On This Page – Quick Medical Summary
If a doctor told you your prostate is enlarged — or that your PSA is a little high — your mind may have jumped straight to cancer. Here is the reassuring part, supported by every major health authority: an enlarged prostate is not cancer, and having it does not raise your risk of prostate cancer. The two are separate conditions.
The harder truth is just as important. The urinary symptoms they cause can look almost identical, and early prostate cancer often causes no symptoms at all. So symptoms alone cannot tell you which one you have — only an evaluation can.
This guide is written for a few different readers. If you have urinary symptoms and want to know what they mean, start with the symptom comparison below. If you were told you have an enlarged prostate or a high PSA and have an appointment coming, the testing section is for you. If you are reading for someone you care about, the side-by-side table gives the clearest overview. For the bigger picture, our complete guide to prostate cancer’s signs, stages, and treatment covers what happens if cancer is actually found.
ℹ️ Medical Disclaimer: This article is general health education, not medical advice, and it cannot diagnose your condition or interpret your PSA result, imaging, or biopsy. Decisions about screening, diagnosis, and treatment for an enlarged prostate or prostate cancer should be made with a board-certified urologist or your primary care clinician, who can evaluate your individual situation. If you are unable to urinate at all or have heavy blood in your urine, seek urgent medical care.
What’s the difference between an enlarged prostate and prostate cancer?
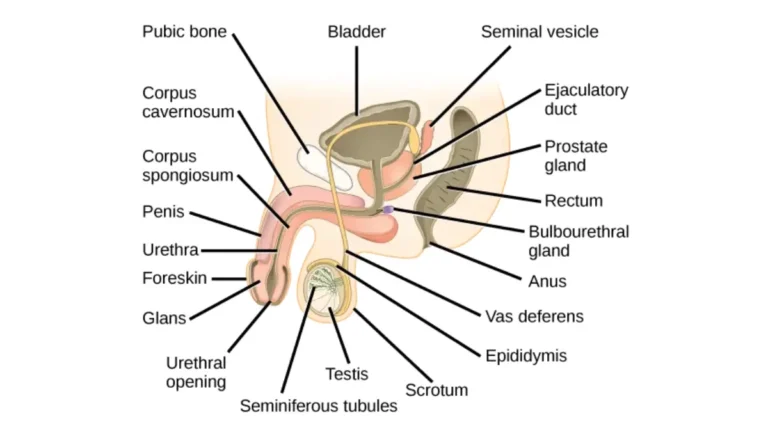
Both conditions involve the same walnut-sized gland, but they are biologically different events.
Benign vs. malignant: what each word means
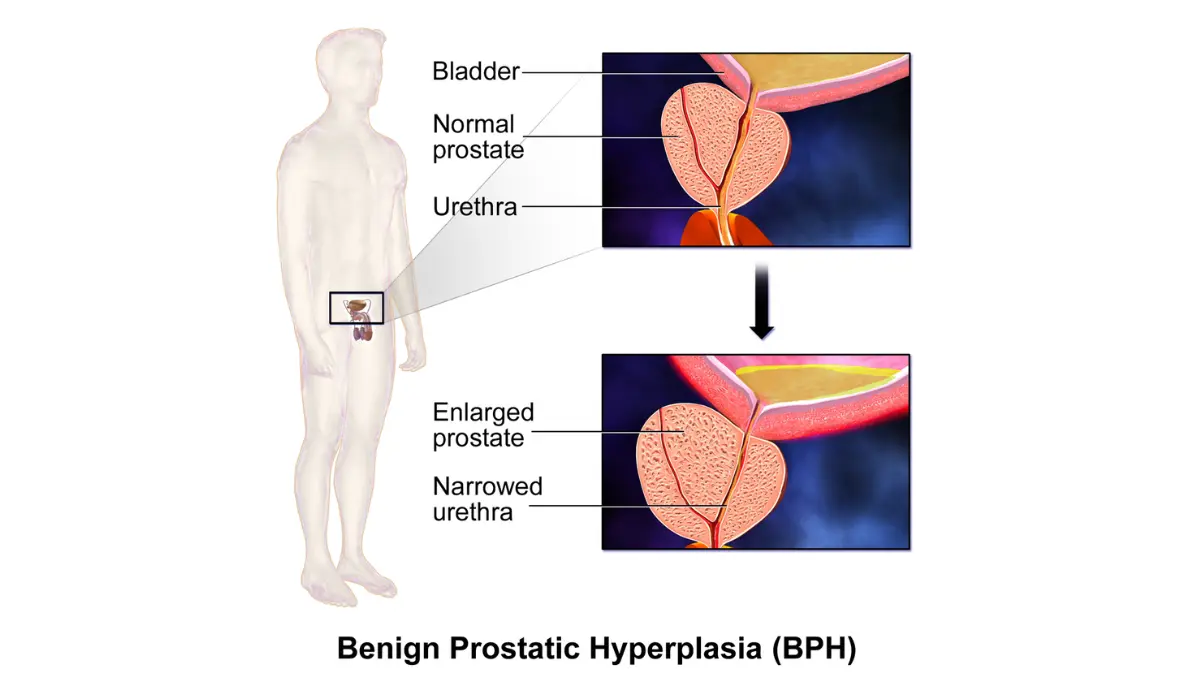
Benign prostatic hyperplasia (BPH) is the medical name for an enlarged prostate. Benign means non-cancerous, and hyperplasia means an increase in the number of otherwise normal cells. The gland grows, but the cells stay put — they do not invade nearby tissue or spread.
