On This Page – Quick Medical Summary
Melanoma is diagnosed through a structured, step-by-step process: a clinical skin exam using the ABCDE rule, dermoscopy to magnify suspicious lesions without cutting the skin, and a biopsy to confirm cancer under a microscope. Catching melanoma early — ideally at Stage I — gives you a 97% five-year survival rate. Missing it until Stage IV drops that figure to just 20%.
This guide explains exactly what happens at every step, from your first appointment to understanding your pathology report.
The First Sign — How Doctors Spot Melanoma Before Any Test
The ABCDE Rule: What Dermatologists Check First
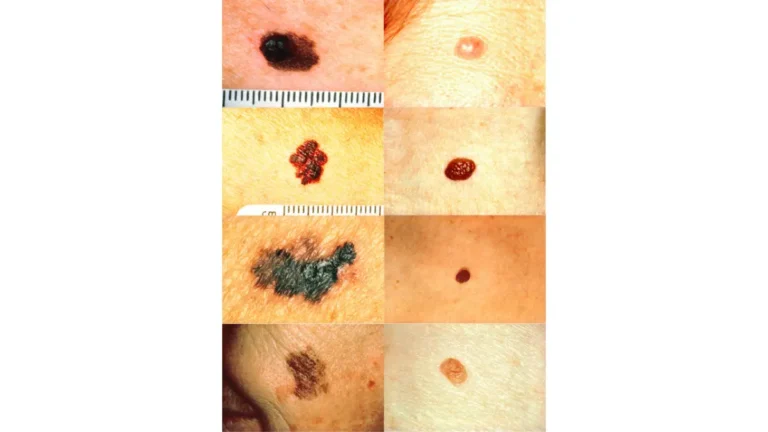
When melanoma skin cancer diagnosis begins, it starts with the human eye — specifically, a trained dermatologist performing a full-body clinical skin exam. The foundation of this exam is the ABCDE rule, the globally accepted framework for evaluating suspicious moles and pigmented lesions.
Understanding the warning signs before your appointment is essential. Our in-depth guide on melanoma warning signs and symptoms covers every visual indicator doctors look for.
| ABCDE Criterion | What It Means | Red Flag Example |
|---|---|---|
| A — Asymmetry | One half doesn’t match the other | Irregular oval shape |
| B — Border | Ragged, notched, or blurred edges | Scalloped or poorly defined border |
| C — Color | Multiple shades in one mole | Mix of brown, black, red, and white |
| D — Diameter | Larger than 6mm (size of a pencil eraser) | Any mole growing beyond 6mm |
| E — Evolving | Any change in size, shape, or color | New itching, bleeding, or color shift |
For a complete visual breakdown of the ABCDE criteria, our dermatologist-reviewed article on melanoma ABCDE signs and moles explains each criterion with clinical examples.

Marcus’s Story: Why “Just a Mole” Nearly Cost Him Everything
Marcus, a 44-year-old construction worker from Texas, noticed a dark spot on his upper back that had been slowly changing color for eight months. He assumed it was a harmless freckle. His physician, during a routine checkup, flagged it immediately using the ABCDE criteria. It was Stage IIA melanoma.
This is not unusual. According to the CDC’s skin cancer data, over 100,000 Americans are diagnosed with invasive melanoma annually — and a significant portion are detected during unrelated doctor visits, not dedicated skin checks.
What Happens at Your First Dermatology Appointment
- The dermatologist examines your entire body surface, including the scalp, between toes, and under nails
- You’ll be asked about personal history of sunburn, tanning bed use, and family history of melanoma
- Any suspicious lesion is flagged for closer evaluation with dermoscopy
- The American Academy of Dermatology recommends annual full-body skin checks for anyone with more than 50 moles or a family history of skin cancer
Dermoscopy — The Magnifying Tool That Sees What the Naked Eye Misses
What Is Dermoscopy and How Does It Work?
Dermoscopy (also called dermatoscopy or epiluminescence microscopy) is a non-invasive diagnostic technique that uses a hand-held device — a dermoscope — equipped with polarized light and 10x magnification. It eliminates surface light reflection, allowing doctors to visualize structures beneath the skin’s surface that are completely invisible to the naked eye.
Before dermoscopy, skilled dermatologists diagnosed melanoma correctly about 60% of the time. With dermoscopy, that accuracy rises to 75–84%, according to a landmark systematic review published at NCBI/StatPearls. A 2001 meta-analysis found dermoscopy improved diagnostic odds from 16:1 to 76:1 compared to naked-eye examination alone.

