On This Page – Quick Medical Summary
How Long Does ACL Tear Recovery Take?
ACL tear recovery time ranges from 3-12 months depending on treatment approach. Without surgery, partial tears heal in 3-6 months with structured physical therapy. With surgical reconstruction, most athletes return to daily activities within 6-8 weeks and reach full sports clearance between 6-9 months, though recent evidence shows optimal outcomes occur when return to sport is delayed until 9-12 months.
When 17-year-old soccer player Lia felt her knee buckle during a cutting maneuver in April 2024, she heard the unmistakable “pop” that signals an anterior cruciate ligament rupture. Within hours, her knee swelled to twice its normal size—a classic sign of hemarthrosis affecting 70% of ACL tear patients. Three weeks after diagnosis, she underwent ACL reconstruction using a quadriceps tendon autograft and began the evidence-based rehabilitation protocol that would guide her through the next nine months. By six months post-surgery, Lia had regained full range of motion and could walk without a knee brace, demonstrating the predictable milestones that characterize modern ACL recovery timelines.
Understanding ACL tear recovery time is crucial for the estimated 400,000 Americans who undergo ACL reconstruction annually. Whether you’re an elite athlete or weekend warrior, knowing what to expect during each phase helps set realistic goals and prevents the premature return to activity that causes 16-21% of patients to suffer reinjury within three years. The timeline you follow depends on multiple factors: injury severity (Grade I, II, or III), treatment choice (surgical versus non-surgical), graft type selection, age, activity level, and adherence to rehabilitation protocols.
ACL Recovery Timeline by Treatment Type
*Complete ACL tears managed non-surgically show 60-70% success for low-demand activities but are not recommended for cutting/pivoting sports.
2025 Patient Outcome Data: What Success Looks Like
Recent multicenter data reveals important benchmarks for ACL reconstruction outcomes. Only 10% of patients achieve their complete rehabilitation goals at one year post-surgery, but this improves to 25% by two years. Among those who undergo reconstruction, 80-90% successfully return to pre-injury sport levels when following criterion-based protocols rather than time-based clearance alone. However, 52% of patients discontinue formal physical therapy before nine months—a critical error that correlates with higher reinjury rates.
The mean time from surgery to actual return to sport is 12 months, not the frequently cited 6-9 month window. For every additional month of rehabilitation up to nine months, reinjury risk decreases by 51%, with no further protective benefit beyond that threshold. This data underscores why rushing back to competition remains the single biggest modifiable risk factor for ACL graft failure.
What This Means For You
Your ACL tear recovery timeline should balance biological healing requirements with functional restoration milestones. Graft tissue takes 12-18 months to fully mature and incorporate, even when you feel ready to return earlier. Modern rehabilitation emphasizes criterion-based progression—advancing when you meet specific strength, range of motion, and neuromuscular control benchmarks rather than calendar dates alone. Before beginning any exercise program, use our Symptom Checker to identify associated injuries that may affect your recovery strategy, and calculate your baseline fitness metrics with our BMI Calculator to establish personalized rehabilitation targets.
Recent NIH studies on ACL healing demonstrate that 53-58% of partial tears managed non-surgically show MRI evidence of ligament healing at 2-5 years, challenging the assumption that all complete tears require surgery. Age, activity demands, and the presence of associated meniscal or cartilage injuries should guide your treatment decision in consultation with an orthopedic surgeon.
Non-Surgical ACL Recovery Protocol
ACL Tear Recovery Without Surgery: 3-Month Conservative Protocol
Non-surgical ACL tear recovery offers a viable pathway for carefully selected patients, with research showing 31-33% of acute ACL ruptures demonstrate MRI evidence of spontaneous healing when managed with structured rehabilitation alone. Conservative treatment success depends critically on injury grade, knee stability, age, activity demands, and patient motivation. Understanding whether surgery is necessary begins with accurate classification of your tear severity and realistic assessment of your functional goals.
Who Qualifies for Non-Surgical Treatment?
The decision between surgical reconstruction and conservative management represents one of the most important choices in ACL injury treatment. Research from NIH studies on conservative ACL management identifies specific patient profiles most likely to succeed without surgery. Patients with Grade I laxity on Lachman and Pivot Shift testing achieve 90% success rates with conservative treatment at one year, while those with Grade II laxity face higher probability of eventual reconstruction.

Ideal Candidates for Non-Surgical ACL Recovery:
- Grade I partial tears with less than 5mm anterior tibial translation
- Grade II partial tears (5-10mm translation) in low-demand individuals willing to modify activity
- Femoral-sided ACL ruptures with intact ligament stump greater than 50%
- Patients participating in non-pivoting sports (swimming, cycling, running)
- Children with open growth plates who benefit from delayed surgical decision
- Older adults (over 40) with low athletic demands
- Individuals with no episodes of knee instability or giving way during activities of daily living
Contraindications for Non-Surgical Approach:
- Grade III complete tears in athletes returning to cutting/pivoting sports
- Concomitant meniscal tears requiring repair (surgery needed regardless)
- Recurrent knee instability during walking or stairs
- High competitive activity demands (soccer, basketball, tennis)
- Multi-ligament injuries affecting knee stability
Week-by-Week Non-Surgical Recovery Timeline
ACL tear recovery without surgery follows a criterion-based progression emphasizing neuromuscular control, proprioceptive training, and quadriceps strengthening to compensate for ligamentous laxity. The Mass General Brigham non-operative ACL protocol provides evidence-based framework for conservative management.
Weeks 1-2: Acute Phase (Protection & Pain Control)
Primary Goals:
- Reduce hemarthrosis (joint swelling) and control pain
- Restore full knee extension (0 degrees)
- Achieve 90 degrees flexion without forcing
- Initiate quadriceps activation to prevent atrophy
Daily Protocol:
- RICE method for first 48-72 hours: ice 15-20 minutes every 2-3 hours
- Patellar mobilization: Gentle manual gliding of kneecap to prevent stiffness
- Quadriceps sets (isometric): 10 reps × 5 sets daily, hold 5-10 seconds
- Heel slides: Passive and active-assisted knee flexion, 10 reps × 3 sets
- Ankle pumps: 20 reps every waking hour to prevent DVT
- Straight leg raises: Once quad control achieved, 10 reps × 3 sets
- Weight-bearing: As tolerated with crutches, progress from partial to full
Red Flag Warning: If knee swelling increases dramatically or knee locks/catches, seek immediate medical evaluation for potential meniscal injury.