Prostate cancer is malignant: abnormal cells grow without control and can, over time, spread (metastasize) to lymph nodes, bones, or other organs. That capacity to spread is the defining difference between the two.
Does an enlarged prostate raise your cancer risk? No. Having BPH does not increase your risk of developing prostate cancer — they are separate processes, and one does not turn into the other, according to the NIDDK’s overview of benign prostatic hyperplasia.
Why an enlarged prostate causes symptoms but early cancer doesn’t
The short answer is location.
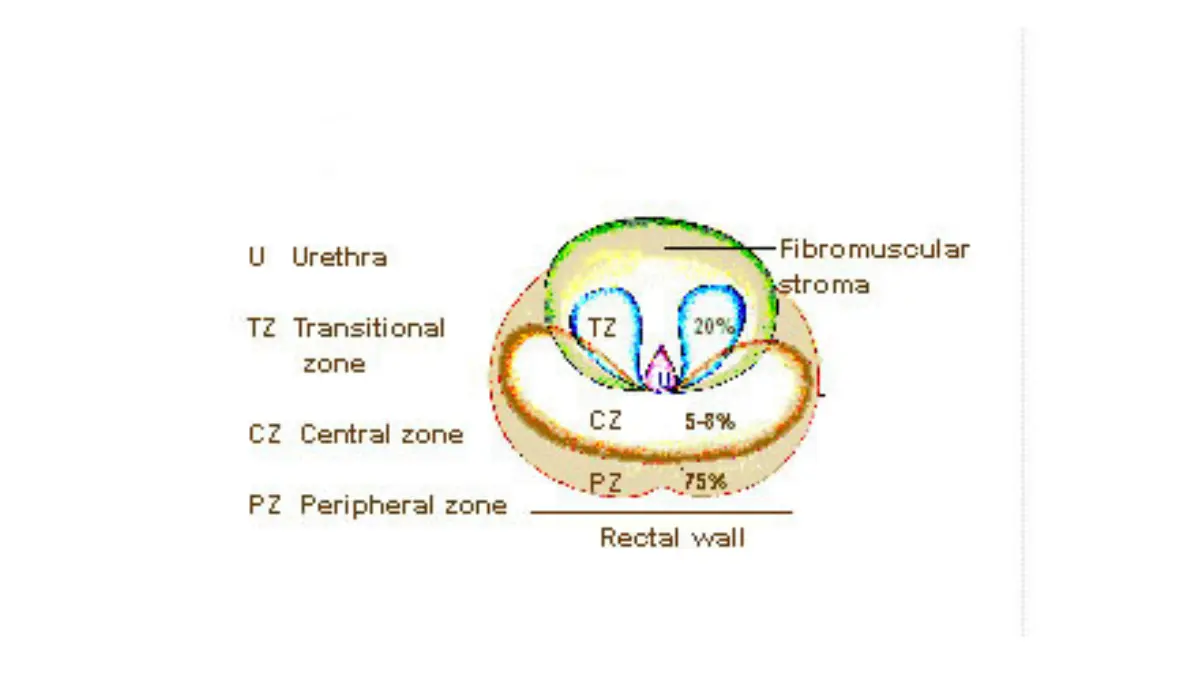
🔬 How It Works: BPH grows in the transition zone — the inner part of the prostate that wraps directly around the urethra. As that tissue enlarges, it squeezes the urethra like a hand tightening around a straw, which is why BPH so often causes urinary symptoms. Most prostate cancers begin in the peripheral zone, the outer back portion of the gland, away from the urethra. A tumor there can grow quietly, frequently with no symptoms at all, until it is more advanced.
