FDA Approves 2 Oral Gonorrhea Drugs: What You Need to Know
The FDA approved two groundbreaking oral gonorrhea drugs in December 2025—Nuzolvence (zoliflodacin) and Blujepa (gepotidacin)—offering the first convenient, pill-based alternatives to painful injections for treating this increasingly drug-resistant sexually transmitted infection.
Sarah Martinez, a 28-year-old from Austin, Texas, remembers the embarrassment and discomfort of her gonorrhea diagnosis two years ago. “Getting the injection was painful, and I had to take time off work to visit the clinic,” she recalls. For millions facing similar situations, these newly FDA approved gonorrhea drugs represent a transformative shift in gonorrhea treatment accessibility and patient comfort.
The U.S. Food and Drug Administration approved both oral gonorrhea antibiotics on December 10 and 11, 2025, marking a historic moment in the fight against drug resistant gonorrhea. Nuzolvence, approved December 11, comes as granules that dissolve in water for a single 3-gram dose, while Blujepa gained approval December 10 as the first new antibiotic class for bacterial infections in decades. Both medications target uncomplicated urogenital gonorrhea in adults and children 12 years and older, offering critical ceftriaxone alternatives as antibiotic resistance continues threatening global health.
Clinical trials demonstrated impressive results: 91% of patients treated with zoliflodacin achieved bacterial cure within four to eight days, compared to 96% with standard injectable ceftriaxone treatment. These new gonorrhea antibiotics work through novel mechanisms that bypass existing resistance patterns, providing renewed hope as CDC surveillance data shows rising treatment failures with current options.
If you’re experiencing unusual symptoms, our symptom checker can help identify potential concerns before consulting a healthcare provider.
What This Means For You
Oral convenience: No more painful injections or mandatory clinic visits for gonorrhea medication—patients can now take single-dose pills at home with proper prescription and medical guidance.
Resistance solution: These FDA approved gonorrhea drugs utilize completely different molecular targets than previous antibiotics, making them effective against strains that resist older gonorrhea treatment options.
Expanded access: Both Nuzolvence and Blujepa received priority review, Fast Track designation, and Qualified Infectious Disease Product (QIDP) status, accelerating availability for patients who need urgent STI treatment.
Quick Facts: The New Oral Gonorrhea Drugs
Research from the National Institutes of Health confirms that antibiotic resistant gonorrhea poses one of the most urgent public health threats, with Neisseria gonorrhoeae developing resistance to nearly every antibiotic class introduced over the past 80 years. The approval of these oral alternatives arrives at a critical moment when treatment options have dwindled to essentially one injectable medication.
For comprehensive guidance on maintaining sexual health and preventing infections, explore our health tips resource center.
Deep Dive – The Two New Gonorrhea Drugs
Understanding the New Oral Gonorrhea Antibiotics
The December 2025 approval of zoliflodacin and gepotidacin represents a paradigm shift in how healthcare providers can deliver gonorrhea treatment, offering patients unprecedented convenience and addressing the urgent threat of antibiotic resistant gonorrhea spreading globally.
