On This Page – Quick Medical Summary
If you just opened your lab results, saw a PSA test number, and felt your stomach drop, start here. An elevated result is frightening, but a higher-than-expected PSA most often turns out to be something other than cancer.
Where you are right now shapes what you need. If you have a result in hand and want to know whether it’s normal for your age, the age reference table below is for you. If your number looks high and you’re scared, the section on what “high” actually means will put it in context. If you want to know what happens next, there’s a clear, step-by-step pathway further down, and if you’re deciding whether to test at all, the screening section covers that.
This page explains what the test measures, typical ranges by age, and the calm, methodical steps that usually follow an elevated PSA. For the larger picture, our guide to how prostate cancer is staged and treated covers what happens if a diagnosis is ever made.
ℹ️ Medical Disclaimer: This article is general health education, not medical advice, and does not create a clinician–patient relationship. A PSA result can only be interpreted alongside your age, health history, prior readings, and exam findings, so do not diagnose yourself and do not start, stop, or change any screening, testing, or treatment based on this page. Discuss your results and any decisions about a biopsy, imaging, or screening frequency with a board-certified urologist or your primary care clinician.
What is a PSA test and what does the number mean?
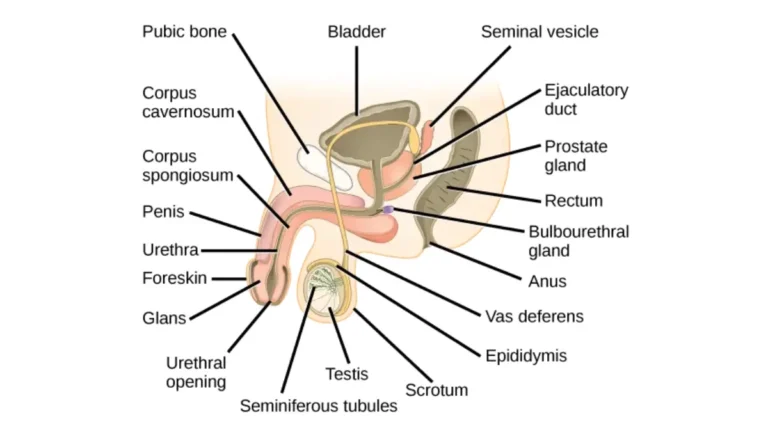
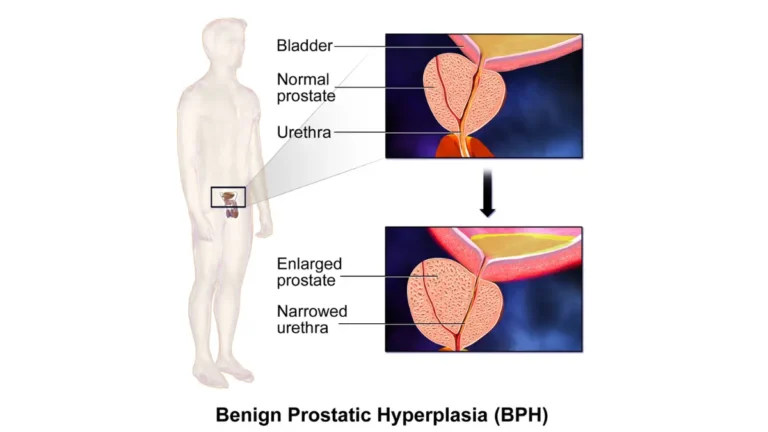
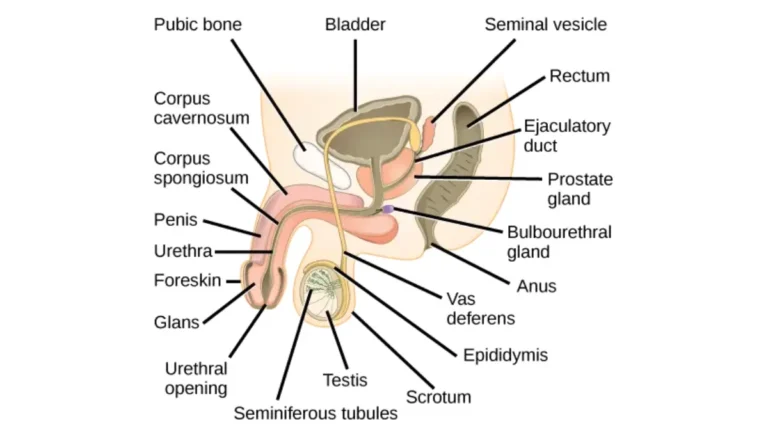
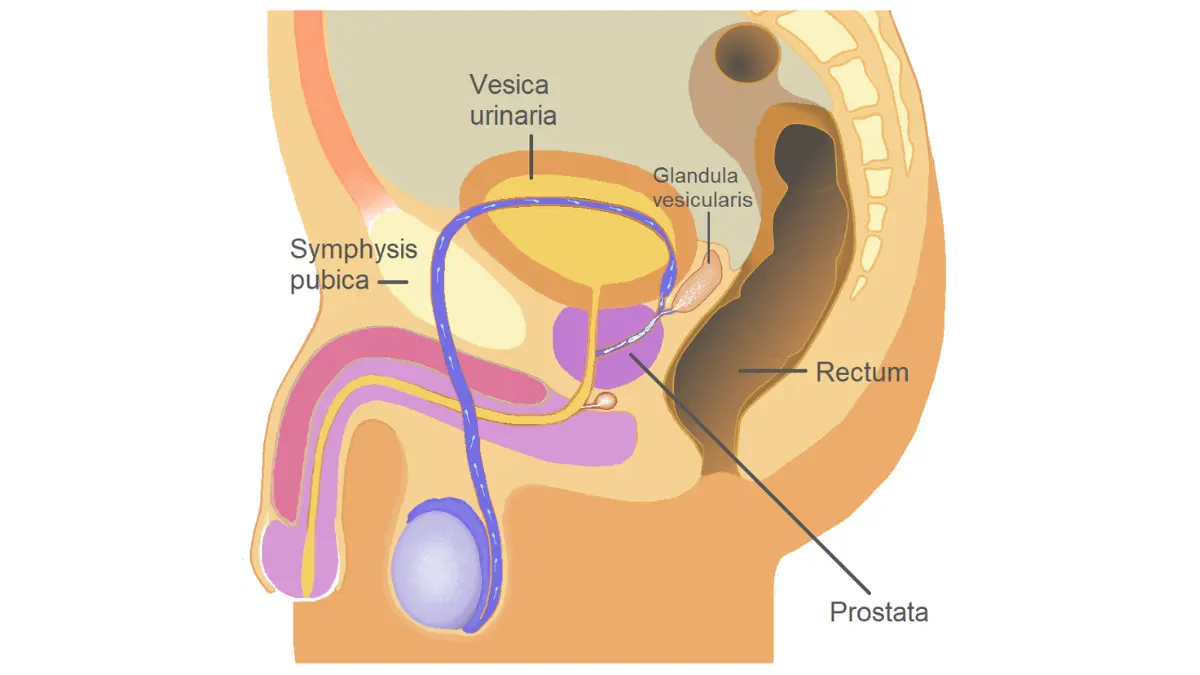
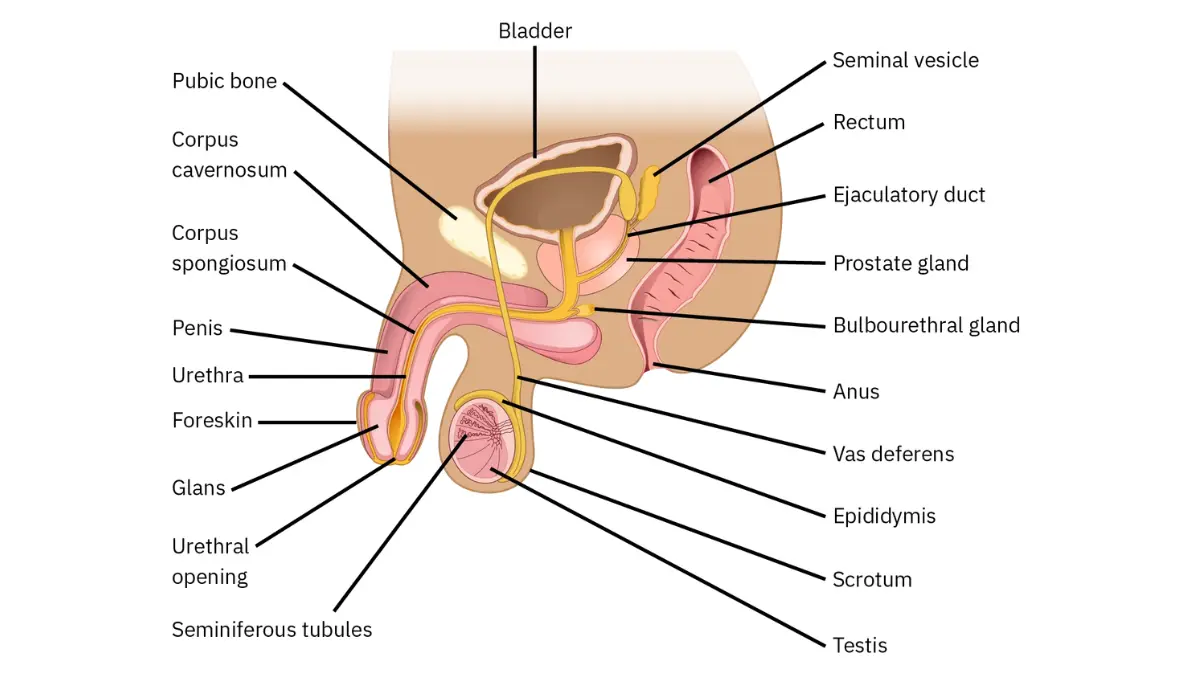
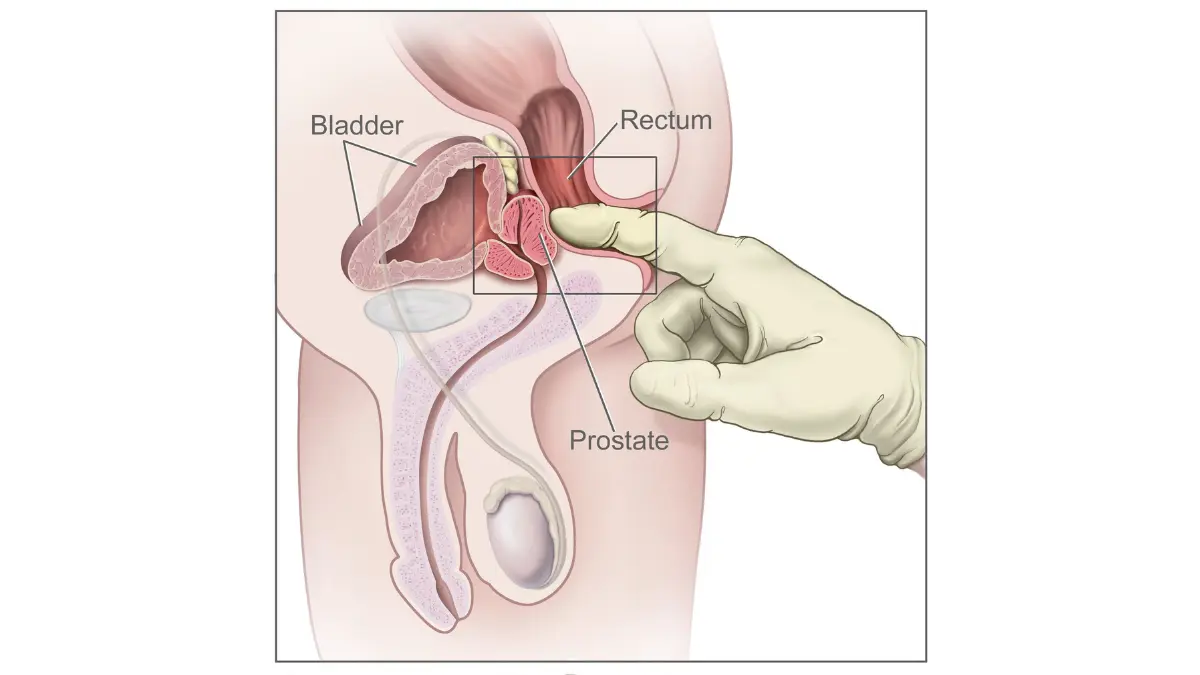
A PSA test is a blood test that measures prostate-specific antigen, a protein made by cells in the prostate gland, a small gland below the bladder that produces part of semen. Results are reported in nanograms per milliliter (ng/mL). Both healthy and cancerous prostate cells make PSA, which is exactly why the number alone cannot confirm or rule out cancer.
