On This Page – Quick Medical Summary
Being told you have cancer and then hearing your doctor suggest not treating it right away is one of the most disorienting moments a man can face. Yet for many men with low-risk prostate cancer, careful monitoring — not immediate surgery or radiation — is what major guidelines now recommend first.
This guide is for you whether you were just diagnosed and active surveillance was raised as an option, you are weighing surveillance against surgery or radiation, you are a partner trying to understand a loved one’s choices, or you are already being monitored. Below: who qualifies, what monitoring involves, what the long-term data show, and when surveillance ends. For the full picture of how prostate cancer is staged and treated, start with our main guide.
ℹ️ Medical Disclaimer: This article is educational. It does not diagnose prostate cancer, determine your personal eligibility for active surveillance, or replace individualized advice about treatment, monitoring, medication, or insurance. Whether surveillance is right for you depends on details only your own clinician can assess. Discuss your situation with a board-certified urologist or urologic oncologist before acting on anything here.
What active surveillance actually means
Active surveillance is a structured plan to monitor a slow-growing prostate cancer closely, with intent to treat it for cure if it becomes more aggressive. It is an active strategy of scheduled tests — not a decision to ignore the cancer.
It uses regular PSA blood tests, exams, imaging, and repeat biopsies to watch whether the cancer changes — sparing men the side effects of treatment they may never need while keeping cure firmly available.
How it differs from watchful waiting
These terms are often confused; the National Cancer Institute notes they are used interchangeably even though their goals differ. Watchful waiting is a lighter, symptom-directed approach for men with limited life expectancy, aiming for comfort rather than cure. Active surveillance is curative-intent — built to catch progression early enough to still treat successfully.
Does active surveillance mean no treatment?
No — it means no treatment yet. If your cancer shows defined signs of progressing, your team moves to treatment while cure is still very achievable.
🔬 How It Works: Most prostate cancers grow slowly. By tracking your PSA trend, repeating imaging, and re-sampling the tumor over time, your team can catch the small share that turn aggressive — and act before the window for cure closes.
The National Cancer Institute’s patient overview of prostate cancer treatment shows where surveillance sits among all the options.
Who qualifies for active surveillance?
Eligibility comes down to how low-risk your cancer looks on a few measures your urologist already has. Major guidelines, including the NCCN, treat surveillance as the preferred first option for most men with low-risk, localized disease.
🩺 Physician Note: Current NCCN guidance treats active surveillance as the preferred strategy for the large majority of men with low-risk disease. For very-low-risk cancer with a life expectancy of 10 years or more, it is the recommended approach.
The low-risk and very-low-risk criteria
You are most likely to be a strong candidate if your cancer meets the standard low-risk measures:
- Grade Group 1 — a Gleason score of 6, the classic surveillance-eligible grade
- A PSA under 10 ng/mL
- Clinical stage T1–T2a (the tumor is confined)
- For very-low-risk: stage T1c, fewer than 3 positive biopsy cores with no more than 50% cancer in each, and a PSA density below 0.15 ng/mL/g
Your Gleason score matters most here, because grade best predicts how the cancer will behave.
Can Gleason 7 (3+4) qualify?
Sometimes. Surveillance may be offered to select men with favorable intermediate-risk cancer — Grade Group 2 (Gleason 3+4) with a low percentage of pattern 4, low tumor volume, and low PSA density. The AUA/ASTRO guideline supports this as a conditional option but is clear it carries a higher chance of spread, so it calls for careful shared decision-making.
When a second opinion or genomic test helps
Near the border between risk groups, a genomic test on your biopsy tissue (Decipher, Oncotype DX, or Prolaris) can refine risk for low or favorable intermediate-risk disease. A second pathology opinion can also confirm your Grade Group.
📊 Clinical Data Point: Use of active surveillance among US men with low-risk prostate cancer rose from 26.5% in 2014 to 59.6% in 2021 — Source: AUA Quality (AQUA) Registry, JAMA Network Open, 2023.
✅ Patient Action: Before treatment planning, ask: “Based on my Grade Group, PSA, PSA density, stage, and percent of positive cores, am I low- or favorable-intermediate-risk — and would a genomic test change your recommendation?” If it runs in your family, you can also weigh your inherited risk factors.
Compare your numbers against the standard prostate cancer risk groups from the American Cancer Society.
