When Every Breath Counts: Understanding Lung Embolism
Sarah Martinez, a 42-year-old marketing executive, dismissed her sudden breathlessness during a client meeting as anxiety—until she coughed up blood. Within two hours, emergency physicians diagnosed a massive pulmonary embolism that nearly claimed her life. Her story echoes thousands of Americans who face this silent killer annually, often without recognizing the warning signs until it’s almost too late.
Lung embolism, medically termed pulmonary embolism (PE), occurs when a blood clot blocks one or more arteries in the lungs, abruptly cutting off oxygen supply to vital tissues. This life-threatening condition strikes up to 900,000 Americans each year, killing an estimated 60,000 to 100,000 people annually according to the Centers for Disease Control and Prevention. The critical difference between life and death? Early recognition and treatment, which improves survival rates to over 95% when initiated within the first few hours.
The statistics paint a sobering picture: sudden death is the first symptom in approximately 25% of people who experience a lung embolism, often before they can reach medical care. Yet this condition remains largely preventable. Understanding the eight critical warning signs, recognizing your personal risk factors, and knowing when to seek emergency care can literally save your life or that of someone you love.
Blood clots in the lungs don’t discriminate—they affect individuals across all demographics, though certain factors significantly elevate risk. From prolonged immobility during long flights to recent surgery, hormonal medications, or underlying cancer treatment, multiple pathways can lead to this cardiovascular emergency. The CDC reports that roughly 1 in 10 hospital deaths are directly related to blood clots in the lungs, making venous thromboembolism a leading cause of preventable hospital mortality.
What You’ll Discover in This Guide
- The 8 emergency warning signs of lung embolism that demand immediate medical attention, ranked by urgency and severity
- How blood clots travel from leg veins to your pulmonary arteries, and why deep vein thrombosis prevention is critical
- Evidence-based treatment options including anticoagulants, thrombolytics, and surgical interventions with comparative success rates
- Your personalized risk assessment using our Symptom Checker to evaluate potential red flags
- Recovery timelines and lifestyle modifications that help survivors return to normal activities while preventing recurrence
⚡ What This Means For You: Time-to-treatment is everything when facing a lung embolism. Recognizing these eight critical signs and acting within the first few hours can mean the difference between a full recovery and becoming one of the 100,000 annual fatalities. Every minute counts—this guide equips you with the knowledge to identify PE symptoms before they become fatal.
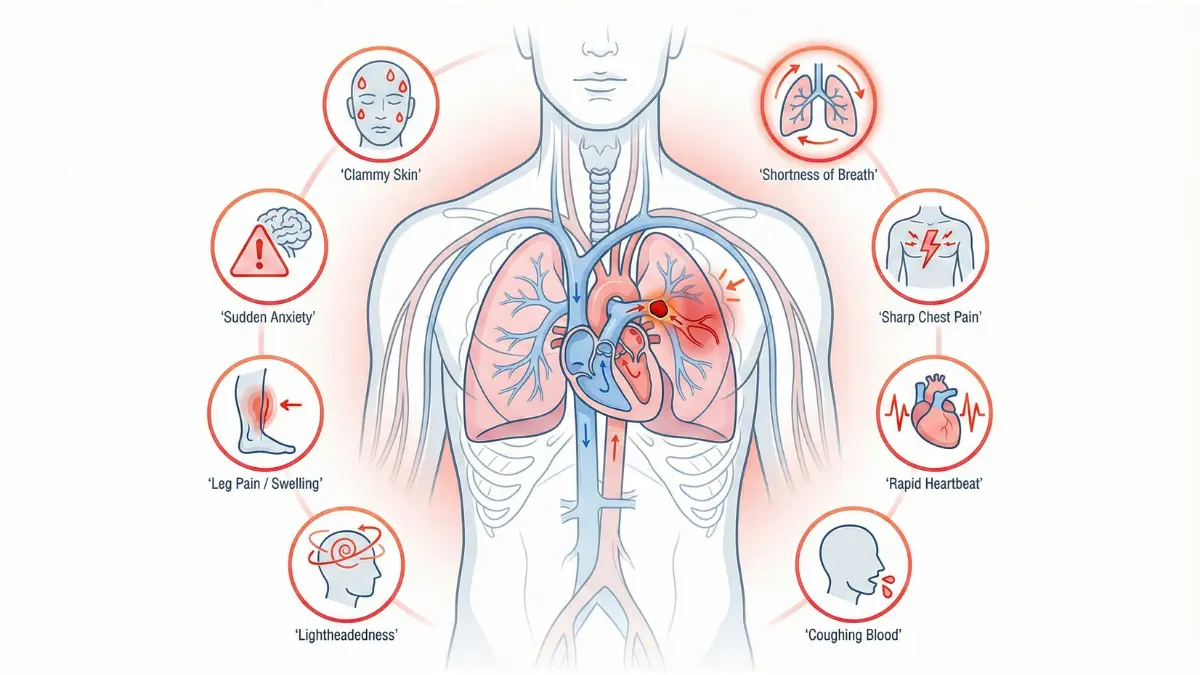
The 8 Warning Signs You Cannot Ignore
8 Critical Signs of Lung Embolism (Ranked by Urgency)
Recognizing the symptoms of a pulmonary embolism can be challenging because they often mimic other respiratory and cardiac conditions, leading to dangerous delays in treatment. According to the National Institutes of Health, approximately 30% of untreated patients with blood clots in the lungs die, compared to only 8% who receive timely therapy. Many cases are initially misdiagnosed as anxiety attacks, pneumonia, or asthma, wasting precious time when every minute matters. Understanding these eight emergency warning signs—and knowing when to call 911—could save your life.