🔬 How It Works: A small amount of PSA normally leaks from the prostate into the blood. Anything that disturbs prostate tissue — benign enlargement, inflammation, infection, or cancer — can raise that amount. The test measures the protein, not the cause, so a high reading is a prompt to investigate rather than a diagnosis.
What PSA actually measures
The number reflects how much antigen is circulating, nothing more. According to the National Cancer Institute’s PSA test overview, there is no single level that means a person has cancer, though the likelihood rises as the number goes up.
Total PSA vs. free PSA
Most testing starts with total PSA, the full amount in your blood. A second measure, free PSA — the share circulating unbound — can add information when the total is borderline. A lower proportion of free PSA leans toward higher risk, but your clinician interprets both figures together with your age and exam.
What are normal PSA levels by age?
There is no universal cutoff that defines a “normal” PSA, because the typical range rises with age. Still, clinicians use age reference points as a starting place:
| Age range | Often flagged for a closer look above | Typical median |
|---|---|---|
| 40s–50s | 2.5 ng/mL | ~0.6–0.7 ng/mL |
| 60s | 4.0 ng/mL | ~1.0–1.5 ng/mL |
| 70+ | higher thresholds sometimes used | rises with age |
Reference points adapted from Johns Hopkins Medicine age-specific screening guidance and MD Anderson; confirm against your own history with your clinician.
📊 Clinical Data Point: There is no single PSA threshold that separates “normal” from “abnormal.” — Source: National Cancer Institute. The same number can be reassuring at 70 and worth a closer look at 45.
Why there is no single “normal” number
Some clinicians apply a lower cutoff, around 2.5 ng/mL, for younger men and a higher one, up to roughly 5 ng/mL, for older men. That is because the prostate enlarges with age and naturally releases more PSA, per the National Cancer Institute. Certain medicines for benign enlargement, such as finasteride and dutasteride, lower PSA, so your reading is always read against your own history.
PSA in your 60s and 70s
In your 60s, a reading above about 4.0 ng/mL is commonly flagged, while a younger man’s average sits well under 1.0 ng/mL. What matters most is the trend in your own numbers over time, not a single snapshot.
What counts as a high PSA, and what a high number does and doesn’t mean
A PSA above 4.0 ng/mL is generally considered elevated and may prompt a clinician to recommend further testing, but a high number is a signal to investigate, not a diagnosis. The level of concern rises with the number:
- Under 4 ng/mL: most men without cancer fall here, though the American Cancer Society notes about 15% of men with a low PSA still have cancer found if a biopsy is done.
- 4–10 ng/mL (the “gray zone”): roughly a 1 in 4 chance of cancer, which means about 75% of men in this range do not have it (American Cancer Society).
- Above 10 ng/mL: the likelihood of cancer is higher and a biopsy is generally discussed (Mayo Clinic Laboratories).
