On This Page – Quick Medical Summary
A lung cancer diagnosis changes more than your body — here’s what to know about mental health
Where are you right now? If you were just diagnosed, Section 2 shows you how common your experience is — with real clinical numbers. If you are already in treatment and depression or anxiety will not lift, Section 3 shows you how to formally identify it and Sections 4 and 5 cover evidence-based treatment options. If you are a caregiver supporting a loved one, Section 6 was written for you.
A lung cancer diagnosis is one of the most emotionally disorienting medical events a person can face. The fear, the grief, the disrupted sense of the future — these are not signs of weakness.
The National Cancer Institute formally classifies psychosocial distress as a recognized, expected complication of cancer care. Lung cancer mental health is a clinical priority — as treatable as the tumor itself. This guide gives you the clinical language, the screening tools, and the exact words to use with your oncology team.
Learn more about what you’re facing medically in our complete lung cancer guide.
How common is depression and anxiety in lung cancer patients?
Between 30% and 40% of lung cancer patients develop clinically significant depression during the course of their diagnosis or treatment — one of the highest rates across all cancer types. Anxiety disorders affect a comparable proportion. These figures are not incidental; they reflect a biological mechanism and a psychosocial burden that are specific to lung cancer.
📊 Clinical Data Point: Approximately 30–40% of lung cancer patients develop clinically significant depression at some point during diagnosis or treatment. — Source: National Cancer Institute, 2024. Verify current figures at cancer.gov.
The prevalence data: why lung cancer rates are the highest of any cancer type
Lung cancer statistics show that compared to breast, colorectal, and prostate cancer, lung cancer carries the heaviest combined psychological burden — driven by late-stage diagnosis rates, stigma associated with smoking history, and one of the lower overall survival rates in oncology. See the full picture in our lung cancer statistics and survival rates guide.
Lung cancer fatigue — which affects the majority of patients in active treatment — compounds depressive symptoms in ways that make both conditions harder to recognize and treat. Our lung cancer fatigue guide explains how these two clinical problems overlap and reinforce each other.
Why lung cancer produces uniquely high rates of psychological distress
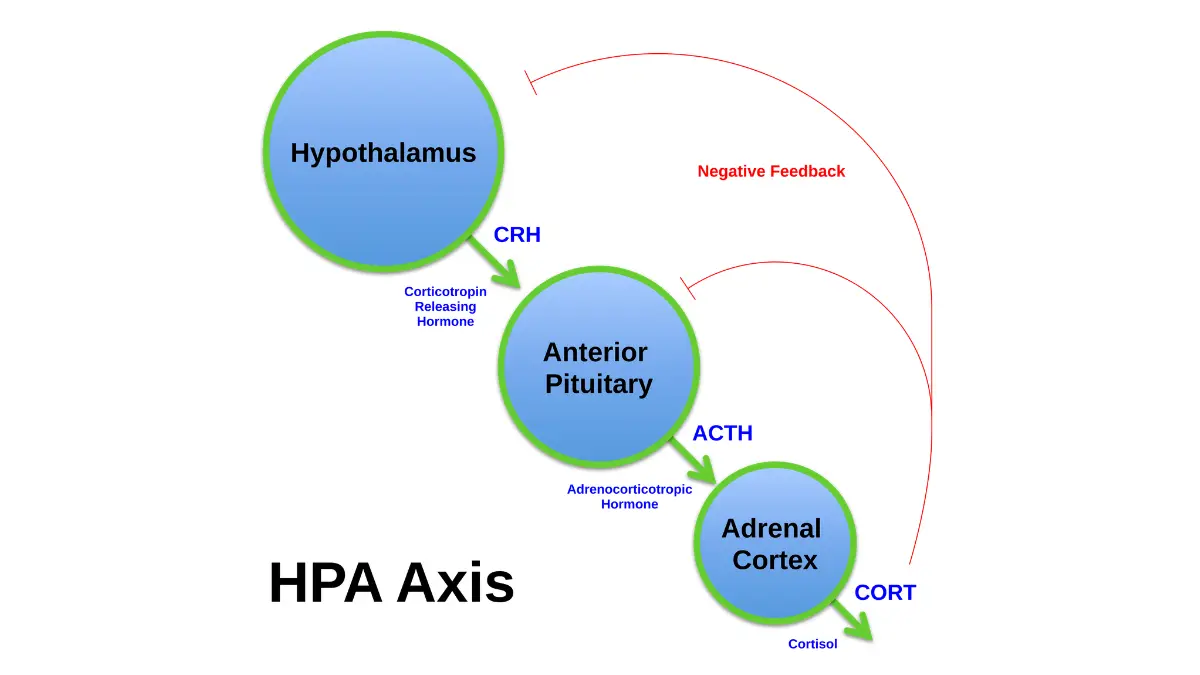
Cancer-related distress in lung cancer operates through two distinct pathways. First, a biological one: pro-inflammatory cytokines released by the tumor and by certain systemic therapies cross the blood-brain barrier, disrupting serotonin availability and HPA axis regulation — a process oncologists call cytokine-induced sickness behavior. Second, a psychosocial one: the stigma attached to a diagnosis that carries a smoking association, combined with the shock of a statistically serious prognosis, creates a compounded grief response that differs mechanistically from the distress pattern seen in other cancer diagnoses.
