On This Page – Quick Medical Summary
Melanoma is caused primarily by DNA damage in skin cells — most often triggered by ultraviolet (UV) radiation from the sun or tanning beds. But UV exposure is only one piece of the puzzle. Genetics, skin type, mole count, and even your immune system all play critical roles in who develops this cancer and who doesn’t.
A Story That Changes How You Think About Melanoma
Marcus was 36, athletic, and had no family history of cancer. He didn’t use tanning beds. But a doctor’s visit following a changing mole on his back revealed Stage II melanoma. His biggest risk factor? A pattern of intense summer sunburns throughout his twenties — intermittent, severe, and never taken seriously.
His story is not unusual. Every year, over 100,000 Americans receive a new melanoma diagnosis, according to melanoma statistics tracked through 2026. Understanding what causes melanoma is the first step in stopping it.
How Melanoma Actually Develops — The Root Biology
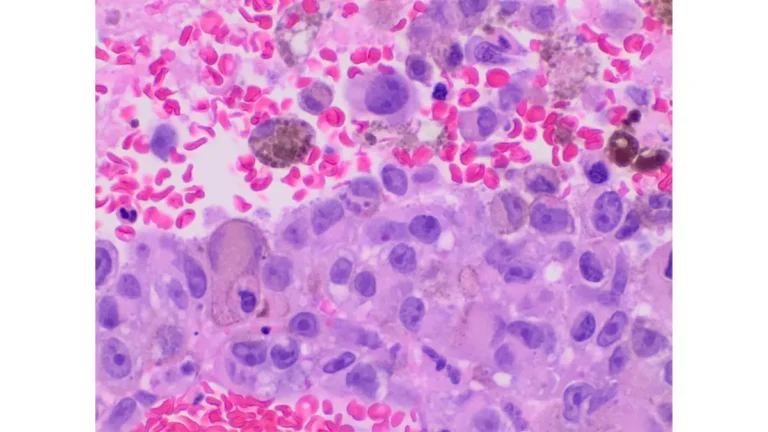
What Are Melanocytes, and Why Do They Turn Cancerous?
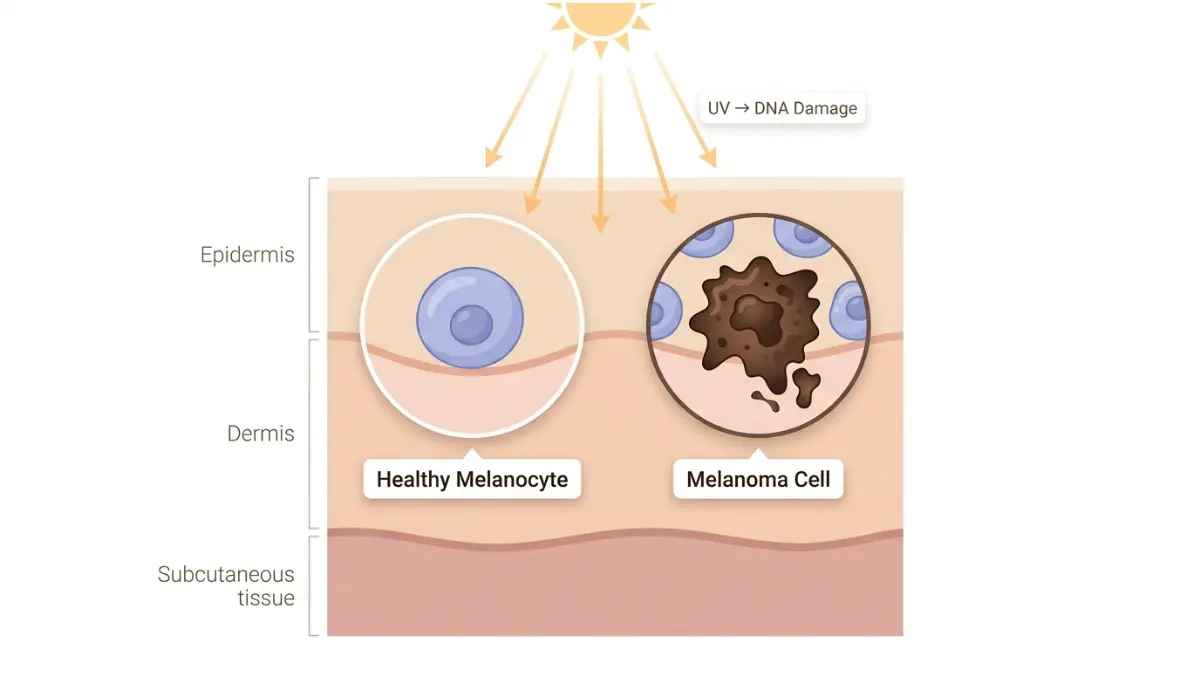
Melanocytes are the specialized cells in your skin that produce melanin — the pigment responsible for skin, hair, and eye color. They sit at the base of the outer skin layer (epidermis) and normally grow in a controlled, orderly way.
