On This Page – Quick Medical Summary
When James, a 61-year-old firefighter from Houston, Texas, was told he needed lung cancer surgery, his first question was blunt: “Will I ever breathe normally again?” His thoracic surgeon’s answer surprised him — and it may surprise you too.
Lung cancer surgery is not a one-size-fits-all procedure. In 2026, patients have access to multiple surgical options — from minimally invasive robotic techniques to life-saving pneumonectomies — each with dramatically different recovery timelines and survival outcomes.
This guide explains every type of lung cancer surgery, who qualifies, what the latest 2025–2026 survival data actually shows, and exactly what week-by-week recovery looks like. If you or someone you love is facing a thoracic surgery decision, this is the most complete resource available.
If you’ve recently noticed new respiratory symptoms, use our free Symptom Checker to document them before your surgical consultation.
Types of Lung Cancer Surgery — Every Option Explained
What Is Lung Cancer Surgery?
Lung cancer surgery involves the surgical removal of cancerous tissue from the lung. According to the National Cancer Institute, surgery remains the most effective curative treatment for early-stage non-small cell lung cancer (NSCLC).
The right operation depends on tumor size, location, cancer stage, and your pulmonary reserve — meaning how much lung function you can afford to lose. Understanding your full options before surgery is not optional. It’s essential.
Lobectomy — The Gold Standard for Lung Cancer Surgery
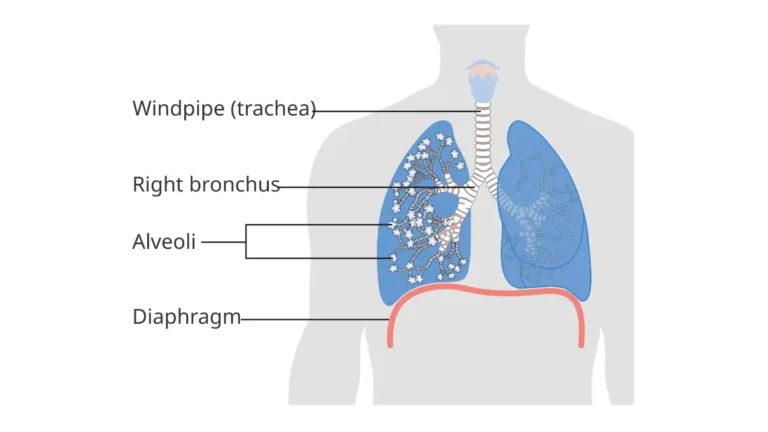
A lobectomy removes one entire lobe of the lung. Your lungs have five lobes — three on the right, two on the left.
Lobectomy is the most commonly performed lung cancer surgery worldwide and is considered the gold standard for Stage I and Stage II NSCLC. It effectively removes tumors while preserving healthy lung tissue in the remaining lobes.
It can be performed using three approaches: open thoracotomy (large chest incision), VATS (video-assisted thoracoscopic surgery via small incisions), or RATS (robotic-assisted thoracoscopic surgery).
