On This Page – Quick Medical Summary
If you are staring at a blood test result with a value highlighted in red, your stomach dropping, this section is written for you first.
A complete blood count — a CBC — is one of the most common blood tests ordered in the United States. It counts the cells in your blood and flags patterns. It rarely, on its own, tells you exactly what is wrong. That gap between “something is flagged” and “here is the diagnosis” is where most of the fear lives, and it is what this guide is built to close.
Read the path that matches where you are right now:
- You just saw a flagged result on your patient portal. Skip to the section on what a single abnormal value does and doesn’t mean, then find your specific value — red cells, white cells, or platelets — in the sections below. A flag is a starting point for a conversation, not a verdict.
- You are reading results for a parent, partner, or child. The reference-range section explains why “normal” shifts with age and sex, and the section on higher-stakes situations covers why these results always need a clinician’s read.
- You have symptoms, or a CBC is coming up, and you haven’t talked it through with a doctor yet. Start with what the test is and how to prepare, and pair your symptoms with your result using our symptom checker before your appointment.
- You get CBCs regularly to monitor a condition or a medication. The red-cell, white-cell, and platelet sections explain what your doctor watches over time, and the monitoring section covers why trends matter more than any single number.
And if your CBC came back completely normal but you still feel unwell, do not skip the section on what a CBC can’t show. A normal blood count is reassuring, but it does not measure everything.
One honest fact to carry through everything below: reference ranges vary slightly among different laboratories, and they shift with factors like age, sex, and even altitude, so the range printed on your own report is the one that applies to you.
ℹ️ Medical Disclaimer: This article explains what a complete blood count measures, how to interpret abnormal red blood cell, white blood cell, and platelet results, what a CBC can and cannot detect (including its limits around anemia, infection, bleeding risk, and cancer), how results differ in pregnancy, childhood, and during cancer treatment, and which results warrant prompt medical attention. It is for general education only.
Reference ranges and the meaning of any individual result depend on your laboratory, your age and sex, your medical history, your medications, and your clinician’s assessment. Nothing here diagnoses a condition or replaces testing, and no figure should be used to make or change a medical decision on your own. Always consult a licensed healthcare provider — and, for blood-count abnormalities, sometimes a board-certified hematologist — about your specific results.
What a complete blood count actually is
A CBC is a group of measurements taken from a single small sample of your blood, and understanding what it counts makes every result that follows easier to read.
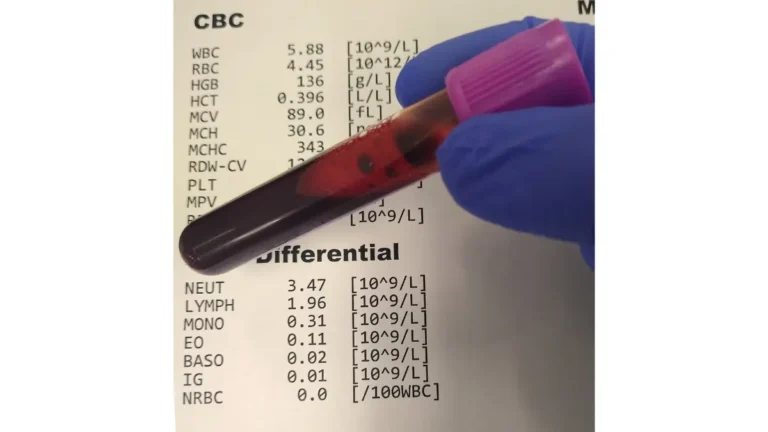
A complete blood count measures the number and size of the different cells circulating in your blood. According to the National Library of Medicine, it looks at your red blood cells, your white blood cells, your platelets, your hemoglobin, and your hematocrit. It is a screening and monitoring test — a wide-angle snapshot of your blood, not a targeted test for one disease.
Your blood is made of three cell types, each with a distinct job. Red blood cells carry oxygen from your lungs to the rest of your body. White blood cells are part of your immune system and help fight infection and other diseases. Platelets are cell fragments that help your blood clot to stop bleeding.
🔬 How It Works: A machine called a hematology analyzer draws your sample through a narrow channel and counts each cell as it passes, measuring size and, for red cells, hemoglobin content. If anything looks unusual, a laboratory professional called a pathologist examines a drop of your blood smeared on a glass slide under a microscope to check the machine’s reading. That is why some results take longer than others — a flagged sample may get a human second look.
Why your doctor ordered this test
Doctors order a CBC for three broad reasons, and knowing which one applies to you changes how you should read the result.
The first is routine screening — a CBC is often part of a general check-up, giving a baseline picture of your health. The second is to investigate symptoms such as fatigue, unexplained weight loss, fever or other signs of infection, weakness, bruising, or bleeding. The third is to monitor an ongoing condition or a treatment — for example, chronic kidney disease, or medicines and radiation that can change your blood counts.
If your CBC was routine and everything is in range, that is genuinely good news and usually needs no further thought. If it was ordered because of a symptom, the result is one piece of a larger puzzle your clinician is assembling.
A CBC versus a CBC with differential
You may see two versions of this test, and the difference is worth understanding because it appears on many reports.
A standard CBC measures the total number of white blood cells. A CBC with differential goes further and measures how many of each type of white blood cell you have — a breakdown that can point toward specific causes, like a bacterial versus a viral pattern. Many modern analyzers produce the differential automatically, so you may get it whether or not it was separately requested.
Neither version diagnoses a disease by itself. Both are designed to reveal patterns that a clinician then interprets alongside your symptoms, history, and — often — additional tests. You can read more in the National Library of Medicine’s overview of the complete blood count.
Everything a CBC measures, line by line
Once you can map every value on your report to what it counts, an intimidating page of numbers becomes far less frightening — so here is the full panel, plain and complete.
A CBC reports several counted values and several calculated values, and the distinction matters. Counted values — red cells, white cells, platelets — are tallied directly. Calculated values, called indices, are derived by the machine from those counts to describe the character of your cells, not just their number.
Red blood cell measures
Three core numbers describe your oxygen-carrying capacity.
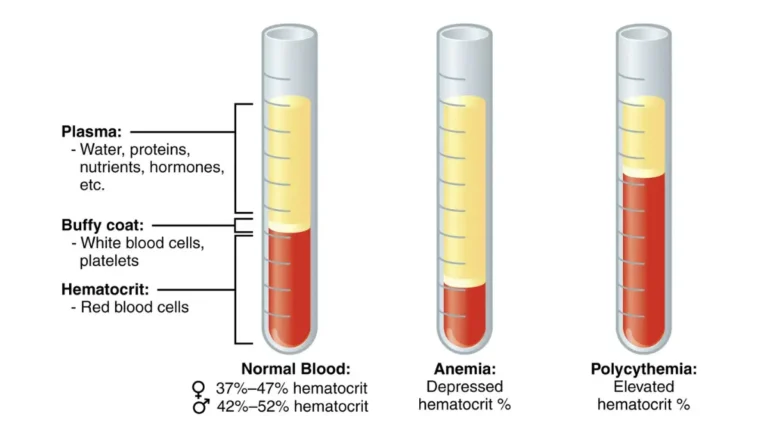
Red blood cell count (RBC) is the number of red cells in a set volume of blood. Hemoglobin is the iron-rich protein inside those cells that actually binds and carries oxygen. Hematocrit is the fraction of your whole blood made up of red cells — essentially how much of your blood, by volume, is red cells versus liquid plasma.