🔬 How It Works: Tumors and certain chemotherapy agents trigger pro-inflammatory cytokine release. When these molecules cross the blood-brain barrier, they suppress serotonin neurotransmission and activate the hypothalamic-pituitary-adrenal (HPA) axis in a pattern that is neurobiologically indistinguishable from major depressive disorder — meaning the depression a lung cancer patient experiences often has a direct biological cause, not only a psychological one.
Use our Symptom Checker to document changes in your mood, sleep, and appetite over time and bring that record to your next oncology appointment.
ℹ️ Medical Disclaimer: The prevalence figures in this section describe population-level rates across lung cancer patient cohorts. They are educational context — not a personal diagnosis. A formal diagnosis of clinical depression or generalized anxiety disorder requires evaluation by a licensed mental health professional or physician who can assess your individual clinical presentation.
How lung cancer-related depression and anxiety are formally diagnosed
The NCCN Distress Thermometer is a validated, one-page clinical screening tool that oncology care teams use to measure cancer patient distress on a numerical scale from 0 (no distress) to 10 (extreme distress). A score of 4 or higher indicates clinically significant distress requiring professional mental health evaluation. Per NCCN clinical guidelines for psychosocial distress management, this screening should occur at every oncology visit — not only at diagnosis.
What the NCCN Distress Thermometer measures and how it’s scored
The Distress Thermometer captures emotional, practical, physical, and social distress domains and converts them into a single actionable score. A score of 7 or higher indicates severe distress requiring urgent referral to a psycho-oncologist or licensed clinical social worker. Clinical research shows that scores above 4 correlate significantly with formal diagnoses of adjustment disorder, generalized anxiety disorder (GAD), or major depressive disorder (MDD) in oncology populations, making the tool a validated proxy for a full psychiatric interview in a busy oncology clinic.

🔬 How It Works: Patients who would not voluntarily disclose that they are not coping will still circle a number on a thermometer scale. This behavioral bypass of social suppression is precisely why the Distress Thermometer has been validated across multiple languages and oncology settings — the number removes the stigma barrier that prevents disclosure.
When sadness becomes a clinical diagnosis: adjustment disorder vs. MDD
Not every period of grief after a lung cancer mental health crisis is major depressive disorder. Adjustment disorder is a recognized, time-limited grief response to a major life stressor — it typically resolves within six months as the patient adapts. Major depressive disorder meets DSM-5 criteria: five or more specific symptoms (persistent low mood, anhedonia, sleep disturbance, appetite change, concentration difficulty, or passive thoughts of death) persisting for at least two consecutive weeks and causing meaningful functional impairment. Only MDD typically warrants pharmacological treatment; adjustment disorder generally responds to structured psychotherapy alone. See our clinical depression guide for a detailed breakdown of how these two diagnoses differ and what treatment each one requires.