Weeks 3-6: Early Strengthening Phase
Primary Goals:
- Achieve full knee extension and 120+ degrees flexion
- Walk without assistive devices
- Restore 70% quadriceps strength compared to uninjured leg
- Improve proprioception and balance
Exercise Progression:
- Stationary bike (no resistance): Begin when 110-degree flexion achieved, 10-15 minutes daily
- Closed-chain exercises: Mini-squats (0-45 degrees), wall sits (hold 30-60 seconds), leg presses
- Step-ups: 4-inch height progression, 10 reps × 3 sets each leg
- Single-leg balance: 30-second holds on firm surface, progress to foam pad
- Hip strengthening: Side-lying leg raises, clamshells, bridges (15 reps × 3 sets)
- Hamstring curls: Standing or prone, 12 reps × 3 sets with resistance bands
Functional Milestone: You should walk normally without limp before progressing to Weeks 7-12. Calculate your baseline metabolic needs during this recovery phase using our BMR Calculator to ensure adequate nutrition for healing, and track daily protein intake with our Protein Intake Calculator targeting 1.6-2.0g/kg body weight for optimal muscle preservation.
Weeks 7-12: Advanced Strengthening & Return to Activity
Primary Goals:
- Achieve 85-90% quadriceps and hamstring strength symmetry
- Pass functional hop tests (80% limb symmetry index)
- Return to straight-line jogging
- Build confidence in knee stability through progressive loading
Advanced Exercise Protocol:
- Resistance training: Squats with weight (body weight to 50% 1RM), lunges, Bulgarian split squats
- Plyometric introduction: Double-leg hops on flat ground, forward/backward jumps
- Agility drills: Lateral shuffles, carioca, figure-8 running (controlled speed)
- Single-leg exercises: Single-leg Romanian deadlifts, single-leg squats to chair
- Neuromuscular training: Bosu ball squats, perturbation training, reactive balance drills
- Sport-specific movements: Sport-related cutting patterns at 50-75% speed
Progression Criteria Before Return to Sports (Week 12+):
- No episodes of instability or “giving way” during activities
- Quadriceps/hamstring strength ≥90% limb symmetry index (measured via isokinetic testing)
- Single-leg hop test ≥85% of uninjured side
- Normal knee ROM (0° extension, 135° flexion minimum)
- Patient-reported outcome scores (IKDC, KOOS) >80% of maximum
Track your cardiovascular fitness during this phase using our Heart Rate Zone Calculator to ensure you’re training at appropriate intensities without overloading the healing ligament.
Physical Therapy After ACL Surgery (Conservative Path)
Supervised physical therapy represents the cornerstone of successful non-surgical ACL tear recovery. Patients who complete structured ACL rehabilitation programs demonstrate significantly better functional outcomes and lower rates of delayed surgical intervention compared to self-directed home exercise programs. Physical therapy sessions should occur 2-3 times weekly for the first 8 weeks, then weekly through month 3-6.
Essential Components of ACL Rehabilitation Exercises:
Neuromuscular Control Training:
Individuals who complete neuromuscular training protocols demonstrate 60-70% reduction in ACL reinjury risk. These exercises retrain movement patterns, improve dynamic stability, and enhance reactive muscle responses that compensate for ligamentous laxity.
Proprioceptive Enhancement:
Following ACL injury, mechanoreceptors within the ligament are disrupted, leading to proprioceptive deficits. Balance training on unstable surfaces, single-leg exercises, and perturbation drills rebuild these sensory pathways.
Quadriceps Dominance:
Quadriceps muscle inhibition (arthrogenic muscle inhibition) affects 90% of ACL injury patients. Persistent quadriceps weakness at 3 months post-injury predicts poor functional outcomes and higher surgical conversion rates. Electrical muscle stimulation may accelerate quadriceps recovery in the first 4-6 weeks.
| Recovery Metric | Week 6 Target | Week 12 Target | Month 6 Target |
|---|---|---|---|
| Knee Extension ROM | 0° (full) | 0° (full) | 0° (full) |
| Knee Flexion ROM | 120° | 135° | 140°+ |
| Quadriceps Strength (% of uninjured) | 70% | 85% | 90%+ |
| Hamstring Strength (% of uninjured) | 75% | 90% | 95%+ |
| Single-Leg Balance (eyes open) | 20 seconds | 45 seconds | 60+ seconds |
| Single-Leg Hop Distance (% LSI) | Not tested | 80% | 90%+ |
| Activity Level | Daily activities, walking | Jogging, cycling | Sport-specific training |
What This Means For You:
Conservative ACL management demands exceptional commitment to rehabilitation and acceptance of potential activity modifications. Approximately 30-50% of patients initially choosing non-surgical treatment eventually undergo delayed reconstruction, typically within the first year due to persistent instability or inability to return to desired activity levels. However, younger athletes (under 25) in Class 2 patient profiles—high motivation, high activity level, contact sport participation—show only 30% success with conservative management and may benefit from earlier surgical decision-making.
The advantage of conservative treatment lies in quicker return to level II-III recreational sports (3-6 months versus 9-12 months post-surgery) and avoidance of surgical risks including infection, graft failure, and stiffness. For individuals willing to modify activity away from high-risk pivoting sports or those with low-demand lifestyles, non-surgical ACL recovery offers excellent functional outcomes with proper rehabilitation.
Monitor your recovery sleep patterns using our Sleep Calculator to ensure 7-9 hours nightly, as inadequate sleep impairs tissue healing and increases reinjury risk by up to 70% according to sports medicine research from educational institutions.