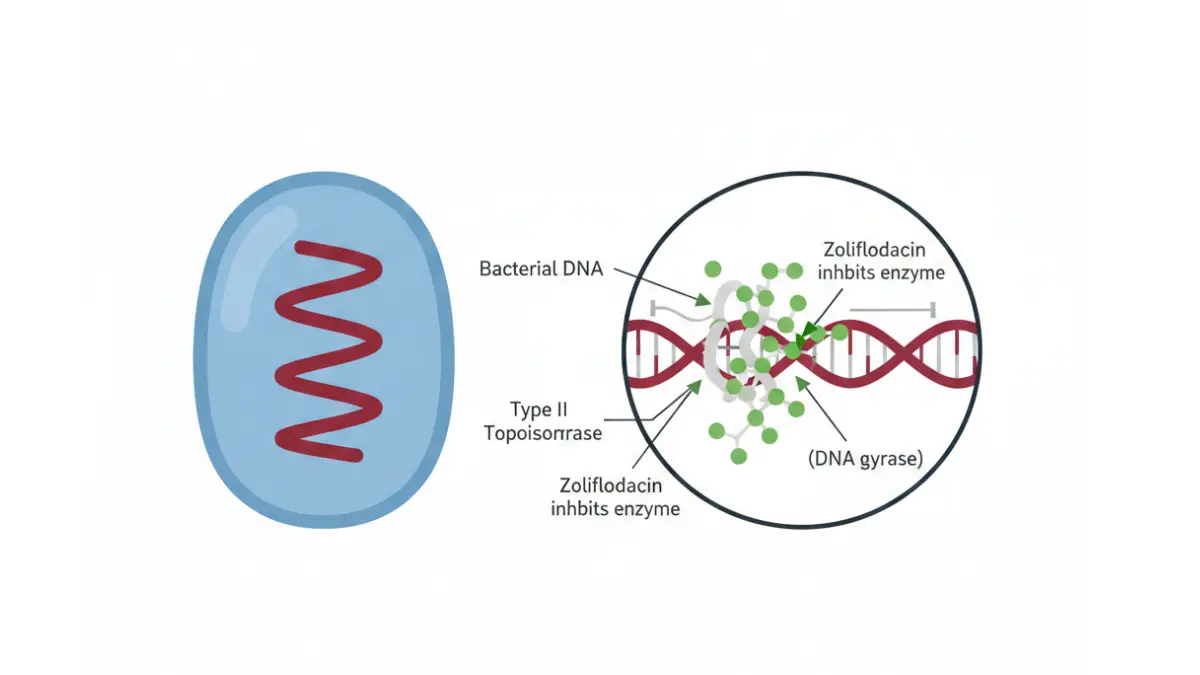
Zoliflodacin (Nuzolvence) – How It Works
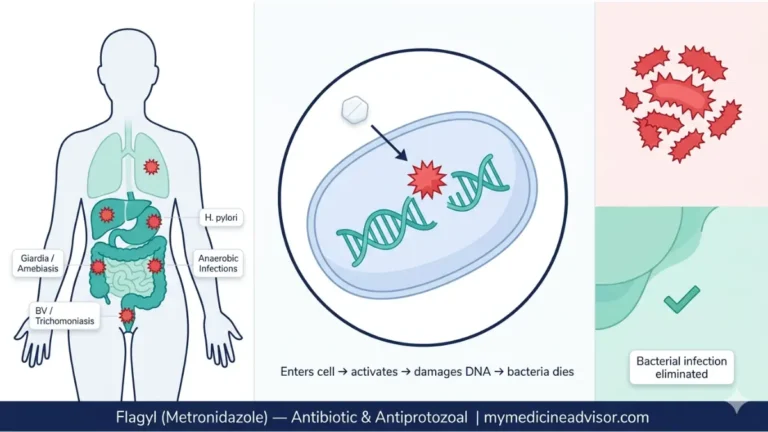
Zoliflodacin belongs to an entirely new antibiotic class called spiropyrimidinetriones (SPTs), targeting bacterial DNA gyrase—a type II topoisomerase enzyme essential for Neisseria gonorrhoeae survival. Unlike fluoroquinolones that have become largely ineffective against drug resistant gonorrhea, this oral gonorrhea antibiotic creates more stable enzyme-DNA complexes and generates significantly higher levels of DNA cleavage in bacterial cells, making resistance development far more difficult.
Research published by the National Center for Biotechnology Information demonstrates that zoliflodacin displays remarkable potency against gyrase compared to topoisomerase IV, a balanced targeting approach that prevents the rapid resistance evolution seen with older gonorrhea drugs. Clinical trials involving 930 patients showed that 91% achieved bacterial cure within four to eight days after a single 3-gram dose, compared to 96% with standard injectable ceftriaxone treatment—a statistically comparable outcome that proves this ceftriaxone alternative can match current standards.
The FDA granted Nuzolvence multiple designations including Fast Track, Qualified Infectious Disease Product (QIDP), and Priority Review status, recognizing the critical need for new gonorrhea antibiotics in combating this increasingly untreatable infection. Patients aged 12 years and older weighing at least 77 pounds can receive the medication as granules dissolved in water, eliminating the need for painful injections or clinic-based administration.
Common side effects include low white blood cell counts, headache, dizziness, nausea, and diarrhea—generally mild and self-limiting compared to complications from untreated gonorrhea. If you’re taking multiple medications, check potential drug interactions before starting any new gonorrhea medication.
Gepotidacin (Blujepa) – First New Class in Decades
Gepotidacin represents the first novel antibiotic mechanism approved for bacterial sexually transmitted infections in over 30 years, belonging to the triazaacenaphthylene class that inhibits both DNA gyrase and topoisomerase IV through a unique binding mechanism. Manufactured by GSK, this groundbreaking oral gonorrhea antibiotic received FDA approval December 10, 2025, following successful completion of the global EAGLE-1 phase III clinical trial.
The EAGLE-1 trial enrolled approximately 628 patients with uncomplicated urogenital gonorrhea, with half receiving two 3,000 mg doses of Blujepa taken 10 to 12 hours apart. Results demonstrated 93% bacterial clearance four to 10 days after treatment versus 91% with standard intramuscular ceftriaxone plus oral azithromycin, meeting the non-inferiority endpoint and establishing gepotidacin as a legitimate single dose gonorrhea treatment alternative.
Studies at the National Institutes of Health reveal that gepotidacin stabilizes DNA-enzyme complexes differently than fluoroquinolones, using mechanisms that circumvent established resistance pathways affecting other gonorrhea drugs. This unique approach makes Blujepa particularly valuable for treating drug resistant gonorrhea cases where traditional antibiotics fail.
