On This Page – Quick Medical Summary
If you are dealing with erection problems after prostate cancer treatment — or searching on behalf of someone you love — two things are worth knowing up front: this is one of the most common effects of treatment, and it is often manageable.
Where you are in your journey changes what matters, so use this guide by your situation:
- Just had, or facing, surgery (radical prostatectomy)? Go to the recovery timeline and the options ladder below.
- Treated with radiation? Your timeline looks different — changes tend to appear later, not right away.
- On hormone therapy? The cause is low testosterone rather than nerve damage, which changes what helps.
- A partner trying to help? The section on intimacy and relationships is written for you.
Erectile dysfunction after prostate cancer does not mean the cancer is worse or that treatment failed. It is a known consequence of treating an organ wrapped in the nerves and blood vessels an erection depends on. Real, staged options exist whether or not natural erections return on their own — and the rest of this guide to prostate cancer treatment explains them.
ℹ️ Medical Disclaimer: This article is general education, not medical advice, and does not diagnose any condition or recommend any specific treatment, medication, or procedure for you. Do not start, stop, or combine any medication — including erectile dysfunction medication — based on this page; some combinations, such as ED pills with nitrate heart medicines, can be dangerous. Decisions about diagnosis, treatment, surgery, and medication should be made with a board-certified urologist or your cancer care team.
Why prostate cancer treatment causes erection problems
Erections rely on healthy nerves, open blood vessels, and enough testosterone — and prostate cancer treatment can affect all three. Understanding which one your treatment touched is the key to knowing what will help.
Nerve and blood-vessel damage (surgery and radiation)
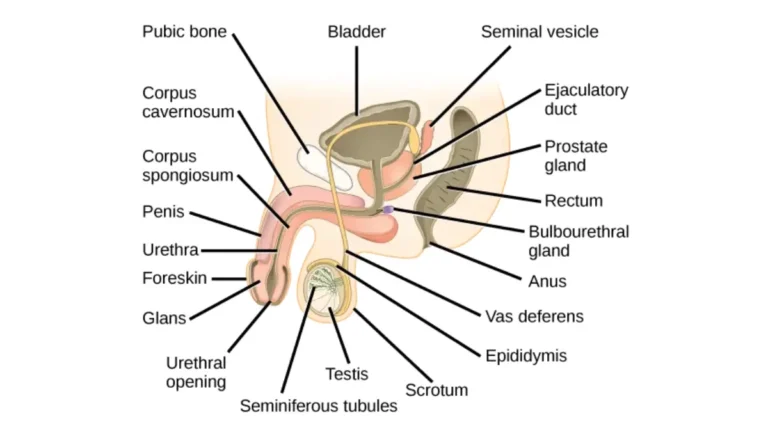
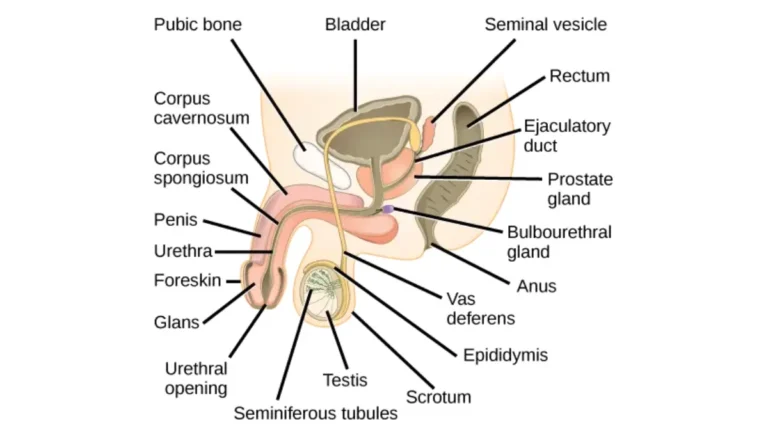
The nerves needed for an erection run along the back and sides of the prostate, which makes them vulnerable during a radical prostatectomy. According to the American Cancer Society, surgery to organs in the pelvis can damage these nerves, and even with nerve-sparing technique they need time to heal.
