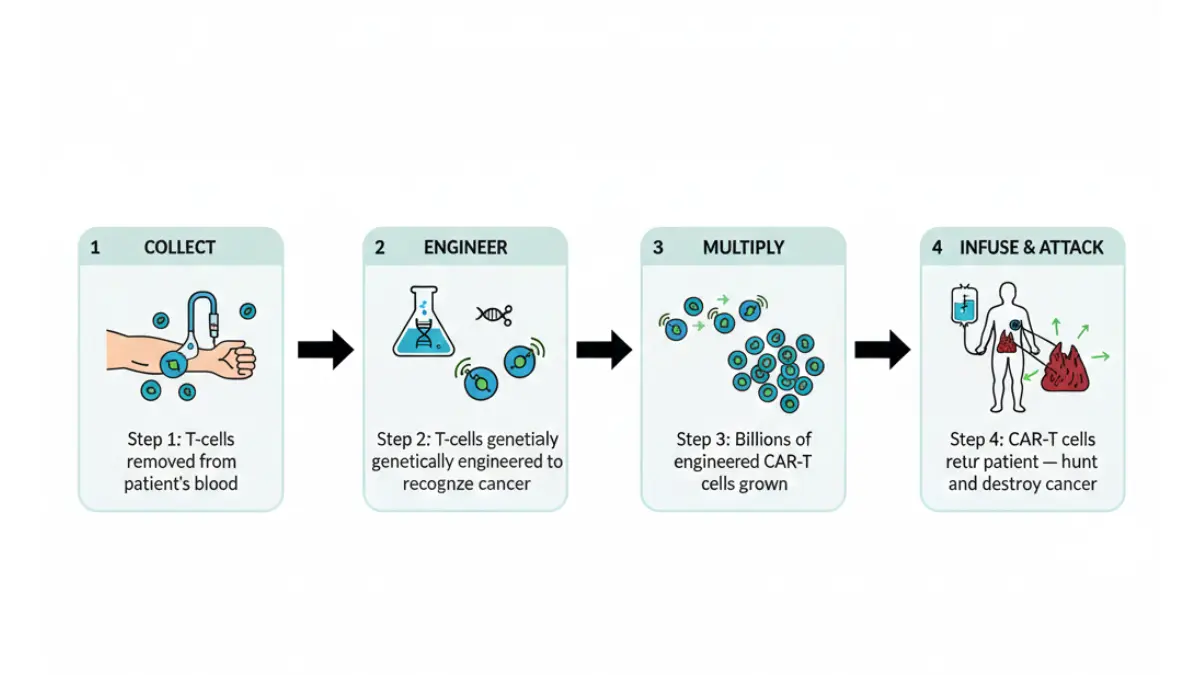
2. CAR-T Cell Therapy — The Engineered Immune Cell Revolution
CAR-T (Chimeric Antigen Receptor T-cell) therapy involves:
- Removing T cells from the patient’s blood
- Genetically engineering them in a lab to add “targeting receptors”
- Growing billions of these new cells
- Infusing them back into the patient as a personalized cancer-fighting army
Currently approved for: B-cell lymphoma, multiple myeloma, leukemia, and some other blood cancers. Solid tumor trials are actively ongoing as of 2026.
3. TIL Therapy — The Newest FDA Approval (2024)
Tumor-Infiltrating Lymphocyte (TIL) therapy harvests immune cells already present inside a patient’s tumor, supercharges them in the laboratory, and returns them to the body in much larger numbers.
In 2024, the FDA approved lifileucel (Amtagvi) — the first TIL therapy for a solid cancer (advanced melanoma). A 2025 NIH clinical trial showed promising early results extending TIL therapy into gastrointestinal cancers for the first time.
4. Cancer Vaccines — Teaching Immunity Before and After Diagnosis
Cancer vaccines work differently from preventive vaccines. Rather than preventing a disease, treatment vaccines train the immune system to recognize and attack existing tumors.