When melanocyte DNA becomes damaged, those cells can begin multiplying uncontrollably. That uncontrolled growth is what causes melanoma to develop.
How DNA Damage Triggers the Cancer Process
UV radiation penetrates the skin and chemically alters DNA strands inside melanocytes. Your immune system repairs most of this damage — but not always all of it.
Over time, unrepaired mutations accumulate. When those mutations affect tumor-suppressor genes or growth-control genes, the cell no longer follows normal stop-and-start signals for division. The result: runaway growth that forms a tumor.
The BRAF Mutation: Present in Half of All Melanomas
One of the most clinically important discoveries in modern oncology is the BRAF V600E mutation, found in approximately 50% of all cutaneous melanomas, according to the National Cancer Institute’s melanoma treatment summary. This mutation supercharges cell growth signals, making the cancer more aggressive.
Other key driver mutations include NRAS and NF1 — each defining distinct molecular subtypes of the disease.
💡 What This Means For You: You cannot feel DNA damage occurring. That is precisely why visible changes in your skin — not symptoms like pain — are the earliest signal. Use our Symptom Checker if you’ve noticed any new or changing moles.
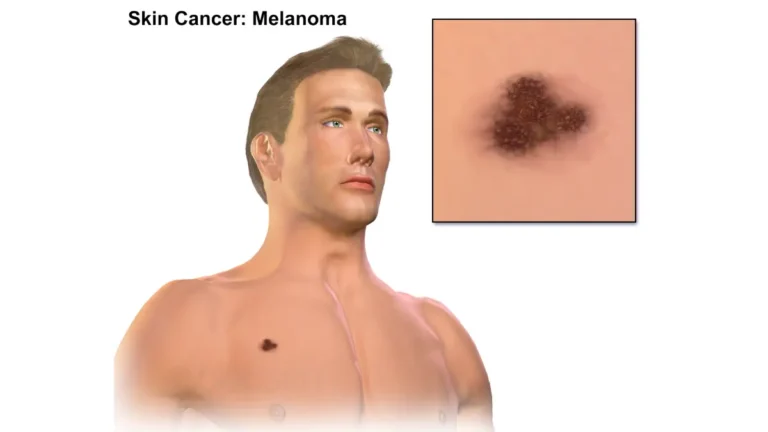
UV Radiation — The #1 Proven Cause of Melanoma
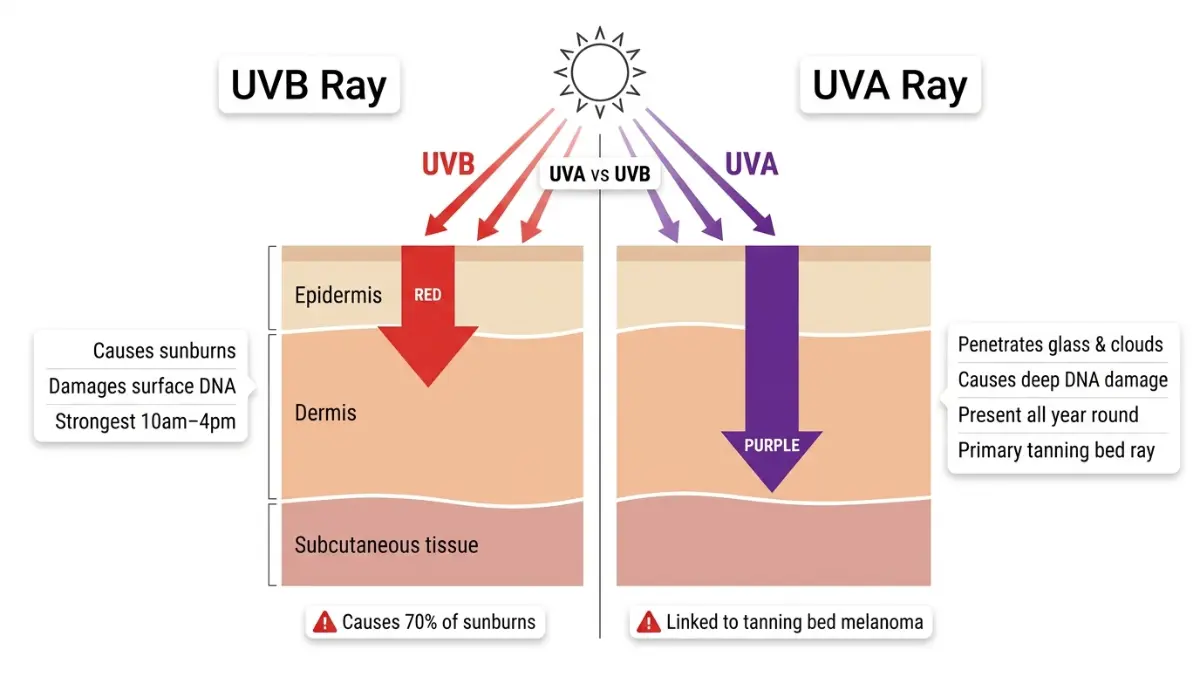
UVA vs. UVB: Which Type Actually Causes Melanoma?