🔬 How It Works: Oxygen you breathe in crosses from your lungs into red blood cells and latches onto hemoglobin, which ferries it to every tissue. The amount of oxygen your body receives depends on both how many red cells and how much functioning hemoglobin you have — which is why low hemoglobin can leave you tired and short of breath even before anything else feels wrong.
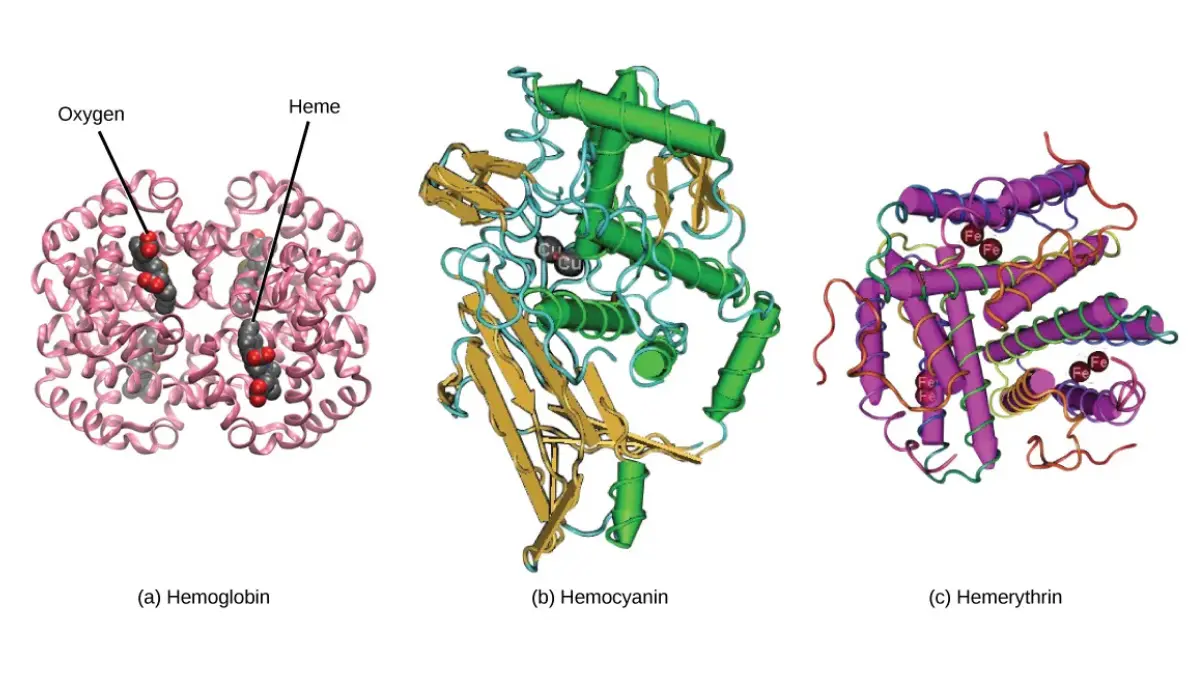
Adapted from OpenStax Figure 31.6a, licensed under [CC BY 4.0]
Red cell indices
Four calculated values describe the size and hemoglobin content of your red cells, and they are the clues that help pinpoint the type of a red-cell problem.
MCV (mean corpuscular volume) is the average size of your red cells — are they smaller than usual, normal, or larger than usual. MCH and MCHC describe the average amount and concentration of hemoglobin per cell. RDW (red cell distribution width) measures how much your red cells vary in size from one another; a high RDW means the cells are unusually uneven, which can be an early clue in certain anemias. Ranges for RDW vary by laboratory and appear on your own report.
White blood cell count and the differential
The white-cell portion measures your immune-cell army — its total size and, on a differential, its composition.
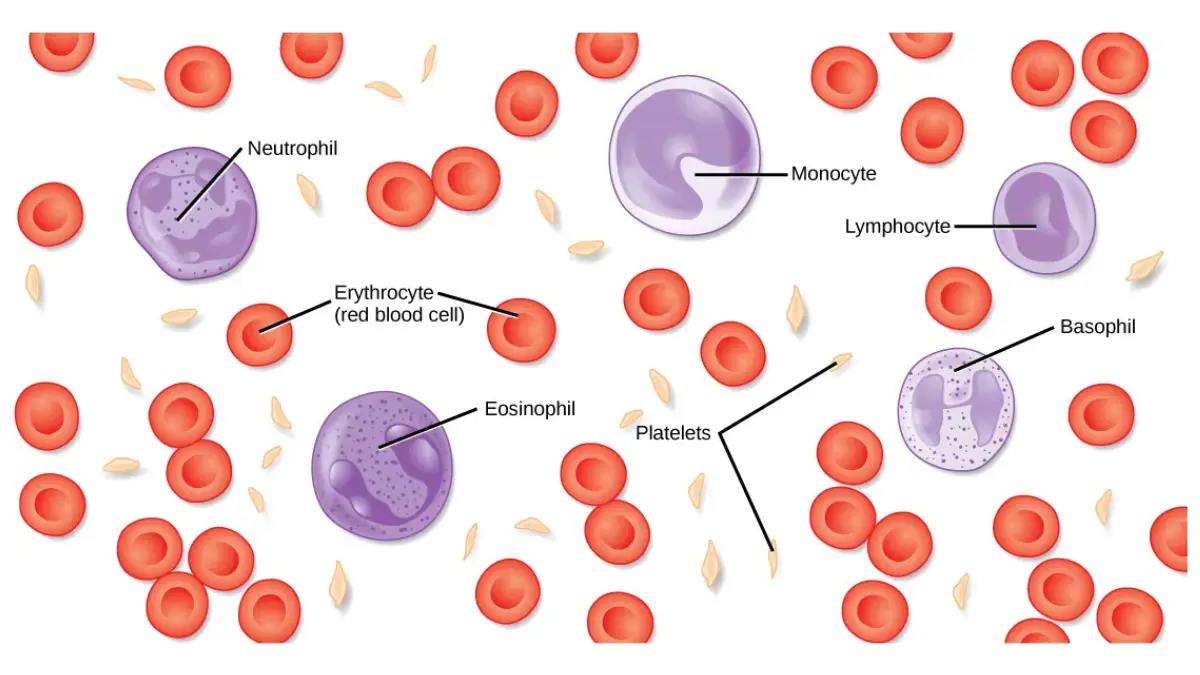
The white blood cell count is the total number of immune cells. The differential breaks that total into the five normal types: neutrophils, lymphocytes, monocytes, eosinophils, and basophils. Each type fights different threats, so a shift in the mix — say, a jump in neutrophils — can hint at what kind of challenge your body is facing.