The 3 Dermoscopy Checklists Doctors Use
Dermatologists apply structured scoring systems to standardize their assessment:
3-Point Checklist (most used globally):
- Structural asymmetry
- Atypical pigment network (thickened, irregular branches)
- Blue-white structures (blue-gray areas over dense pigment)
→ Two or more of these present = biopsy strongly recommended
7-Point Checklist (major criteria):
- Atypical pigment network
- Blue-whitish veil
- Atypical vascular pattern
Minor criteria include: Irregular streaks, irregular dots/globules, irregular blotches, and regression structures.
The NCI’s melanoma resource confirms that trained dermoscopy use in primary care settings significantly improves both sensitivity and the referral accuracy rate for high-risk lesions.
Digital Dermoscopy and AI: The 2026 Revolution
The most significant advancement in melanoma diagnosis right now is AI-assisted digital dermoscopy. High-resolution imaging systems now capture standardized lesion photographs over time, with machine learning algorithms detecting subtle changes that even expert dermatologists miss.
Recent studies show AI dermoscopy models achieving 84–91% diagnostic accuracy — matching or exceeding trained specialists in certain high-volume settings. Our detailed report on melanoma AI screening advances in 2026 explains how these tools are changing early detection outcomes.
If you’ve noticed a suspicious mole and aren’t sure whether it warrants a doctor visit, start with our free Symptom Checker to assess your risk level before booking an appointment.
When Dermoscopy Is NOT Enough
Dermoscopy screens for melanoma — it does not confirm it. A biopsy is always required for definitive diagnosis in the following scenarios:
- Any lesion scoring positive on dermoscopy checklists
- Amelanotic melanoma (no pigment, appears pink or skin-colored)
- Nodular melanoma with limited surface features
- Lesions on acral sites (palms, soles, nails) requiring specialist evaluation
The Melanoma Biopsy — Every Type Explained Clearly
Why Biopsy Is the Only Confirmed Diagnosis Method
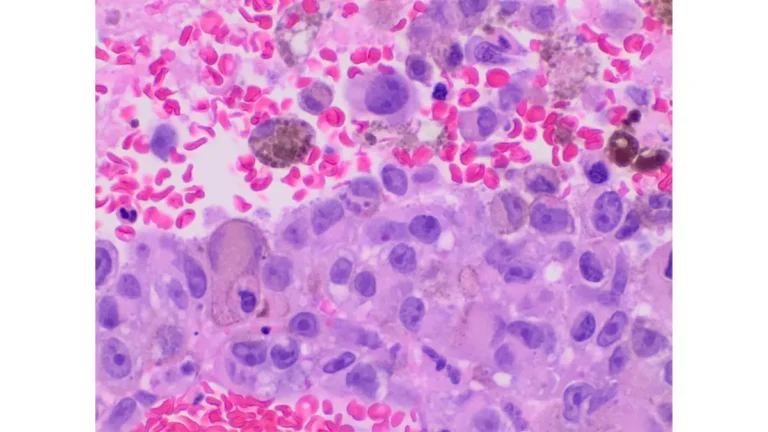
Dermoscopy can identify suspicious lesions with high accuracy, but histopathological examination — analysis of actual tissue under a microscope — is the gold standard for confirming melanoma diagnosed. No imaging, blood test, or clinical exam alone can replace it.
Understanding what causes melanoma and your personal risk profile is critical before your biopsy. Our comprehensive guide on what causes melanoma and its risk factors details who is most vulnerable.
If you want to assess your inherited genetic risk before or after diagnosis, our Genetic Risk Assessment Tool provides a personalized risk profile based on your family history and personal factors.
4 Types of Melanoma Biopsy Compared
| Biopsy Type | Depth | Best For | Stitches? | Scar Risk |
|---|---|---|---|---|
| Shave Biopsy | Superficial layers only | Low-suspicion or very thin lesions | No | Low |
| Punch Biopsy | Full skin depth (circular cut) | Moderate suspicion, smaller lesions | Yes | Moderate |
| Excisional Biopsy | Full thickness + narrow margin | Preferred for suspected melanoma | Yes | Moderate |
| Incisional Biopsy | Partial sample of large lesion | Large lesions where full excision isn’t feasible | Yes | Moderate |
The American Cancer Society’s biopsy guide confirms that excisional biopsy — removing the entire lesion with a small margin — is the preferred approach for most suspected melanomas because it provides the most complete tissue sample for Breslow thickness measurement.