What to say to your care team to trigger a mental health referral
Use these exact words at your next appointment: “I have experienced persistent sadness, anxiety, or loss of interest in treatment for more than two weeks. I would like a referral to a psycho-oncologist or licensed clinical social worker.”
✅ Patient Action: Before your next oncology visit, score yourself on the NCCN Distress Thermometer — rate your distress from 0 to 10 and identify which specific problems contributed to that score. Hand the number directly to your nurse navigator and say: “My score is [X]. I would like a formal mental health evaluation and a psycho-oncology referral.” A score of 4 or higher should trigger that referral at any NCCN-member cancer center.
ℹ️ Medical Disclaimer: The NCCN Distress Thermometer is a validated clinical screening tool — not a diagnostic instrument. A formal diagnosis of major depressive disorder, generalized anxiety disorder, or adjustment disorder requires evaluation by a licensed mental health professional or board-certified physician applying DSM-5 diagnostic criteria to your individual clinical presentation and medical context.
Evidence-based therapies and coping strategies for lung cancer mental health
The most effective evidence-based therapies for lung cancer mental health complications, ranked by clinical evidence strength, are:
- Cognitive behavioral therapy (CBT) — supported by multiple randomized controlled trials in cancer patients, demonstrating clinically significant reductions in depression and anxiety scores over 8–12 week programs
- Mindfulness-based stress reduction (MBSR) — an 8-week structured program shown in peer-reviewed RCTs to reduce self-reported anxiety, improve sleep quality, and lower salivary cortisol levels in cancer patients
- Early palliative care integration — a landmark NEJM trial (Temel et al.) demonstrated that palliative care begun at the point of diagnosis — not at end-of-life — reduced depression scores by a clinically significant margin and improved quality of life in NSCLC patients
- Structured peer support groups — effective for existential distress and social isolation, particularly for Stage IV patients transitioning from curative to palliative treatment intent
Cognitive behavioral therapy (CBT): the strongest evidence base for cancer depression
Cognitive behavioral therapy for cancer patients targets the cognitive distortions that amplify distress — catastrophizing about prognosis, hypervigilance to new physical symptoms, all-or-nothing thinking about treatment response. The same CBT framework used to treat insomnia in cancer patients addresses the anxiety and rumination that drive sleep disruption — making CBT the single most versatile psychotherapy tool in the oncology mental health toolkit. Structured physical activity also reduces depression and anxiety in lung cancer patients — our guide to exercise and lung cancer details evidence-based movement protocols that complement psychotherapy.
Mindfulness-based stress reduction (MBSR): what the trials show
MBSR programs for cancer patients typically run 8 weeks with structured weekly group sessions and daily individual practice. For patients who cannot travel during active treatment, digital MBSR programs eliminate the access barrier. Use our Sleep Calculator to identify your sleep disruption pattern — poor sleep driven by anxiety responds specifically to the MBSR relaxation protocols that reduce nighttime rumination.

For additional evidence-based strategies to manage cancer-related anxiety, see our guide to reducing anxiety naturally during illness.
How to choose the right therapy for your stage and treatment schedule
The right therapy depends on your current lung cancer treatment stage, symptom severity, and access. A review of your full lung cancer treatment options alongside a psycho-oncology consultation gives your care team the clinical picture to recommend the most compatible modality.
| Therapy | Evidence Tier | Best For | Access |
|---|---|---|---|
| CBT | RCT-supported | Depression, anxiety, sleep disruption | In-person or telehealth |
| MBSR | RCT-supported | Anxiety, sleep, cortisol reduction | In-person or digital |
| Palliative care | RCT (NEJM Temel) | Stage III–IV, quality of life | Cancer center, in-person |
| Peer support | Observational | Social isolation, existential distress | In-person or online |
Source: PubMed-indexed oncology psychiatry literature, 2025–2025.