🩺 Physician Note: Current guidance stresses that “elevated” does not mean “cancer.” In the borderline 4–10 ng/mL range, most men turn out not to have prostate cancer, which is why clinicians repeat and refine a result before any invasive step.
What free PSA adds
When the total sits in the gray zone and the exam is not suspicious, the free PSA percentage helps refine the picture. A lower share of free PSA leans toward higher risk and a higher share toward a benign cause, according to Mayo Clinic Laboratories.
Things that can falsely raise PSA
Several everyday and medical factors can push PSA up temporarily, including a urinary tract infection or prostate inflammation, a recent prostate biopsy or catheter (which can keep PSA raised for a month or two), vigorous cycling, and recent ejaculation, per the National Cancer Institute. Pairing your number with the early signs of prostate cancer can help you and your clinician decide what to watch.
✅ Patient Action: If your PSA came back elevated, ask your clinician or a urologist: “Given my total PSA, free PSA, and exam, what is my actual risk, and should we repeat the test before any biopsy?”
What to do if your PSA is high: the next steps
An elevated PSA usually starts a measured sequence, not an immediate biopsy. The typical pathway looks like this:
- Repeat the PSA. For a newly elevated result, guidelines advise repeating the blood test before any biomarker, imaging, or biopsy (AUA/SUO early-detection guideline).
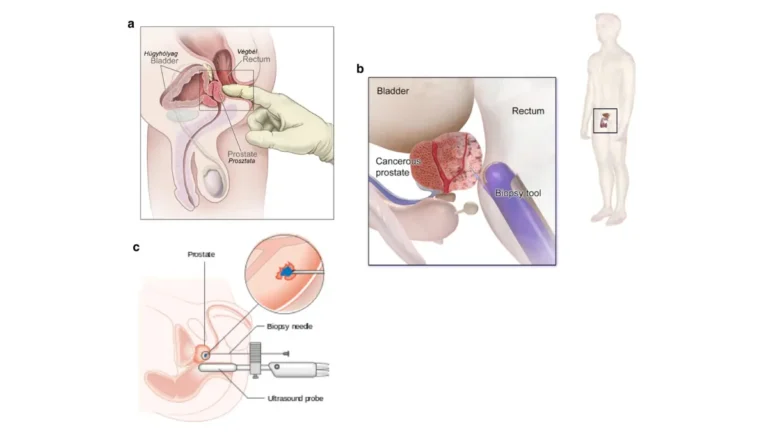
- Refine the risk. Options include a free PSA percentage, PSA density (PSA adjusted for prostate size on ultrasound), blood or urine biomarker tests, and a multiparametric MRI of the prostate.
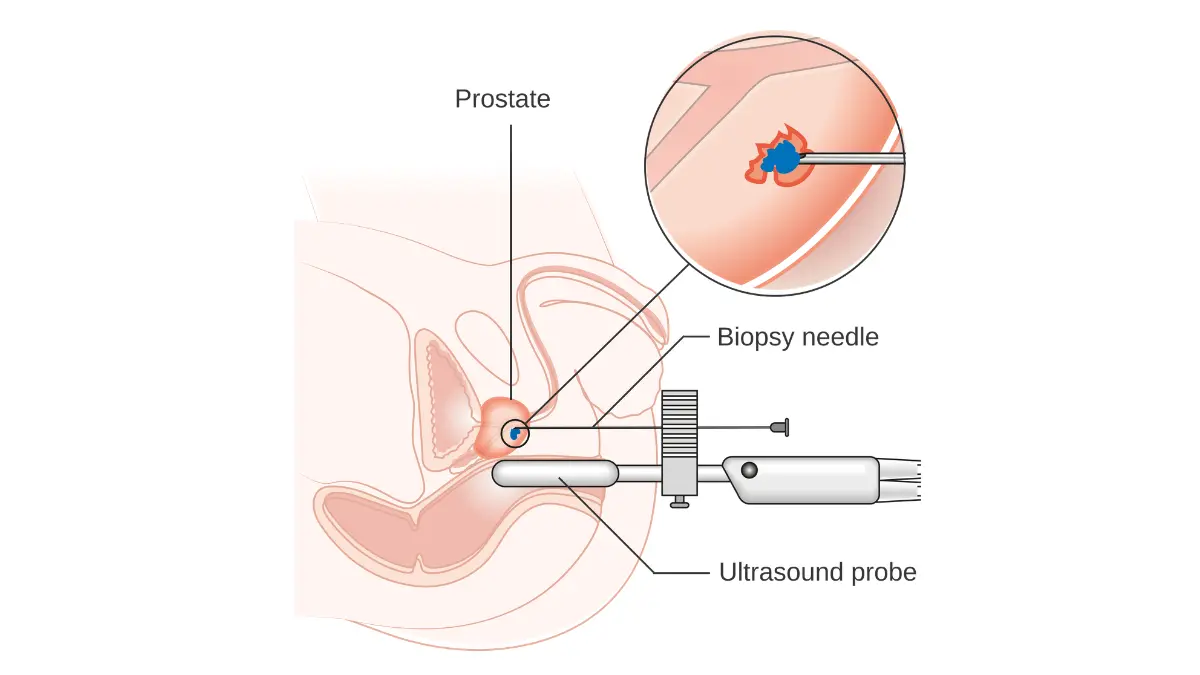
- Biopsy only if indicated. A biopsy is considered when the combined picture points to meaningful risk, and modern practice often uses MRI to decide whether and where to biopsy.
🔬 How It Works: A multiparametric MRI photographs the prostate in detail. If it shows a suspicious area, a biopsy can be targeted to that spot; if it is reassuring, you and your clinician may reasonably decide to monitor instead of biopsy.
Refining the risk
A digital rectal exam is now optional for initial screening but still helps with risk and staging, per the AUA/SUO guideline. PSA velocity — how fast the number climbs — is informative, but guidelines say it should not be used by itself to trigger a biopsy.