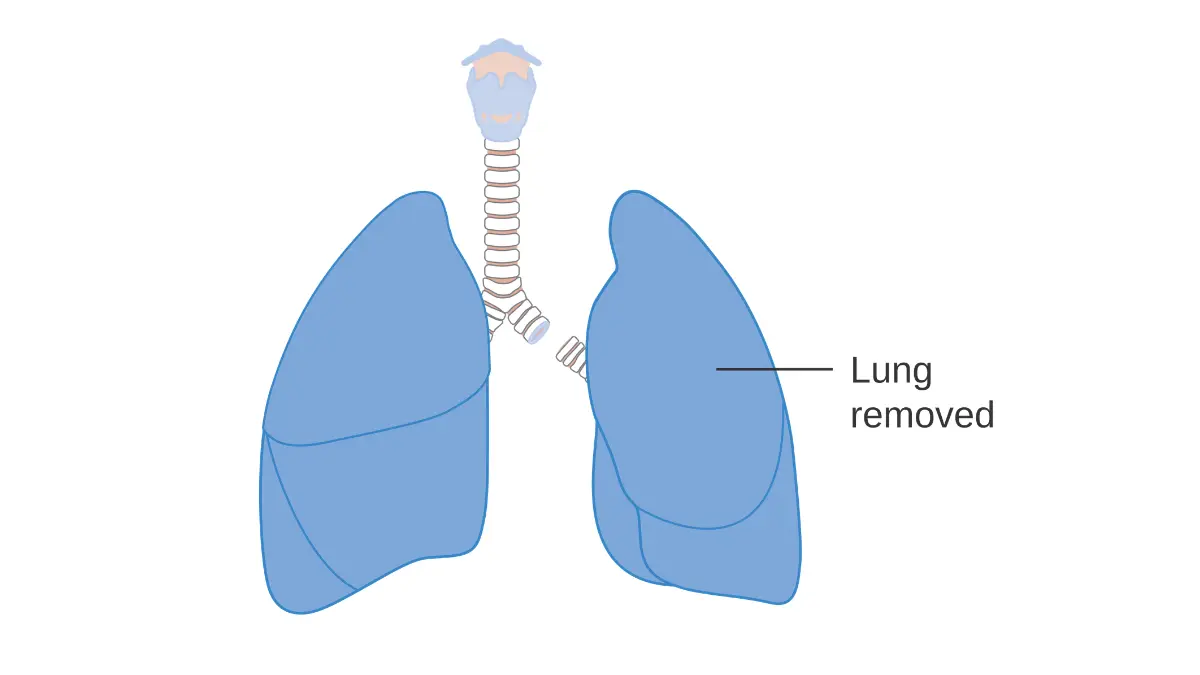
Pneumonectomy — When the Entire Lung Must Go
A pneumonectomy removes the entire lung affected by cancer. It is reserved for centrally located tumors or cases where a lobectomy cannot achieve clear surgical margins.
This is the most aggressive lung cancer surgery option, with higher operative risks and a longer recovery. However, for the right patient with locally advanced disease, it can be curative.
Right pneumonectomy carries higher risks than left pneumonectomy because the right lung handles approximately 55% of total lung function.
Sleeve Lobectomy — The Lung-Saving Alternative
A sleeve lobectomy removes a lobe plus a portion of the bronchus (airway), then reconnects the remaining airway. It is used when tumors are located near a central bronchus.
The critical advantage: sleeve lobectomy preserves far more lung function than pneumonectomy. A 2022 meta-analysis published in NIH PubMed Central confirmed that sleeve lobectomy patients had a 37% better overall survival than pneumonectomy patients (HR 0.63).
Segmentectomy & Wedge Resection — For Smaller Tumors
Segmentectomy removes one or more anatomic segments of a lobe. Wedge resection removes a small, wedge-shaped piece of peripheral lung tissue. Both are lung-sparing procedures suited for patients with reduced pulmonary function or very small peripheral tumors.
Master Surgical Comparison Table
| Surgery Type | What’s Removed | Best For | Hospital Stay | Recovery |
|---|---|---|---|---|
| Lobectomy | One lobe | Stage I–II NSCLC | 3–5 days | 4–6 weeks |
| Pneumonectomy | Entire lung | Central/large tumors | 7–10 days | 3–6 months |
| Sleeve Lobectomy | Lobe + bronchus section | Central airway tumors | 5–7 days | 6–8 weeks |
| Segmentectomy | 1–4 lung segments | Small tumors, low PFT | 2–4 days | 3–4 weeks |
| Wedge Resection | Small tissue wedge | Tiny peripheral tumors | 1–3 days | 2–3 weeks |
For a deeper understanding of your diagnosis before surgery, read our guide on Lung Cancer Stages Explained and the complete overview of Lung Cancer Treatment Options available in 2026.