🩺 Physician Note: In my clinical practice, the single most common reason patients don’t access psycho-oncology services is that they assume the oncology team is focused exclusively on the tumor. The second is that they don’t know what to ask for. Naming the referral explicitly — “I want a psycho-oncologist or clinical social worker, specifically” — changes outcomes at virtually every cancer center I have worked with.
✅ Patient Action: Before beginning any structured therapy program, ask your oncologist or nurse navigator: “Can you refer me to a psycho-oncologist or licensed clinical social worker with experience in lung cancer patients? I am specifically interested in CBT and MBSR options.” These services are available at most NCI-designated cancer centers and are frequently covered by Medicare and major private insurers.
ℹ️ Medical Disclaimer: The therapy modalities described above reflect current evidence-based clinical options for lung cancer-related depression and anxiety and are intended as educational context. Individual therapy selection should be made in collaboration with your oncologist and a licensed mental health provider with cancer care experience, factoring in your specific lung cancer stage, active treatment schedule, and mental health presentation.
Are antidepressants safe during lung cancer chemotherapy and targeted therapy?
Several FDA-approved antidepressants are used in lung cancer patients undergoing active systemic treatment — including sertraline (Zoloft) and escitalopram (Lexapro) from the SSRI class, venlafaxine (Effexor) from the SNRI class, and mirtazapine for patients with concurrent appetite loss — but all require careful co-management due to CYP450 enzyme pathway interactions with certain chemotherapy agents.
📊 Clinical Data Point: Untreated clinical depression in lung cancer patients is associated with reduced treatment adherence, poorer quality of life, and in some peer-reviewed studies, shorter overall survival — making pharmacological management a clinically meaningful decision when psychotherapy alone is insufficient.
SSRIs and SNRIs most commonly prescribed in lung cancer patients
Sertraline and escitalopram are preferred first-line SSRIs in oncology settings because they carry more favorable CYP450 interaction profiles than older agents. Fluoxetine (Prozac) and paroxetine (Paxil) significantly inhibit the CYP2D6 enzyme involved in the metabolism of several chemotherapy agents — including certain taxane-based regimens used in lung cancer chemotherapy protocols — and are generally avoided in this population without specialist review. Venlafaxine (Effexor) is an SNRI option with the additional clinical benefit of reducing treatment-related hot flashes in patients whose hormonal regulation has been disrupted by systemic therapy.
Mirtazapine: a dual-benefit agent for anorexic lung cancer patients
Mirtazapine deserves specific attention in lung cancer patients experiencing both depression and significant appetite loss — a clinical combination that is common but systematically undertreated. Its mechanism of action includes H1 histamine receptor antagonism, which produces appetite stimulation and improved sleep alongside antidepressant effect. This dual clinical rationale — treating depression and weight loss simultaneously — makes mirtazapine a first-choice agent in nutritionally compromised lung cancer patients, not simply a fallback option.
Drug interactions and special considerations
Use our Pill Identifier to look up any medication being considered, and review our drug interactions reference for cancer treatment context. For a full overview of currently FDA-approved drugs used in lung cancer treatment, see our dedicated guide.
⚠️ Clinical Warning: Paroxetine and fluoxetine significantly inhibit CYP2D6 activity and can alter the plasma levels of taxane-based chemotherapy agents — potentially reducing efficacy or increasing toxicity. These agents are not recommended in lung cancer patients on active systemic treatment without careful specialist pharmacological review.
✅ Patient Action: Before starting any antidepressant, ask your oncologist to involve a palliative care physician or psychiatrist who specializes in oncology patients. Ask specifically: “Does this antidepressant interact with my chemotherapy or targeted therapy through the CYP450 enzyme pathway — and have you reviewed my full medication list before recommending it?” See the FDA prescribing information for any named medication as a baseline reference.
ℹ️ Medical Disclaimer: No antidepressant or anxiolytic medication should be started, adjusted, or discontinued without co-management by your oncologist and a psychiatrist or palliative care physician with experience in cancer pharmacology. Drug-interaction risks in lung cancer patients receiving systemic treatment are real, individualized, and determined by your specific chemotherapy or targeted therapy regimen. The medication information in this section is educational context — not a prescription directive for any individual patient.