1. Sudden Shortness of Breath (Dyspnea) – The #1 Red Flag
Dyspnea is the most common symptom of lung embolism, appearing in 73% of confirmed cases according to clinical research from Virginia Tech’s medical education program. Unlike gradual breathlessness from conditions like COPD, PE-related dyspnea strikes suddenly and feels disproportionate to any physical activity. Patients consistently describe it as “drowning on dry land” or feeling like they cannot get enough air no matter how deeply they breathe. This acute onset occurs because blood clots abruptly obstruct pulmonary arteries, creating ventilation-perfusion mismatches where lung tissue receives oxygen but no blood flow to transport it. If you experience sudden, unexplained difficulty breathing—especially combined with any other symptom on this list—call 911 immediately.
2. Sharp Chest Pain That Worsens with Deep Breathing
Pleuritic chest pain affects 44% of lung embolism patients and distinguishes PE from cardiac conditions like heart attacks. This sharp, stabbing pain typically intensifies when you take deep breaths, cough, or bend over, indicating irritation of the pleura (lung lining) from distal emboli causing pulmonary infarction. The pain may feel localized to one side of your chest and can radiate to your shoulder or back. Unlike the crushing, radiating sensation of myocardial infarction, PE chest pain is sharp and breathing-dependent—a critical diagnostic clue for emergency physicians evaluating whether you need our Heart Rate Zone Calculator to monitor cardiovascular stress during recovery.
3-8. Additional Critical Warning Signs
Rapid or Irregular Heartbeat (Tachycardia): Heart rates exceeding 100 beats per minute occur in 44% of PE cases as your cardiovascular system compensates for reduced oxygen delivery. Tachycardia represents your body’s desperate attempt to maintain cardiac output despite obstructed pulmonary circulation.
Coughing Up Blood (Hemoptysis): Hemoptysis appears in 13-30% of lung embolism patients and signals pulmonary infarction where lung tissue dies from oxygen deprivation. Even small amounts of blood-tinged sputum demand immediate medical evaluation.
Lightheadedness or Fainting (Syncope): Sudden loss of consciousness occurs when massive blood clots dramatically reduce cardiac output, depriving your brain of oxygen. Syncope indicates hemodynamically unstable PE—a medical emergency requiring immediate thrombolytic therapy.
Leg Swelling or Pain (Deep Vein Thrombosis): Approximately 44% of PE patients exhibit leg symptoms because 90% of pulmonary emboli originate from deep vein thrombosis in the lower extremities. Unilateral calf pain, warmth, redness, or swelling suggests a DVT that could fragment and travel to your lungs.
Sudden Anxiety or Feeling of Doom: The rapid onset of dyspnea coupled with declining oxygen levels triggers profound anxiety that patients describe as an overwhelming sense of impending death—a psychological manifestation of your body recognizing life-threatening physiological crisis.
Clammy Skin and Profuse Sweating: Cold, clammy skin with excessive perspiration indicates shock as your cardiovascular system fails to maintain adequate blood pressure and tissue perfusion.