Am I a Candidate for Lung Cancer Surgery?
Who Qualifies for Lung Cancer Surgery? (And Who Doesn’t)
Not every lung cancer patient is a surgical candidate. According to the American Lung Association, surgical eligibility depends on cancer stage, overall health, and lung function reserve.
The decision is made by a multidisciplinary tumor board — a team of thoracic surgeons, oncologists, pulmonologists, and radiologists who review each case collectively.
Surgical Eligibility Criteria — The Full Checklist
You may be a surgical candidate if:
- ✅ Diagnosed with Stage I, II, or select Stage IIIA NSCLC
- ✅ Predicted post-operative FEV1 (lung function) above 40–60% threshold
- ✅ No confirmed distant metastasis on PET-CT scan
- ✅ Medically fit for general anesthesia
- ✅ No uncontrolled cardiovascular disease
- ✅ DLCO (diffusing capacity) within acceptable pre-operative range
Surgery is typically NOT an option if:
- ❌ Stage IIIB or Stage IV disease with distant spread
- ❌ Severely reduced pulmonary function (ppoFEV1 < 30%)
- ❌ Recent myocardial infarction within 3 months
- ❌ Active uncontrolled infection
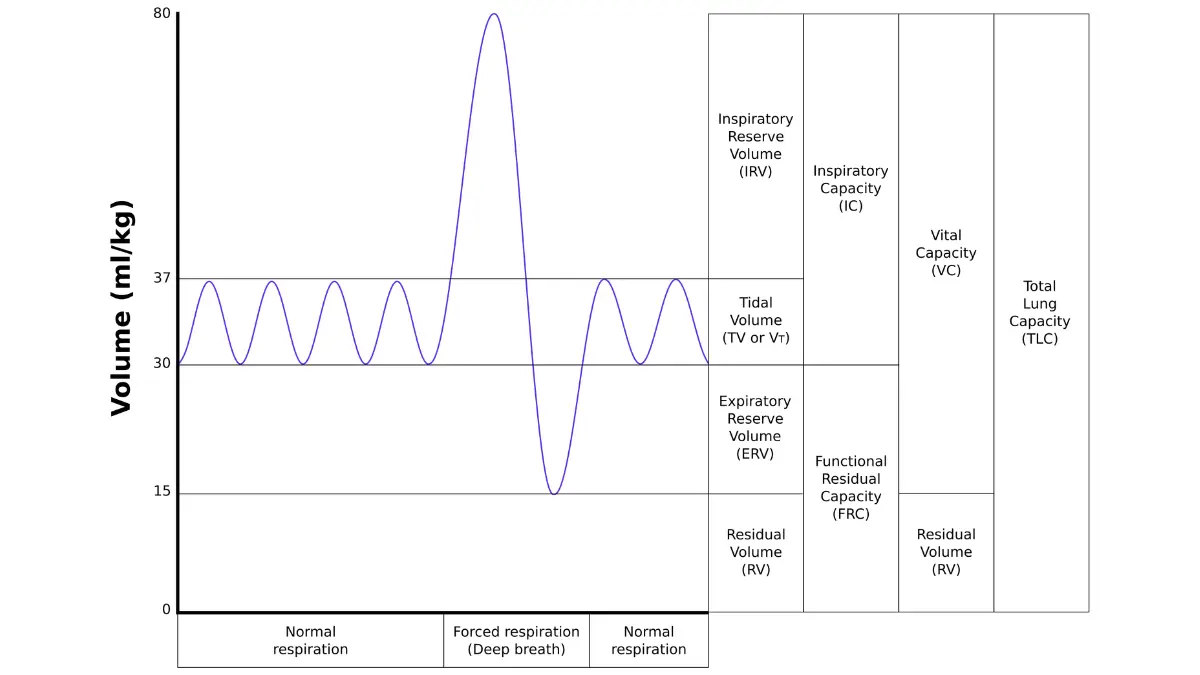
The Pulmonary Function Test — Your Surgical Green Light
Before any lung cancer surgery, your team orders Pulmonary Function Tests (PFTs), specifically measuring FEV1 (forced expiratory volume) and DLCO. These numbers predict how well you’ll function after tissue removal.