🔬 How It Works: White blood cells are the mediators of inflammation and the immune response. Neutrophils, the most common type, are your front line against bacteria; lymphocytes (B cells and T cells) largely handle viruses; eosinophils rise with allergies and parasites; monocytes clear debris and germs; basophils act in allergic reactions. A differential reads the balance among them, which is often more informative than the total alone.
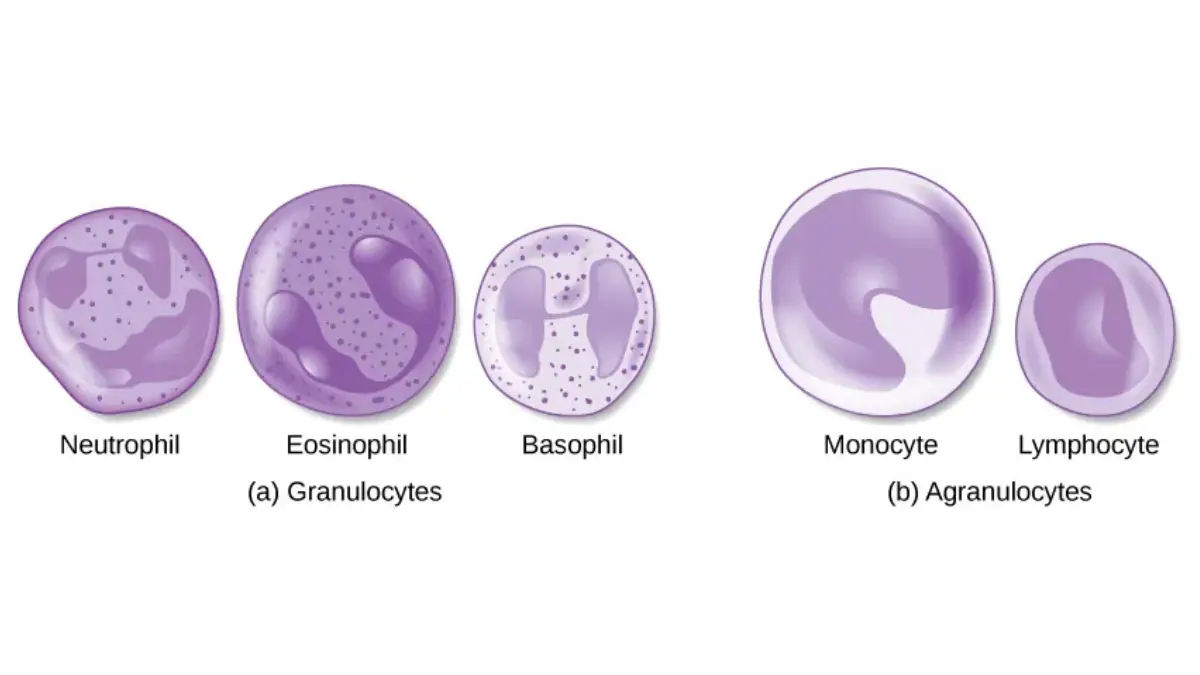
Adapted from OpenStax Figure 31.7, licensed under [CC BY 4.0]
Platelets and MPV
The final component measures your blood’s ability to form clots.
The platelet count is the number of these clotting fragments in your blood. Some reports also list MPV (mean platelet volume), the average platelet size, which can occasionally help distinguish causes of an abnormal count. As with the other indices, MPV ranges are laboratory-specific.
How to read your own results sheet
Most CBC reports lay the numbers out the same way, and a simple habit makes them readable.
Each line shows your result, the lab’s reference range beside it, and a flag (often H for high or L for low) if you fall outside that range. Read your own reference column first — not a range you found online — because that is the range your laboratory considers normal for its equipment and its population. A flag simply means “outside this lab’s usual range,” which is the beginning of a question, not an answer.
What your red blood cell numbers can mean
Your red-cell values are the part of the CBC most people react to first, because low numbers are common and the word attached to them — anemia — sounds alarming, so here is what they actually signal.
Anemia is the condition of having a lower-than-normal amount of healthy red blood cells, and it is what low hemoglobin, low hematocrit, or a low red blood cell count most often points toward. According to the National Heart, Lung, and Blood Institute, when your body does not get enough oxygen-rich blood, you may feel tired or weak, or notice shortness of breath, dizziness, headaches, or an irregular heartbeat. It is a common, usually treatable condition — not automatically a sign of something dire.
📊 Clinical Data Point: About 3 million people in the United States have anemia, according to the National Heart, Lung, and Blood Institute (citing CDC figures). Mild anemia is common and treatable, and it can be caused by diet, medicines, or another medical condition. (Source: NHLBI, Anemia.)
What low hemoglobin and hematocrit suggest
A low red-cell result tells you that your oxygen-carrying capacity is reduced, but not yet why — and the “why” list is long.
Low red blood cells, hemoglobin, or hematocrit can result from blood loss (sudden, or slow loss such as heavy menstrual periods over time), from too little iron, or from deficiencies of vitamin B12, folate, or vitamin B6. It can also stem from certain chronic conditions such as chronic kidney disease, from bone marrow problems, from the breakdown of red cells, and — importantly to name honestly — from some cancers and cancer treatments, including leukemia and multiple myeloma. That range is exactly why a low value is a clue, not a diagnosis.
Because the causes are so varied, a single low hemoglobin cannot tell you which of these applies. That determination comes from your symptoms, your history, and follow-up testing — most commonly iron studies and vitamin-level tests.
✅ Patient Action: If your red-cell values are low, ask your primary care clinician: “What is the most likely cause of my anemia given my history, and which follow-up test — iron studies, B12 and folate, or something else — do you recommend first?” You can prepare by reviewing what abnormal iron studies can mean and how to read your vitamin B12 result.
What high hemoglobin or hematocrit can mean
Less commonly, red-cell values run high, and the causes range from the entirely benign to conditions that need management.
High red blood cells, hemoglobin, or hematocrit can simply reflect dehydration — when you are low on fluids, your blood is more concentrated, so the red-cell fraction reads higher. It can also result from long-standing low blood oxygen (from heart or lung disease, chronic carbon monoxide exposure, or living at high altitude), from kidney conditions, from smoking or testosterone use, or from a bone marrow condition called polycythemia vera.
This is one of the clearest examples of why context matters: the same high hematocrit could mean you were dehydrated on the morning of the draw, or could point to something your doctor will want to investigate further.