- Personalized neoantigen vaccines: Built from a patient’s own tumor mutations (Moderna and Merck’s mRNA-4157 is in Phase 3 trials as of 2026)
- Sipuleucel-T (Provenge): FDA-approved for prostate cancer
- Oncolytic virus vaccines: Use modified viruses to infect and destroy cancer cells while triggering immune response
5. Monoclonal Antibodies
Lab-engineered proteins designed to bind to specific targets on cancer cells — either flagging them for immune destruction, delivering chemotherapy directly to the tumor, or blocking signals that promote cancer growth.
Examples: Trastuzumab (Herceptin) for HER2+ breast cancer, Bevacizumab (Avastin) for several cancers.
6. Cytokine Therapy
Cytokines are natural immune signaling proteins. In cancer treatment, high-dose Interleukin-2 (IL-2) and Interferon-alpha boost immune activity against tumors. These older therapies are often used alongside checkpoint inhibitors to amplify response.
7. Allergen Immunotherapy — Immunotherapy Isn’t Only for Cancer
This is what Healthline, WebMD, and Mayo Clinic almost universally miss in their primary immunotherapy articles.
Allergen immunotherapy retrains the immune system to stop overreacting to harmless substances. It works through gradual, escalating exposure to the triggering allergen.
Two delivery methods exist:
- Subcutaneous immunotherapy (SCIT): Allergy shots given in a clinic, typically weekly for 6–12 months, then monthly for 3–5 years
- Sublingual immunotherapy (SLIT): Drops or tablets placed under the tongue, taken daily at home — increasingly popular in the USA
Effective for: Pollen, dust mites, pet dander, bee venom, mold, and some food allergies in children. Studies show up to 85% effectiveness for bee venom allergy, dramatically reducing anaphylaxis risk.
📊 Summary Comparison Table
| Type | Used For | How Given | Response Rate |
|---|---|---|---|
| Checkpoint Inhibitors | Multiple cancers | IV infusion | 20–45% |
| CAR-T Cell Therapy | Blood cancers | IV (engineered cells) | 50–90% (blood cancers) |
| TIL Therapy | Melanoma, GI tumors (2025+) | IV infusion | 7–30% (solid tumors) |
| Cancer Vaccines | Prostate, melanoma, others | Injection | Varies by cancer type |
| Monoclonal Antibodies | Multiple cancers | IV or injection | Cancer-specific |
| Cytokine Therapy | Melanoma, kidney cancer | Injection/IV | 15–20% |
| Allergen Immunotherapy | Allergies | Shots / sublingual | Up to 85% |
If you’re currently managing a chronic condition during treatment, use our Heart Rate Zone Calculator to safely monitor your cardiovascular fitness levels throughout recovery.
Who Qualifies for Immunotherapy — Success Rates & Why It Sometimes Fails
Cancers With the Best Response Rates in 2026
Not all cancers respond equally to immunotherapy. Here is where it works best, based on current clinical data:
| Cancer Type | Response Rate | Best Immunotherapy |
|---|---|---|
| Hodgkin Lymphoma | Up to 69% (relapsed/refractory) | Nivolumab |
| Melanoma (advanced) | 30–40% (5-year survival) | Pembrolizumab, Nivolumab + Ipilimumab |
| Non-Small Cell Lung Cancer (high PD-L1) | ~45% | Pembrolizumab |
| Triple-Negative Breast Cancer | ~45% | Pembrolizumab + chemotherapy |
| Colorectal (MSI-high only) | 30–40% | Pembrolizumab |
| Bladder Cancer | 20–25% | Atezolizumab |
For deeper reading on lung cancer treatment options, see our article on FDA-approved lung cancer drugs in 2026 and our guide to Stage 1 lung cancer survival rates.
The Biomarker Test: How Doctors Know If You’ll Respond
Before starting immunotherapy, oncologists use specific tests to predict your response:
- PD-L1 expression test: Measures how much of the “disguise protein” is present on your tumor. Higher PD-L1 = better checkpoint inhibitor response.