Biopsy, only if indicated
The goal of all this is to catch clinically significant prostate cancer while sparing men unnecessary biopsies for harmless elevations. If a biopsy does find cancer, the Gleason score and the cancer’s stage describe how it is likely to behave.
When to see a urologist
A persistently elevated or rising PSA is the usual reason to be referred to a urologist, who can coordinate imaging and any biopsy decision.
✅ Patient Action: Before agreeing to a biopsy, ask a urologist: “Should I have a repeat PSA and a prostate MRI first to decide whether a biopsy is truly needed?”
Should you get a PSA test? Screening guidance by age and risk
Whether to get a PSA test is a shared decision, not a blanket yes or no.
What the guidelines say by age
The U.S. Preventive Services Task Force advises that men aged 55 to 69 make an individual decision after weighing the benefits and harms with a clinician, and it recommends against routine PSA screening for men 70 and older. Urology guidelines similarly emphasize shared decision-making rather than reflex testing, with PSA as the first screening test (AUA/SUO).
Higher-risk men
Men at higher risk, including those with a family history of prostate cancer and Black men, who face higher incidence, may reasonably discuss starting the conversation earlier (American Cancer Society). A genetic risk assessment can help you frame that discussion before an appointment.
Does insurance cover the PSA test?
📊 Clinical Data Point: Medicare Part B covers a PSA blood test once every 12 months for eligible men over 50, and you pay nothing for the test itself. — Source: Medicare’s prostate cancer screening coverage.
Many private insurers cover screening as well, per the National Cancer Institute.
✅ Patient Action: Ask your primary care clinician: “Given my age, family history, and overall health, do the benefits of PSA screening outweigh the harms for me?”
When a high PSA needs urgent care, and when to simply follow up
An elevated PSA on its own is not an emergency. It is a reason for follow-up, not panic.
Most high PSAs are not an emergency
Most elevated readings trace back to a benign cause or simply need a repeat test and a clinic visit. The calm sequence described above is the norm, not the exception, and rushing rarely changes the outcome.