Reading MCV: small cells versus large cells
The size of your red cells, captured by MCV, is one of the most useful clues on the whole panel for narrowing down a cause of anemia.
When red cells are smaller than usual (a low MCV, called microcytic), iron deficiency is a common cause. When they are larger than usual (a high MCV, called macrocytic), deficiencies of vitamin B12 or folate are frequent culprits, along with some other causes. When the size is normal but the count is low, causes such as recent blood loss or chronic disease come into consideration.
🩺 Physician Note: Clinicians rarely read MCV in isolation. They combine it with your hemoglobin, your RDW (how uneven your cells are), and often a follow-up panel to move from “you have anemia” toward “you have this type of anemia” — which is what determines treatment. This is general clinical practice, not a substitute for your own doctor’s interpretation of your specific numbers.
Why a red-cell flag is a starting point, not a diagnosis
It is worth stating plainly, because it is where so much unnecessary fear comes from.
A flagged red-cell value means your number sits outside your lab’s usual range. It does not, by itself, tell you whether the cause is a minor dietary shortfall, a heavy period, a chronic condition, or something more serious. The value’s job is to prompt the next question — and iron-deficiency anemia, the single most common type, is very treatable once identified. You can read the National Heart, Lung, and Blood Institute’s patient guide to anemia for a fuller picture of the types and causes.
What your white blood cell count is telling you
White-cell results tend to trigger fears of infection or leukemia, so it helps to know that a high count is common, usually reactive, and rarely the whole story on its own.
The white blood cell count measures the total number of infection-fighting cells in your blood, and the normal count runs a wide range. A CBC with differential then shows how many of each type you have, which is often where the useful information lives.
📊 Clinical Data Point: The normal white blood cell count is 4,500 to 11,000 cells per microliter, according to the National Library of Medicine, which also notes that normal value ranges vary slightly among different laboratories. (Source: MedlinePlus, CBC blood test.)
What a high white count (leukocytosis) can mean
A white count above your lab’s range is called leukocytosis, and most of the time it reflects your immune system doing its job.
According to the National Library of Medicine, a high white blood cell count can result from infections, from inflammation-related conditions such as rheumatoid arthritis, lupus, or allergy, from certain medicines like corticosteroids, from severe physical or emotional stress, and from tissue damage such as burns or a heart attack. It can also, less commonly, reflect leukemia. That last possibility is real and worth naming, but it sits at the end of a list dominated by ordinary, reactive causes.
The most frequent reason for a mildly high white count is simply that your body is responding to an infection or inflammation. Your clinician weighs the degree of elevation, the differential pattern, and your symptoms before drawing any conclusion.
What a low white count (leukopenia) can mean
A white count below your lab’s range is called leukopenia, and it too has a broad set of causes.
The National Library of Medicine lists causes including viral infections such as infectious mononucleosis, autoimmune diseases such as lupus, an enlarged spleen or liver disease, bone marrow problems, chemotherapy medicines, alcohol overuse with liver damage, and certain other medicines. Some of these are transient — a viral illness can temporarily lower your count — while others need closer evaluation.
Reading the differential: neutrophils, lymphocytes, and the rest
The differential is where a single “high white count” becomes a more specific story, because the type that is elevated hints at the cause.
Neutrophils are the most common white cell and your main defense against bacteria, while lymphocytes largely target viruses. A shift toward neutrophils can accompany a bacterial pattern; a shift toward lymphocytes can accompany a viral one. Eosinophils rise with allergies and parasitic infections, and monocytes and basophils each play their own roles.
📊 Clinical Data Point: In adults, the differential typically runs about 40% to 60% neutrophils, 20% to 40% lymphocytes, and 2% to 8% monocytes, with eosinophils and basophils making up only small fractions — though these are commonly used intervals and are lab-specific in practice. (Source: NCBI StatPearls, Normal and Abnormal Complete Blood Count With Differential.)
🩺 Physician Note: An increase in one white-cell type mathematically lowers the percentage of the others, so clinicians often look at absolute counts (the actual number of each cell type) rather than percentages alone — for instance, tracking the absolute neutrophil count during chemotherapy. This is standard laboratory interpretation, offered as general education.
Does a CBC prove I have an infection?
This is one of the most common misconceptions about the test, and the honest answer helps set expectations.
A high white count is consistent with infection, but it does not confirm one, and it cannot identify which specific germ is responsible. Plenty of non-infectious things raise the white count, and some infections do not raise it at all. To identify a specific infection, your clinician needs other tests — a culture, a specific pathogen test, or imaging — guided by your symptoms.
A CBC also does not directly measure inflammation. Markers such as CRP are separate tests; you can read about what a CRP result means if that has been ordered alongside your CBC.
When a white-count change needs prompt review
Most white-count changes are handled routinely, but a few situations warrant timelier attention, described here in general terms.
A markedly abnormal white count — very high or very low — or a count paired with concerning symptoms such as a high fever, signs of a serious infection, or unusual bruising and bleeding, deserves prompt medical evaluation rather than waiting. The specifics of urgency depend on your full picture, which is covered in the section on results that warrant prompt attention.
What your platelet count means
Platelets govern your blood’s ability to clot, so an abnormal count naturally raises worries about bleeding — but the number is interpreted in context, and it is not the same as your actual clotting ability.
The platelet count measures the number of clotting fragments in your blood, and the normal range spans a wide band.
📊 Clinical Data Point: A normal platelet count runs from about 150,000 to 400,000 per microliter, according to the National Library of Medicine, with the note that normal ranges vary slightly between laboratories. (Source: MedlinePlus, CBC blood test.)