Blujepa carries specific warnings for QTc prolongation (heart rhythm changes), acetylcholinesterase inhibition, and potential allergic reactions, requiring careful patient screening before administration. Common side effects include diarrhea, nausea, stomach pain, vomiting, gas, dizziness, and headache—manageable symptoms that pale compared to serious complications like pelvic inflammatory disease from untreated infections.
Patients approved for Blujepa must be at least 12 years old and weigh 99 pounds or more, with dosing administered as oral tablets rather than injections. For those managing chronic conditions alongside STI treatment, tools like our BMI calculator help track overall health metrics during and after gonorrhea treatment.
Comparing Treatment Options
What This Means For You
Access matters: These new gonorrhea antibiotics eliminate barriers to treatment for patients who avoid healthcare due to injection anxiety, transportation challenges, or privacy concerns about visiting STI clinics.
Resistance backup: Having multiple effective oral gonorrhea antibiotics provides critical options when standard treatments fail, ensuring patients can achieve a gonorrhea cure even with resistant bacterial strains.
Future protection: The novel mechanisms of zoliflodacin and gepotidacin give public health authorities powerful new tools to combat the growing crisis of antibiotic resistant gonorrhea threatening global sexual health.
Similar to breakthrough treatments in other infectious diseases like hepatitis B prevention and HIV management, these FDA approved gonorrhea drugs represent hope for patients facing increasingly limited treatment options.
The Drug Resistance Crisis – Why New Options Matter
Why We Urgently Need New Gonorrhea Medication
Neisseria gonorrhoeae has earned its reputation as a “superbug” by systematically developing resistance to every antibiotic class introduced over the past century, making the December 2025 approval of zoliflodacin and gepotidacin a critical turning point in the battle against drug resistant gonorrhea.
The Antibiotic Resistance Timeline
1940s: Penicillin became the first effective gonorrhea cure, providing near-100% success rates for two decades before widespread resistance emerged.
1970s-1980s: As penicillin resistance spread globally, healthcare providers shifted to tetracyclines and spectinomycin, only to see Neisseria gonorrhoeae treatment options narrow again within years.
1990s-2007: Fluoroquinolones like ciprofloxacin offered hope as oral gonorrhea antibiotics, but the CDC discontinued fluoroquinolone recommendations in 2007 after surveillance data revealed alarming resistance rates approaching 100% in some regions.
2010-present: Ceftriaxone injections combined with azithromycin became the last-resort standard for gonorrhea treatment, leaving virtually no backup options when resistance develops.
The World Health Organization designated Neisseria gonorrhoeae as a high-priority pathogen in 2017 due to multidrug resistance affecting penicillin, tetracyclines, macrolides, sulphonamides, quinolones, and now emerging resistance to extended-spectrum cephalosporins. This decades-long pattern demonstrates why new gonorrhea antibiotics with novel mechanisms are essential for maintaining any effective gonorrhea medication arsenal.
Global Resistance Patterns
Recent WHO global antimicrobial resistance surveillance analyzing over 23 million bacterial samples revealed deeply concerning trends in antibiotic resistant gonorrhea worldwide. The China Gonococcal Resistance Surveillance Program documented ceftriaxone resistance jumping from 2.9% in 2017 to 8.1% in 2022, with some Chinese provinces reporting resistance exceeding 10%—a rate that would devastate STI treatment programs if replicated globally.
Canadian surveillance through the Gonococcal Antimicrobial Susceptibility Programme (GASP) tested 3,439 N. gonorrhoeae isolates in 2021, finding rising cefixime resistance of 1.5%—seemingly small percentages that translate to thousands of patients left with no effective oral treatment options. Dr. Magnus Unemo, WHO Collaborating Centre Director for Gonorrhoea and Other STIs, warns that “decreased susceptibility or resistance to ceftriaxone now affects 0-21% of isolates depending on geographic region, while ciprofloxacin resistance ranges from 0-100%”.
The CDC’s Enhanced Gonococcal Isolate Surveillance Project monitors resistance patterns across multiple anatomic sites, recognizing that pharyngeal (throat) and rectal infections often harbor more resistant strains that can spread through sexual networks. This surveillance infrastructure provides early warning signs that help guide treatment recommendations and highlight why FDA approved gonorrhea drugs with completely different mechanisms are urgently needed.
What Makes These Drugs Different
Unlike previous antibiotics where Neisseria gonorrhoeae simply modified existing resistance mechanisms, zoliflodacin and gepotidacin attack bacterial DNA replication through pathways that current resistant strains cannot easily bypass. The novel spiropyrimidinetrione and triazaacenaphthylene classes create enzyme-DNA complexes that differ structurally from fluoroquinolone binding sites, meaning decades of accumulated fluoroquinolone resistance mutations provide no protection against these new gonorrhea drugs.