A stair-climb test or 6-minute walk test is also commonly used to assess cardiopulmonary fitness in surgical candidates. Your inherited genetic makeup can also influence surgical risk — use our Genetic Risk Assessment Tool to understand your baseline inherited cancer risk factors before your consultation.
The Tumor Board Process — What Happens Before Your Surgery Date
Your case goes to a tumor board where specialists review imaging (CT, PET-CT, MRI), pathology results from your lung biopsy, and functional test data. This process typically takes 5–10 business days.
The board determines: which surgery type, which approach (VATS vs. open), and whether neoadjuvant (pre-surgery) chemotherapy is needed first. This collaborative model reduces surgical complications and improves long-term outcomes.
Lobectomy vs Pneumonectomy — What the 2025–2026 Survival Data Shows
The Numbers That Actually Matter for Your Decision
This is where most articles fail patients — they omit or underreport actual survival data. Here is what peer-reviewed 2025–2026 research confirms about lung cancer surgery outcomes.
5-Year Survival Rates — Updated 2025 STS Database Findings
At the January 2025 Society of Thoracic Surgeons Annual Meeting, researchers presented data from 32,000+ Stage IA NSCLC patients — the largest survival analysis of its kind.
Key findings:
| Procedure | 5-Year Overall Survival | 10-Year Overall Survival | 30-Day Mortality |
|---|---|---|---|
| Lobectomy (Stage IA) | 71.9% | 44.8% | ~2.0% |
| Segmentectomy (Stage IA) | 69.6% | ~43.0% | ~1.5% |
| Wedge Resection | Lower than anatomic | — | ~1.2% |
| VATS Lobectomy | ~74% | — | 1.3% |
| Pneumonectomy | ~45–55% | ~30% | 4.0–4.3% |
Bold Takeaway: Lobectomy delivers the highest 5-year survival for Stage IA NSCLC at 71.9% — and minimally invasive VATS lobectomy reduces 30-day mortality to just 1.3%.
For complete survival statistics by stage, see our in-depth guide on Lung Cancer Statistics & Survival Rates.
Operative Mortality — Modern Surgery Is Dramatically Safer
According to a landmark review published in NIH PubMed Central, the 30-day mortality rate has fallen significantly:
- Open lobectomy: ~2.0%
- Minimally invasive (VATS/RATS) lobectomy: ~1.3%
- Pneumonectomy: ~4.0–4.3%
High-volume thoracic surgery centers — those performing 50+ resections annually — consistently show 30–40% lower complication rates than low-volume hospitals. Volume matters. Ask your center how many lung cancer surgeries they perform per year.
Quality of Life After Pneumonectomy — Can You Live Normally With One Lung?
This is the question James asked his surgeon — and the answer is nuanced. Most patients adapt remarkably well after pneumonectomy.
According to the CDC’s lung cancer data, the majority of pneumonectomy survivors report acceptable quality of life within 6–12 months. Activities like walking, light exercise, and desk work are typically achievable. High-intensity exercise and strenuous labor may remain permanently limited.
Your BMI directly affects post-pneumonectomy respiratory reserve. Maintaining a healthy weight reduces breathing strain after lung removal — use our free BMI Calculator to track your pre-surgical and recovery weight status.
What Happens During & After Lung Cancer Surgery
Inside the Operating Room — VATS, RATS & Open Thoracotomy
Modern lung cancer surgery has been transformed by minimally invasive techniques. Understanding what happens during your procedure reduces anxiety and improves pre-surgical preparation.