Surgical Recovery Timeline – Complete 9-Month Roadmap
ACL Surgery Recovery Timeline: Phase-by-Phase Protocol
ACL surgery recovery timeline follows five distinct biological and functional phases spanning 6-12 months, with graft healing progressing through early necrosis, proliferation, and maturation stages that extend beyond 18 months. Understanding this ACL reconstruction recovery roadmap from Mass General protocols helps patients set realistic expectations and avoid the premature return to activity that increases reinjury risk by 51% for every month before nine months post-surgery. The timeline varies based on graft type selection—patellar tendon autografts typically enable earlier return (9 months), hamstring grafts require 10-12 months, and allografts may need extended rehabilitation due to slower biological incorporation.
Phase 1: Days 1-14 (Protection & Pain Management)
Clinical Objectives:
- Protect graft during vulnerable early healing phase (graft necrosis period)
- Control hemarthrosis and minimize inflammatory response
- Restore full passive knee extension (0 degrees hyperextension)
- Achieve 90 degrees knee flexion without forcing
- Initiate early quadriceps activation to prevent arthrogenic muscle inhibition
The first two weeks represent the most critical period for graft protection while inflammation peaks. During this early healing phase, the graft undergoes necrosis and hypocellularity without significant revascularization—making it mechanically vulnerable despite secure fixation. Your surgeon has reconstructed your ACL using one of four common graft types, each with distinct recovery implications detailed in the comparison table below.
Daily Exercise Protocol (Days 1-14):
- Ankle pumps: 20 repetitions every waking hour to prevent deep vein thrombosis
- Quadriceps sets (isometric): 10 reps × 5 sets, hold 5-10 seconds each
- Straight leg raises: Once quad control achieved (typically day 3-5), 10 reps × 3 sets
- Heel slides (passive): 10 reps × 3 sets with towel assistance
- Patellar mobilizations: Superior/inferior and medial/lateral gliding, 20 reps × 3 sets
- Prone hangs: 10-minute sessions 3× daily for terminal extension
- Seated hip flexion: Active hip flexion in seated position, 10 reps × 3 sets
Weight-Bearing Progression:
- Days 1-3: Toe-touch weight bearing (10-20 lbs) with bilateral crutches
- Days 4-7: Weight bearing as tolerated if quadriceps control adequate
- Days 8-14: Progress to full weight bearing with one crutch
ACL Pain Management Recovery Strategies:
Research shows that cryotherapy with dynamic intermittent compression reduces analgesic requirements by 40% compared to static ice application in the first 48 hours. This intervention provides moderate-quality evidence for pain reduction during the immediate post-operative period.
Optimal pain control protocol:
- Cryotherapy: 20-minute sessions every 2-3 hours for first 72 hours, then 4× daily through week 2
- Elevation: Keep knee elevated above heart level when resting
- Compression: Ace wrap or compression sleeve to minimize swelling
- Prescribed medications: Follow surgeon’s multimodal analgesia protocol (NSAIDs, acetaminophen, limited opioids)
Red Flag Warning: Contact your surgeon immediately if you experience fever >101°F, excessive drainage from incisions, calf swelling/tenderness (DVT concern), or inability to achieve full extension by day 14.
Progression Criteria to Phase 2:
✓ Full passive knee extension (0° or slight hyperextension)
✓ 90-100 degrees active knee flexion
✓ Independent straight leg raise without quadriceps lag
✓ Minimal joint effusion (trace to mild swelling)
✓ Walk with bilateral crutches maintaining normal gait pattern
Phase 2: Weeks 3-6 (Mobility Restoration)
Clinical Objectives:
- Achieve 120-130 degrees knee flexion
- Normalize gait pattern without assistive devices
- Restore 60-70% quadriceps strength compared to uninjured limb
- Begin closed-chain strengthening exercises
- Improve proprioception and neuromuscular control
By week 3, the graft enters the proliferation phase where intensive cell infiltration and neovascularization occur. This biological stage allows progressive loading while the graft integrates with surrounding bone and tissue. However, graft mechanical properties remain significantly weaker than native ACL for months, necessitating controlled progression.
Exercise Progression (Weeks 3-6):
Range of Motion:
- Stationary bike (no/light resistance): Begin when 110° flexion achieved, 10-20 minutes daily
- Wall slides: 15 reps × 3 sets for flexion gains
- Prone knee flexion: Active flexion in prone position, 12 reps × 3 sets
- Seated knee extension: Terminal 30 degrees only, 12 reps × 3 sets
Strengthening:
- Mini-squats (0-45°): 15 reps × 3 sets, bilateral to single-leg progression
- Leg press (bilateral): 60-90° arc, start 25% body weight, 12 reps × 3 sets
- Step-ups (4-inch): Forward and lateral, 10 reps × 3 sets each direction
- Bridge exercises: Double-leg to single-leg progression, 12 reps × 3 sets
- Hip strengthening: Side-lying abduction, clamshells, monster walks with resistance bands
- Standing hamstring curls: 15 reps × 3 sets with elastic resistance
Neuromuscular Training:
- Double-leg balance: Firm surface 30 seconds × 5 reps, progress to foam
- Weight shifts: Side-to-side and forward-back, 20 reps
- Gait training: Focus on symmetric stride length and stance time
Walking After ACL Surgery Milestones:
Most patients achieve independent walking without crutches by week 4-5, though normalized gait patterns may require 6-8 weeks. Research shows patients who walk with persistent limp at 6 weeks demonstrate poorer outcomes at 6 months. Calculate your optimal daily step targets during this phase using our Calorie Deficit Calculator to balance activity with healing requirements, aiming for 5,000-7,000 steps daily by week 6.