Can you have both at the same time?
Yes. Because both become more common with age, many men have an enlarged prostate and prostate cancer at once. This does not mean the BPH caused the cancer — it simply means two common age-related conditions can exist in the same gland.
Do the symptoms feel different?
Most men arrive at this question because of urinary changes — and those changes are where the two conditions overlap the most.
Symptoms BPH and prostate cancer share
Both an enlarged prostate and prostate cancer can affect urination, producing what clinicians call lower urinary tract symptoms. These commonly include:
- A frequent or urgent need to urinate, especially at night (nocturia)
- A weak, slow, or interrupted stream
- Difficulty starting, or straining to urinate
- A feeling that the bladder has not fully emptied
- Dribbling after you finish
These symptoms are far more typical of BPH, which physically narrows the urethra. You can compare them against your own situation with our symptom checker tool as a starting point, not a diagnosis, and read the fuller picture in our guide to prostate cancer symptoms.
Symptoms that point to something more advanced
A few symptoms deserve prompt attention because they can signal a problem beyond ordinary BPH:
- Blood in the urine or semen
- New pain in the pelvis, hips, lower back, or bones
- Unexplained weight loss
These are reasons to see a clinician sooner — not proof of cancer.
Why you can’t tell them apart from symptoms alone
Can you tell prostate cancer from an enlarged prostate by symptoms? No. Because early prostate cancer is usually silent and BPH is usually noisy, a man with bothersome symptoms most often has BPH, while a man with no symptoms could still have early cancer. That mismatch is exactly why symptoms cannot serve as the test — a point plain-language references like MedlinePlus on prostate diseases make clearly.
BPH vs. prostate cancer: a side-by-side comparison
Here is how the two conditions line up across the features that matter most to a patient.
How the two conditions compare at a glance
| Feature | Enlarged Prostate (BPH) | Prostate Cancer | Key Clinical Detail |
|---|---|---|---|
| Nature | Benign (non-cancerous) | Malignant (cancerous) | Only cancer can spread to other organs |
| Where it grows | Transition zone, around the urethra | Usually the peripheral zone, outer gland | Location explains the symptom difference |
| Does it spread? | No | Yes, if not controlled | Spread (metastasis) is what makes cancer dangerous |
| Raises cancer risk? | No | — | Having BPH does not increase cancer risk |
| Typical symptoms | Urinary symptoms, often noticeable | Often none early; urinary or bone symptoms later | Symptoms alone cannot distinguish them |
| How it’s diagnosed | Symptoms, exam, PSA, urine-flow tests | PSA, exam, MRI, biopsy | Only a biopsy confirms cancer |
| How common (US) | 5–6% of men 40–64; 29–33% of men 65+ | About 333,830 new cases in 2026 | Both rise sharply with age |
| Outlook | Not life-threatening; treatable | ~98% 5-year survival overall; ~100% if localized | Outcomes depend heavily on early detection |
Sources: prevalence — NIDDK; incidence and survival — American Cancer Society and NCI SEER (2026 estimates; survival data 2016–2022).
What the comparison does and doesn’t tell you
This table explains how the two conditions differ — but it cannot tell you which one you have. Two men with identical symptoms can have entirely different diagnoses, and the only way to know is testing. Use the comparison to understand the landscape and to ask sharper questions at your appointment, not to reach a verdict on your own.
How doctors tell them apart
No single test separates an enlarged prostate from prostate cancer. Clinicians combine several, escalating only as needed.