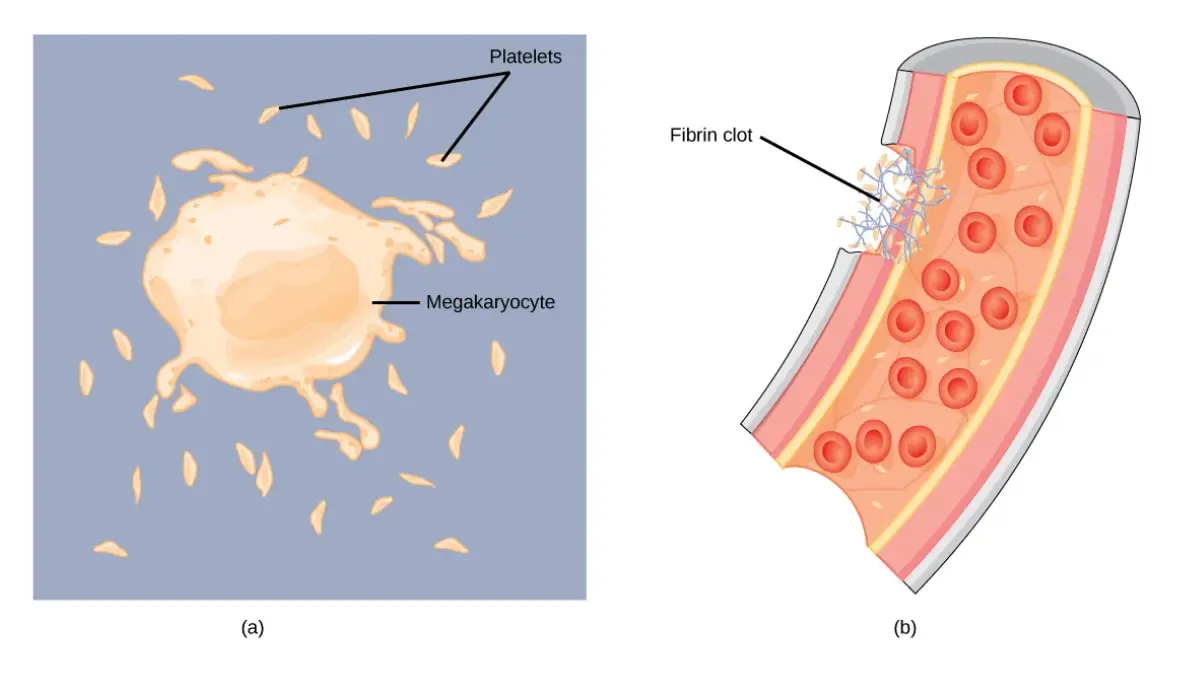
Adapted from OpenStax Figure 31.8b, licensed under [CC BY 4.0]
What a low platelet count (thrombocytopenia) can mean
A platelet count below your lab’s range is called thrombocytopenia, and it has many possible causes, most of which are identified with a clinician’s help.
The National Library of Medicine lists causes including conditions in which platelets are destroyed, an enlarged spleen, bone marrow problems, chemotherapy medicines, and — as a common and usually mild example — pregnancy. A mildly low platelet count is frequently rechecked before any conclusion is drawn, because a single value can be affected by how the sample was collected or by a temporary cause.
What a high platelet count (thrombocytosis) can mean
A count above your lab’s range is called thrombocytosis, and it is often reactive — a response to something else rather than a primary problem.
According to the National Library of Medicine, a high platelet count can accompany iron deficiency, bleeding, bone marrow problems, or certain diseases including cancer or blood disorders. Reactive causes, such as inflammation or iron deficiency, are common, and the count often returns to normal when the underlying trigger resolves.
Platelet count is not the same as clotting ability
This distinction genuinely surprises many people, and it is clinically important.
Your platelet count tells you how many platelets you have, but it does not measure how well your blood actually clots. Clotting also depends on proteins called clotting factors, which are measured by entirely different tests. If your clotting function needs checking, your clinician orders tests such as PT/INR or PTT — you can read about coagulation test results and decode a high or low platelet count in more detail.
✅ Patient Action: If your platelet count is flagged, ask your primary care clinician: “Is this result likely reactive or something that needs further testing, and should it be rechecked before we act on it?” Bring any history of easy bruising, unusual bleeding, or new medications to that conversation.
Normal CBC ranges and why they vary
The single most useful thing to understand about “normal” on a blood test is that it is not one fixed set of numbers — which is exactly why the range printed on your own report matters more than any chart you find online.
The values below are common adult reference ranges, drawn from the National Library of Medicine, but the National Heart, Lung, and Blood Institute is explicit that factors such as age, sex, high altitude, and race can also affect what counts as normal. Read this table as typical, not definitive.
Typical adult reference ranges
| Measurement | Typical adult range | What it reflects |
|---|---|---|
| White blood cells (WBC) | 4,500–11,000 cells/mcL | Total immune-cell count |
| Red blood cells (RBC) | Male 4.6–6.2 million/mcL; Female 4.2–5.4 million/mcL | Number of oxygen-carrying cells |
| Hemoglobin | Male 13–18 g/dL; Female 12–16 g/dL | Oxygen-carrying protein |
| Hematocrit | Male 40%–55%; Female 36%–48% | Fraction of blood that is red cells |
| Platelets | 150,000–400,000 /mcL | Clotting-fragment count |
| MCV | 80–100 fL | Average red-cell size |
| MCH | 27–32 pg/cell | Average hemoglobin per cell |
| MCHC | 32–36 g/dL | Hemoglobin concentration per cell |
| Differential | Neutrophils ~40%–60%; Lymphocytes ~20%–40%; Monocytes ~2%–8% | Proportions of white-cell types |
Sources: reference ranges from MedlinePlus, CBC blood test; differential percentages from NCBI StatPearls, Normal and Abnormal Complete Blood Count With Differential. Ranges vary slightly among laboratories and with age, sex, altitude, and other factors.
Why ranges differ by lab, age, and sex
If two labs report your identical blood a little differently, both can still be “right,” and here is why.
Each laboratory establishes its own reference intervals based on its equipment and the population it serves, so the “normal” band can shift slightly from one lab to another. Ranges also differ by sex — men and women have different typical hemoglobin and hematocrit values — and by age, with children’s ranges changing as they grow. Even altitude matters, because people living at higher elevations often carry more red cells.
What “flagged” on your report actually means
A flag looks official and final, but its meaning is narrower than it appears.
A high or low flag simply indicates that your value falls outside that laboratory’s usual range. It is a prompt for interpretation, not a diagnosis, and being marginally outside a range is common and often unremarkable. What your clinician weighs is how far outside, in what pattern, and alongside which symptoms.
✅ Patient Action: When reviewing your results, read your own laboratory’s reference column first and compare each value to that range — not to a number from a search result. If a value is flagged, note by how much and bring the report to your clinician rather than self-interpreting from an online chart.
What a CBC can’t show you
Here is the section the biggest health sites tend to bury, and it may be the most reassuring part of this entire guide: knowing the test’s limits protects you from both false alarm and false comfort.
A complete blood count counts and sizes your blood cells. That is genuinely useful — but it means a CBC is blind to a great deal, and understanding the blind spots is as important as understanding the numbers.
A normal CBC does not rule out serious disease
This is the hardest limit to accept when you feel unwell but your results came back “normal,” and it is true nonetheless.
A normal CBC is reassuring, but it does not measure everything, and many serious conditions can be present with a normal blood count. If you have persistent or worsening symptoms, a normal CBC is a reason to keep investigating with your clinician — not a reason to stop. The test screens your blood cells; it does not screen your whole body.
Can a CBC detect cancer or leukemia?
This is the fear underneath most abnormal-result searches, so it deserves a direct, honest answer.
A CBC cannot diagnose cancer on its own, and a normal CBC does not rule cancer out. Abnormal counts can appear with some cancers — particularly blood cancers like leukemia — but they can equally appear with dozens of benign causes, so an abnormal CBC raises a question rather than delivering an answer. Many solid tumors do not change the CBC at all, especially early on.