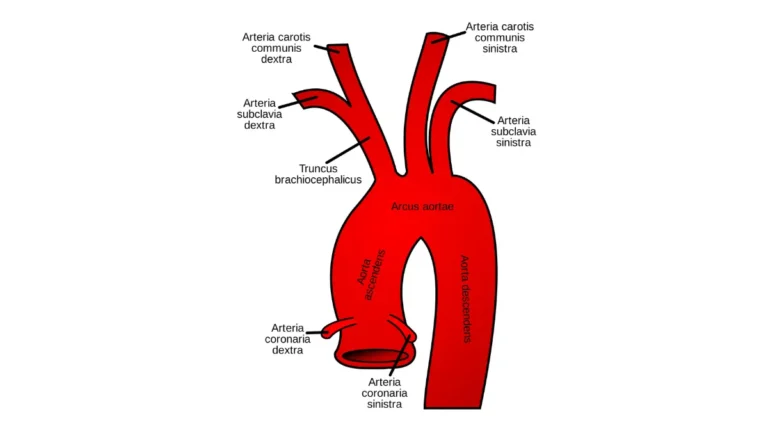
Radiation works differently. As the treated area heals, scar tissue can keep blood vessels from widening normally, and radiation can narrow or harden the pelvic arteries that carry blood to the penis.
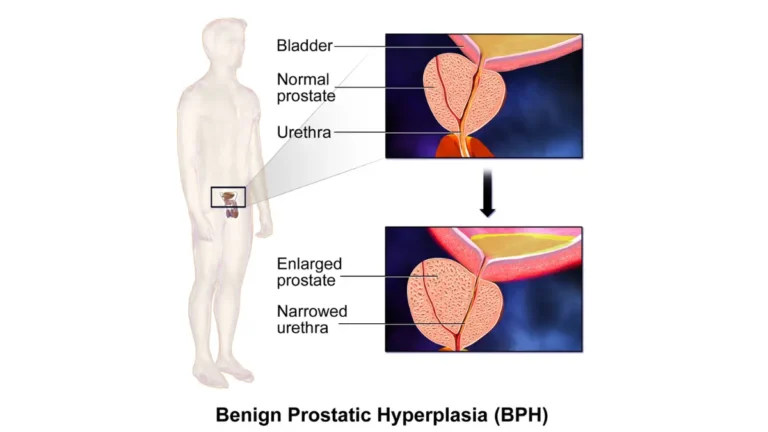
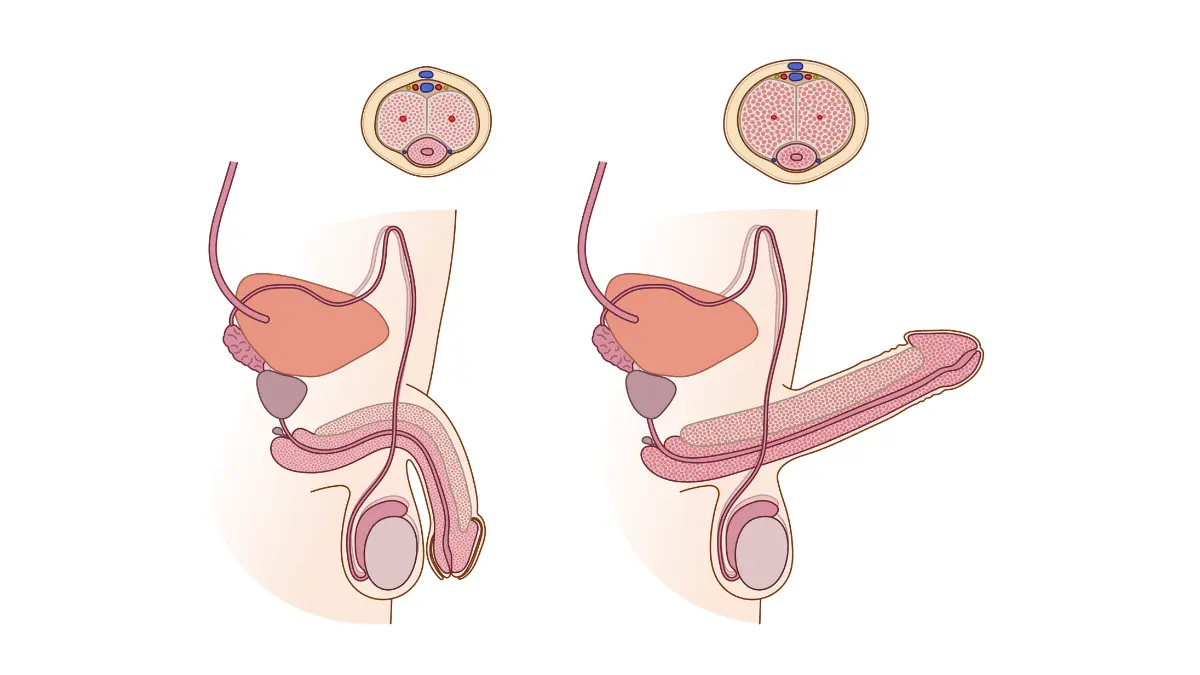