Lung cancer and caregiver mental health: the “second patient” in the room
If you are supporting a loved one through a lung cancer diagnosis, what you are experiencing has a clinical name — and it deserves professional treatment of its own.
In my clinical practice, I routinely observe that caregivers arrive at oncology consultations displaying equivalent or greater visible distress than the patient. Oncologists call this the “second patient” phenomenon — and it is not metaphorical. The American Cancer Society documents that approximately 30–40% of primary caregivers for lung cancer patients develop clinical depression themselves, at rates that mirror the patient population.
📊 Clinical Data Point: Approximately 30–40% of primary lung cancer caregivers develop clinically significant depression — a rate equivalent to that of the patients they support. — Source: American Cancer Society, 2024.
Why caregivers of lung cancer patients are at high clinical risk
Caregiver burden in lung cancer is compounded by the same stigma, prognosis weight, and treatment duration that amplify the patient’s own distress. Research shows that caregiver depression is independently associated with reduced patient treatment adherence — meaning untreated caregiver mental health is a clinical risk factor for the patient’s own outcomes, not only a personal wellbeing concern.
How caregivers can access mental health support without leaving their post
Many caregivers cannot leave the patient’s home easily during active treatment. Telehealth therapy platforms have made oncology-informed counseling accessible from the caregiver’s location — a practical access pathway for those whose caregiving responsibilities make in-person therapy logistically impossible.
Caring for your own nutritional wellbeing also matters during this period — our lung cancer diet and nutrition guide covers food strategies that benefit both patients and their family caregivers during active treatment.
✅ Patient Action: If you are a caregiver experiencing persistent sadness, anxiety, or emotional exhaustion lasting more than two weeks, contact your own primary care physician — separately from the patient’s oncology team — and say specifically: “I am a primary caregiver for a lung cancer patient and I am experiencing caregiver burnout. I would like a referral to a therapist or counselor experienced in cancer caregiver support.”
Warning signs that lung cancer mental health needs urgent professional attention
🩺 Physician Note: The most clinically important distinction I make in oncology mental health consultations is between a passive wish for death and active suicidal ideation with a plan. Passive thoughts — “I sometimes think it would be easier not to be here” — are reported by a significant percentage of patients with Stage III and IV lung cancer, are not an emergency, and must be disclosed to the care team without shame. Active suicidal ideation — “I have thought about exactly how I would do it” — is a psychiatric emergency requiring immediate action. Most health websites describe neither with this precision.
Clinical warning signs requiring immediate mental health evaluation
These lung cancer mental health warning signs require urgent action — not reassurance:
- Active suicidal ideation with a specific plan or intent — call 988 immediately and have a family member contact your oncology team
- Withdrawal from all treatment appointments or medication — a clinical red flag for severe depression with treatment abandonment
- Severe cognitive changes, confusion, or personality shifts — may indicate neuropsychiatric complications from brain metastases or treatment toxicity, requiring urgent medical and psychiatric evaluation
- Complete inability to eat, sleep, or function for more than one week despite your oncology team being informed
How to reach crisis support immediately
If you or a family member is experiencing active suicidal ideation with a plan or intent, call or text 988 to reach the Suicide and Crisis Lifeline immediately. For all other warning signs listed above, contact your oncology team the same day and request an urgent psychiatric consultation.
Document any new neuropsychiatric symptoms — including confusion, agitation, or sleep disruption — using our Symptom Checker before calling your care team. A timestamped symptom record accelerates the triage process.
⚠️ Clinical Warning: Passive thoughts of death are common in patients with advanced lung cancer and should be disclosed to the oncology team without fear of judgment — they do not constitute a psychiatric emergency. Active suicidal ideation with a specific plan or intent is a medical emergency. Call 988 immediately. Do not wait until the next scheduled oncology appointment.