Clinical evidence shows no cross-resistance between zoliflodacin, gepotidacin, and existing cephalosporin-resistant or fluoroquinolone-resistant N. gonorrhoeae strains, giving healthcare providers truly independent treatment options for the first time in decades. Similar to how advances in vaccine development have transformed disease prevention, these new antibiotic classes represent a paradigm shift in fighting antibiotic resistant gonorrhea before it becomes completely untreatable.
Without new antibiotics, gonorrhea could become effectively untreatable within a generation, leaving millions at risk for serious complications including infertility and systemic infection.
Comprehensive Gonorrhea Guide – Symptoms, Testing & Diagnosis
Complete Guide to Gonorrhea Symptoms and Testing
What Is Gonorrhea?
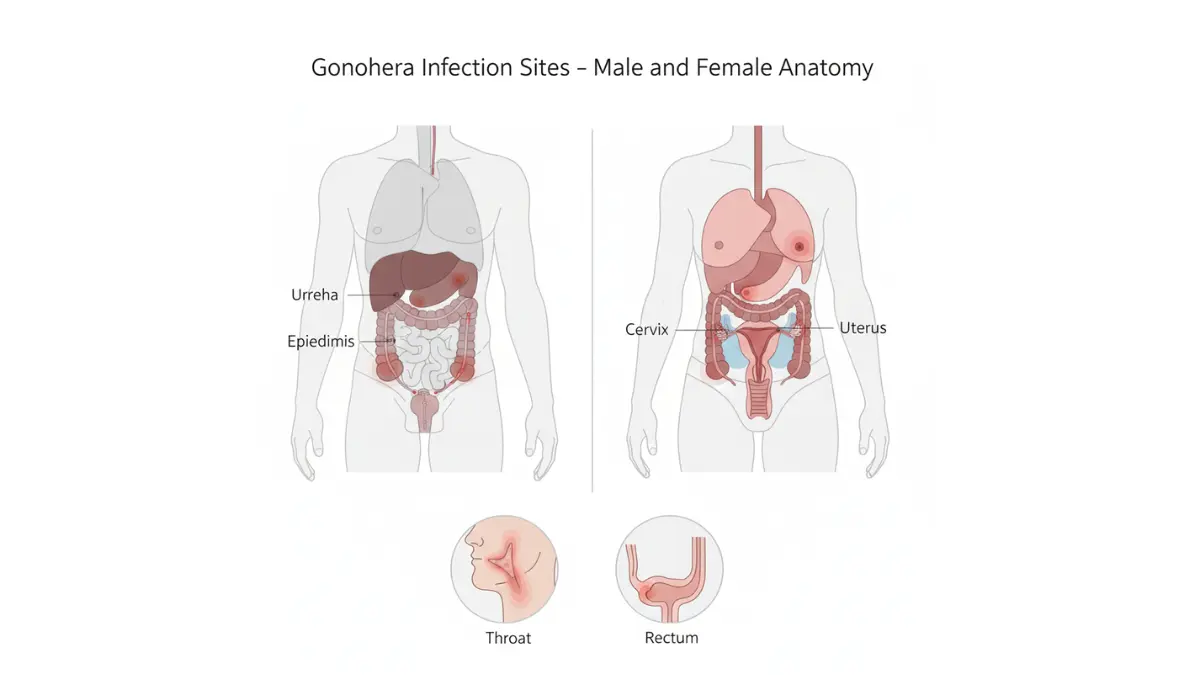
Gonorrhea is a sexually transmitted bacterial infection caused by Neisseria gonorrhoeae, ranking as the second most commonly reported bacterial STI in the United States with over 700,000 diagnosed cases annually. This infection affects the mucous membranes of the reproductive tract, urethra, rectum, throat, and eyes in both men and women, with peak infection rates occurring among sexually active individuals aged 15-24 years.
The bacteria spreads through vaginal, anal, or oral sex with an infected partner, and pregnant individuals can transmit gonorrhea to newborns during childbirth, potentially causing serious eye infections or bloodstream infections in infants. Research published in the National Library of Medicine reveals that roughly half of all gonococcal infections in women remain asymptomatic, creating a dangerous “iceberg effect” where actual prevalence far exceeds reported cases and allowing untreated infections to silently progress toward serious complications.
Understanding what is gonorrhea and recognizing early symptoms remains critical because untreated infections can lead to pelvic inflammatory disease, infertility, and increased HIV transmission risk.