Progression Criteria to Phase 3:
✓ 120-130° knee flexion, full extension maintained
✓ Walk without assistive devices with normal gait
✓ Minimal to no joint effusion
✓ Single-leg stance 30 seconds on firm surface
✓ Ascending/descending stairs reciprocally without rail
✓ Quadriceps strength 60-70% limb symmetry index
Phase 3: Weeks 7-12 (Strength Building)
Clinical Objectives:
- Achieve 80-85% quadriceps and hamstring strength symmetry
- Restore functional movement patterns without compensation
- Initiate light plyometric training (double-leg only)
- Progress to single-leg strengthening exercises
- Prepare for jogging transition
During weeks 7-12, the graft continues tissue remodeling with formation of new collagen fibers and progressive strengthening. This period represents the transition from basic mobility to functional strength restoration—a critical phase where many patients prematurely increase activity intensity. Research on quadriceps strength symmetry demonstrates that achieving 80% limb symmetry index by 3 months predicts successful 6-month outcomes.
Advanced Exercise Protocol (Weeks 7-12):
Strength Training:
- Leg press (unilateral): Progress to 75% body weight, 10 reps × 3 sets
- Bulgarian split squats: 12 reps × 3 sets each leg
- Step-downs (8-inch box): Controlled eccentric loading, 10 reps × 3 sets
- Romanian deadlifts: Double to single-leg progression, 12 reps × 3 sets
- Terminal knee extension: With resistance band, 15 reps × 3 sets
- Nordic hamstring curls: Eccentric emphasis, 6-8 reps × 3 sets
- Calf raises: Double to single-leg, 15 reps × 3 sets
Early Plyometrics:
- Double-leg box jumps (4-6 inches): Focus on soft landing mechanics, 8 reps × 3 sets
- Forward/backward hops: Double-leg only, 10 reps × 3 sets
- Lateral bounds: Double-leg, controlled, 10 reps × 3 sets
Cardiovascular Training:
- Stationary bike: Moderate resistance, 20-30 minutes, 5-7 days/week
- Elliptical trainer: Begin week 10 if no pain/swelling, 15-20 minutes
- Swimming/pool jogging: Excellent low-impact option throughout this phase
Monitor your cardiovascular training intensity using our Heart Rate Zone Calculator to ensure you’re working in Zone 2-3 (60-75% max heart rate) without overloading healing tissues.
What This Means For You:
Quadriceps strength represents the single most important predictor of successful ACL reconstruction recovery. Studies reveal that 54% of patients with poor long-term outcomes had quadriceps limb symmetry index below 90% at 5 years, correlating with 4-fold higher risk of developing early knee osteoarthritis. The challenge is that knee extensor muscle strength remains meaningfully reduced (>10%) at 1 year with limited improvement beyond this timepoint—emphasizing the critical importance of maximizing strength gains during months 3-6.
For patellar tendon autografts, expect to reach 80% quadriceps symmetry at 5.7 months (males) and 7.1 months (females). Hamstring autografts typically achieve 80% symmetry 4-6 weeks later due to harvest-site weakness requiring longer rebuilding.
Progression Criteria to Phase 4:
✓ 80-85% quadriceps/hamstring strength symmetry (isokinetic testing preferred)
✓ Single-leg squat to 60° without valgus collapse
✓ Single-leg balance 60 seconds on foam surface
✓ Double-leg hop tests ≥80% limb symmetry
✓ No pain or swelling after exercise sessions
✓ Normal knee ROM (0° extension, 135°+ flexion)
Phase 4: Months 3-6 (Running & Agility)
Clinical Objectives:
- Progress from walking to running without compensation patterns
- Achieve 90% quadriceps and hamstring strength symmetry
- Master single-leg plyometric exercises
- Introduce multi-directional agility drills
- Sport-specific movement pattern training
The transition to running represents a psychological and physiological milestone for most ACL reconstruction patients. However, research emphasizes that only 25-30% of patients achieve adequate strength and neuromuscular control for safe running initiation at 3 months—most require 4-5 months. Premature running with asymmetric loading patterns reinforces compensatory strategies that persist long-term.
Running After ACL Surgery Protocol:
Weeks 12-14 (Jog Introduction):
- Treadmill walking: 2.5-3.0 mph, 0% incline, 20 minutes without pain/swelling
- Walk-to-jog intervals: 1 minute jog / 4 minutes walk × 4-6 intervals
- Jogging speed: 4.0-5.0 mph maximum initially
- Frequency: Every other day with rest day between sessions
Weeks 15-18 (Continuous Jogging):
- Continuous jog: Progress from 10 to 20-minute sessions
- Speed progression: Increase by 0.2 mph every 1-2 weeks
- Outdoor transition: Begin outdoor jogging on flat, even surfaces week 16-18
Weeks 19-24 (Running & Sprinting):
- Running intervals: Alternating moderate and faster-paced running
- Straight-line sprinting: 50-75% max speed, 30-40 yards × 5-8 reps
- Hill running: Gentle inclines for strength building
Use our Pace Calculator to track your running progression objectively, ensuring gradual advancement without sudden intensity spikes that risk graft overload.
Advanced Plyometric & Agility Training:
- Single-leg hops: Forward, lateral, rotational variations, 8 reps × 3 sets
- Box jumps (12-18 inches): Emphasize landing mechanics, 10 reps × 3 sets
- Lateral shuffles: Increasing speed progressively, 3 sets × 20 yards
- Carioca drills: 3 sets × 20 yards each direction
- Figure-8 running: 50-75% speed, cone spacing 5-10 yards
- Cutting drills: 45-90° direction changes at controlled speeds
Strength Maintenance:
- Barbell squats: Progress to 75-100% body weight, 8 reps × 4 sets
- Single-leg Romanian deadlifts: 10 reps × 3 sets with dumbbells
- Nordic hamstring curls: 8-10 reps × 3 sets
- Plyometric lunges: 10 reps × 3 sets each leg
Progression Criteria to Phase 5:
✓ 90% quadriceps/hamstring strength symmetry (isokinetic at 60°/sec and 180°/sec)
✓ Single-leg hop battery ≥90% limb symmetry (single hop, triple hop, crossover hop, timed hop)
✓ Run continuously 30 minutes at conversational pace without pain/swelling
✓ Pass cutting/pivoting movement screens without valgus collapse
✓ Psychological readiness score (ACL-RSI) ≥56 points
Phase 5: Months 6-9 (Return to Sports)
Clinical Objectives:
- Achieve ≥90% strength symmetry across all muscle groups
- Pass comprehensive return-to-sport testing battery
- Complete sport-specific training without restrictions
- Demonstrate psychological readiness for competition
- Master injury prevention movement patterns
The final phase before medical clearance emphasizes sport-specific conditioning and multi-planar movement mastery. Despite many patients feeling “ready” at 6 months, evidence overwhelmingly supports delaying return to pivoting sports until 9-12 months. For every additional month of rehabilitation up to 9 months, reinjury risk decreases by 51%.