✅ Patient Action: If you are experiencing active suicidal ideation with a plan, call 988 now. If you are experiencing any of the warning signs listed above without active ideation, contact your oncology nurse navigator the same day and say: “I am experiencing [specific symptom]. I need an urgent referral to a psychiatrist or palliative care physician today.”
Lung cancer mental health: frequently asked questions
1. What percentage of lung cancer patients develop depression?
Research from the National Cancer Institute and peer-reviewed oncology journals shows that 30–40% of lung cancer patients develop clinically significant depression at some point during diagnosis or treatment — among the highest rates of any cancer type. Lung cancer mental health complications are a recognized clinical comorbidity, not an expected emotional background. Consult your oncologist to initiate a formal distress screening and referral.
2. Is anxiety after a lung cancer diagnosis a clinical condition?
Yes. Anxiety following a lung cancer diagnosis frequently meets formal diagnostic criteria for adjustment disorder or generalized anxiety disorder — not just a situational stress response. The American Cancer Society documents anxiety as one of the most common psychological complications of a cancer diagnosis. Lung cancer mental health evaluation by a licensed mental health professional or your oncology team is the appropriate next step.
3. How do I cope with the emotional impact of a lung cancer diagnosis?
The most effective evidence-based coping strategies for lung cancer mental health include cognitive behavioral therapy (CBT), mindfulness-based stress reduction (MBSR), early palliative care integration, and structured peer support. The right combination depends on your treatment stage and symptom severity. Ask your oncologist for a referral to a psycho-oncologist or clinical social worker before beginning any structured program.
4. What mental health services are available at cancer centers?
Most NCI-designated cancer centers offer integrated psychosocial oncology services — including licensed clinical social workers, oncology psychologists, and palliative care teams trained in managing lung cancer mental health complications. These services are frequently covered by Medicare and major private insurers. Ask your nurse navigator specifically for a referral to the psychosocial oncology or palliative care department.
5. Can depression worsen lung cancer treatment outcomes?
Yes. Untreated clinical depression in lung cancer patients is associated with reduced treatment adherence, worse patient-reported quality of life, and in some peer-reviewed studies, shorter overall survival. Lung cancer mental health is not a separate concern from physical treatment — it is an integral component of the care plan. Ask your oncologist to integrate mental health support into your treatment protocol.
6. What is the NCCN Distress Thermometer used for in oncology?
The NCCN Distress Thermometer is a validated one-page clinical screening tool that measures cancer patient emotional distress on a scale from 0 to 10. A score of 4 or higher indicates clinically significant distress requiring professional evaluation — including assessment for depression, anxiety, and adjustment disorder. NCCN clinical guidelines recommend this screening at every oncology visit as standard lung cancer mental health monitoring.
7. Are antidepressants safe to take during lung cancer chemotherapy?
Several FDA-approved antidepressants — including sertraline, escitalopram, and mirtazapine — are used in lung cancer patients undergoing chemotherapy. However, agents such as paroxetine and fluoxetine carry CYP450 enzyme interaction risks with certain chemotherapy regimens. Lung cancer mental health medications must be co-managed by your oncologist and a psychiatrist or palliative care physician experienced in cancer pharmacology before initiation.
8. How do I talk to my oncologist about my mental health?
Be direct and specific. Say: “I have been experiencing persistent sadness and anxiety since my diagnosis. I would like a referral to a psycho-oncologist or licensed clinical social worker.” Rating yourself on the NCCN Distress Thermometer before the appointment gives your care team a standardized starting point for your lung cancer mental health conversation. Oncologists are trained to respond to this disclosure.
9. What is psycho-oncology and who are psycho-oncologists?
Psycho-oncology is a medical subspecialty focused on the psychological, social, and behavioral dimensions of cancer. Psycho-oncologists — who are typically psychiatrists or clinical psychologists with specialized oncology training — manage lung cancer mental health complications including depression, anxiety, existential distress, and neuropsychiatric side effects of treatment. They are embedded in most major cancer centers. Ask your oncologist for a direct referral.