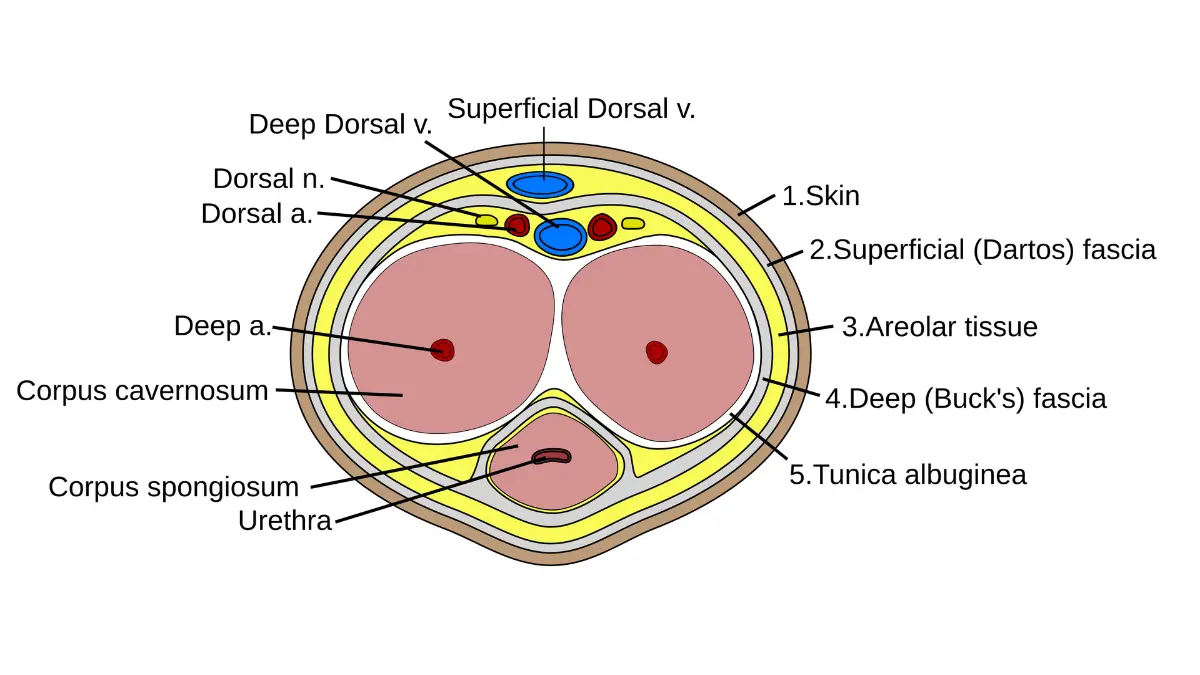
🔬 How It Works: An erection happens when nerve signals tell the arteries in the penis to widen, letting blood flow in and fill the erectile tissue. Surgery or radiation near the prostate can interrupt those nerve signals or limit that blood flow, so the same arousal no longer produces the same firmness.