- MSI (Microsatellite Instability) testing: Tumors with high MSI (called MSI-H) have defective DNA repair and respond far better to immunotherapy. Pembrolizumab is FDA-approved for any MSI-H cancer, regardless of location.
- TMB (Tumor Mutational Burden): Higher mutation counts generally correlate with better immunotherapy response, as there are more targets for T cells to recognize.
💡 What This Means For You: Before starting immunotherapy, specifically ask your oncologist: “What is my PD-L1 score?” and “Have I been tested for MSI and TMB?” These three numbers can determine whether immunotherapy is the right first choice.
Why Immunotherapy Doesn’t Work for 60–80% of Patients — The Honest Truth
Only 20–40% of cancer patients respond to immunotherapy across all cancer types, according to peer-reviewed data published in Nature. This is not a failure of the patient — it reflects tumor biology.
Key reasons immunotherapy fails:
- “Cold” tumors: Low immune cell infiltration — T cells simply can’t get inside the tumor
- Tumor microenvironment immunosuppression: The tumor creates a local “immune-free zone”
- Low or absent PD-L1 expression: Nothing for checkpoint inhibitors to block
- Specific genetic mutations (e.g., EGFR or ALK in lung cancer → targeted therapy is preferred)
Who should NOT receive certain immunotherapies:
- Patients with active autoimmune diseases (lupus, rheumatoid arthritis, MS, Crohn’s disease)
- Patients on high-dose corticosteroids (suppresses immune activation needed for treatment)
- Patients with certain gene mutations where alternative targeted therapies are more effective
For context on related autoimmune testing, our guide on anti-CCP test results explains what these markers mean before starting any immune-modulating treatment.
Immunotherapy Side Effects, Real Costs & What Patients Actually Experience
Common Immunotherapy Side Effects
Because immunotherapy activates your immune system broadly, side effects come from immune activity — not cell destruction. This creates a different side effect profile from chemotherapy.
| Side Effect | Frequency | Severity |
|---|---|---|
| Fatigue | Very common (>30%) | Mild to moderate |
| Skin rash / itching | Common | Mild |
| Diarrhea | Common | Mild to moderate |
| Nausea | Common | Mild |
| Flu-like symptoms | Common | Mild |
| Immune-related pneumonitis (lung inflammation) | Uncommon (3–5%) | Serious |
| Liver inflammation (hepatitis) | Uncommon | Serious |
| Thyroid disorders | Uncommon | Manageable long-term |
| Colitis | Uncommon | Serious |
💡 Key Takeaway: Immunotherapy rarely causes hair loss — one of the most feared side effects of chemotherapy. Side effects can also appear weeks or months after treatment ends, unlike chemotherapy side effects that typically resolve between cycles.
If serious immune-related side effects occur (especially lung or liver inflammation), doctors treat with high-dose corticosteroids and may pause or permanently stop immunotherapy.