For blood cancers specifically, the picture is telling. According to the National Library of Medicine, a white blood count can show whether your white-cell number is too high or too low, but it cannot confirm a diagnosis — so it is used alongside other tests, which may include a CBC, a blood differential, a blood smear, and a bone marrow test. In other words, a suspicious count points toward further, definitive testing; it is never the last word. You can read the National Library of Medicine’s overview of the white blood count for how these tests fit together.
⚠️ Clinical Warning: Do not use a normal CBC to talk yourself out of investigating real, ongoing symptoms, and do not read an abnormal CBC as a cancer diagnosis. Both errors are common and both are harmful. Only a clinician, using your full picture and the right follow-up tests, can interpret what your counts mean for you.
What a CBC doesn’t measure at all
Beyond cancer, a CBC simply does not test for many of the things people assume it covers.
A CBC does not measure your blood sugar, so it cannot screen for or monitor diabetes. It does not measure your electrolytes, kidney function, or liver function — those come from a metabolic panel. It does not measure your cholesterol, and it does not directly measure your clotting function or inflammation markers. Each of those requires a separate, specific test.
That is why your doctor often orders several panels together: each one sees a different part of your health that the others miss.
Why one test is a snapshot, not the whole picture
Even for what it does measure, a CBC captures a single moment.
Your blood counts fluctuate with hydration, recent activity, illness, stress, and the time of day. A CBC freezes one instant of that moving picture, which is why a borderline value is so often rechecked before it means anything. Trends across several tests usually tell your clinician far more than any single draw.
What a CBC can and can’t do — at a glance
| A CBC can help with | A CBC cannot do |
|---|---|
| Flag anemia (low red cells/hemoglobin) | Identify the cause of anemia on its own |
| Show a high or low white-cell count | Confirm a specific infection or name the germ |
| Reveal a high or low platelet count | Measure how well your blood actually clots |
| Signal patterns that may prompt further testing | Diagnose cancer by itself, or rule it out |
| Monitor known conditions and treatments over time | Measure blood sugar, cholesterol, kidney, or liver function |
A CBC is a screening and monitoring test that points toward next steps; definitive answers come from targeted follow-up testing interpreted by a clinician.
When one abnormal value matters — and when it usually doesn’t
If you take one practical skill from this guide, make it this: a calm framework for judging a single flagged value, so a lone red flag on a portal does not cost you a sleepless night it didn’t need to.
How a single flag differs from a pattern
Clinicians react very differently to one out-of-range number than to a consistent pattern, and so should you.
A single value slightly outside your lab’s range, with no symptoms and no other abnormalities, is common and frequently benign. A pattern — several related values off together, or one value trending in the same direction across repeated tests — carries more weight. The isolated flag usually earns a recheck; the pattern usually earns a next step.
Benign reasons a value can be off
Many abnormal CBC results have entirely ordinary explanations that have nothing to do with disease.
Dehydration can concentrate your blood and push red-cell values up. Recent intense exercise or physical or emotional stress can temporarily raise your white count. A recent viral illness can lower it. Pregnancy shifts several values, and even normal laboratory variation means a result near the edge of a range can land just inside on one day and just outside on another.
🩺 Physician Note: Because a borderline result can reflect timing rather than illness, repeating an out-of-range value is a normal, expected step — not a sign that something was missed. Clinicians routinely recheck a single mildly abnormal number before ordering anything further. This reflects general clinical practice and is not specific medical advice for your situation.
When a repeat test is the normal next step
Rechecking is so common that it is worth normalizing, because being asked to repeat a test can feel ominous when it isn’t.
If your clinician asks you to repeat a CBC in a few weeks, that is typically prudence, not alarm — it distinguishes a real, persistent change from a one-off blip. If you want to understand your specific flagged values in more depth before that follow-up, you can decode your specific abnormal CBC values as background for the conversation.
Signs a result deserves prompt attention
Calibration cuts both ways: most flags can wait for a routine follow-up, but some should not.
A markedly abnormal value, or any abnormal result paired with concerning symptoms — significant unexplained bruising or bleeding, signs of a serious infection, severe fatigue, or feeling acutely unwell — should prompt timely contact with your clinician rather than waiting. Which situations these are, and what to do while you wait to be seen, are covered in the section on results that warrant prompt attention.
What happens after an abnormal CBC
Knowing the realistic sequence of next steps takes much of the dread out of an abnormal result, because “we need another test” is the normal, expected response to a flag — not a sign of catastrophe.
Repeating the CBC
The first step is often the simplest one.
For a mildly abnormal or borderline value, your clinician may simply repeat the CBC after an interval to see whether the change is real and persistent or a one-time blip. A result that normalizes on recheck often needs nothing more.
Iron studies, ferritin, and B12/folate testing
When anemia is the question, targeted nutrient tests usually come next.
Because a CBC can flag anemia but not its cause, follow-up commonly includes iron studies (including ferritin, a measure of stored iron), and vitamin B12 and folate testing. These distinguish, for example, iron-deficiency anemia from a B12-deficiency anemia — a distinction that directly changes treatment. Nutrient testing such as understanding a vitamin D result may also be part of a broader work-up depending on your symptoms.
The peripheral blood smear
Sometimes the machine’s count needs a human eye.
A peripheral blood smear places a drop of your blood on a slide so a professional can examine the cells’ size, shape, and appearance directly under a microscope. It can reveal features an automated count misses, and it is a routine next step when a CBC shows an unexplained or unusual result.
🔬 How It Works: On a smear, a trained reviewer looks for red cells that are too small, too large, or oddly shaped, for abnormal or immature white cells, and for clues the analyzer flagged. This is also how features suggestive of certain blood disorders are first spotted — after which more definitive tests, such as a bone marrow examination, may follow if needed.
When you might see a specialist
Most CBC abnormalities are handled by primary care, but some lead to a referral.
If results suggest a blood disorder or remain unexplained after initial testing, your clinician may refer you to a hematologist, a doctor who specializes in blood conditions. A bone marrow test, when needed, helps find the cause of low or high blood cell counts and is typically arranged through that specialist.
✅ Patient Action: At your follow-up, ask: “Given my specific result, which single follow-up test makes the most sense first, and what would each possible outcome mean for next steps?” This keeps the work-up focused and helps you understand the plan rather than just waiting for calls.
How to prepare for a CBC and what to expect
If your CBC is still ahead of you, preparation is refreshingly simple — and knowing what the draw is like helps if needles make you uneasy.
Do you need to fast for a CBC?
This is the most common prep question, and the answer is reassuringly straightforward.
For a CBC alone, no special preparation is needed, and you generally do not need to fast. However, if your provider ordered other tests on the same blood sample — such as a glucose or cholesterol test — you may need to fast for several hours beforehand. Your provider will tell you if any special instructions apply, so follow their specific guidance.
What the blood draw is like
The procedure itself is brief and low-risk.