Creative Commons Attribution 3.0 Unported license.
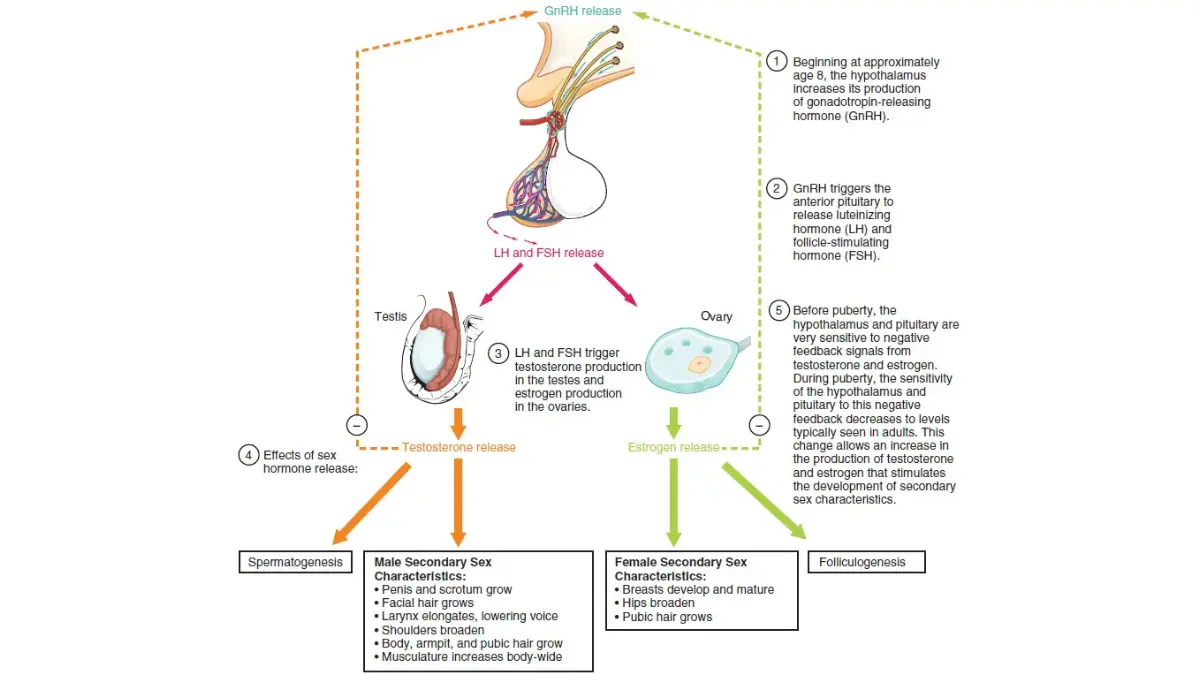
Low testosterone (hormone therapy)
Some prostate cancer treatments lower testosterone on purpose. The ACS notes that androgen deprivation therapy (ADT) can reduce sex drive and cause problems with erections and orgasm, and that erections may or may not recover after ADT stops — recovery is more likely in younger men, though medication may still be needed.
Why the cause changes what helps
Because the cause differs, so does the fix. Nerve-related problems after surgery or radiation therapy often respond to treatments that boost blood flow, while problems driven by hormone therapy may also involve lost desire that blood-flow medications alone do not fix.
How likely is ED — and will it get better over time?
For many men, erectile function improves over time, but the timeline depends heavily on the treatment. Here is what the evidence shows, with the honest caveat that recovery numbers vary widely depending on how studies define and measure erections.
After surgery (radical prostatectomy)
Erections are usually weakest right after surgery and can improve gradually as nerves heal — a process the ACS says can take up to about two years. Recovery is more likely when both sides of nerves are spared, when you are younger, and when your erections were strong beforehand.