Both types of ultraviolet radiation contribute to melanoma risk — but in different ways.
- UVB rays cause direct DNA damage and are responsible for sunburns and most skin cancers
- UVA rays penetrate deeper into the skin, cause aging damage, and also contribute to melanoma — including through glass and clouds
The Memorial Sloan Kettering Cancer Center’s melanoma prevention guide confirms that UVA exposure from tanning beds is particularly dangerous because it’s concentrated and unregulated.
The Sunburn–Melanoma Link: 5 Sunburns Doubles Your Risk
This is one of the most important — and most underestimated — facts about what causes melanoma:
- Having 5 or more blistering sunburns before age 20 more than doubles your lifetime melanoma risk
- A severe childhood sunburn does not disappear with time — the DNA damage it causes is cumulative
- Sunburns at any age, not just in childhood, increase risk, according to Cancer Research UK’s melanoma risk data
The Intermittent Exposure Paradox (What No Competitor Explains)
This is the finding that surprises most people — and it matters enormously.
Research published in PMC’s epidemiological review of melanoma risk factors reveals:
- Chronic, daily UV exposure (outdoor workers, farmers) shows no increased melanoma risk in meta-analysis (RR: 0.95)
- Intermittent, intense UV exposure — beach holidays, vacation sunburns — is far more strongly linked to melanoma development
- The reason: chronic exposure allows skin to adapt (keratinocyte thickening). Intermittent intense bursts overwhelm repair mechanisms
In plain terms: The office worker who takes two beach holidays a year and gets sunburned may face more melanoma risk than a construction worker with daily sun exposure.
Tanning Beds: An IARC Group 1 Carcinogen
The International Agency for Research on Cancer classifies tanning beds as a Group 1 carcinogen — the same category as tobacco and asbestos. This is not a theoretical risk. The Skin Cancer Foundation’s melanoma risk data confirms that using a tanning bed before age 35 increases melanoma risk by 59%.
In countries like the UK, sunbed use by anyone under 18 is now banned by law.
UV Index: Your Daily Melanoma Risk Level
| UV Index | Risk Level | Action Required |
|---|---|---|
| 0–2 | Low | Basic protection |
| 3–5 | Moderate | SPF 30+, hat recommended |
| 6–7 | High | Limit 10am–4pm exposure |
| 8–10 | Very High | Seek shade, SPF 50+ |
| 11+ | Extreme | Avoid midday outdoors |
💡 What This Means For You: A beach holiday with three severe sunburns may carry more long-term melanoma risk than decades of daily moderate sun exposure. It’s the intensity and suddenness that matters, not just the duration.
Genetic Risk Factors — What Your DNA Reveals
Family History and Melanoma: The Numbers
If one or more first-degree relatives — parent, sibling, or child — has had melanoma, your risk increases significantly. According to the American Cancer Society’s melanoma risk factor overview, approximately 1 in 10 people with melanoma have a family history of the disease.