What the monitoring schedule looks like
Surveillance follows a defined rhythm rather than open-ended worry. Schedules are individualized, but most share a broadly similar pattern set at the start:
- A PSA blood test roughly every 6 months
- A digital rectal exam about once a year
- A multiparametric MRI of the prostate, reported on the PI-RADS scale
- Repeat surveillance biopsies at defined intervals
PSA, exams, and MRI
PSA is tracked for its trend over time rather than a single reading, and MRI helps target areas of concern. Knowing what PSA levels mean by age helps you read your own results.
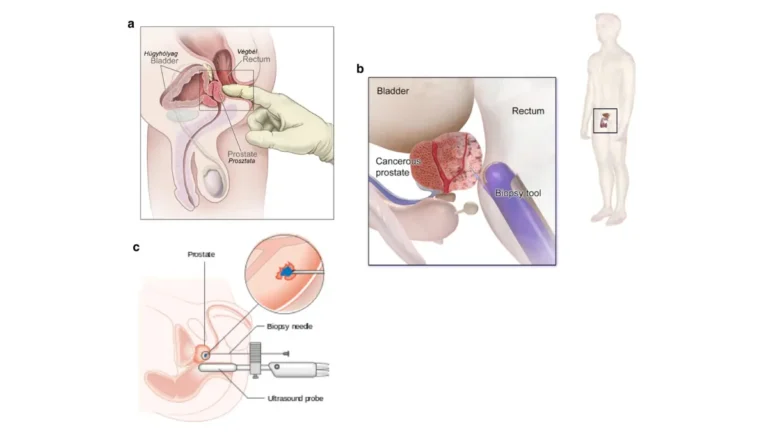
Confirmatory and repeat biopsies
A confirmatory biopsy early in surveillance is standard, because it verifies no higher-grade cancer was missed at diagnosis. Under AUA guidance, men with a suspicious MRI (PI-RADS 4–5) have a prompt repeat targeted biopsy; those with lower-suspicion imaging typically repeat within 12–18 months, then have surveillance biopsies every 1–4 years based on age, health, and preference.
What a typical year looks like
In a steady year you might have two PSA checks, an exam, and imaging or a biopsy if your protocol calls for it. Understanding your prostate biopsy report makes these visits less stressful.
✅ Patient Action: Ask your urologist to write down your exact schedule: “When are my next PSA, MRI, and biopsy, and what change would prompt treatment?”
How safe is active surveillance? What the evidence shows
For most men with low-risk disease, the long-term safety data are reassuring. The strongest evidence is the ProtecT trial, which followed 1,643 UK men with localized prostate cancer for a median of 15 years. After 15 years, prostate-cancer survival was about 97% whether men chose monitoring, surgery, or radiation, with no significant difference in prostate cancer deaths.
15-year survival data
📊 Clinical Data Point: In ProtecT, deaths from prostate cancer at 15 years were 3.1% with active monitoring, 2.2% with surgery, and 2.9% with radiotherapy (P=0.53) — Source: Hamdy et al., New England Journal of Medicine, 2023.
This trial enrolled men from 1999 to 2009, before today’s MRI-guided surveillance, so modern monitoring is likely at least as safe.
The metastasis trade-off
The honest trade-off is here: in ProtecT, cancer spread (metastasis) in 9.4% of the monitoring group versus about 5% with surgery or radiation. Yet over 15 years this did not translate into more prostate cancer deaths.
How many men stay on surveillance
Surveillance is often a chapter, not a permanent path. By 15 years, about 61% of monitored men had moved to surgery or radiation — most while their cancer was still curable. You can read the 15-year ProtecT trial results in the published summary.
When active surveillance ends and treatment begins
Surveillance has clear triggers signaling it is time to treat, so it works as a monitored pathway with a safety net rather than a gamble. Moving to treatment is an expected branch for many men, not a failure. The main signals:
- A rise in Grade Group on a repeat biopsy — the strongest trigger
- A rising PSA pattern over time
- Progression seen on MRI
- Your own decision to stop monitoring
Signs that prompt treatment
Biopsy reclassification to a higher grade carries the most weight, because grade best predicts behavior.
⚠️ Clinical Warning: A stable MRI does not rule out progression. In one study, 31% of men with stable MRI findings were found to have Grade Group 2 or higher cancer on biopsy — which is why repeat biopsies stay part of surveillance and should not be skipped.
What treatment options remain
If you transition, the standard curative options — surgery and radiation — remain fully available, and outcomes for men who move while still on protocol are generally excellent. You can review prostate surgery, cure rates, and recovery to understand one path.
✅ Patient Action: Ask: “Exactly which finding would move me to treatment, and which treatments would I still be a candidate for?”