Gonorrhea Symptoms in Men
Most men with gonorrhea develop noticeable symptoms within 2-14 days after exposure, though some remain asymptomatic carriers who can unknowingly transmit the infection. According to CDC clinical guidance, gonorrhea symptoms in men typically include:
- Burning sensation when urinating – often the first and most common symptom that prompts medical attention
- Penile discharge – white, yellow, or greenish discharge from the urethral opening
- Testicular pain or swelling – less common but indicates potential spread to the epididymis
- Urethral irritation – redness, tenderness, or discomfort at the tip of the penis
Marcus, a 32-year-old teacher from Chicago, initially dismissed his mild burning during urination as dehydration before noticing yellow gonorrhea discharge two days later. “I thought it would go away on its own, but the symptoms got worse quickly,” he shared, highlighting why prompt testing and treatment matters for achieving a gonorrhea cure.
Men experiencing these symptoms should use our symptom checker for preliminary assessment, though professional medical evaluation remains essential for accurate diagnosis and appropriate gonorrhea treatment.
Gonorrhea Symptoms in Women
Gonorrhea symptoms in women present more subtly than in men, with 50-80% of infected women experiencing no symptoms at all during the early stages—a dangerous pattern that allows infections to progress undetected toward serious complications like pelvic inflammatory disease. When symptoms do appear, they often mimic other common conditions, leading to delayed diagnosis and treatment.
Symptomatic gonorrhea in women may cause:
- Unusual vaginal discharge – increased volume, watery consistency, or greenish-yellow coloration that differs from normal discharge patterns
- Painful or burning urination – frequently mistaken for urinary tract infections, delaying proper STI treatment
- Pelvic pain – lower abdominal discomfort or pain during sexual intercourse indicating potential cervical involvement
- Abnormal vaginal bleeding – spotting between menstrual periods or heavier periods than usual
- Cervical inflammation – redness and irritation of the cervix visible during pelvic examination
Women planning pregnancy should particularly prioritize testing, as untreated gonorrhea can cause complications during pregnancy and infertility. Our pregnancy due date calculator and ovulation calculator help track reproductive health, but regular STI screening remains essential for protecting fertility.
Other Infection Sites
Gonorrhea affects multiple body sites beyond the genital tract, with symptoms varying by location:
Rectal gonorrhea (affecting all genders):
- Anal discharge or bleeding
- Rectal pain, soreness, or itching
- Painful bowel movements
- Most cases remain asymptomatic
Oral/throat gonorrhea:
- Usually produces no symptoms
- Occasionally causes sore throat or difficulty swallowing
- Easily missed without specific pharyngeal testing
Gonococcal conjunctivitis (eye infection):
- Severe eye redness and swelling
- Thick pus discharge from eyes
- Requires immediate medical treatment to prevent vision loss
- Most common in newborns exposed during delivery
Disseminated gonococcal infection (bloodstream):
- Fever and chills
- Skin lesions or rash
- Joint pain and swelling (septic arthritis)
- Affects 0.5-3% of untreated cases
How Gonorrhea Testing Works
Modern nucleic acid amplification tests (NAATs) provide the most accurate gonorrhea testing, with sensitivity exceeding 95% for detecting Neisseria gonorrhoeae DNA in various specimen types. The University of Washington STD/HIV Prevention Training Center reports that FDA-cleared NAATs demonstrate 100% sensitivity in women and 97.3% sensitivity in men using vaginal swabs and urine samples respectively.
Testing methods include:
- Urine test – preferred for men, non-invasive collection requiring first-catch morning sample
- Vaginal swab – most accurate for women, can be self-collected or provider-collected
- Cervical swab – collected during pelvic examination
- Urethral swab – used in men when urine testing unavailable
- Pharyngeal swab – throat testing for those with oral sexual exposure
- Rectal swab – essential for individuals with receptive anal intercourse
Results typically return within 24-72 hours, with rapid point-of-care NAATs providing results in approximately 30 minutes at some clinics. The CDC recommends annual gonorrhea testing for sexually active women under 25, men who have sex with men, and anyone with multiple partners or STI symptoms.
Get tested immediately if you:
- Experience any symptoms described above
- Had sexual contact with someone diagnosed with gonorrhea
- Are sexually active with multiple or new partners
- Are pregnant or planning pregnancy
- Had unprotected sexual contact
Treatment Options & Complications – What Happens If Untreated
How to Treat Gonorrhea: Current and New Options
Current Standard Treatment
Until the December 2025 approval of zoliflodacin and gepotidacin, CDC gonorrhea treatment guidelines recommended a single 500mg intramuscular injection of ceftriaxone as the only first-line option for treating uncomplicated urogenital, anorectal, and pharyngeal gonorrhea. For patients weighing 150 kg (330 pounds) or more, healthcare providers increase the dose to 1 gram to ensure adequate blood concentrations above the bacterial minimum inhibitory concentration for approximately 50 hours.
This ceftriaxone monotherapy approach emerged after mounting azithromycin resistance prompted CDC to abandon dual-drug therapy in 2020, leaving gonorrhea treatment dependent on essentially one antibiotic class—a precarious situation as resistance continues evolving globally. The injectable nature of ceftriaxone requires clinic visits, causes injection-site pain, and creates barriers to treatment access for patients in rural areas, those without transportation, or individuals avoiding healthcare settings due to stigma concerns.