This risk comes from two sources:
- Shared behavioral patterns — similar sun habits, outdoor lifestyles
- Inherited gene mutations — actual DNA changes passed from parent to child
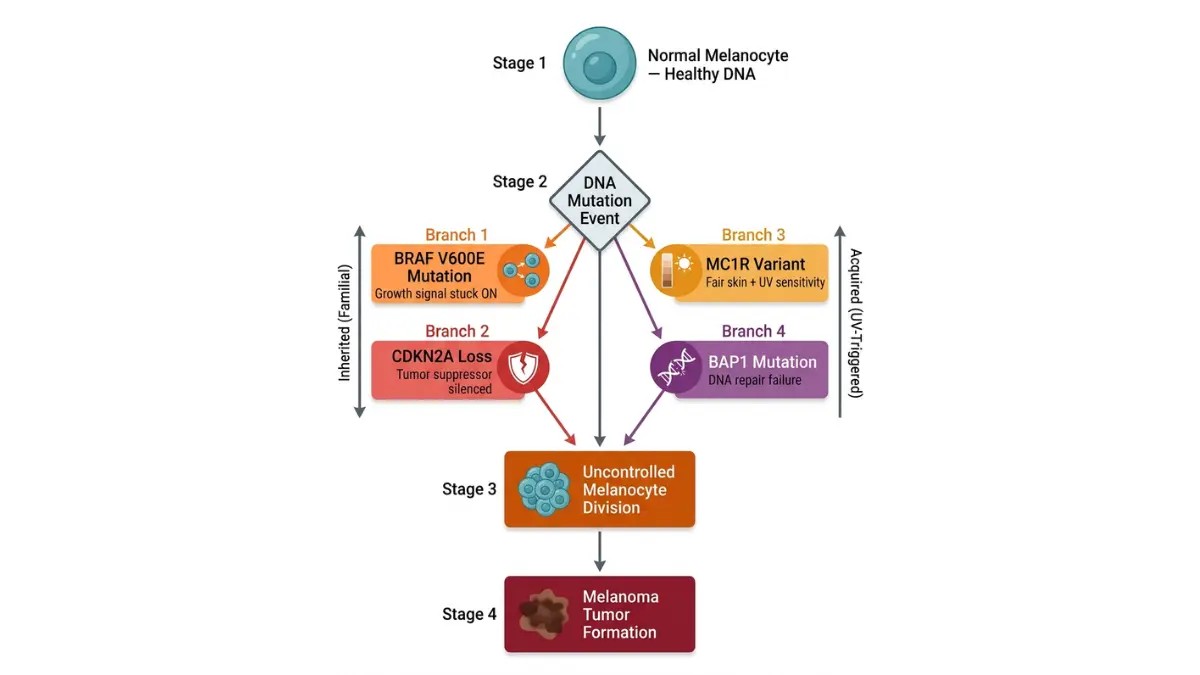
The 4 Key Gene Mutations Explained Simply
| Gene | What It Does | Risk Impact |
|---|---|---|
| CDKN2A | Tumor suppressor — controls cell growth | Very High — found in familial melanoma clusters |
| BAP1 | Controls cell division and DNA repair | High — linked to eye and skin melanoma |
| MC1R | Controls pigment production (fair skin, red hair) | Moderate–High |
| BRAF | Growth signal driver mutation | Present in ~50% of tumors — influences treatment |
If you have a strong family history of melanoma, your doctor may recommend genetic counseling. Our Genetic Risk Assessment Tool can help you evaluate your personal hereditary risk profile.
FAMMM Syndrome: When Entire Families Carry Elevated Risk
Familial Atypical Multiple Mole Melanoma (FAMMM) syndrome occurs in families where members carry CDKN2A mutations and develop many unusual moles (atypical nevi). Members of FAMMM families should begin annual dermatologist screenings from puberty onwards.
The good news: familial melanomas are typically detected earlier because these families are vigilantly monitored — and earlier detection dramatically improves survival rates.