VATS vs RATS vs Open Thoracotomy — Side-by-Side
| Approach | Incisions | Camera Used? | Recovery Speed | Best For |
|---|---|---|---|---|
| Open Thoracotomy | 1 large (8–12 cm) | No | Slowest | Complex central tumors |
| VATS | 2–4 small (1–2 cm) | Yes | Faster | Most lobectomies & segmentectomies |
| RATS (Robotic) | 4–5 small (1 cm) | Yes (3D HD) | Fastest | Precision complex resections |
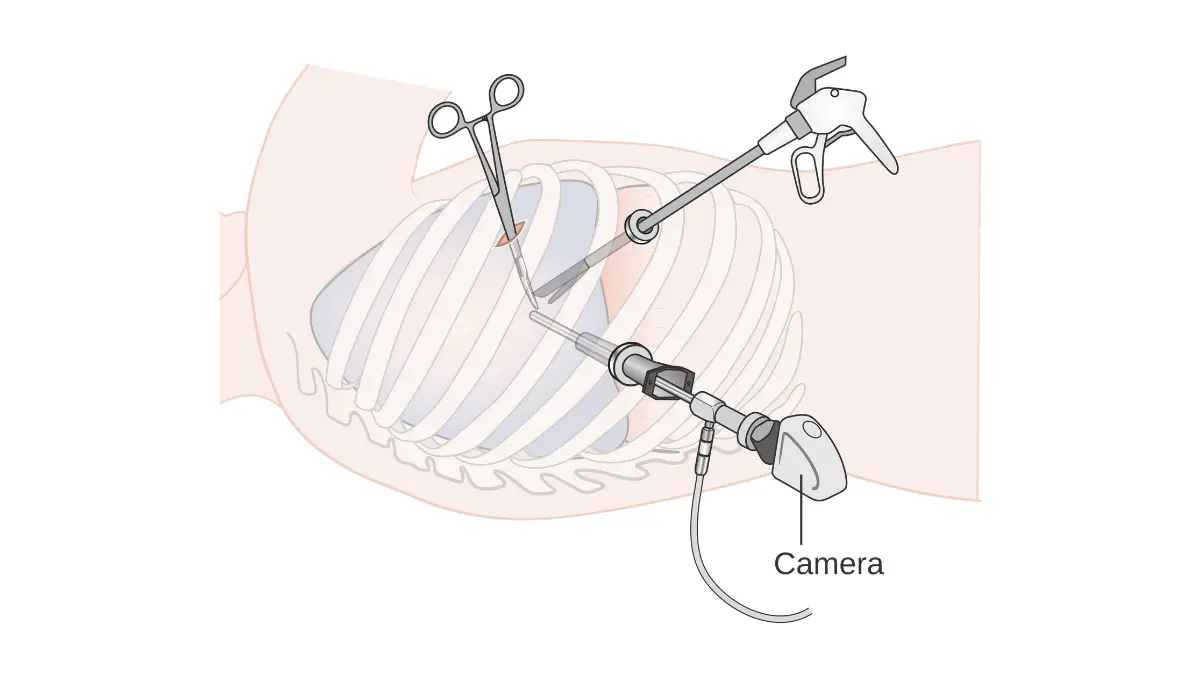
Robotic-assisted surgery (RATS) now accounts for a growing share of lung cancer surgeries at major US cancer centers. The 3D high-definition camera and articulated robotic arms allow precision that surpasses human hand movement in tight thoracic spaces.
The ERAS Protocol — How Top Hospitals Cut Recovery Time by 40%
The Enhanced Recovery After Surgery (ERAS) protocol is the single biggest advancement in post-surgical care that most patients have never heard of — and that virtually no competitor article explains.
According to a peer-reviewed study in NIH PubMed Central on ERAS for Lung Cancer, patients managed under ERAS protocols showed significantly shorter hospital stays and lower complication rates compared to traditional perioperative care.