What Actually Happens During a Melanoma Biopsy
Here’s the step-by-step experience for a typical excisional biopsy:
- Local anesthetic injection — A small needle numbs the site (rated 2/10 discomfort by most patients)
- Lesion removal — The dermatologist removes the mole and a thin margin of surrounding skin
- Closure — Stitches or steri-strips close the wound (stitches removed in 7–14 days)
- Sample labeling — The tissue sample is sent to a pathology lab
- Aftercare — Keep the site clean and dry; mild soreness for 2–3 days is normal
Sentinel Lymph Node Biopsy — When Cancer May Have Spread
If your initial biopsy confirms melanoma and the tumor is thicker than 1mm, your oncologist may recommend a sentinel lymph node biopsy (SLNB). This procedure identifies the first lymph node(s) that drain from the melanoma site. If melanoma cells are found there, the cancer has likely spread beyond the original lesion.
The Skin Cancer Foundation explains that SLNB is a key staging tool and guides decisions about further surgery, adjuvant immunotherapy, and follow-up imaging.
Your Pathology Report Decoded — Plain English
How Long Do Melanoma Biopsy Results Take?
- Standard processing: 7–14 business days
- Rush/urgent processing: 3–5 days (requested for large or rapidly changing lesions)
- Complex cases (immunohistochemistry needed): Up to 21 days
This waiting period is one of the most anxiety-inducing parts of the diagnostic process. Our article on biopsy results timelines and what to expect walks you through exactly what happens inside the pathology lab during this period.
Understanding Your Pathology Report — Plain English
Most patients receive a report full of clinical terms that feel overwhelming. Here is what each key term means:
| Pathology Term | Plain English Meaning | Why It Matters |
|---|---|---|
| Breslow Thickness | How deep the melanoma grew (in mm) | Primary factor in determining stage and surgery margin width |
| Clark Level | Which skin layer was invaded (I–V) | Older system, still referenced in some reports |
| Mitotic Rate | How fast cancer cells are dividing | Higher rate = more aggressive behavior |
| Ulceration | Surface skin breakdown over the tumor | Automatically upstages the melanoma |
| Clear Margins | No cancer cells found at tissue edge | Suggests complete removal during biopsy |
| Positive Margins | Cancer cells present at the tissue edge | Re-excision surgery will be recommended |
For a full breakdown of how to read your complete pathology report, our decoded pathology report guide covers every term in the same plain-English format.
According to the NCI’s pathology reports fact sheet, patients have the right to request a second pathology opinion — especially important for borderline or ambiguous melanoma cases.
What Happens the Moment Your Biopsy Comes Back Positive
- Your dermatologist or oncologist calls you (usually within 24 hours of results availability)
- A follow-up appointment is scheduled immediately
- Wide local excision (WLE) is typically the next surgical step, even if the biopsy removed the entire lesion
- Referral to a melanoma specialist or surgical oncologist is arranged
- Depending on Breslow thickness and stage, imaging tests may be ordered
The Cancer Research UK melanoma diagnosis guide notes that most Stage I–II melanomas are treated surgically with curative intent — meaning the goal is complete eradication, not management.
Staging, Imaging, and What Comes After Diagnosis
How Melanoma Is Staged After Biopsy Confirmation
Melanoma staging is based on Breslow thickness, presence of ulceration, mitotic rate, lymph node involvement, and distant metastasis. Understanding your stage determines your entire treatment pathway.
| Stage | Breslow Thickness | Spread Status | 5-Year Survival Rate |
|---|---|---|---|
| Stage I | < 1–2 mm | Skin only, no spread | 92–97% |
| Stage II | > 2 mm | Deeper skin invasion, possible ulceration | 53–82% |
| Stage III | Any | Spread to regional lymph nodes | 40–78% |
| Stage IV | Any | Distant organs (lung, liver, brain) | 15–20% |
Our comprehensive pillar article on melanoma symptoms, stages, and treatment covers every stage in full clinical detail, including treatment options at each point.
For patients already facing advanced disease, our Stage IV melanoma survival and therapy guide covers immunotherapy and targeted therapy outcomes with 2026 data.

When Are CT Scans, MRIs, and PET Scans Ordered?
Imaging tests are not routine for early-stage melanoma. They are typically ordered when:
- Breslow thickness exceeds 4mm
- Lymph node involvement is confirmed or suspected
- Symptoms suggest possible distant spread (persistent cough, bone pain, neurological changes)
| Imaging Test | What It Shows | Typical Wait Time |
|---|---|---|
| CT Scan | Chest, abdomen, pelvis organ involvement | Same day – 3 days |
| MRI | Brain and spinal cord metastases | 3–7 days |
| PET Scan | Full-body cancer cell activity | 5–10 days |
The NCCN Melanoma Patient Guidelines specify that PET-CT is recommended for Stage III+ melanoma to assess systemic spread before treatment decisions are finalized.