When injectable treatment proves impossible, expedited partner therapy using a single 800mg oral dose of cefixime serves as an alternative, though this option carries higher treatment failure rates and is reserved for specific circumstances where the recommended injection cannot be administered.
New Treatment Options (2025)
The FDA approval of Nuzolvence (zoliflodacin) and Blujepa (gepotidacin) fundamentally transforms how to treat gonorrhea by providing convenient oral alternatives that eliminate injection requirements while maintaining comparable cure rates to standard therapy. These new gonorrhea drugs represent the first major expansion of treatment options in decades, offering patients privacy, convenience, and immediate accessibility through pharmacy dispensing rather than mandatory clinic procedures.
Zoliflodacin achieves 91% bacterial clearance with a single 3-gram oral dose dissolved in water, while gepotidacin requires two 3,000mg doses taken 10-12 hours apart—both protocols far more patient-friendly than intramuscular injections. The distinct mechanisms of action targeting bacterial DNA replication through pathways unaffected by existing cephalosporin or fluoroquinolone resistance mutations give healthcare providers genuine backup options when standard gonorrhea treatment fails.
Patients taking these new oral gonorrhea antibiotics can complete treatment privately at home, eliminating time off work, transportation costs, and the emotional discomfort many experience receiving STI treatment in clinical settings. If you’re currently taking multiple medications, use our pill identifier tool to track your prescriptions and avoid confusion when adding new gonorrhea medication to your regimen.
How to Treat Gonorrhea at Home – Critical Limits
No home remedies, supplements, or over-the-counter products can cure gonorrhea. Despite countless internet claims, Neisseria gonorrhoeae requires prescription antibiotics for bacterial elimination, and attempting alternative treatments only delays proper care while allowing complications to develop and transmission to continue.
Essential treatment rules:
- Prescription antibiotics are mandatory—no exceptions
- Complete the full antibiotic course even if symptoms disappear
- Abstain from all sexual contact during treatment and for 7 days after completing antibiotics
- Notify all sexual partners from the previous 60 days so they can receive testing and treatment
- Return for follow-up testing 3 months after treatment to check for reinfection
Serious Complications of Untreated Gonorrhea
For People with Vaginas
Pelvic inflammatory disease (PID) develops in 10-20% of women with untreated gonorrhea, causing infection that spreads from the cervix through the uterus into the fallopian tubes. Research published in the National Library of Medicine demonstrates that Neisseria gonorrhoeae-associated PID causes more severe illness, higher fever, and increased hospitalization rates compared to PID from other pathogens, with patients seeking medical care more rapidly due to symptom intensity.
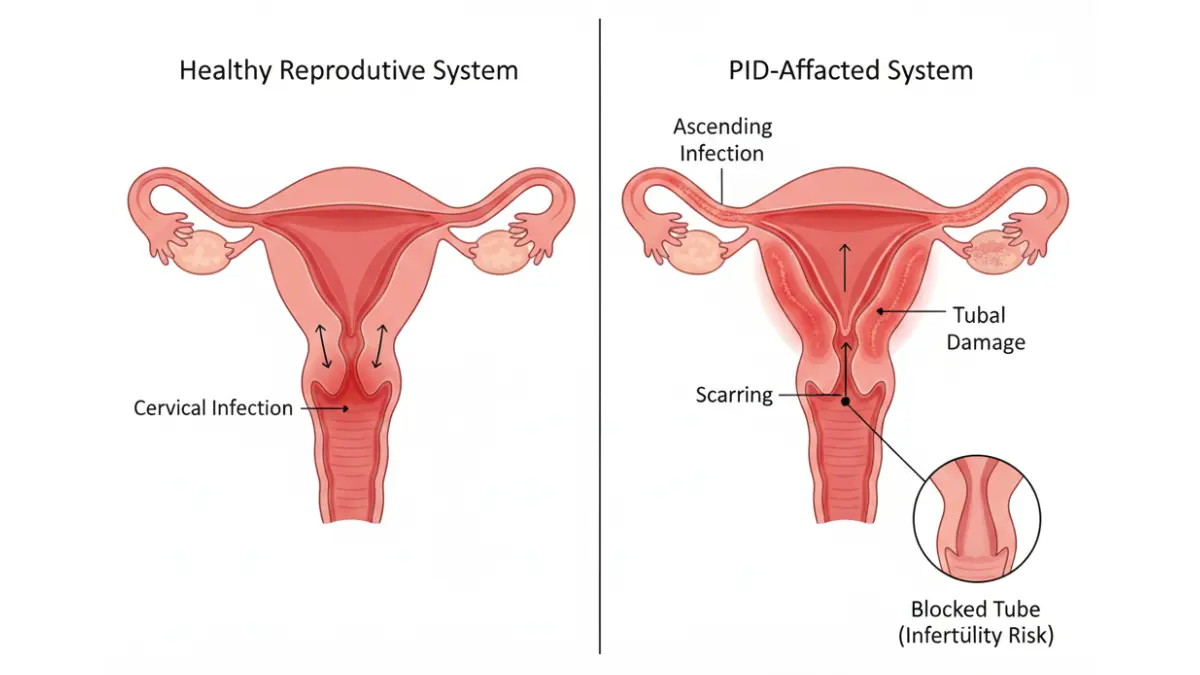
Long-term PID consequences include:
- Tubal factor infertility – Scarring and damage to fallopian tube ciliated cells permanently impairs fertility in 15-20% of women after a single PID episode, with risk increasing to 40% after three or more episodes
- Ectopic pregnancy – Damaged fallopian tubes increase ectopic pregnancy risk sevenfold, a life-threatening condition where fertilized eggs implant outside the uterus
- Chronic pelvic pain – Persistent pain affecting 18% of women who experienced PID, significantly impacting quality of life
- Tubo-ovarian abscess – Severe pockets of infection requiring hospitalization, intravenous antibiotics, or surgical drainage
Most concerning, many women who develop tubal factor infertility have no history of symptomatic PID, meaning silent infections can destroy fertility without the patient ever knowing they had gonorrhea. This reality underscores why routine screening and prompt gonorrhea treatment remain essential reproductive health priorities. Women planning pregnancy should track their reproductive health using tools like our pregnancy weight gain calculator while ensuring regular STI screening.