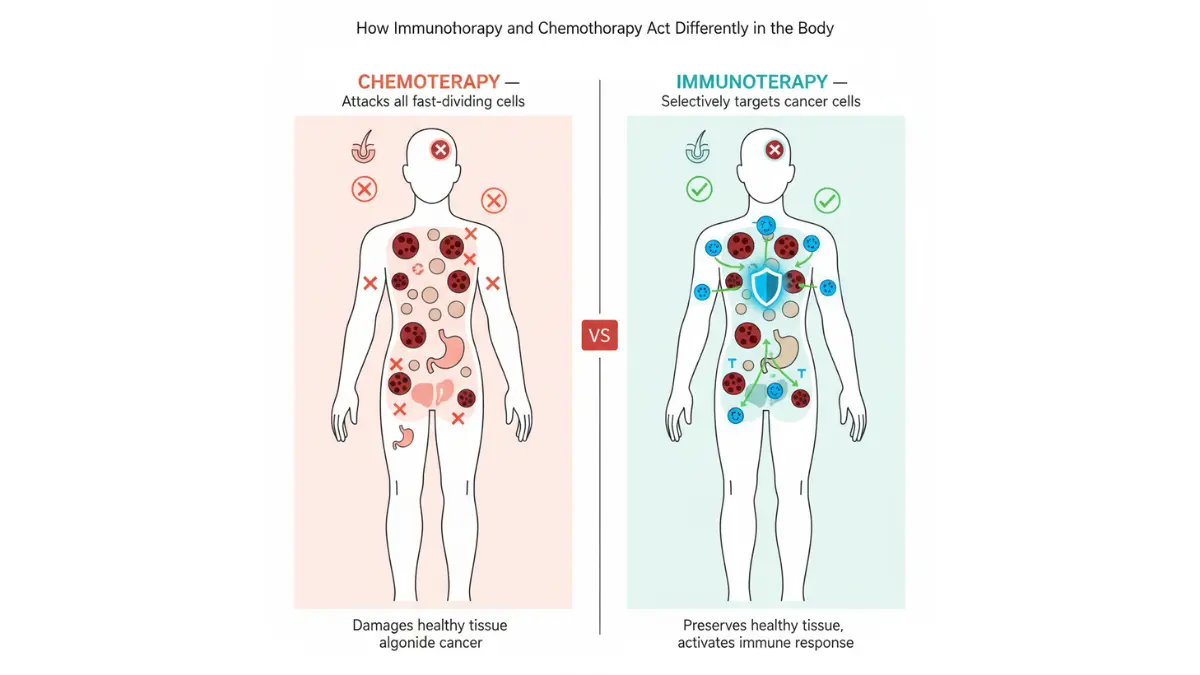
Immunotherapy vs. Chemotherapy: Side-by-Side
| Feature | Immunotherapy | Chemotherapy |
|---|---|---|
| Mechanism | Activates immune system | Kills fast-dividing cells |
| Hair loss | Rarely | Very common |
| Suppresses immune system | No | Yes |
| Nausea/vomiting | Less common | Very common |
| Fatigue | Moderate | Often severe |
| Lasting memory effect | ✅ Yes | ❌ No |
| Autoimmune risk | Yes (immune activation) | Low |
For a detailed guide on chemotherapy side effects and what to expect, read our 2026 Chemotherapy Guide and our overview of radiation therapy as a comparison.
The Real Cost of Immunotherapy in 2026 — What No Competitor Will Tell You
This section does not exist in any depth on Healthline, WebMD, or Mayo Clinic’s immunotherapy articles. Here are the real numbers:
| Treatment | Estimated Annual Cost (USA) |
|---|---|
| Checkpoint inhibitor (e.g., Keytruda) | $150,000–$250,000/year |
| Combination checkpoint therapy (Opdivo + Yervoy) | $250,000–$350,000/year |
| CAR-T cell therapy | $400,000–$500,000 (one-time treatment) |
| TIL therapy (lifileucel / Amtagvi) | ~$500,000 per course |
| Allergen immunotherapy (allergy shots) | $800–$4,000/year (most insured) |
Insurance coverage: Medicare, Medicaid, and most major private insurers cover FDA-approved immunotherapies when prescribed for their approved indications. Prior authorization is typically required.
Financial assistance programs to know:
- Merck’s Keytruda Patient Assistance Program
- Bristol Myers Squibb’s Access Support for Opdivo and Yervoy
- The HealthWell Foundation and CancerCare — both offer treatment-specific grants
💡 Key Takeaway: Ask your oncology social worker about Patient Assistance Programs before your first infusion. Most major cancer centers have dedicated financial navigators. This step alone can save tens of thousands of dollars.