📊 Clinical Data Point: Among men who were potent before nerve-sparing surgery, about 40% to 65% retained erections firm enough for intercourse — though the procedure induces at least a partial deficit in nearly all patients. Source: NCI, Prostate Cancer Treatment (PDQ).
📊 Clinical Data Point: In one peer-reviewed cohort of bilateral nerve-sparing prostatectomy, about 72% of men under 55 recovered erectile function, versus about 30% of men over 70. Source: peer-reviewed study, PubMed (PMID 22240189).
After radiation therapy
Radiation-related erection problems tend to come on more slowly than after surgery. The ACS reports they usually begin 6 months to 2 years after treatment ends, may improve after 2 to 3 years, and are more likely with higher radiation doses and larger treatment areas.
After hormone therapy
Because ADT lowers testosterone, it can reduce both desire and erections. Function may return after stopping treatment — more often in younger men — but recovery is not guaranteed.
What improves your odds
Modifiable health factors matter. The ACS lists diabetes, high blood pressure, heart disease, obesity, and smoking as conditions that worsen erectile recovery, which is one reason cardiovascular health is part of the picture — you can check your BMI as one starting point. Over the long term, studies don’t show much difference between surgery and radiation in erectile outcomes. Improvement is common but gradual, and effective treatments exist regardless of natural recovery.
What helps: treatment options, from first-line to advanced
There is no single “best” treatment — clinicians work through an ordered set of options with you, starting simple and escalating only if needed. Here is the general ladder.
- First-line — PDE5 inhibitor pills. Medications such as sildenafil, tadalafil, and vardenafil are usually the first option offered.
- If pills aren’t enough — devices and injections. A vacuum erection device, or injection/suppository therapy, are common next steps.
- Advanced — a penile implant. A surgically placed prosthesis is an option for men who don’t respond to other treatments.
First-line: PDE5 inhibitors (the “ED pills”)
PDE5 inhibitors improve blood flow to the penis, and the ACS notes some men need to heal from surgery before the pills work well. Responsiveness can also increase as nerve injury slowly resolves. They do not work for everyone, and they are not safe with certain other medicines (see the safety section).
If pills aren’t enough: vacuum devices and injections
A vacuum erection device draws blood into the penis using gentle suction; systematic reviews report it can help preserve penile length and works well in combination with pills. If pills are ineffective or unsuitable, injection therapy or an intraurethral suppository can also produce erections.
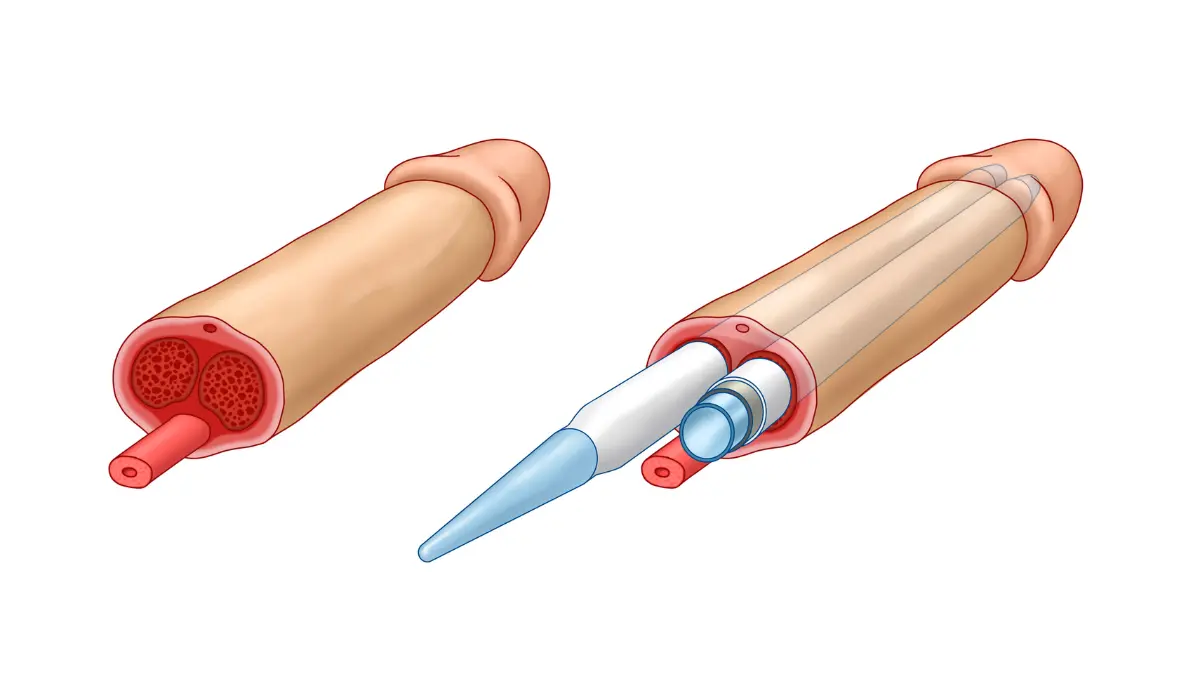
Advanced option: a penile implant
For men who don’t respond to less-invasive options, a penile implant is a well-established surgical treatment.
Creative Commons Attribution-Share Alike 4.0 International license.
🩺 Physician Note: Clinical guidance generally favors trying the least invasive effective option first and reserving surgery for when other treatments don’t work. The right choice depends on your overall health, your other medications, and how far along you are in recovery.