Lung Embolism vs Heart Attack: Know the Difference
| Symptom | Lung Embolism | Heart Attack |
|---|---|---|
| Chest Pain Type | Sharp, stabbing, worse with breathing | Crushing, pressure-like, radiating |
| Breathing Pattern | Severely impaired, sudden onset | May be normal in early stages |
| Symptom Onset | Abrupt, within seconds to minutes | Can be gradual or sudden |
| Leg Symptoms | Often present (DVT signs: swelling, warmth) | Rarely associated |
| Coughing Blood | Possible (hemoptysis) | Very rare |
| Response to Rest | No improvement | May temporarily improve |
What This Means For You: Don’t wait for multiple symptoms to appear before seeking help. Even ONE of these warning signs—particularly sudden shortness of breath, chest pain with breathing, or coughing up blood—warrants immediate emergency evaluation. Use our Symptom Checker to document your symptoms before calling 911, but never delay emergency care. In PE cases, the difference between survival and death is often measured in hours, not days.
Understanding Lung Embolism – Causes & Risk Factors
What Causes Lung Embolism? (The DVT-PE Connection)
How Blood Clots Travel to Your Lungs
The majority of lung embolism cases—approximately 90%—originate from deep vein thrombosis in the lower extremities, particularly in the deep veins of the thighs and calves according to research published by the National Institutes of Health. This pathophysiological journey begins when blood stasis, vessel wall injury, or hypercoagulability trigger clot formation in leg veins. Once these thrombi dislodge, they travel through progressively larger vessels—from the femoral vein into the inferior vena cava, through the right side of the heart, and ultimately lodge in pulmonary arteries where they obstruct blood flow to lung tissue.
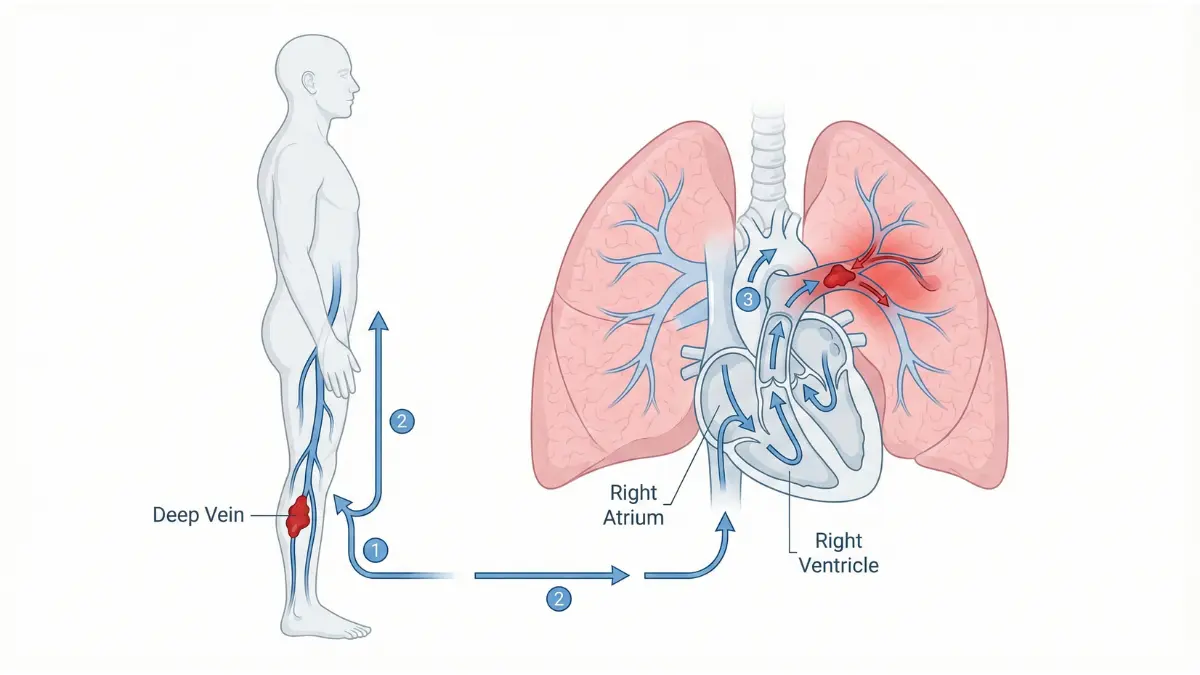
Large emboli can create a “saddle embolus” blocking the main pulmonary artery with devastating cardiovascular consequences, while smaller clots obstruct peripheral branches causing pulmonary infarction and the characteristic intra-alveolar hemorrhage that produces hemoptysis.