How do doctors tell BPH and prostate cancer apart? They use a combination of steps:
- A PSA blood test to measure prostate-specific antigen
- A digital rectal exam (DRE) to feel the prostate’s size and texture
- Multiparametric MRI of the prostate when results are unclear
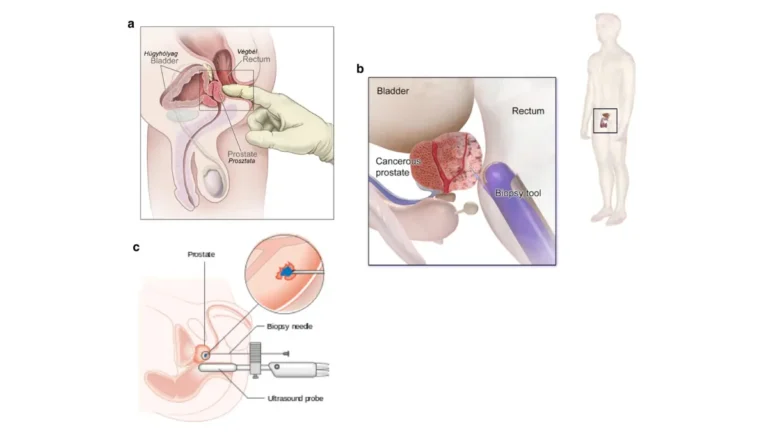
- A prostate biopsy, the only test that confirms or rules out cancer cells
PSA test and digital rectal exam: the first steps
PSA is a protein made by the prostate, and higher levels can reflect a larger or irritated gland. A digital rectal exam lets the clinician feel for hard or irregular areas. Neither one diagnoses cancer on its own — together they help decide whether more testing is warranted. You can see how results are interpreted by age group in our guide to PSA levels by age.
Does a high PSA mean cancer?
No — not by itself. PSA can rise with BPH and with prostate inflammation (prostatitis), not only with cancer, so an elevated number is a reason to investigate rather than a diagnosis. Many men with a high PSA turn out not to have cancer, which we cover in high PSA with no cancer.
MRI and biopsy: confirming the diagnosis
When PSA or the exam raises concern, an MRI can map suspicious areas and guide what comes next. A biopsy — sampling small pieces of prostate tissue — is what actually confirms whether cancer cells are present, as our guide to prostate biopsy results explains. Many men never need to reach this step.
✅ Patient Action: At your visit, ask your urologist directly: “Given my PSA level and exam, do I need an MRI or biopsy now, or is monitoring the right next step for me?”
How common is each — and what’s the outlook?
Numbers help put both conditions in perspective, and most of what they show is reassuring.
How common is an enlarged prostate?
An enlarged prostate is one of the most common parts of aging for men.
📊 Clinical Data Point: BPH affects about 5–6% of men ages 40–64 and 29–33% of men 65 and older, and it is the most common prostate problem in men over 50 — Source: NIDDK.
How common is BPH compared with prostate cancer? An enlarged prostate is more common and is not dangerous; prostate cancer is also common but more serious, though usually very treatable when caught early.
Prostate cancer by the numbers
Prostate cancer is the most frequently diagnosed cancer in American men and the second-leading cause of cancer death among them.
📊 Clinical Data Point: The American Cancer Society estimates about 333,830 new prostate cancer cases and 36,320 deaths in the United States in 2026, and roughly 1 in 8 men will be diagnosed in his lifetime — Source: American Cancer Society.
Older age, a family history, and being a Black man genuinely raise prostate cancer risk; an enlarged prostate does not. You can review these in prostate cancer causes and risk factors or assess your own risk factors.
What survival rates really say about early detection
The 5-year relative survival is tied closely to how early the cancer is found.
📊 Clinical Data Point: Five-year relative survival for prostate cancer is about 98% overall, and 100% when the cancer is localized or regional; for cancer that has spread to distant sites it is about 40%. Roughly 69% of cases are found while still localized — Source: NCI SEER (2016–2022).
The case for evaluation, then, is not fear — it is that early detection is what keeps survival high, as detailed in prostate cancer survival rates and the NCI’s prostate cancer survival data. For the full yearly statistics, see the American Cancer Society’s prostate cancer figures.
When to see a doctor — and when it’s urgent
Understanding the difference only helps if you know what to do with it.
Symptoms that warrant a routine appointment
When should you see a doctor about an enlarged prostate? Book an appointment if you have:
- Urinary symptoms that are bothersome, worsening, or disrupting your sleep or daily life
- A new need to strain, or a sense that your bladder never fully empties
- Any concern about your PSA result or prostate exam
Most causes are treatable, and raising symptoms early tends to improve quality of life rather than simply waiting them out.