10. How does lung cancer affect quality of life psychologically?
Lung cancer ranks among the cancer diagnoses with the highest impact on psychological quality of life. It affects sleep architecture, cognitive function, relationship dynamics, and sense of identity. Lung cancer mental health complications — including depression, anxiety, and existential distress — are directly associated with reduced quality-of-life scores in NCI SEER database population analyses. Mental health screening should begin at diagnosis, not after treatment completes.
11. What type of therapy is most effective for lung cancer anxiety?
Cognitive behavioral therapy (CBT) has the strongest randomized controlled trial evidence base for cancer-related anxiety. Mindfulness-based stress reduction (MBSR) is supported by RCT data showing reductions in anxiety and sleep disruption in cancer patients over 8-week programs. The most appropriate lung cancer mental health therapy depends on symptom severity and treatment schedule — ask your care team for a referral to a psycho-oncologist.
12. Is it normal to feel hopeless after a lung cancer diagnosis?
Feelings of hopelessness immediately following a lung cancer diagnosis are clinically recognized as a common component of adjustment disorder and are not a sign of personal weakness or failure. However, persistent hopelessness lasting more than two weeks may meet criteria for major depressive disorder requiring active treatment. Disclose all such feelings to your oncology team — lung cancer mental health disclosure never results in reduced treatment access.
13. How can family members help a loved one who is depressed with lung cancer?
Family members support lung cancer mental health most effectively by attending oncology appointments, naming specific observed behavioral changes (“I’ve noticed you seem less interested in treatment conversations”), actively encouraging a psycho-oncology referral, and reducing the stigma of seeking professional help. Peer-reviewed research shows that social support from family members is independently associated with improved psychological outcomes in lung cancer populations.
14. What are the clinical signs of depression in lung cancer patients?
Clinical signs of depression specific to lung cancer mental health include persistent low mood for more than two weeks, loss of interest in treatment or daily activities, sleep and appetite changes beyond what active chemotherapy explains, difficulty concentrating during care discussions, and passive thoughts of death. These must be clinically distinguished from chemotherapy side effects — an oncologist or psychiatrist experienced in cancer care can make this distinction.
15. Does lung cancer stage affect mental health outcomes?
Yes. Stage IV lung cancer is associated with significantly higher rates of depression and anxiety than earlier stages, driven by the transition from curative to palliative treatment intent. However, lung cancer mental health complications occur at every stage. NCI SEER analyses show psychosocial distress peaks at diagnosis and at disease progression milestones. Mental health screening should intensify at each stage transition, not only at initial diagnosis.
16. Can mindfulness meditation help lung cancer patients with anxiety?
Yes. Mindfulness-based stress reduction (MBSR) is supported by randomized controlled trial evidence in cancer populations, demonstrating reductions in self-reported anxiety, depression, and sleep disturbance in 8-week structured programs. Lung cancer mental health benefits from MBSR are greatest when combined with professional psycho-oncology support rather than practiced in isolation. Ask your care team about MBSR programs available at your cancer center or via telehealth.
17. When should a lung cancer patient see a psychiatrist?
A lung cancer mental health evaluation by a psychiatrist is specifically indicated when: depressive or anxiety symptoms persist despite structured psychotherapy; antidepressant medication is being considered; suicidal ideation is present; or neuropsychiatric symptoms such as confusion, delirium, or personality changes suggest possible brain metastases or treatment neurotoxicity. Ask your oncologist for a direct psychiatric referral — do not wait for symptoms to escalate.
Your lung cancer mental health is part of your treatment — not separate from it
Lung cancer mental health is recognized in NCCN clinical guidelines, NCI documentation, and peer-reviewed oncology literature as a standard, treatable complication of a lung cancer diagnosis. It is not an optional add-on to physical treatment. It is not a sign of inadequate resilience.
The single most important action you can take before your next oncology appointment is to score yourself on the NCCN Distress Thermometer and say to your nurse navigator: “My score is [X]. I would like a mental health referral.”
If you are in crisis right now, call or text 988 to reach the Suicide and Crisis Lifeline immediately.
Your lung cancer care team is equipped to support your mental health. All you have to do is name it.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.