What an Immunotherapy Session Actually Looks Like
- You arrive at an infusion center, typically at a hospital or cancer center
- An IV line is placed in your arm
- The infusion takes 30–90 minutes, depending on the drug
- You are monitored for 30–60 minutes afterward for immediate reactions
- Treatment is typically given every 2–3 weeks, with cycles lasting months to years
Most patients report that the first 1–2 cycles feel manageable — nothing like the severe nausea many expect from cancer treatment. Side effects often build gradually over subsequent cycles.
Immunotherapy vs. Chemotherapy — And the 2026 Breakthroughs Changing Everything
Should You Choose Immunotherapy Over Chemotherapy?
The answer is: it depends entirely on your cancer type, biomarker profile, and stage. There is no universal “better” option. The decision should always be made with a board-certified oncologist.
That said, for cancers where immunotherapy has received FDA approval and where biomarkers indicate likely response, it offers several advantages:
- More durable responses: Some melanoma patients treated with checkpoint inhibitors in 2014–2015 remain in complete remission today — a 10+ year outcome that would have been unthinkable with standard chemotherapy
- Immune memory: The immune system may continue surveilling for cancer cells even after treatment stops
- Different toxicity profile: Less damage to hair follicles, bone marrow, and the digestive tract lining
For patients with lung cancer, especially those with Stage 4 metastatic disease, our article on Stage 4 melanoma survival and therapy provides important survival rate context for patients comparing treatment paths.
2026 Breakthrough Treatments Entering the Pipeline
1. Personalized mRNA Cancer Vaccines Moderna and Merck’s mRNA-4157 (V940), combined with pembrolizumab, completed Phase 2b trials showing a 44% reduction in recurrence or death in high-risk melanoma patients. Phase 3 trials are actively enrolling in 2026.
2. Next-Generation TIL Therapy Following the 2025 NIH study, researchers at the National Cancer Institute are expanding TIL therapy trials into pancreatic, esophageal, and colorectal cancers — all notoriously resistant to current treatments.
3. AI-Guided Biomarker Prediction NIH scientists published research in 2025 developing an AI model to predict immunotherapy response from standard blood tests — potentially replacing expensive tissue biopsies for initial patient selection.
4. Bispecific Antibodies A new class of antibodies that simultaneously bind to cancer cells AND T cells, physically bringing immune cells into direct contact with tumors. Multiple FDA approvals came in 2024–2025 for blood cancers, with solid tumor trials underway.
5. Combination Immunotherapy + Chemotherapy Protocols pairing checkpoint inhibitors with targeted chemotherapy are showing synergistic benefits in triple-negative breast cancer and non-small cell lung cancer, significantly outperforming either treatment alone.
Your Action Plan — Is Immunotherapy Right for You?
3 Questions to Ask Your Oncologist Before Starting Immunotherapy
If you or someone you love has been told immunotherapy is an option, bring these three questions to your next appointment:
- “What is my PD-L1 expression score, and what does it mean for my treatment?”
- “Have I been tested for microsatellite instability (MSI) and tumor mutational burden (TMB)?”
- “Does my cancer have an EGFR or ALK mutation that would make targeted therapy a better first choice?”
These three questions can fundamentally change your treatment path — and no competitor’s article tells patients to ask them.
For Allergy Patients: Is Allergen Immunotherapy Worth It?
If you’ve been managing allergies with antihistamines for years without full relief, allergen immunotherapy may offer a long-term solution rather than daily symptom management. Discuss these points with a board-certified allergist:
- The specific allergens driving your symptoms
- Whether subcutaneous shots or sublingual therapy is appropriate
- A realistic 3–5 year treatment commitment for full benefit
For Cancer Patients: Explore Clinical Trial Options
New immunotherapy protocols are enrolling patients across the USA. The National Cancer Institute’s clinical trial search allows you to filter by cancer type, location, and eligibility criteria — and participation is often free of charge for enrolled patients.
If you’re tracking your health during treatment — including weight, fitness, and energy levels — our tools can support you. Use our Sleep Calculator to optimize rest during treatment cycles, and our Water Intake Calculator to maintain proper hydration, which is particularly important during immunotherapy.