For People with Penises
Untreated gonorrhea in men commonly progresses to epididymitis—painful inflammation of the coiled tube (epididymis) that stores and carries sperm from the testicle. Cornell University Health reports this condition causes severe testicular pain, fever, and in rare cases permanent sterility through scarring that blocks sperm transport.
Male complications include:
- Epididymitis – Painful swelling, fever, and potential long-term fertility impairment requiring extended antibiotic therapy
- Urethral stricture – Scarring that narrows the urethra, causing painful urination and requiring surgical correction
- Prostatitis – Prostate gland inflammation causing pelvic pain and urinary symptoms
- Testicular abscess – Requires surgical drainage and carries permanent fertility risk
For Everyone
Disseminated gonococcal infection (DGI) affects 0.5-3% of people with untreated gonorrhea when bacteria enter the bloodstream, causing potentially life-threatening systemic illness. Symptoms include fever, chills, skin lesions with pustules on hands and feet, and septic arthritis—painful joint infections most commonly affecting knees, ankles, and wrists requiring hospitalization and intravenous antibiotics.
Additional universal risks include:
- Increased HIV transmission – Gonorrhea inflammation damages mucosal barriers and increases HIV acquisition risk 3-5 fold during sexual contact
- Endocarditis – Rare but serious heart valve infections requiring prolonged intravenous antibiotics
- Meningitis – Extremely rare brain and spinal cord membrane infections
- Neonatal transmission – Pregnant individuals can transmit gonorrhea during delivery, causing severe eye infections (ophthalmia neonatorum) or bloodstream infections in newborns
Untreated gonorrhea can cause permanent infertility, life-threatening systemic infections, and irreversible damage to reproductive organs—complications that are 100% preventable with timely antibiotic treatment.
Prevention, Future Outlook & Actionable Next Steps
Preventing Gonorrhea and What’s Next in Treatment
Evidence-Based Prevention Strategies
CDC prevention guidelines emphasize that latex condoms remain highly effective at preventing gonorrhea transmission during vaginal, anal, and oral sex when used consistently and correctly. Condoms reduce gonorrhea transmission risk by creating a physical barrier that blocks Neisseria gonorrhoeae bacteria from entering mucous membranes, with proper use achieving 98% effectiveness in preventing STI transmission.
Additional gonorrhea prevention strategies include:
- Regular STI screening – The CDC recommends annual gonorrhea testing for all sexually active women under 25, men who have sex with men, and anyone with multiple partners or STI symptoms
- Partner communication – Discussing STI status and testing history before sexual contact reduces transmission risk and enables prompt treatment if exposure occurs
- Mutual monogamy – Sexual relationships between two uninfected partners who have sex exclusively with each other eliminate transmission risk
- Dental dams – Barrier protection during oral-vaginal or oral-anal contact prevents oral gonorrhea transmission
- No vaccine currently available – Unlike other bacterial infections, no licensed gonorrhea vaccine exists, making barrier methods and screening essential for prevention

What’s Coming Next
Research published in the National Institutes of Health details promising vaccine candidates targeting conserved Neisseria gonorrhoeae surface proteins that could provide long-term immunity against multiple bacterial strains. Scientists are investigating novel adjuvant strategies and identifying immune correlates that may finally overcome the bacterium’s remarkable ability to evade immune responses and prevent natural immunity from developing after infection.