ERAS for lung cancer surgery includes:
Pre-Surgery (2–4 Weeks Before):
- Respiratory muscle training exercises (incentive spirometry)
- Carbohydrate loading drinks the night before surgery
- Smoking cessation — mandatory minimum 4 weeks prior
- Pre-habilitation: light aerobic walking program
During Surgery:
- Epidural or paravertebral nerve block analgesia (reduces opioid need)
- Minimally invasive approach where possible
- Temperature management and fluid optimization
Post-Surgery:
- Early mobilization: walk within 12–24 hours of surgery
- Multimodal pain control (NSAIDs + nerve blocks, not opioids alone)
- Early chest drain removal (within 24–48 hours if output permits)
- Oral diet resumed within hours of extubation
What This Means For You: Ask your surgical center directly: “Do you follow ERAS protocols for thoracic surgery?” Hospitals without ERAS programs have measurably longer stays and higher complication rates.
Your First 48 Hours Post-Surgery — What to Expect
You will wake up in the recovery room with a chest tube (or two) draining fluid from around the lung. Pain is managed — modern ERAS protocols mean most patients rate pain as 3–5/10, not 8–10/10 as feared.
Day 1 milestones under ERAS:
- Sit upright in a chair within 6 hours
- Walk the corridor within 12–24 hours
- Begin incentive spirometry every 1–2 hours while awake
- IV fluids transitioned to oral intake
Sleep quality during recovery critically affects healing speed. Use our Sleep Calculator to build an optimal rest schedule for your discharge week.
Lung Cancer Surgery Recovery — Week-by-Week Roadmap
The Recovery Timeline Competitors Never Give You
Every top-ranked article says “recovery takes weeks to months.” That is not a roadmap. Here is the actual week-by-week breakdown — the most detailed recovery guide for lung cancer surgery available online.
Master Recovery Timeline Table
| Milestone | VATS Lobectomy | Open Lobectomy | Pneumonectomy |
|---|---|---|---|
| Hospital discharge | Day 3–5 | Day 5–7 | Day 7–10 |
| Chest tube removed | Day 1–3 | Day 3–5 | Day 3–5 |
| Off opioid pain meds | Week 2 | Week 3–4 | Week 3–5 |
| 30-minute daily walk | Week 2–3 | Week 3–4 | Week 4–6 |
| Return to desk work | Week 4–6 | Week 6–8 | Week 8–12 |
| Resume driving | Week 4–6 | Week 6 | Week 8 |
| Light exercise | Month 2 | Month 2–3 | Month 3–4 |
| Full physical activity | Month 2–3 | Month 3–4 | Month 4–6 |
Weeks 1–2 at Home — Managing Pain, Fatigue & Breathlessness
Fatigue is the most underreported post-surgical symptom. Most patients are surprised by how exhausted they feel even after VATS lobectomy.
Normal symptoms in weeks 1–2:
- Chest tightness and mild breathlessness (especially when bending)
- Shoulder soreness on the surgical side
- Interrupted sleep from discomfort
- Low-grade fatigue even with minimal activity
Not normal — call your surgeon immediately if you experience:
- ❗ Fever above 101°F (38.3°C)
- ❗ Increasing shortness of breath at rest
- ❗ Chest pain that worsens suddenly
- ❗ Coughing up blood
- ❗ Redness, warmth or pus at incision site
Weeks 3–8 — Rebuilding Lung Capacity
This phase is where pulmonary rehabilitation makes its biggest difference. Pulmonary rehab — a structured program of breathing exercises, supervised aerobic training, and nutritional guidance — is strongly recommended after all major lung cancer surgeries.
According to the American Thoracic Society patient resources, pulmonary rehabilitation improves exercise capacity and quality of life in post-surgical lung cancer patients. Ask your surgeon for a referral before discharge.
During pulmonary rehab, keeping your heart rate in the right training zone is critical to safe recovery. Use our Heart Rate Zone Calculator to identify your safe aerobic training range throughout rehabilitation.