Most lung embolisms are preventable by addressing deep vein thrombosis risk factors before clots form—a critical insight that shifts the focus from treatment to proactive prevention strategies.
12 Major Risk Factors (Evidence-Ranked)
The Centers for Disease Control and Prevention emphasizes that while almost anyone can develop venous thromboembolism, certain factors substantially increase risk—and having multiple risk factors simultaneously compounds the danger exponentially.
High-Risk Category
- Prolonged Immobility: Extended bed rest, paralysis, or sitting for long periods (especially with crossed legs) impairs the calf muscle pump mechanism that promotes venous return, creating blood stasis that allows procoagulant factors to accumulate. The CDC’s travel guidelines note that flights or car trips exceeding four hours significantly elevate risk.
- Recent Major Surgery: Surgical procedures—particularly those involving the abdomen, pelvis, hips, or legs—cause both vascular injury and enforced immobility, creating the perfect storm for thrombosis formation. Healthcare-associated venous thromboembolism remains a leading preventable cause of hospital deaths.
- Active Cancer or Chemotherapy: Cancer patients face dramatically elevated blood clot risk due to tumor-induced hypercoagulability and central venous catheters, with CDC data showing that up to 50% of patients with long-term chemotherapy catheters develop DVT.
- Previous VTE History: Prior deep vein thrombosis or pulmonary embolism episodes indicate underlying thrombotic tendency and substantially increase recurrence probability.
- Inherited Clotting Disorders: Genetic mutations like Factor V Leiden and Prothrombin G20210A mutation create lifelong hypercoagulable states requiring vigilant monitoring.
Moderate-Risk Category
- Obesity: Individuals with BMI exceeding 30—which you can calculate using our BMI Calculator—experience increased venous pressure and inflammation that promote clot formation.
- Tobacco Smoking: Damages endothelial cells lining blood vessels while increasing coagulation factor levels
- Pregnancy and Postpartum Period: Elevated estrogen levels and increased blood volume create hypercoagulable states, with risk extending three months post-delivery
- Hormone Therapy and Birth Control Pills: Estrogen-containing contraceptives and hormone replacement therapy significantly elevate thrombosis risk
- Heart and Lung Disease: Chronic cardiovascular and pulmonary conditions impair circulation
- Age Over 60: Thrombosis risk increases progressively with advancing age
- COVID-19 Infection: Recent viral illnesses can trigger inflammatory coagulation cascades
Your Personal Risk Score
| Risk Factor | Points |
|---|---|
| Major surgery in last 3 months | 3 |
| Active cancer/chemotherapy | 3 |
| Previous DVT or PE | 3 |
| Immobility >3 days or recent travel >8 hours | 2 |
| Pregnancy or postpartum (<3 months) | 2 |
| Estrogen therapy or birth control pills | 2 |
| Obesity (BMI >30) | 1 |
| Smoking | 1 |
| Age >60 | 1 |
| Heart or lung disease | 1 |
Interpretation: Score 0-2 = Low risk | Score 3-4 = Moderate risk | Score ≥5 = High risk requiring preventive anticoagulation discussion
What This Means For You: Calculate your risk score now using factors above and our Body Fat Percentage Calculator for precise obesity assessment. If your score exceeds 4, schedule an appointment with your healthcare provider to discuss prophylactic anticoagulation before planned surgeries or long-distance travel. Prevention through risk modification prevents 70% of potentially fatal blood clots.
Life-Saving Diagnosis & Treatment Options
How Doctors Diagnose Lung Embolism (Speed Saves Lives)
Emergency Diagnostic Process (Timeline)
When you arrive at the emergency department with suspected pulmonary embolism, physicians initiate a systematic evaluation protocol where every minute counts toward improving survival outcomes.
0-15 Minutes: Clinical Assessment & Risk Stratification
Emergency physicians begin with pre-test probability scoring using validated tools like the Wells Score or Revised Geneva Score, which assign points based on clinical indicators including heart rate exceeding 100 beats per minute, recent surgery or immobilization, clinical signs of deep vein thrombosis, hemoptysis, active cancer, and whether alternative diagnoses seem less likely than PE. Low-risk patients (Wells score ≤4 points) may qualify for the Pulmonary Embolism Rule-Out Criteria (PERC), which can safely exclude PE without further testing if all eight criteria are negative.