💡 Expert Insight: “Immunotherapy has fundamentally changed cancer medicine with the possibility of a cure for cancers once considered completely incurable. A patient with metastatic advanced melanoma today has a 1-in-3 chance of being cured — that’s a dramatic improvement.” — Dr. Svetomir Markovic, MD, PhD, Mayo Clinic Comprehensive Cancer Center
⚠️ Medical Disclaimer: This article is for educational purposes only and does not constitute medical advice. All treatment decisions should be made in consultation with a licensed, board-certified healthcare professional.
Frequently Asked Questions About Immunotherapy
Q1: What is immunotherapy in simple terms?
Immunotherapy is a treatment that activates your own immune system to find and destroy disease — most commonly cancer or allergy triggers — rather than using drugs that attack cells directly.
Q2: Does immunotherapy work for all types of cancer?
No. It works best for cancers with high PD-L1 expression, MSI-H status, or high tumor mutational burden — such as melanoma, lung cancer, bladder cancer, and Hodgkin lymphoma. Biomarker testing determines whether you are likely to respond.
Q3: What are the most common side effects of immunotherapy?
Fatigue, skin rash, diarrhea, nausea, and flu-like symptoms are most common. Rare but serious effects include immune-related lung inflammation (pneumonitis), liver inflammation, and thyroid disorders.
Q4: How is immunotherapy different from chemotherapy?
Chemotherapy destroys all fast-dividing cells, including healthy ones. Immunotherapy activates your immune system to selectively target cancer cells — resulting in a different, often more manageable side effect profile, and a potential lasting immune memory effect.
Q5: What is CAR-T cell therapy?
CAR-T involves removing a patient’s T cells, genetically engineering them to recognize cancer-specific markers, growing them in large quantities in a lab, and returning them to the patient as a highly targeted cancer-fighting force. It is currently most effective against blood cancers.
Q6: How long does immunotherapy treatment last?
Most patients receive IV infusions every 2–3 weeks. Depending on cancer type and response, treatment can last anywhere from several months to 2 or more years. Some patients remain on maintenance therapy indefinitely if they continue to respond.
Q7: What is the success rate of immunotherapy?
Response rates range from 20–69% depending on cancer type and biomarker status. Advanced melanoma patients show 30–40% five-year survival rates with checkpoint inhibitors — compared to under 5% with older treatments. Some patients achieve complete and durable remission.
Q8: Is immunotherapy used for allergies?
Yes. Allergen immunotherapy — through allergy shots or sublingual tablets — gradually desensitizes the immune system to specific triggers such as pollen, dust mites, bee venom, and pet dander. It is a well-established, long-term treatment for allergic rhinitis, asthma, and insect sting allergies.
Q9: How much does immunotherapy cost in the USA in 2026?
Checkpoint inhibitor therapy typically costs $150,000–$250,000 per year. CAR-T cell therapy ranges from $400,000–$500,000 for a single course. Most FDA-approved immunotherapies are covered by Medicare, Medicaid, and major private insurers. Manufacturer assistance programs are available.
Q10: Why doesn’t immunotherapy work for some patients?
Approximately 60–80% of cancer patients don’t respond. “Cold” tumors with low immune infiltration, the absence of key biomarkers like PD-L1 or MSI, and immune-suppressive tumor microenvironments are primary reasons. Combination therapies are being developed to overcome these barriers.
Q11: Can immunotherapy permanently cure cancer?
In select patients, yes. Some individuals with advanced melanoma treated with checkpoint inhibitors in early trials remain cancer-free more than 10 years later. This remains a minority outcome, but it represents the most significant advance in oncology in decades — and research continues to expand who can benefit.
For more on related cancer conditions and treatments, explore our guides on sarcoma cancer survival and detection, skin cancer warning signs, and biopsy results explained.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.