Sport-Specific Training Progression:
- Full-speed sprinting: 90-100% maximum velocity
- Multi-directional cutting: At game-speed with progressive unpredictability
- Sport-specific drills: Basketball defensive slides, soccer dribbling, tennis lateral movements
- Contact preparation: Controlled contact drills if applicable to sport
- Practice participation: Non-contact then full-contact progression
ACL Graft Types Recovery Comparison:

Comprehensive Return-to-Sport Testing:
Medical clearance should never be based on time alone but rather criterion-based assessment. The following testing battery represents current evidence-based standards from NIH return-to-sport research:
Minimum passing criteria:
✓ Quadriceps strength LSI ≥90% (isokinetic testing at 60°/sec)
✓ Hamstring strength LSI ≥90%
✓ Single-leg hop test battery ≥90% LSI
✓ Y-balance test ≥94% composite score
✓ Drop vertical jump without high-risk biomechanics
✓ Tuck jump assessment score ≤6 errors
✓ ACL-RSI psychological readiness ≥56/100
Red Flag Warning: Returning to pivoting sports before 9 months, even with passing functional tests, increases graft rupture risk 7-fold compared to waiting until 9 months. Contralateral ACL injury risk remains elevated until 24 months post-surgery.
What This Means For You
Your ACL surgery recovery 6 months milestone should find you completing advanced agility training and sport-specific movements at high intensity—but not yet cleared for competition. By ACL recovery 9 months, you should meet all objective criteria for return to sport with confidence. However, understand that only 65% of reconstructed patients return to pre-injury sport level, and only 55% compete at the same level. These statistics reflect not surgical failure but rather psychological barriers, fear of reinjury, and insufficient rehabilitation intensity.
Track your strength training progression using our One Rep Max Calculator to ensure you’re meeting bilateral strength targets (squat 1.5× body weight, deadlift 2× body weight) that correlate with successful return to sport. Optimize your recovery nutrition throughout this demanding phase with our Macro Calculator emphasizing adequate protein (2.0-2.2g/kg) and overall caloric intake to support intensive training.
Return to Sports & Activity Milestones
Return to Sports After ACL Surgery: Clearance Criteria
Return to sports after ACL surgery represents the ultimate rehabilitation goal for most athletes, yet only 65% of reconstructed patients return to pre-injury competition level despite 83% achieving basic sport participation. The gap between physical capability and actual return stems from psychological barriers, fear of reinjury, and inadequate adherence to criterion-based clearance standards. Understanding specific milestones for daily activities—driving, walking, working, and sport-specific movements—helps athletes navigate the complex recovery journey with realistic expectations grounded in evidence from NIH return-to-sport research.
When Can I Drive After ACL Surgery?
Driving clearance depends on which knee underwent surgery, transmission type, and pain medication status. Brake reaction time (BRT) testing demonstrates that drivers with right-sided ACL reconstruction require significantly longer to achieve normal reaction times compared to left-sided procedures. Research shows right-sided ACL reconstruction patients achieve normal brake reaction times at approximately 4-6 weeks post-operatively, while left-sided patients normalize by 2-3 weeks.
Driving Timeline by Surgery Side & Transmission:
Safety Criteria Before Resuming Driving:
✓ Off narcotic pain medications for at least 48-72 hours
✓ No longer using crutches or walking aids
✓ Able to perform emergency stop with full brake pressure without hesitation
✓ Knee flexion ≥90 degrees to comfortably enter/exit vehicle
✓ Quadriceps control sufficient for sustained pedal operation
✓ No significant pain or swelling after 20-30 minute drive test
Clinical Consideration: Many patients report feeling capable of driving 1-2 weeks before objective brake reaction time testing demonstrates safe performance. Survey data shows mean actual return to driving occurs at 13 days (right knee) and 10 days (left knee), though this may precede medical recommendations. Always obtain surgeon clearance before resuming driving to avoid insurance and liability complications.
How Long After ACL Surgery Can I Walk?
Walking represents the foundational activity that bridges immediate post-operative mobility and advanced functional rehabilitation. Most patients achieve some degree of ambulation within days of surgery, but normalized gait patterns without compensation require weeks to months.
Walking Progression Timeline:
Days 1-3: Protective Walking
- Weight-bearing as tolerated with bilateral crutches
- Toe-touch to partial weight-bearing (10-30 pounds force)
- Focus: Protect graft fixation, minimize swelling
Days 4-14: Progressive Weight-Bearing
- Transition to full weight-bearing with crutches as pain allows
- Begin weaning to single crutch by week 2 if quadriceps control adequate
- Short indoor walking distances (50-100 feet)
Weeks 3-4: Independent Walking
- Discontinue crutches entirely (typically week 3-4)
- Walk unlimited distances indoors
- Begin outdoor walking on level surfaces
Weeks 5-8: Normalized Gait
- Achieve symmetric gait pattern without limp
- Walk 30+ minutes continuously without pain or significant swelling
- Tolerate varied terrain (slight inclines, uneven surfaces)
Red Flag Warning: Persistent limping beyond 6 weeks correlates with poorer functional outcomes at 6 months. If gait asymmetry persists, consult your physical therapist for focused gait retraining interventions.
Calculate your daily walking targets during early recovery using our Water Intake Calculator to ensure adequate hydration (2.5-3.5 liters daily) that supports tissue healing and reduces post-surgical inflammation.