The NHS UK melanoma diagnosis pathway mirrors US protocols for Stages I–II but recommends earlier staging imaging for high-risk anatomical sites such as the scalp and subungual (nail) melanoma.
Take Action — Self-Exam, High-Risk Groups, and Appointment Prep
How to Perform a Monthly Skin Self-Exam
Dermatologists recommend checking your skin once a month, in good lighting, using a full-length and hand-held mirror. Follow this body-map approach:
- Face, scalp, ears — Use a comb to part hair and examine scalp
- Neck, chest, abdomen — Check front and sides
- Arms, underarms, hands — Include fingernails and between fingers
- Back and buttocks — Use a hand mirror or ask a partner to check
- Legs and feet — Check soles, between toes, and toenails
Any mole that changes within 4–6 weeks warrants immediate medical review.
Who Is at Highest Risk in 2026?
According to WHO’s global cancer fact sheet and US melanoma data, high-risk individuals include:
- Fair-skinned individuals with light hair and eyes
- Anyone with more than 50 moles or atypical (dysplastic) nevi
- Personal or family history of melanoma
- History of blistering sunburns, especially before age 18
- Immunosuppressed patients (organ transplant recipients, those on biologics)
- Older adults 65+ — melanoma incidence peaks in this group
- Individuals with significant occupational UV exposure
Our melanoma 2026 statistics article breaks down the latest incidence data by age, gender, and US state.
5 Questions to Ask Your Dermatologist
Before or after your appointment, prepare these questions:
- “What dermoscopy scoring system are you using to evaluate this lesion?”
- “If you recommend a biopsy, which type will be most appropriate for this lesion?”
- “How long will it take to receive my pathology results, and how will they be communicated?”
- “If results are positive, what does the next 30 days look like in terms of treatment?”
- “Should I have my immediate family members screened given my diagnosis?”
FAQs: Melanoma Diagnosis — People Also Ask
1. Can melanoma be diagnosed without a biopsy?
No. Dermoscopy can strongly suggest melanoma, but a skin biopsy with histopathological analysis is the only method that definitively confirms melanoma diagnosed.
2. How long does it take to get melanoma biopsy results?
Standard results return in 7–14 business days. Rush processing can deliver results in 3–5 days for urgent cases.
3. Is dermoscopy painful?
No. Dermoscopy is entirely non-invasive. The dermoscope is simply held against the skin surface — no cutting, no injection, no discomfort.
4. What does a melanoma biopsy feel like?
The local anesthetic injection causes a brief sting (2–3 seconds). The biopsy itself is painless. Mild soreness lasting 2–3 days afterward is normal.
5. Can a blood test detect melanoma?
No standard blood test diagnoses melanoma. However, an LDH (lactate dehydrogenase) blood test is used in Stage IV melanoma to track disease spread and treatment response.
6. What is Breslow thickness in melanoma?
Breslow thickness measures how deeply the melanoma has grown into the skin, reported in millimeters. It is the single most important factor in determining melanoma stage and prognosis.
7. What happens immediately after melanoma is confirmed?
A wide local excision surgery is typically scheduled, followed by staging evaluation, possible sentinel lymph node biopsy, and an oncology referral depending on the stage.
8. Can melanoma be mistaken for a normal mole?
Yes. Early melanoma, especially amelanotic (non-pigmented) melanoma, frequently resembles benign skin lesions. Dermoscopy significantly reduces misdiagnosis rates.
9. Is excisional biopsy the best option for melanoma?
Yes, in most cases. Excisional biopsy removes the entire lesion and provides the complete tissue depth needed to measure Breslow thickness accurately.
10. What stage is melanoma most often at when first diagnosed in the US?
Approximately 84% of melanomas in the US are diagnosed at Stage I or Stage II (localized), according to SEER database data — underlining the value of routine skin checks.
11. Can melanoma spread before it is diagnosed?
Yes. Melanoma can spread to regional lymph nodes or distant organs while the primary skin tumor is still very small. This is why early dermoscopy evaluation and prompt biopsy are critical.
⚠️ Medical Disclaimer: This article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a board-certified dermatologist or oncologist for evaluation of any suspicious skin lesion. If you notice a changing mole, do not delay seeking professional evaluation.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.