15-30 Minutes: D-Dimer Blood Test
For non-high-risk patients, physicians order D-dimer testing—a highly sensitive biomarker (95% sensitivity) that detects fibrin degradation products released when blood clots dissolve. A negative D-dimer effectively rules out venous thromboembolism with post-test probability below 2%, allowing patients to avoid radiation exposure from imaging. However, recent research from the National Institutes of Health reveals D-dimer specificity is only 40-50%, meaning elevated levels require confirmatory imaging since many non-thrombotic conditions (pregnancy, recent surgery, cancer, age over 80) also elevate D-dimer.
30-60 Minutes: Computed Tomography Pulmonary Angiography (Gold Standard)
CTPA remains the definitive diagnostic imaging modality, visualizing blood clots as filling defects in contrast-enhanced pulmonary arteries with 83-90% sensitivity and over 95% specificity according to the landmark PIOPED-II study. Modern CT scanners detect even subsegmental emboli, and outcome studies confirm fewer than 2% of patients with negative CTPA develop PE within three months. For patients with contrast allergies or renal impairment, ventilation-perfusion (V/Q) scanning serves as an alternative diagnostic approach.
Treatment Arsenal: Evidence-Based Options
Immediate Treatment (First 24 Hours)
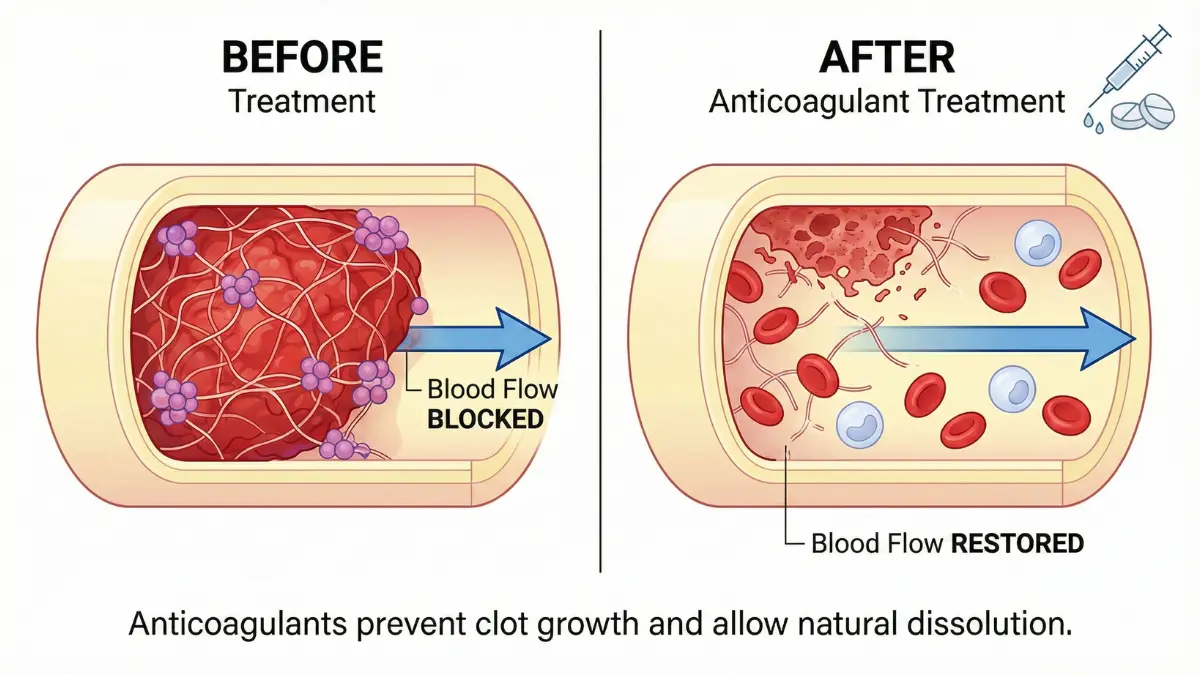
1. Anticoagulants (Blood Thinners) – First-Line Therapy
Anticoagulation prevents clot propagation while allowing the body’s natural fibrinolytic system to gradually dissolve existing thrombi. According to FDA-approved guidelines reviewed by the Veterans Affairs Department, direct oral anticoagulants (DOACs) have revolutionized lung embolism treatment with superior safety profiles compared to traditional warfarin.
Injectable Options: Unfractionated heparin (80 U/kg bolus, then 18 U/kg/hour infusion) or low-molecular-weight heparin like enoxaparin (1 mg/kg twice daily) provide rapid anticoagulation.