A healthcare professional inserts a small needle into a vein, usually in your arm, and collects a sample into a tube; the whole process typically takes only a few minutes. When the needle goes in, you may feel a brief prick or moderate pinch, and afterward there may be minor throbbing or slight bruising that soon fades. Serious risks are very uncommon.
How long results take
Turnaround is usually fast, though it varies.
A CBC is a common, automated test, and results are often available within a day, depending on the laboratory. A sample that the analyzer flags for a manual smear review may take a little longer, because a person is giving it a closer look.
Tips if you’re nervous about needles
Feeling anxious about a blood draw is common, and a few small steps help.
Tell the person drawing your blood that needles make you nervous — they do this all day and can help. Sitting down, looking away, breathing slowly, and staying well hydrated (which can make veins easier to access) all tend to make the experience easier. If you have ever felt faint during a draw, mention that too, so they can have you lie down.
CBC results in pregnancy, children, and chronic conditions
Some situations change how a blood count is read entirely, and in these cases the safest guidance this article can give is that the numbers require individual interpretation by the clinician who knows the full context.
Why CBC ranges shift in pregnancy
Pregnancy changes the blood in normal, expected ways.
During pregnancy, blood volume expands and several CBC values shift as a result, so a value that would be flagged outside of pregnancy may be entirely normal during it. This is one reason pregnancy-related results should be interpreted by the clinician managing the pregnancy, using pregnancy-specific expectations rather than standard adult ranges.
Reading a child’s CBC
Children are not small adults when it comes to reference ranges.
Normal CBC values change as a child grows, so a pediatric result must be compared against age-appropriate ranges, not adult ones. A pediatrician interprets a child’s counts in the context of their age, growth, and symptoms.
CBC monitoring on certain medications
For some treatments, repeat CBCs are a built-in safety measure.
Certain medications and treatments — including chemotherapy and some others — can lower blood counts, so clinicians schedule regular CBCs to monitor for this and adjust care accordingly. If you have been asked to get repeat CBCs while on a medication, that monitoring is the point of the schedule, and the specific numbers your care team watches for are theirs to define and act on.
CBC and cancer treatment monitoring
In cancer care, the CBC is a workhorse for tracking treatment effects.
Because treatments such as chemotherapy and radiation affect the bone marrow where blood cells are made, CBCs are used to watch red cells, white cells, and platelets over the course of treatment. Low counts during treatment are common and are managed by the oncology team; this is monitoring, not a new diagnosis.
Why these results always need clinician interpretation
Across all of these situations, the through-line is the same.
Pregnancy, childhood, and active treatment each change what “normal” means, and each raises the stakes of misreading a number. That is why this section deliberately does not offer population-specific cutoffs to act on — those belong to the clinician managing your care.
✅ Patient Action: If you are pregnant, reading a child’s result, or in treatment, ask the relevant specialist — your OB, your pediatrician, or your oncologist — directly: “How should this specific result be interpreted given my situation, and is any action needed right now?” Do not compare these results to a general adult range on your own.
CBC results that warrant prompt medical attention
Most abnormal counts can wait for a routine follow-up, but a few situations should not — and this section is meant to help you recognize them in general terms, not to hand you numbers to self-diagnose with.
When to contact your clinician promptly
Some combinations of result and symptom call for timelier contact.
If a CBC value is markedly abnormal, or if an abnormal result comes with symptoms that concern you, contact your clinician promptly rather than waiting for a scheduled call. Trust that pairing — a flagged number plus a symptom that feels wrong — as your cue to reach out.
Symptoms that shouldn’t wait for a routine follow-up
Certain symptoms deserve attention regardless of what a number says.
New or unexplained easy bruising or bleeding, signs of a serious infection (such as a high fever with feeling very unwell), severe or rapidly worsening fatigue, or shortness of breath are examples of symptoms that warrant prompt medical evaluation. These are categories to take seriously, not a checklist to self-diagnose from — the specifics of urgency depend on your full clinical picture.
⚠️ Clinical Warning: If you have severe symptoms — such as heavy or uncontrollable bleeding, signs of a severe infection, chest pain, or trouble breathing — seek emergency care immediately rather than waiting for blood-test interpretation. A test result is never a reason to delay care for a genuine emergency.
Why context — not a single number — drives urgency
Urgency is a clinical judgment, and it rests on more than one value.
The same platelet or white-cell number can be routine in one person and urgent in another, depending on symptoms, history, medications, and how quickly the value changed. That is precisely why this article does not attach action thresholds to specific numbers: only a clinician can weigh the full context that determines how fast you need to be seen.
What to do while you wait to be seen
Practical steps help while you arrange care.
Write down your symptoms and when they started, bring your full results and your medication list to your appointment, and note any recent illnesses or changes. If your symptoms worsen while you wait, escalate — call back, use an urgent care option, or seek emergency care for anything severe.
✅ Patient Action: Ask your clinician directly: “Given my result and these specific symptoms, how quickly should I be seen, and what warning signs should make me seek care sooner?” Having that threshold spelled out for your situation is far more useful than any general rule.
CBC vs. the other common blood tests
A CBC is often drawn alongside other panels, and people frequently assume it covers ground it doesn’t — so here is how it differs from the tests it most often sits beside.
CBC vs. a metabolic panel
These two are the most commonly confused, and they measure completely different things.
A CBC counts your blood cells. A metabolic panel measures blood chemistry — glucose, electrolytes, and markers of kidney and liver function. Neither overlaps with the other, which is why both are frequently ordered together to give a fuller picture. If your liver markers were part of your bloodwork, you can review how to read liver function tests separately.
CBC vs. a blood sugar or A1C test
If diabetes is a concern, a CBC is not the test that answers it.
A CBC does not measure blood sugar at all, so it cannot screen for or monitor diabetes. That requires a glucose test or an HbA1c, which reflects your average blood sugar over time — you can read about what your HbA1c number means if that was ordered.
CBC vs. a lipid (cholesterol) panel
Cholesterol is another common assumption that a CBC does not cover.
Your cholesterol is measured by a lipid panel, not a CBC, and it is one of the tests that often requires fasting beforehand. If cholesterol was part of your bloodwork, see reading a cholesterol (lipid) panel for what those numbers mean.
CBC vs. clotting tests
Finally, the platelet count on a CBC is not a clotting test.
A CBC counts your platelets, but it does not measure how well your blood clots; that function is measured by coagulation tests such as PT/INR. This is why someone can have a normal platelet count and still need clotting function checked separately.
Why you often get several panels at once
Ordering multiple tests together is efficient, not excessive.
Each panel sees a different dimension of your health — cells, chemistry, cholesterol, clotting — and combining them from a single blood draw gives your clinician a broad view while sparing you extra needle sticks. A “normal CBC” therefore says your blood cells look fine; it says nothing about the parts other tests measure.