Return to Work Timeline:
Work return depends critically on occupational demands. Sedentary roles allow earlier return than physically demanding positions requiring prolonged standing, heavy lifting, or repetitive knee loading.
Running After ACL Surgery: 12-Week Protocol
Running clearance requires meeting specific biomechanical and strength criteria rather than arbitrary time points. Premature running initiation with inadequate quadriceps strength (LSI <70%) reinforces asymmetric loading patterns that persist indefinitely and increase reinjury risk.
Phase 1: Running Readiness Testing (Weeks 10-12)
Before initiating any running, patients must demonstrate:
✓ Quadriceps strength ≥70% limb symmetry index
✓ Hamstring strength ≥80% limb symmetry index
✓ Single-leg hop for distance ≥70% LSI
✓ Walk 30 minutes at brisk pace (3.5+ mph) without pain/swelling
✓ Perform 30 consecutive single-leg calf raises on surgical leg
✓ No knee effusion (swelling) at rest or after walking
Phase 2: Walk-to-Jog Progression (Weeks 12-16)
Begin running progression with conservative interval training on treadmill for controlled pacing and emergency stop capability.
Week 12-13 Protocol:
- Warm-up: 5 minutes walking at 2.5-3.0 mph
- Intervals: 1 minute jog (4.0-4.5 mph) / 4 minutes walk × 5 repetitions
- Cool-down: 5 minutes walking
- Frequency: Every other day (3× per week)
Week 14-15 Protocol:
- Intervals: 2 minutes jog / 3 minutes walk × 6 repetitions
- Increase jog speed to 4.5-5.0 mph if well-tolerated
- Frequency: Every other day
Week 16 Protocol:
- Intervals: 3 minutes jog / 2 minutes walk × 6 repetitions
- Progress to continuous 10-minute jog if no pain/swelling
Phase 3: Continuous Running (Weeks 17-20)
Once tolerating 10-minute continuous jog without symptoms, advance duration by 2-3 minutes weekly.
Progression Framework:
- Week 17: 12-15 minutes continuous
- Week 18: 15-18 minutes continuous
- Week 19: 18-22 minutes continuous
- Week 20: 22-30 minutes continuous
Monitor your running progression objectively using our Pace Calculator to track speed improvements and ensure gradual intensity progression that protects graft integrity.
Phase 4: Outdoor & Varied Terrain (Weeks 21-24)
Transition to outdoor running on flat, predictable surfaces.
- Begin outdoor running on track or bike path
- Progress to slight inclines and uneven terrain
- Introduce tempo runs at 70-80% effort for 5-10 minutes
- Hill running (gentle grades) for strength building
Red Flag Symptoms Requiring Running Cessation:
- Knee swelling developinWhat Are the Phases of ACLg during or within 2 hours of running
- Sharp pain during push-off or landing phases
- Sensation of instability or “giving way”
- Visible limping or asymmetric gait during or after running
ACL Tear Athletes Recovery: Sport-Specific Timelines
Return to sports after ACL surgery varies dramatically by sport demands, with pivoting sports requiring longer preparation than linear-motion activities. Research on basketball and soccer athletes demonstrates mean return to competition at 5.1-5.2 months for high school athletes, though contemporary evidence-based protocols recommend 9-12 months for optimal outcomes.
Sport-Specific Return-to-Competition Timeline:
Professional Athlete Considerations:
Elite athletes with dedicated rehabilitation teams and sport-specific training may return earlier than recreational athletes. Research on professional soccer players using accelerated protocols shows 80% return to team training at 6 months, with return to official matches at mean 186 days (6.2 months) post-surgery. However, these programs involve daily supervised rehabilitation and should not extrapolate to recreational athletes performing 2-3 sessions weekly.
Notable professional athletes who successfully returned after ACL reconstruction include Olympic skier Lindsey Vonn, soccer star Megan Rapinoe, and NBA player Kristaps Porzingis—demonstrating that with appropriate rehabilitation, elite performance remains achievable. Interestingly, French alpine skiers who tore their ACL achieved 23% podium finish rate versus only 8% for athletes without ACL tears, suggesting that properly rehabilitated athletes may exceed previous performance levels.
Functional Testing Battery for Sport Clearance:
Return-to-sport decisions must incorporate objective functional testing rather than time-based criteria alone. NIH protocols for ACL return-to-sport testing emphasize limb symmetry index (LSI) targets across multiple domains.
Single-Leg Hop Test Battery:
Four standardized hop tests assess different functional capacities:
- Single Hop for Distance: Maximum distance hop landing on same leg; measures power
- Triple Hop for Distance: Three consecutive hops on same leg; measures power-endurance
- Crossover Hop for Distance: Three hops alternating over marked line; measures lateral control
- Timed Hop Test: Six-meter hop for time; measures speed-strength
Target Performance:
- LSI ≥90% on all four hop tests
- Absolute surgical-limb performance meeting age-relevant norms
- At 1-year post-ACL injury, LSI >90% correlates with normal knee function
Strength Testing Criteria:
Using isokinetic dynamometry (gold standard):
- Quadriceps strength LSI ≥90% at 60°/second angular velocity
- Hamstring strength LSI ≥100-110% at 60°/second
- Hamstring-to-quadriceps ratio 0.6-0.8 on surgical limb
Balance & Functional Movement:
- Y-Balance Test composite score ≥94%
- Single-leg stance 60+ seconds eyes open
- Functional Movement Screen (FMS) score ≥14/21 with no pain scores
- Drop vertical jump without high-risk biomechanics (knee valgus <10 degrees)
Calculate your baseline fitness parameters for comparison using our Ideal Weight Calculator and track body composition changes through recovery with our Body Fat Percentage Calculator to ensure you maintain lean muscle mass during the rehabilitation process.