Red flags that need prompt or emergency care
A few situations need same-day or emergency attention:
- A complete inability to urinate
- Heavy blood in the urine
- Fever alongside urinary symptoms, or severe lower-abdominal pain
⚠️ Clinical Warning: Being suddenly unable to pass any urine is a medical emergency known as acute urinary retention — go to urgent care or an emergency room rather than waiting it out. Left untreated, a blocked bladder can lead to infections and kidney problems.
Prostate symptoms are among the most common reasons men see a urologist, so asking for help is routine rather than an overreaction.
Frequently asked questions
1. Does an enlarged prostate turn into prostate cancer?
No. An enlarged prostate (BPH) is a benign condition, and it does not turn into or cause prostate cancer. The two develop through separate processes in different parts of the gland, and having BPH does not raise your cancer risk. They can, however, exist at the same time as men age.
2. Can you have BPH and prostate cancer at the same time?
Yes. Because both an enlarged prostate and prostate cancer become more common with age, many men have both at once. One does not cause the other — they simply coexist in the same gland. This is why a diagnosis of BPH never rules out the value of appropriate prostate cancer evaluation.
3. What are the symptoms of prostate cancer vs. an enlarged prostate?
Both can cause urinary symptoms such as frequent urination, a weak stream, and incomplete emptying. The key difference is that an enlarged prostate usually causes these symptoms, while early prostate cancer often causes none at all. Because the symptoms overlap, they cannot tell the two apart on their own.
4. Why doesn’t early prostate cancer cause symptoms?
Most prostate cancers begin in the peripheral zone, the outer part of the gland away from the urethra. Because they are not pressing on the urinary tube early on, they often grow without any symptoms. An enlarged prostate, by contrast, grows around the urethra, which is why it tends to cause noticeable urinary changes.
5. How do doctors tell BPH and prostate cancer apart?
Doctors use a combination of a PSA blood test, a digital rectal exam, sometimes an MRI, and a biopsy. No single test is definitive, and a biopsy is the only one that confirms whether cancer cells are present. Discuss with a urologist which steps are appropriate for your situation.
6. Does a high PSA mean I have cancer?
No, not by itself. PSA can rise with an enlarged prostate and with prostate inflammation, not only with prostate cancer. An elevated PSA is a signal to investigate further, not a diagnosis, and many men with a high PSA do not have cancer. Your clinician interprets the result alongside your exam and history.
7. How common is an enlarged prostate compared with prostate cancer?
An enlarged prostate is very common, affecting about 5–6% of men ages 40–64 and 29–33% of men 65 and older. Prostate cancer is also common, with about 333,830 new cases estimated in the US in 2026. Both become more likely with age, but only cancer is life-threatening.
8. Is an enlarged prostate dangerous?
An enlarged prostate is not life-threatening, but it can affect quality of life and, if left untreated, lead to complications such as urinary infections, bladder problems, or kidney strain. The good news is that BPH is treatable through monitoring, medication, or procedures. Speak with a clinician if symptoms are bothering you.
9. When should I see a doctor about prostate symptoms?
See a doctor if urinary symptoms are bothersome, worsening, or affecting your daily life, or if you have concerns about a PSA result. Seek emergency care if you are completely unable to urinate or have heavy blood in your urine. Early evaluation usually improves both comfort and outcomes.
10. What is the survival rate for prostate cancer?
Five-year relative survival is about 98% overall, and close to 100% when prostate cancer is found while localized or regional. For cancer that has spread to distant sites, it is about 40%. These figures describe large groups, not any individual, so a clinician is best placed to discuss your personal outlook.
11. Can an enlarged prostate be treated?
Yes. An enlarged prostate can be managed with watchful monitoring for mild cases, medications that relax or shrink the prostate, or minimally invasive procedures and surgery when symptoms are more severe. The right approach depends on your symptoms and health, which you can decide on with a urologist.
The bottom line
An enlarged prostate is common, it is not cancer, and having it does not raise your risk of prostate cancer. That alone resolves the fear that brings most men to this question. What it cannot do is tell you which condition you have, because the symptoms overlap and early cancer is usually silent.
That is why a simple evaluation — a conversation, a PSA test, an exam — is the responsible next step rather than worrying in either direction. And if prostate cancer is found, the outlook when it is caught early is excellent. Bring your symptoms or your PSA result to a urologist or primary care clinician, and for the full picture of what a diagnosis would involve, start with our main prostate cancer guide.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.