Skin Type and Melanoma: The Fitzpatrick Scale
| Fitzpatrick Type | Description | Melanoma Risk |
|---|---|---|
| Type I | Very fair, red/blonde hair, always burns | Very High |
| Type II | Fair, burns easily, tans minimally | High |
| Type III | Medium, burns moderately | Moderate |
| Type IV | Olive, rarely burns | Low–Moderate |
| Type V–VI | Brown to dark, very rarely burns | Lower — but not zero |
Melanoma in Dark Skin: The Overlooked Risk
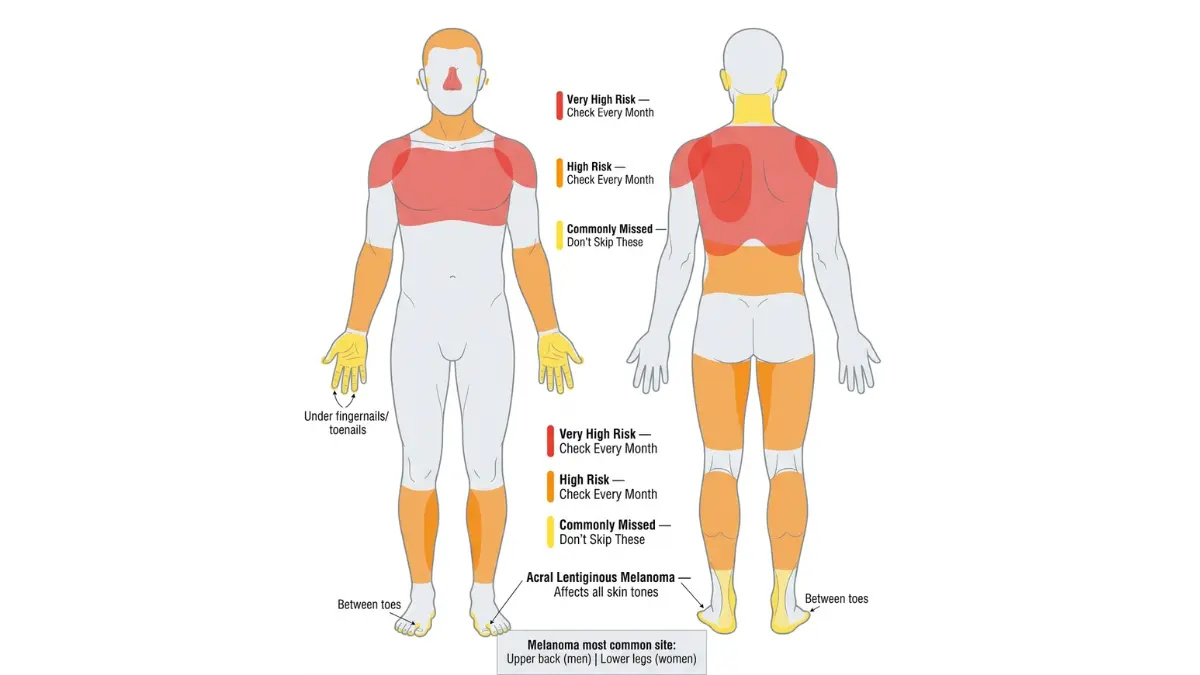
A critical gap in most melanoma content is the failure to address acral lentiginous melanoma (ALM) — a subtype that develops on the palms, soles of feet, and under fingernails or toenails, predominantly affecting people with darker skin tones.
ALM is frequently diagnosed late because neither patients nor clinicians associate dark skin with melanoma risk. It accounts for a disproportionate number of melanoma deaths in Black Americans despite lower overall melanoma incidence. Our detailed guide on subungual (nail) melanoma covers how to recognize this often-missed presentation.
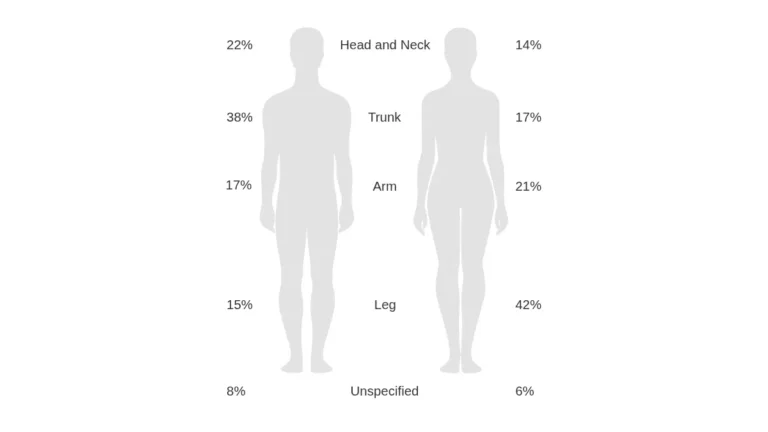
For a broader understanding of where on the body melanoma appears, see our guide on where melanoma appears on the body.