Symptoms that warrant prompt medical attention
⚠️ Clinical Warning: A high PSA number itself is not urgent, but some symptoms need prompt medical care regardless of any test result: being unable to urinate at all, fever with burning or urinary pain (a possible infection), or visible blood in the urine. These are not signs of cancer specifically, but they warrant timely evaluation — seek care rather than waiting for your next scheduled appointment.
PSA test: frequently asked questions
1. Is a PSA of 4 normal?
A PSA test result of 4.0 ng/mL sits at the common threshold where many clinicians consider the level elevated and may suggest further testing. Whether it is concerning depends on your age, prior readings, free PSA, and exam, so a 4 means “look closer,” not “cancer.” Discuss your specific number with your clinician.
2. What is a dangerously high PSA level?
There is no single “dangerous” number, but a PSA test above 10 ng/mL carries a higher likelihood of prostate cancer, and a biopsy is generally discussed at that point. Even then, a high reading must be confirmed and interpreted in context. Talk through any result above 10 with a urologist.
3. Does a high PSA always mean cancer?
No. A high PSA test result most often reflects a benign cause such as an enlarged or inflamed prostate. In the borderline 4–10 ng/mL range, only about 1 in 4 men are found to have cancer, so roughly 75% are not. Your clinician will help confirm what is behind your number.
4. What can cause a falsely high PSA?
Several things can temporarily raise a PSA test reading: a urinary tract infection or prostatitis, a recent prostate biopsy or catheter, vigorous cycling, and recent ejaculation. A recent biopsy can keep PSA elevated for a month or two. If any of these apply, your clinician may simply repeat the test.
5. What is a normal PSA for a 70-year-old?
There is no single normal PSA by age, but levels typically rise as men get older, so an older man’s baseline is generally higher. Some clinicians apply a higher cutoff for men in their 70s. What matters most is your trend over time, reviewed with your clinician rather than judged on one reading.
6. What is the difference between free and total PSA?
Total PSA measures all the prostate-specific antigen in your blood, while free PSA is the portion circulating unbound. When the total PSA test sits in the 4–10 range, a lower free PSA percentage leans toward higher risk and a higher percentage toward a benign cause. Your clinician interprets both together.
7. Do I need a biopsy if my PSA is high?
Not necessarily. A single high PSA test usually leads to a repeat test first, and often a free PSA, biomarker test, or prostate MRI before any biopsy. A biopsy is considered only when the combined picture points to meaningful risk. Ask a urologist whether imaging should come first.
8. At what age should I start PSA testing?
Guidelines suggest men aged 55 to 69 make an individual decision about PSA testing after discussing benefits and harms with a clinician. Men at higher risk may start the conversation earlier. There is no universal start age, so treat it as a shared decision with your clinician.
9. How often should I get a PSA test?
There is no fixed interval that fits everyone; frequency is individualized based on your PSA level, age, risk, and prior results. After a normal result, some men are re-checked every couple of years. Your clinician sets the right cadence with you rather than following a single rule.
10. Can exercise or sex raise my PSA?
Yes, temporarily. Vigorous cycling and recent ejaculation can transiently raise a PSA test result. That is why clinicians sometimes ask you to avoid these beforehand or simply repeat a borderline reading under steady conditions. A short-lived bump from activity is not the same as a persistently elevated level.
11. Should men over 70 get a PSA test?
The U.S. Preventive Services Task Force recommends against routine PSA screening for men 70 and older, citing greater harms than benefits at that age. Some men in excellent health may still discuss it individually. The decision should be made with your clinician based on your health and preferences.
The bottom line on your PSA result
A PSA test is not a cancer test. It is a prompt to look closer. “Normal” depends on your age, and a single elevated reading usually means repeat-and-refine, not an immediate biopsy.
If your number came back higher than expected, the most useful next step is simple: book a follow-up, bring your results and any prior PSA values, and ask whether a repeat test or MRI should come before anything invasive. For the bigger picture, our guide to how prostate cancer is staged and treated walks through what comes after a diagnosis, if one is ever made.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.