✅ Patient Action: Ask a urologist or sexual-medicine specialist: “Given my treatment and the other medicines I take, which ED options are safe for me, and in what order would you try them?”
What penile rehabilitation is — and what the evidence actually says
Penile rehabilitation is any early, proactive effort to help erectile function recover during the healing window, rather than simply waiting to see what returns.
The idea behind it
The thinking is that keeping blood flowing to the penis while nerves recover may protect the erectile tissue from low-oxygen changes that make lasting ED more likely.
What it can involve
In practice, rehabilitation can include PDE5 inhibitor pills, a vacuum device, or injection therapy — used soon after treatment rather than only once problems become permanent.
What the research does and doesn’t show
This is where honesty matters. A systematic review of penile rehabilitation after surgery and radiation found the rationale sound and some supportive data — particularly for vacuum devices preserving length and for certain medication schedules — but human results are contradictory, and there is no single agreed-upon protocol yet. You can read the underlying research on penile rehabilitation for the full picture. The practical takeaway: it may be worth doing, but it is not a guaranteed fix, so ask your urologist whether and when it fits your case.
Safety first: drug interactions, counterfeits, and when to get help
Before trying anything for erections, a few safety points can prevent real harm.
The one combination to never mix
⚠️ Clinical Warning: ED pills (PDE5 inhibitors) must never be combined with nitrate medicines such as nitroglycerin, which are taken for chest pain and some heart conditions. The FDA warns this combination can lower blood pressure to dangerous levels. If you take any heart medication, confirm with a clinician before using any ED treatment.
Avoid counterfeit ED products sold online
Be wary of “natural” sexual-enhancement pills sold online. The FDA reports that many contain hidden, undeclared drug ingredients, are not reviewed or approved, may carry the same dangerous nitrate interaction, and have sent users to the hospital — and it maintains a searchable health-fraud product database of more than 1,000 such products.
When to see a specialist
Persistent erection problems, no response to first-line pills, or significant distress are all reasons to seek specialist care rather than wait it out.
✅ Patient Action: If first-line treatment isn’t working, ask your care team for a referral to a urologist or sexual-medicine specialist, and tell them every medication and supplement you take so they can check for interactions.
Beyond erections: intimacy, identity, and your partner
Erectile dysfunction after prostate cancer is not only physical, and treating the emotional side is part of recovery — not a footnote to it.
How it can affect mood and identity
Many men feel grief, frustration, or a sense of lost identity. The ACS notes that emotional distress can itself contribute to erection problems, so mental-health support is genuinely useful, not a sign of weakness.