💡 What This Means For You: Melanoma does not discriminate by skin color. If you have dark skin, inspect your palms, soles, and nails regularly.
Hidden & Overlooked Melanoma Risk Factors
Mole Count and Atypical Nevi
The more moles you have, the higher your melanoma risk — even if those moles look normal. Research from PMC’s comprehensive skin cancer risk factor analysis found:
- People with 101–120 moles face nearly 7 times the risk of those with fewer than 15 moles (RR: 6.89)
- The presence of just 5 atypical (irregular) moles increases risk by 6-fold
- Congenital nevi (moles present at birth) that cover large body areas carry significantly elevated risk
Weakened Immune System
Your immune system plays a critical surveillance role — it identifies and destroys abnormal cells before they become tumors. When that surveillance fails, melanoma risk rises sharply.
High-risk groups include:
- Organ transplant recipients on immunosuppressive therapy
- HIV-positive individuals with reduced CD4 counts
- Lymphoma patients or those currently undergoing chemotherapy
- People taking long-term corticosteroids
Alcohol: The Emerging Risk Factor Nobody Talks About
This is one of the most significant and least discussed findings in melanoma research. A peer-reviewed analysis found that high alcohol consumption (>3.08g/day of spirits) is associated with a 47% increased melanoma risk compared to minimal intake.
The mechanism may involve alcohol’s suppressive effect on immune function and its ability to increase skin photosensitivity to UV radiation. This risk factor is absent from virtually all mainstream melanoma content — including the top-ranked competitors.
Altitude and Geographic Location
UV radiation intensity increases by approximately 4% for every 1,000 feet of elevation. This places pilots, flight crew, and residents of high-altitude cities (Denver, Salt Lake City, parts of Colorado) at elevated baseline risk compared to sea-level populations.
Globally, WHO’s ultraviolet radiation data shows Australia leads the world at 60 new melanoma cases per 100,000 population, compared to 30 per 100,000 in the USA.
Prior Skin Cancer History
If you’ve already had melanoma, your risk of a second primary melanoma is significantly elevated. This also applies to a history of basal cell carcinoma or squamous cell carcinoma — their presence signals cumulative UV damage to the same skin. Review the 12 warning signs of skin cancer to understand the full spectrum of risk signals.
💡 What This Means For You: Risk is multifactorial. UV exposure, your mole count, immune health, alcohol intake, and where you live all contribute. One risk factor alone rarely tells the whole story.
Modifiable vs. Non-Modifiable Risk Factors — Your Master Control Table
Which Melanoma Risk Factors Can You Actually Control?
Understanding this distinction is critical for actionable risk reduction.
| Risk Factor | Modifiable? | Risk Severity |
|---|---|---|
| UV exposure from sun | ✅ Yes | ⚠️ Very High |
| Tanning bed use | ✅ Yes | ⚠️ Very High |
| Sunscreen & protective clothing habits | ✅ Yes | ⚠️ High |
| Alcohol consumption | ✅ Yes | 🔶 Moderate |
| Fair / light skin type (Fitzpatrick I–II) | ❌ No | ⚠️ High |
| Family history / inherited genetics | ❌ No | ⚠️ High |
| CDKN2A / BRAF gene mutations | ❌ No | ⚠️ Very High |
| Mole count | ❌ No (monitoring: Yes) | ⚠️ High |
| Weakened immune system | ⚠️ Partial | 🔶 Moderate–High |
| Age (>50, especially men) | ❌ No | 🔶 Moderate |
| Geographic location / altitude | ⚠️ Partial | 🔶 Moderate |
Are You at Low, Moderate, High, or Very High Risk?
Very High Risk — See a dermatologist annually or more:
- 3+ first-degree relatives with melanoma
- Confirmed CDKN2A or BAP1 mutation
- History of melanoma + multiple atypical moles
- Organ transplant recipient with fair skin
High Risk — Annual skin check recommended:
- Fitzpatrick Type I or II skin
- 50+ moles or 5+ atypical moles
- 5 or more blistering sunburns in lifetime
- Personal history of any skin cancer
Moderate Risk — Biennial screening + monthly self-exams:
- Fitzpatrick Type III with UV-heavy lifestyle
- Single first-degree relative with melanoma
- Immunosuppressive therapy user
Low Risk — Monthly self-exams + sun protection habits:
- Dark skin tone with no family history
- Minimal UV exposure history
- No atypical moles
For a personalized assessment, use our Genetic Risk Assessment Tool to evaluate your hereditary risk profile.