Beyond vaccines, pharmaceutical companies continue developing additional oral antibiotics targeting unexploited bacterial mechanisms, ensuring future backup options as resistance inevitably evolves against current gonorrhea drugs. Point-of-care rapid testing technologies in development promise results within 15-30 minutes, enabling immediate single dose gonorrhea treatment during the same clinic visit and preventing transmission from delayed treatment.
Your Action Plan – What to Do Now
- Get tested immediately if you experience symptoms, had unprotected sexual contact, or your partner was diagnosed with gonorrhea
- Use barrier protection consistently during all sexual activity including vaginal, anal, and oral sex
- Schedule annual STI screening if you’re sexually active, especially if under 25 or have multiple partners
- Complete full antibiotic courses if diagnosed, even when symptoms resolve quickly
- Abstain from sexual contact during treatment and for 7 days after completing antibiotics to prevent reinfection
- Notify sexual partners from the previous 60 days so they can receive testing and treatment
- Return for follow-up testing 3 months after treatment to check for reinfection
For comprehensive wellness tracking alongside sexual health management, explore tools like our water intake calculator and sleep calculator to support overall health. Understanding reproductive health connections through our genetic risk assessment tool can also inform discussions with healthcare providers about STI screening frequency.
What This Means For You
The December 2025 FDA approval of Nuzolvence and Blujepa represents genuine hope in the fight against antibiotic resistant gonorrhea. You now have access to convenient oral gonorrhea antibiotics that eliminate injection requirements while providing comparable cure rates to standard therapy, making STI treatment more accessible and reducing barriers to care that previously prevented many from seeking help.
These new gonorrhea drugs aren’t just convenient alternatives—they’re critical tools that expand treatment options when resistance develops and provide backup mechanisms that could save the effectiveness of gonorrhea medication for future generations. By seeking timely testing and treatment, you protect not only your own health but also contribute to reducing gonorrhea transmission and slowing resistance development in your community.
For additional guidance on maintaining overall health and wellness, visit our comprehensive health tips resource center covering topics from infectious disease prevention to chronic condition management.
Disclaimer: This article is for educational purposes only and does not constitute medical advice. Always consult a qualified healthcare provider for diagnosis and treatment of gonorrhea or any sexually transmitted infection. The information provided here should not replace professional medical consultation, examination, or treatment recommendations from licensed healthcare professionals.
Frequently Asked Questions about FDA approved gonorrhea drugs
1. What are the two new FDA approved gonorrhea drugs?
Nuzolvence (zoliflodacin) and Blujepa (gepotidacin) are the two new oral gonorrhea antibiotics approved by the FDA in December 2025, offering pill-based alternatives to painful injections.
2. How effective are the new oral gonorrhea drugs?
Zoliflodacin achieves 91% bacterial cure rates and gepotidacin achieves 93% cure rates, both comparable to the current standard ceftriaxone injection (96%).
3. Can gonorrhea be cured with a single dose?
Yes, zoliflodacin (Nuzolvence) requires just one 3-gram oral dose, while gepotidacin (Blujepa) needs two doses taken 10-12 hours apart for complete gonorrhea cure.
4. What are the first signs of gonorrhea in women?
Most women (50-80%) have no symptoms, but when present, gonorrhea symptoms in women include unusual vaginal discharge, painful urination, pelvic pain, and abnormal bleeding between periods.
5. What are the first signs of gonorrhea in men?
Gonorrhea symptoms in men typically include burning during urination, yellow or greenish penile discharge, and testicular pain or swelling appearing 2-14 days after exposure.
6. How long does it take to cure gonorrhea?
With proper antibiotic treatment, bacterial clearance occurs within 4-10 days, though symptoms often improve within 24-48 hours of starting gonorrhea medication.
7. Can gonorrhea cause infertility?
Yes, untreated gonorrhea causes pelvic inflammatory disease in women (10-20% risk) and epididymitis in men, both leading to permanent infertility in 15-40% of cases.
8. How is gonorrhea testing done?
Gonorrhea testing uses urine samples or swabs from the genitals, throat, or rectum, with nucleic acid amplification tests (NAATs) providing results within 24-72 hours.
9. Can you get gonorrhea from oral sex?
Yes, gonorrhea spreads through oral sex, causing throat infections (pharyngeal gonorrhea) that are usually asymptomatic but can transmit to partners during kissing or oral contact.
10. Why do we need new gonorrhea antibiotics?
Neisseria gonorrhoeae has developed resistance to nearly every antibiotic class over 80 years, making drug resistant gonorrhea a critical public health threat requiring new treatment options.
11. How can I prevent gonorrhea?
Use latex condoms consistently during all sexual activity (vaginal, anal, oral), get annual STI screening if sexually active, communicate openly with partners about testing, and seek immediate treatment if exposed.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.