Staying well-hydrated accelerates tissue healing and clears post-surgical mucus secretions. Use our Water Intake Calculator to calculate your daily hydration target based on your body weight during recovery.
3–6 Months — What Full Recovery Actually Looks Like
By month 3, most VATS lobectomy patients report feeling 80–90% of their pre-surgical baseline. Full return to demanding physical work may take up to 6 months.
Pneumonectomy patients adapt over a longer arc. The remaining lung undergoes compensatory hyperinflation — it gradually expands to fill some of the space left by the removed lung. This adaptation improves breathing efficiency over 6–12 months.
Attend every follow-up appointment. Post-surgical surveillance CT scans are scheduled at 6 months, 12 months, and annually thereafter. Do not skip these — recurrence detection in the first 2 years dramatically affects outcomes.
For broader context on how surgery fits into your overall cancer plan, our What Is Lung Cancer pillar guide and Lung Cancer Treatment Options article provide comprehensive next-step guidance.
Risks, Complications & 10 Questions to Ask Your Thoracic Surgeon
Complication Risks — What Every Patient Must Understand Before Signing Consent
All lung cancer surgeries carry risks. Understanding them is not frightening — it is empowering.
Common complications (usually manageable):
- Prolonged air leak from the lung (most common, resolves in days–weeks)
- Atrial fibrillation (occurs in ~10–20% of lobectomy patients post-op)
- Pneumonia or respiratory infection
- Blood clots (DVT/PE) — prevented by early walking and anticoagulation
Serious complications (less common):
- Bronchopleural fistula — air leak at the bronchial stump (more common after pneumonectomy)
- Post-pneumonectomy pulmonary edema — fluid accumulation in the remaining lung
- Hemorrhage requiring reoperation
- Prolonged mechanical ventilation
According to CancerCare’s lung cancer support resources, patients who join support groups and understand their surgical risks report significantly lower post-surgical anxiety and better adherence to recovery protocols.
10 Questions Every Patient Should Ask Their Thoracic Surgeon
Before signing your surgical consent, bring this list to your pre-operative appointment:
- Am I a candidate for VATS or robotic surgery — and if not, why not?
- What is your personal complication and mortality rate for this procedure?
- Does this hospital follow ERAS protocols for thoracic surgery?
- What is my predicted post-operative FEV1 (ppoFEV1)?
- Will I need adjuvant chemotherapy or radiation after surgery?
- How many lung cancer resections does your team perform per year?
- What happens if cancer is found in lymph nodes during surgery?
- What are my non-surgical alternatives if I’m borderline eligible?
- How soon after surgery will pathology confirm clear margins?
- Do you have an on-site pulmonary rehabilitation program?
Use our Symptom Checker to track and log any post-surgical symptoms between appointments — bring the full log to every follow-up visit.
Insurance, Cost & Financial Assistance for Lung Cancer Surgery in the USA
Lung cancer surgery costs vary significantly by procedure type, hospital, and insurance coverage:
| Procedure | Average US Cost (Without Insurance) | With Medicare Coverage |
|---|---|---|
| VATS Lobectomy | $30,000–$65,000 | Covered (standard cost-sharing) |
| Open Lobectomy | $40,000–$80,000 | Covered (standard cost-sharing) |
| Pneumonectomy | $50,000–$100,000+ | Covered (standard cost-sharing) |
| Robotic (RATS) Lobectomy | $35,000–$75,000 | Covered at most centers |
Financial assistance programs exist through the NCI Clinical Trials and Support Programs, CancerCare, and hospital charity care programs. Never delay a surgical consult due to cost concerns without first exploring these resources.
Frequently Asked Questions About Lung Cancer Surgery
Q1: What is the most common surgery for lung cancer?
Lobectomy is the most common and most effective lung cancer surgery, removing one lung lobe while preserving healthy tissue and delivering the highest 5-year survival rates.
Q2: How long does lung cancer surgery take?