Complete blood count: your questions answered
1. What does a CBC test show?
A complete blood count shows the number and size of the cells in your blood — red blood cells, white blood cells, and platelets — plus hemoglobin and hematocrit. It can flag anemia, a high or low white-cell count, and a high or low platelet count. It reveals patterns that prompt further testing, but it does not diagnose a specific disease on its own.
2. What’s included in a complete blood count?
A CBC includes your red blood cell count, white blood cell count, platelet count, hemoglobin, and hematocrit, along with red cell indices such as MCV, MCH, MCHC, and RDW. A CBC with differential adds a breakdown of your white blood cells into neutrophils, lymphocytes, monocytes, eosinophils, and basophils. Together these describe both the number and the character of your blood cells.
3. What are normal CBC ranges?
Typical adult ranges include a white cell count of 4,500 to 11,000 per microliter and a platelet count of about 150,000 to 400,000 per microliter, per the National Library of Medicine. Hemoglobin, hematocrit, and red cell counts differ by sex. Ranges vary slightly among laboratories and with age, sex, and altitude, so your own report’s reference range is the one that applies to you.
4. Can a CBC detect cancer?
A CBC cannot diagnose cancer on its own, and a normal CBC does not rule cancer out. Abnormal counts can appear with some cancers but also with many benign causes, so they raise a question rather than confirm anything. Many cancers do not change the CBC at all. Persistent symptoms should always be evaluated by your clinician regardless of a normal result.
5. Can a CBC detect leukemia?
A CBC can raise suspicion of leukemia — for example, through abnormal white-cell counts or unusual cells — but it cannot confirm it. According to the National Library of Medicine, a white blood count can’t confirm a diagnosis and is used with other tests, which may include a blood differential, a blood smear, and a bone marrow test. Definitive diagnosis requires that further testing, interpreted by a specialist.
6. Does a CBC show infection?
A CBC can suggest infection through a high white blood cell count, but it cannot confirm one or identify which germ is responsible. Many non-infectious things raise the white count, and some infections don’t raise it at all. Identifying a specific infection requires other tests, such as a culture, guided by your symptoms and examined by your clinician.
7. What does a high white blood cell count mean?
A high white blood cell count, called leukocytosis, most often reflects your immune system responding to infection or inflammation. Per the National Library of Medicine, it can also result from certain medicines, severe stress, tissue damage such as burns, and, less commonly, leukemia. Most mild elevations are reactive. Your clinician interprets the degree, pattern, and your symptoms before drawing conclusions.
8. What does a low white blood cell count mean?
A low white blood cell count, called leukopenia, can result from viral infections, autoimmune diseases, an enlarged spleen, bone marrow problems, chemotherapy, or certain medicines, according to the National Library of Medicine. Some causes are temporary, such as a passing viral illness, while others need closer evaluation. A clinician interprets the result alongside your history and symptoms to determine whether follow-up is needed.
9. What does low hemoglobin mean?
Low hemoglobin usually points to anemia, meaning your blood carries less oxygen than it should. Causes range widely — from iron, B12, or folate deficiency and blood loss to chronic conditions and, less commonly, bone marrow or blood cancers. A low value flags the problem but not its cause, which follow-up tests such as iron studies help identify. Discuss your specific result and next steps with your clinician.
10. What does high MCV mean?
A high MCV means your red blood cells are larger than usual, described as macrocytic. Deficiencies of vitamin B12 or folate are common causes, among others. MCV is most useful combined with your hemoglobin and RDW to narrow down the type of anemia, which guides treatment. A high MCV is a clue for further testing, not a diagnosis on its own, so review it with your clinician.
11. What does RDW mean?
RDW, or red cell distribution width, measures how much your red blood cells vary in size from one another. A high RDW means the cells are unusually uneven, which can be an early clue in certain anemias, particularly when read alongside MCV. RDW reference ranges vary by laboratory and appear on your own report. Your clinician uses it as one piece of the red-cell picture, not in isolation.
12. What does a low platelet count mean?
A low platelet count, called thrombocytopenia, can result from conditions that destroy platelets, an enlarged spleen, bone marrow problems, chemotherapy, or — commonly and often mildly — pregnancy, per the National Library of Medicine. A mildly low count is frequently rechecked before any conclusion, since collection factors or temporary causes can affect it. Bring any history of easy bruising or bleeding to your clinician for interpretation.
13. What is a CBC with differential?
A CBC with differential is a CBC that also counts how many of each type of white blood cell you have — neutrophils, lymphocytes, monocytes, eosinophils, and basophils — rather than just the total. This breakdown can hint at whether a challenge is bacterial, viral, allergic, or something else. Many analyzers produce it automatically. It still requires clinical interpretation and does not diagnose a condition by itself.
14. Do I need to fast for a CBC?
For a CBC alone, you generally do not need to fast, and no special preparation is required, according to the National Library of Medicine. However, if other tests — such as glucose or cholesterol — are drawn from the same sample, you may need to fast for several hours beforehand. Your provider will give you specific instructions, so follow their guidance for your particular set of tests.
15. How long do CBC results take?
A CBC is a common, automated test, so results are often available within about a day, depending on the laboratory. If your sample is flagged for a manual blood smear review — where a professional examines your cells under a microscope — it may take somewhat longer. Your provider’s office or patient portal is the best source for your specific turnaround time.
16. Can dehydration affect a CBC?
Yes. Dehydration concentrates your blood, which can push red-cell values such as hematocrit higher than they would otherwise read, according to the National Library of Medicine. This is one reason a single out-of-range value is often rechecked, and why context — including how hydrated you were at the draw — matters. Your clinician weighs factors like this when interpreting a borderline result.
17. If my CBC is normal, does that mean I’m healthy?
Not necessarily. A normal CBC is reassuring about your blood cells, but it does not measure everything — it says nothing about your blood sugar, cholesterol, kidney or liver function, or many other conditions. Serious illness can be present with a normal blood count. If you have persistent or worsening symptoms, keep investigating with your clinician rather than treating a normal CBC as an all-clear.
Your next step after reading your CBC
If you arrived here anxious about a flagged number, you now know the most important thing: a CBC is a screening test that points toward questions, and a single abnormal value is far more often the start of a manageable conversation than the sign of a crisis. That is not false reassurance — real problems do show up on a CBC — but it is an accurate frame for what the numbers can and cannot tell you.
Where you go next depends on what your result showed. If your red cells were low, what abnormal iron studies can mean is a useful next read; if your platelets were flagged, see decode a high or low platelet count; and to work through your specific numbers before your appointment, use decode your specific abnormal CBC values.
Before your next appointment, download our free “Questions to ask your doctor about your blood test results” checklist. It turns a page of intimidating numbers into a focused conversation and helps you leave the visit understanding your results and your plan.
The single most important thing you can do is bring your full printed result — with your own laboratory’s reference column — to your clinician and ask one direct question: “Given my specific values and my symptoms, what is the most likely explanation, and what is the one next step you recommend?” That question moves you from worrying about a number to acting on a plan.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.