Prevention, Early Detection, and Your 2026 Action Plan
Sun Protection That Actually Works
The American Academy of Dermatology’s melanoma screening guidance recommends a layered sun protection approach, not SPF alone:
- Broad-spectrum SPF 50+ applied 30 minutes before sun exposure — reapplied every 2 hours
- UPF 50+ clothing for prolonged outdoor time (more reliable than sunscreen alone)
- Avoid peak UV hours — 10am to 4pm, particularly between April and September in the USA
- Never use tanning beds — no safe dose exists
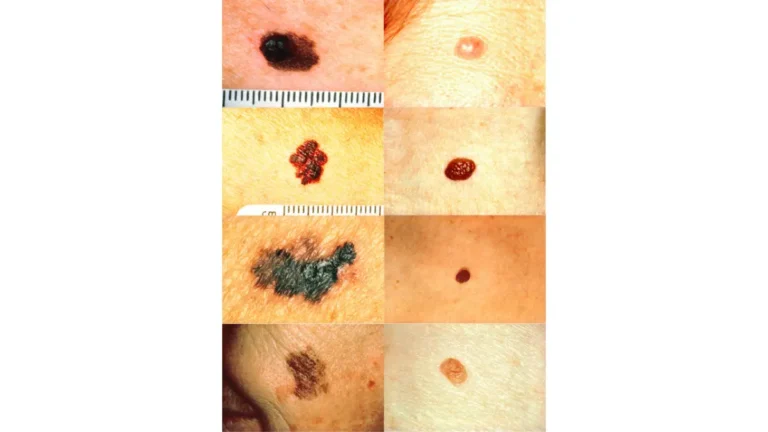
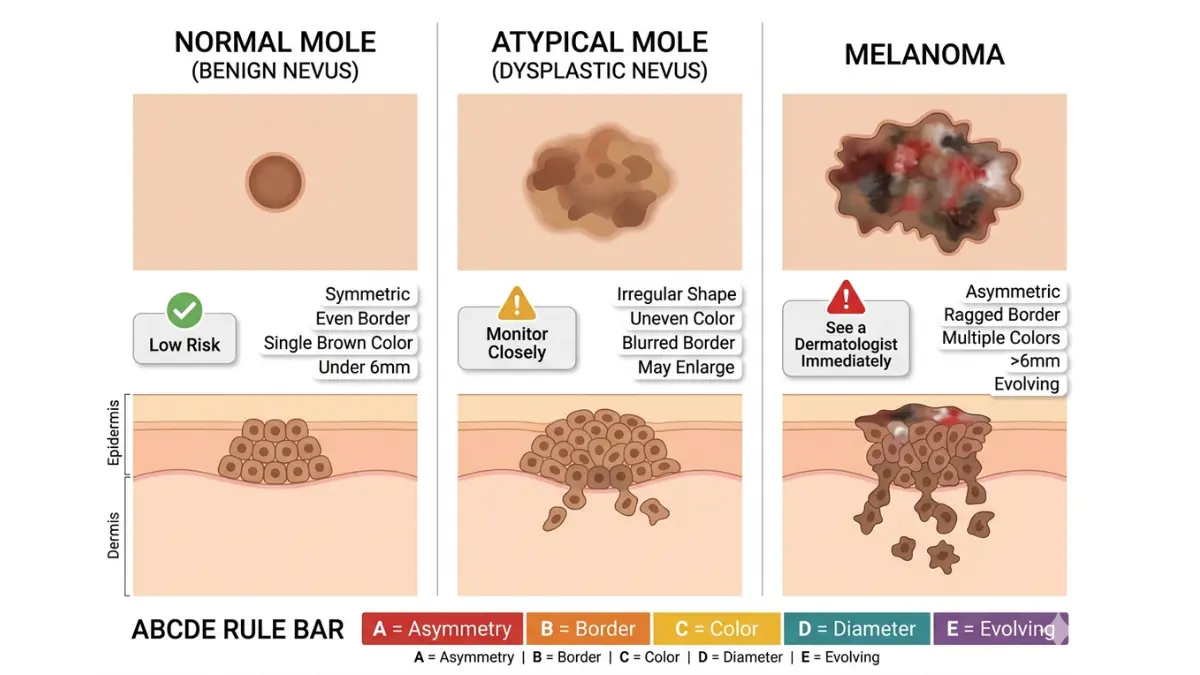
The ABCDE Rule: Your Home Melanoma Detection Checklist
Every mole on your body should be assessed using this framework, consistent with Mayo Clinic’s melanoma symptom criteria:
- A — Asymmetry: One half doesn’t match the other
- B — Border: Edges are ragged, notched, or blurred
- C — Color: Multiple shades — brown, black, red, white, or blue
- D — Diameter: Larger than 6mm (pencil eraser size)
- E — Evolving: Any change in size, shape, color, or texture
For a deeper guide on these visual warning signs, see our full breakdown of melanoma ABCDE warning signs and moles.