VATS lobectomy typically takes 2–3 hours. Open pneumonectomy can take 3–5 hours depending on tumor complexity and lymph node dissection required.
Q3: What is the survival rate after lobectomy for lung cancer?
Per 2025 STS database data analyzing 32,000+ patients, Stage IA NSCLC lobectomy delivers a 71.9% five-year overall survival rate — the strongest of all surgical options.
Q4: Can you live normally after a pneumonectomy?
Yes — most patients adapt well. Daily activities, light work, and walking are achievable. High-intensity physical activity may remain limited, but quality of life is generally acceptable within 6–12 months.
Q5: What is VATS surgery for lung cancer?
VATS (Video-Assisted Thoracoscopic Surgery) uses 2–4 small incisions and a camera, allowing surgeons to remove lung tissue with less trauma, faster recovery, and lower complication rates than open surgery.
Q6: Is lung cancer surgery painful?
Modern ERAS protocols using nerve blocks, epidurals, and multimodal pain control mean most patients rate their pain as manageable (3–5/10), not the severe pain patients once feared.
Q7: When can I fly after lung cancer surgery?
Most thoracic surgeons recommend waiting a minimum of 6–8 weeks before flying, and longer — typically 10–12 weeks — after pneumonectomy, due to trapped gas and pressure risk.
Q8: What is the difference between lobectomy and segmentectomy?
A lobectomy removes an entire lobe (the larger anatomic unit). A segmentectomy removes only one or more segments within a lobe, preserving more lung function — ideal for smaller tumors or patients with reduced baseline lung capacity.
Q9: What is a sleeve lobectomy?
A sleeve lobectomy removes a lung lobe plus a section of the bronchus, then reconnects the airway. It is a lung-saving alternative to pneumonectomy with significantly better survival outcomes for suitable candidates.
Q10: How should I prepare for lung cancer surgery?
Stop smoking immediately (minimum 4 weeks pre-op), complete all pulmonary function tests, begin incentive spirometry exercises, meet with an anesthesiologist, and follow your surgical team’s fasting and medication instructions precisely.
Q11: Does lung cancer surgery cure lung cancer?
Surgery can be curative for early-stage NSCLC when complete tumor removal with clear surgical margins is achieved. Stage I patients who undergo lobectomy have the highest probability of long-term disease-free survival.
Key Takeaways
- Lobectomy is the gold standard for Stage I–II NSCLC with a 71.9% five-year survival rate (2025 STS data)
- VATS and robotic surgery reduce mortality to 1.3% and significantly shorten recovery versus open surgery
- Pneumonectomy carries higher risk but remains essential for central, inoperable-by-lobectomy tumors
- ERAS protocols cut hospital stays by up to 40% — ask your center if they use them
- Pulmonary rehabilitation after surgery is not optional — it is the difference between a good and an excellent recovery
- Surgical eligibility depends on cancer stage, FEV1 lung function, and overall fitness — always request a multidisciplinary tumor board review
For more information on your lung cancer journey, explore our complete library including Lung Cancer Diagnosis, Lung Cancer CT Scan Guide, and Stage 1 Lung Cancer Survival — all available at mymedicineadvisor.com.
⚕️ Medical Disclaimer: This article is written for educational purposes only. It does not replace professional medical advice, diagnosis, or treatment. Always seek the guidance of a qualified thoracic surgeon or oncologist regarding your specific medical condition.
About this content
This medical content is prepared through a structured publishing workflow with expert writing, clinical review and editorial quality checks.

Board Certifications: Internal Medicine (2005); Medical Oncology (2008); Hematology (2009) Experience: 20 years | Location: Houston, Texas Education: BS Biology, Duke University (1999); MD, Baylor College of Medicine…

Board Certifications: General Surgery (2007); Surgical Critical Care (2009); Robotic Surgery (da Vinci Certification 2011) Experience: 18 years | Location: Chicago, Illinois Education: BS Human Biology, Stanford University…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.