The honest downsides of active surveillance
Surveillance asks something real of you, and a fair picture includes its costs — emotional and practical.
The anxiety of living with untreated cancer
Knowing a cancer remains in your body can weigh heavily, and surveillance-related anxiety is a well-recognized part of the experience. Naming it and telling your care team is part of managing it well, and some men benefit from counseling or a support group.
Repeat-biopsy considerations
Surveillance means ongoing biopsies, which carry discomfort and a small risk of infection or bleeding, plus the small, real chance a cancer progresses between checks. These are weighed against the treatment side effects — including urinary and sexual problems — that surveillance helps many men avoid. For an overview to share with family, MedlinePlus offers a general guide to prostate cancer.
Frequently asked questions
1. Who qualifies for active surveillance for prostate cancer?
Active surveillance is generally offered to men with low-risk or very-low-risk prostate cancer: Grade Group 1 (Gleason 6), PSA under 10 ng/mL, and stage T1–T2a. Select men with favorable intermediate-risk disease may also qualify. Your urologist confirms eligibility using your full pathology and PSA details.
2. What is the difference between active surveillance and watchful waiting?
Active surveillance is curative-intent monitoring for men who could be treated, using regular PSA tests, exams, MRI, and biopsies to catch progression early. Watchful waiting is a lighter, symptom-focused approach for men with limited life expectancy, aiming for comfort rather than cure. They are different strategies.
3. Can a Gleason 7 (3+4) cancer be on active surveillance?
Sometimes. Surveillance may be offered to select men with favorable intermediate-risk cancer — Grade Group 2 (Gleason 3+4) with low-volume disease and a low percentage of pattern 4. This carries a higher risk of spread than low-risk surveillance, so discuss the trade-offs carefully with your urologist.
4. How often do you get tested on active surveillance?
Most plans include a PSA test about every 6 months, a yearly exam, periodic prostate MRI, and repeat biopsies at set intervals. A confirmatory biopsy early on is standard, with later surveillance biopsies typically every 1–4 years. Your exact schedule is set by your care team.
5. Is it dangerous to delay prostate cancer treatment?
For low-risk disease, long-term data are reassuring: in the 15-year ProtecT trial, prostate-cancer survival was about 97% whether men monitored or treated immediately. Surveillance keeps cure available by catching progression early. Discuss how these findings apply to your specific risk group with your urologist.
6. What percentage of men on active surveillance eventually need treatment?
In the ProtecT trial, about 61% of men on monitoring moved to surgery or radiation by 15 years. Most who transition do so while their cancer is still curable, which is the purpose of close monitoring. The usual trigger is a higher grade on repeat biopsy.
7. When does active surveillance end?
Surveillance typically ends when a repeat biopsy shows a higher Grade Group, when PSA rises in a concerning pattern, when MRI shows progression, or when you choose treatment. A higher grade on biopsy is the strongest trigger. Your urologist will define your specific thresholds in advance.
8. Does active surveillance mean no treatment at all?
No — it means no treatment yet. You stay on a monitoring schedule, and if your cancer shows defined signs of progressing, your team moves to curative treatment. The aim is to avoid side effects from treatment you may never need while keeping cure on the table.
9. What are the risks of active surveillance?
The main risks are a higher chance of spread than with immediate treatment (9.4% versus about 5% in ProtecT), the burden of repeat biopsies, and surveillance-related anxiety. These are weighed against avoiding treatment side effects. Your urologist can help you balance these for your situation.
10. How long can you stay on active surveillance?
There is no fixed time limit. Men can stay on surveillance for years as long as monitoring shows the cancer is stable; in ProtecT, prostate-cancer survival remained about 97% at 15 years. How long depends on your ongoing PSA, MRI, and biopsy results.
11. Should I get a second opinion or genomic test before choosing?
It can help, especially near the border between risk groups. A second pathology opinion can confirm your Grade Group, and a genomic test such as Decipher, Oncotype DX, or Prolaris can refine risk for low or favorable intermediate-risk disease. Ask your urologist whether either would change your recommendation.
Is active surveillance right for you?
For the right candidate, active surveillance is not a gamble or second-best — it is the option major guidelines recommend first for low-risk prostate cancer, sparing men the harms of treatment they may never need while keeping cure available. The decision rests on your Grade Group, PSA, stage, and preferences, weighed with your care team.
✅ Patient Action: Bring this to your urologist or a urologic oncologist: “Given my risk group, what would my surveillance schedule be, what would trigger treatment, and how do my long-term odds compare with treating now?”
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.