Your Monthly Skin Self-Exam: Step-by-Step
- Use a full-length mirror in good lighting
- Examine face, scalp (use a comb), neck, ears
- Check chest, abdomen, and both sides of arms
- Use a hand mirror to examine back and buttocks
- Inspect legs front and back — including between toes and soles
- Check nails (both finger and toe) for dark streaks
If you notice anything unusual, cross-reference with our guide on melanoma warning signs and symptoms and consult a dermatologist promptly.
Dermatologist Screening Schedule by Risk Level
| Risk Level | Recommended Frequency |
|---|---|
| Low | Self-exam monthly; professional check every 2–3 years |
| Moderate | Self-exam monthly; annual professional skin check |
| High | Self-exam monthly; dermatologist every 6 months |
| Very High | Self-exam monthly; specialist review every 3–6 months |
For a comprehensive understanding of how melanoma progresses when undetected, read our complete melanoma symptoms, stages, and treatment guide.
💡 What This Means For You: Most melanomas are either preventable or detectable at an early, highly treatable stage. The actions you take today — sun protection, regular self-exams, and knowing your risk — can directly change your outcome.
⚠️ Disclaimer: This article is for educational and informational purposes only. It does not replace professional medical advice, diagnosis, or treatment. Always consult a qualified dermatologist or oncologist regarding any skin concerns.
Frequently Asked Questions About Melanoma Causes
1. What is the #1 cause of melanoma?
Ultraviolet (UV) radiation — from sun exposure and tanning beds — is the primary cause of melanoma. It damages DNA in melanocytes, triggering uncontrolled cell growth.
2. Can you get melanoma without sun exposure?
Yes. Acral lentiginous melanoma (ALM) develops on palms, soles, and under nails — areas not exposed to sun. Genetic mutations can also cause melanoma independent of UV exposure.
3. Does one bad sunburn cause melanoma?
A single severe sunburn doesn’t guarantee melanoma, but it does contribute to cumulative DNA damage. Five or more blistering sunburns more than double lifetime risk.
4. Can tanning beds really cause melanoma?
Absolutely. The IARC classifies tanning beds as Group 1 carcinogens. Using them before age 35 raises melanoma risk by 59%.
5. Is melanoma hereditary?
Approximately 10% of melanomas involve inherited gene mutations. CDKN2A and BAP1 mutations are the most significant hereditary risk factors.
6. What gene mutation most commonly causes melanoma?
BRAF V600E is the most common driver mutation, found in ~50% of tumors. CDKN2A is the primary hereditary mutation linked to familial melanoma.
7. Can people with dark skin get melanoma?
Yes. While overall melanoma incidence is lower, acral lentiginous melanoma (ALM) — which appears on palms, soles, and nails — disproportionately affects people with darker skin tones and is often diagnosed later.
8. At what age does melanoma risk peak?
The mean age at melanoma diagnosis is 57. However, melanoma is one of the most common cancers in adults under 40, particularly women in their 20s.
9. Does alcohol increase melanoma risk?
Research indicates that high spirits consumption is associated with up to a 47% increased melanoma risk — likely through immune suppression and increased UV sensitivity.
10. How many moles is considered high risk for melanoma?
Having more than 50 moles is associated with elevated risk. Having 5 or more atypical (irregular) moles increases risk by approximately 6-fold.
11. How can I check my personal melanoma risk?
Start with our Genetic Risk Assessment Tool for a hereditary risk profile, and use our Symptom Checker if you’ve noticed any skin changes. Then consult a board-certified dermatologist for professional evaluation.
Related Articles You Should Read Next:
- Amelanotic Melanoma: The Skin Cancer That Doesn’t Look Like Cancer
- Stage 4 Melanoma: Survival Rates and Latest Therapies
- Melanoma vs. Skin Cancer: Key Differences Explained
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.