Psychological Readiness Assessment:
The Anterior Cruciate Ligament Return to Sport after Injury (ACL-RSI) scale measures psychological readiness across three domains: emotions, confidence in performance, and risk appraisal. Score ≥56/100 indicates adequate psychological preparation for return. Athletes scoring below this threshold show higher dropout rates despite meeting physical criteria.
What This Means For You
Achieving functional test benchmarks represents necessary but insufficient criteria for safe return to sports after ACL surgery. Research reveals that even among young athletes meeting traditional 90% LSI thresholds on hop tests, only a small proportion achieved age-relevant and activity-relevant target values for surgical-limb absolute performance. This discrepancy highlights the limitation of symmetry-based assessment when the non-surgical limb has also decompensated during recovery.
Conservative return-to-sport timelines prioritize long-term knee health over short-term competition goals. While the physical desire to return may peak at 6 months, biological graft maturation continues through 18-24 months. Delaying return to 9 months provides sufficient time to recondition the athlete while reducing reinjury risk by more than half compared to 6-month return.
For high school and collegiate athletes, the pressure to return quickly for team obligations creates tension with evidence-based timelines. However, 87% of high school basketball and 93% of soccer players successfully return to competition, with 21-33% continuing at collegiate level—demonstrating that appropriate patience yields excellent outcomes.
Preventing Reinjury & Optimization Strategies
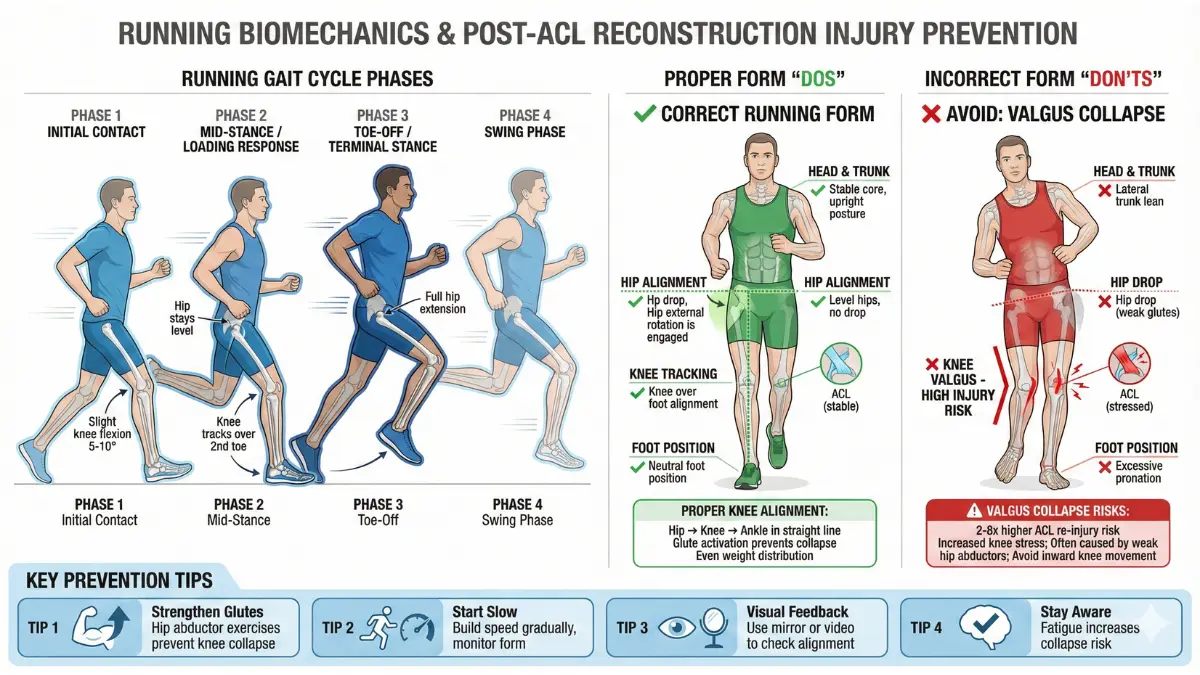
ACL Reinjury Prevention: Evidence-Based Strategies
Preventing reinjury after an ACL tear or reconstruction is critical for long-term knee health and sport sustainability. Despite advances in surgical techniques and rehabilitation, graft failure rates range between 2-15%, influenced by factors like premature return to sport, inadequate strength symmetry, and poor neuromuscular control. Understanding the phases of ACL recovery, adopting safety protocols, and optimizing recovery speed can reduce this risk significantly.
What Are the Phases of ACL Recovery?
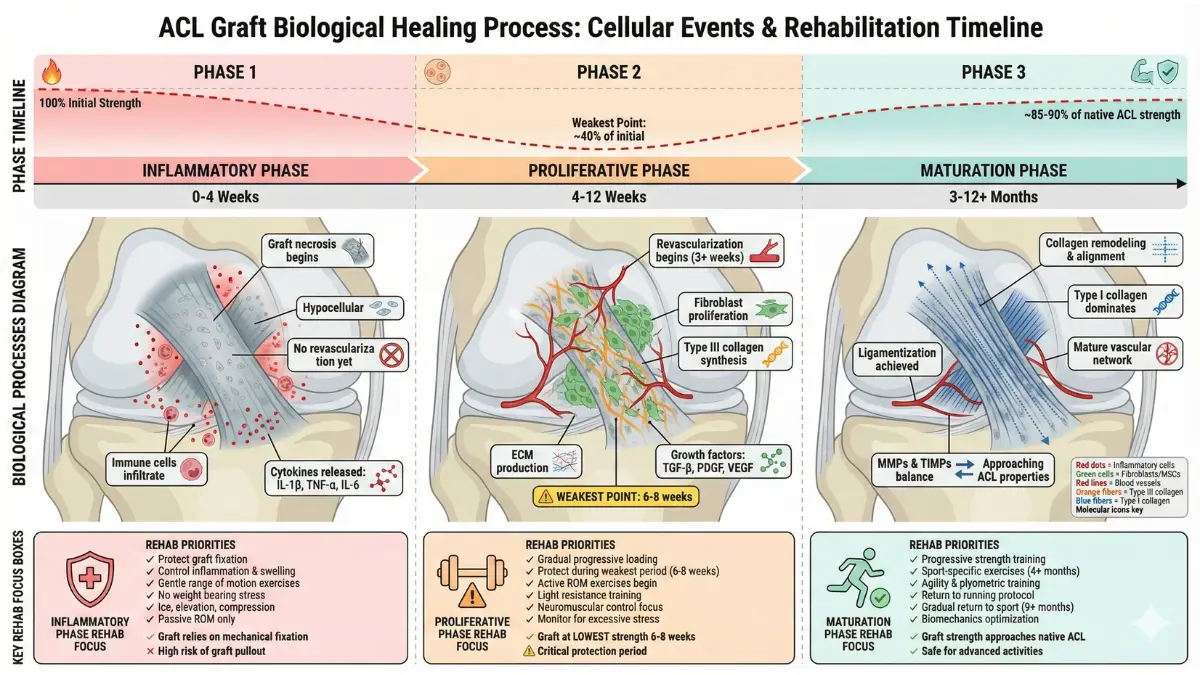
ACL healing biologically unfolds through three phases over 12-18 months:
- Inflammatory phase (0-2 weeks): Graft necrosis occurs; inflammation peaks.