Talking with your partner
Bringing a partner into appointments and decisions helps, and relationship or sex therapy can ease the strain that ED places on a couple. Intimacy is something you navigate together.
Intimacy and orgasm are still possible
Here is a reassurance grounded in the evidence: orgasm is often still possible even without a full erection. After prostate removal, orgasm is typically “dry” — without semen — because the prostate and seminal vesicles are gone, but pleasure and closeness remain achievable.
Frequently asked questions about ED after prostate cancer
1. Does erectile dysfunction after prostate cancer go away?
For many men it improves, but the timeline depends on the treatment. After surgery, function is usually weakest right after the operation and can improve over the following months to about two years as nerves heal. After radiation, problems tend to appear later. Improvement isn’t guaranteed, but effective treatments exist either way.
2. How long does ED last after a prostatectomy?
Erections are typically weakest right after surgery and may improve gradually as nerves heal, a process that can take up to about two years. Recovery is more likely in younger men and those with strong erections before surgery. Ask your urologist for an estimate based on your specific case.
3. Can you still get an erection after prostate removal?
Many men can, especially after nerve-sparing surgery and with time and treatment, though erections may be less firm and often need help from medication or devices. Sparing nerves on both sides improves the odds. Your results depend on your surgery, age, and prior function, so discuss them with your surgeon.
4. What is the best treatment for ED after prostate cancer?
There is no single best option. Clinicians usually start with PDE5 inhibitor pills, then move to vacuum devices or injections if pills aren’t enough, with a penile implant as an advanced choice. The right path depends on your health and other medicines, so decide it with your urologist.
5. Do Viagra and Cialis work after prostate surgery?
They can, and they’re usually tried first, but they may work less well until nerves recover, and some men need to heal from surgery first. They aren’t safe for everyone — never combine them with nitrate heart medicines, and confirm suitability with your clinician before use.
6. What is penile rehabilitation?
Penile rehabilitation is any early, proactive step — such as pills, a vacuum device, or injections — meant to help erectile function recover during healing by keeping blood flowing to the penis. The rationale is sound, but human evidence is mixed and no standard protocol exists. Ask your urologist whether it fits your case.
7. Does radiation cause erectile dysfunction?
It can. Unlike surgery, radiation-related erection problems usually develop more slowly — often 6 months to 2 years after treatment — as scarring and reduced blood flow set in, and they may improve after 2 to 3 years. Higher doses and larger treatment areas raise the risk.
8. Can hormone therapy cause erection problems?
Yes. Androgen deprivation therapy lowers testosterone, which can reduce sex drive and the ability to get or keep an erection. Function may return after stopping it, especially in younger men, but recovery isn’t guaranteed. Talk with your oncology team about what to expect.
9. Is ED permanent after prostate cancer treatment?
Not always. Many men see gradual improvement over months to a couple of years, and treatments help even when natural erections don’t fully return. Whether it lasts depends on the treatment type, your age, your prior erectile strength, and other health conditions. Your care team can give a more personal estimate.
10. When should I see a specialist for ED after prostate cancer?
See a urologist or sexual-medicine specialist if erection problems persist, first-line pills don’t help, or the situation is causing real distress. Also check with a clinician before any ED treatment if you take heart or blood-pressure medicines, since some combinations are unsafe.
11. Can you still orgasm after prostate cancer treatment?
Often yes — orgasm is usually still possible even without a full erection, though it changes. After prostate removal, orgasm is typically “dry,” with no semen, because the prostate and seminal vesicles are gone. Intimacy and pleasure remain achievable, and a counselor or your care team can help you adjust.
The bottom line — and your next step
Erectile dysfunction after prostate cancer is common, it often improves with time, and real treatments help even when natural erections are slow to return. The path forward starts with an honest conversation with the right clinician — and knowing the cause of your erection problems is what points you toward what will actually help.
If you take one action, make it this: bring a written list of your medications and your specific questions to your next appointment, and ask your cancer care team which ED options are safe and likely to work for you.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.