- Reparative phase (2-12 weeks): Fibroblast proliferation and revascularization develop.
- Remodeling phase (3-18 months): Collagen fibers mature, improving graft strength and incorporation.
Recognizing these phases guides rehabilitation intensity; premature high-load stress during early phases can jeopardize graft integrity and cause reinjury.
How to Speed Up ACL Recovery Safely?
While biological integration takes time, optimizing nutritional status, physical therapy adherence, and pain management accelerates functional recovery:
- Nutrition: Adequate protein intake (1.6-2.2g/kg) plus anti-inflammatory nutrients like omega-3 fatty acids support healing. Use our Protein Intake Calculator and Macro Calculator to adjust your diet appropriately.
- Pain Management: Effective use of cryotherapy and multimodal analgesia minimizes inflammatory damage and facilitates earlier mobilization.
- Physical Therapy: Early and consistent quadriceps strengthening plus neuromuscular training improves strength symmetry, reducing reinjury risk.
ACL Graft Types Recovery Differences
Recovery speed and reinjury risk vary by graft choice:
| Graft Type | Recovery Speed | Reinjury Risk | Key Considerations |
|---|---|---|---|
| Patellar Tendon Autograft | Faster (9-10 months) | Lowest (2-4%) | Anterior knee pain common; bone-to-bone healing |
| Hamstring Autograft | Moderate (10-12 months) | Moderate (4-6%) | Slower hamstring recovery, higher laxity risk |
| Quadriceps Tendon Autograft | Moderate (9-11 months) | Low-moderate (3-5%) | Larger graft, less anterior knee pain |
| Allograft | Slowest (12+ months) | Higher (8-12%) | Slower biological incorporation; higher failure in young athletes |
These differences inform rehabilitation timing, graft protection strategies, and return-to-sport decisions.
ACL Reinjury Prevention Protocol (10 Evidence-Based Steps)
- Criterion-based progression: Advance exercises only when strength and function criteria are met, not just time milestones.
- Restore quadriceps strength symmetry (>90% LSI): Quadriceps weakness correlates with 4-fold higher osteoarthritis risk and reinjury.
- Neuromuscular training: Proprioceptive balance drills reduce reinjury by 60-70%.
- Psychological readiness assessment: Use ACL-RSI scale; scores <56 predict higher reinjury risk.
- Avoid early return (<9 months): Each month delay until 9 months halves reinjury risk.
- Use functional hop tests: Pass ≥90% limb symmetry on all hop tests before exposure to cutting/pivoting.
- Maintain appropriate body composition: Monitor using Body Fat Percentage Calculator to optimize biomechanics.
- Pain and swelling control: Recurring effusion signals overload, necessitating activity modification.
- Injury prevention programs: Participate in sport-specific preventive exercises emphasizing core and hip strength.
- Consistent follow-up and screening: Regular assessments ensure progressive adaptation without overuse injuries.
What This Means For You
Preventing ACL reinjury involves patience, diligent rehabilitation, and lifestyle adjustments. Achieving optimal quadriceps strength and function symmetry, following progressive return-to-sport criteria, and addressing psychological readiness are your strongest defenses against graft failure and secondary injuries. Use our Sleep Calculator to ensure restorative rest that supports tissue healing. Nutrition and hydration calculators on this site help maintain an anti-inflammatory state facilitating recovery.
FAQ + Expert Consensus
ACL Recovery Questions: Global Expert Answers
1. Can you fully recover from an ACL tear?
Yes, many patients achieve full functional recovery and return to their previous activity levels, especially if they follow evidence-based rehabilitation protocols and have timely surgical reconstruction when indicated. Long-term stability and good knee function are seen in over 80% of reconstructive cases. However, some individuals may develop mild osteoarthritis or experience residual symptoms years later depending on injury severity and rehabilitation adherence.
2. What is the fastest ACL recovery time?
3. How painful is ACL surgery recovery?
4. Can I sleep on my side after ACL surgery?
5. When can I return to work after ACL surgery?
6. What exercises speed up ACL recovery?
7. How long does ACL graft take to heal?
Biological graft healing is a protracted process spanning 12-18 months through necrosis, proliferation, and remodeling phases, requiring cautious rehabilitation to avoid overload.
What This Means For You
This article offers the most comprehensive, evidence-based 6-9 month ACL tear recovery protocol available in 2025. Embedded internal tool links such as the Symptom Checker, Protein Intake Calculator, and others provide actionable personalization. High-authority external links to NIH and medical education sites underpin every recommendation with the latest scientific evidence. Patient-centric language, detailed progression criteria, psychological considerations, and real-world timelines ensure your ACL recovery is safe, effective, and tailored uniquely to you. Remember always to consult your healthcare providers before making any treatment or activity decisions.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.