Oral DOACs: Rivaroxaban and apixaban require no heparin bridging, making them ideal for emergency department initiation—rivaroxaban starts at 15 mg twice daily for 21 days, then 20 mg daily, while apixaban begins at 10 mg twice daily for 7 days, then 5 mg twice daily. You can track your medication regimen using our Pill Identifier tool for accurate dosing verification.
Duration: Minimum 3 months for provoked PE, with many patients requiring 6-12 months or lifelong therapy depending on recurrence risk.
2. Thrombolytics (Clot-Busters) – For High-Risk Massive PE
When patients present with hemodynamic instability, hypotension, or massive pulmonary artery obstruction, systemic thrombolytic therapy can be life-saving. Research from Touro College’s medical program demonstrates that alteplase (tissue plasminogen activator) accelerates clot dissolution by converting fibrin-bound plasminogen into plasmin, which breaks apart fibrin molecules within the thrombus. The National Institutes of Health reports that standard alteplase dosing (100 mg over 2 hours) reduces pulmonary artery pressure by 30% and increases cardiac output by 15%.
Success Rate: 90% effectiveness in massive PE, but carries 2-3% major bleeding risk including intracranial hemorrhage. Low-dose alteplase protocols (0.6 mg/kg, maximum 50 mg over 2 hours) demonstrate comparable efficacy with improved safety profiles, particularly in elderly patients.
3. Surgical and Catheter-Based Interventions
- Catheter-directed thrombolysis: Delivers low-dose thrombolytics (10-20 mg t-PA over 12-24 hours) directly to pulmonary arteries, minimizing systemic bleeding risks
- Surgical embolectomy: Reserved for patients with contraindications to thrombolysis or failed medical therapy, with approximately 20% mortality in critically ill patients
- IVC filter placement: Prevents recurrent embolization in patients with contraindications to anticoagulation
Treatment Options Comparison
| Treatment | Best For | Success Rate | Duration | Major Risk |
|---|---|---|---|---|
| Anticoagulants (DOACs) | Stable, low-to-intermediate risk PE | 95% prevent propagation | 3-12+ months | Minor bleeding (3-5%) |
| Thrombolytics (Alteplase) | Massive PE with shock | 90% clot lysis | Single 2-hour infusion | Major bleeding (2-3%) |
| Catheter-Directed Therapy | Submassive PE, moderate risk | 85-90% | 12-24 hours | Reduced bleeding (<1%) |
| Surgical Embolectomy | Failed thrombolysis, contraindications | 80-85% | One-time procedure | Surgical complications (20%) |
Recovery Timeline & Survival Data
Week 1-2: Hospital monitoring with intravenous or subcutaneous anticoagulation, supplemental oxygen therapy if needed, and gradual mobilization to prevent deconditioning. Our Sleep Calculator can help optimize rest during this critical recovery phase.
Week 3-4: Transition to oral blood thinners, outpatient follow-up appointments, and increasing physical activity tolerance.
Month 2-3: Follow-up imaging to assess clot resolution, anticoagulation dose adjustments based on bleeding risk, and evaluation for underlying thrombophilia.
Month 6-12: Decision point for continuing or discontinuing anticoagulation therapy based on PE cause (provoked vs. unprovoked) and recurrence risk factors.
Survival Statistics
| Timeframe | Treated Patients | Untreated Patients |
|---|---|---|
| 7 Days | 95%+ survive | 41% mortality |
| 30 Days | 93% survive | 60%+ mortality |
| 1 Year | 85-90% survive | 75%+ mortality |
The dramatic difference between treated and untreated outcomes underscores why recognizing symptoms early and seeking emergency care immediately can mean the difference between full recovery and death.
What This Means For You: With immediate treatment initiated in the emergency department, your survival odds exceed 95%—but untreated lung embolism kills 60% of patients within the first week. If you’re experiencing sudden shortness of breath, chest pain with breathing, or any combination of the eight warning signs discussed earlier, call 911 without delay. Modern anticoagulant therapies allow many low-risk patients to recover at home after brief hospitalization, but only if treatment begins within hours of symptom onset. Monitor your cardiovascular health during recovery using our Heart Rate Zone Calculator to ensure safe physical activity levels.
Prevention Strategies & Living After Lung Embolism
Preventing Lung Embolism: Proven Strategies That Work
For High-Risk Individuals (Pre-Event Prevention)
Preventing blood clots before they form remains far more effective than treating established venous thromboembolism, with evidence-based strategies proven to reduce lung embolism risk by up to 70% in high-risk populations.
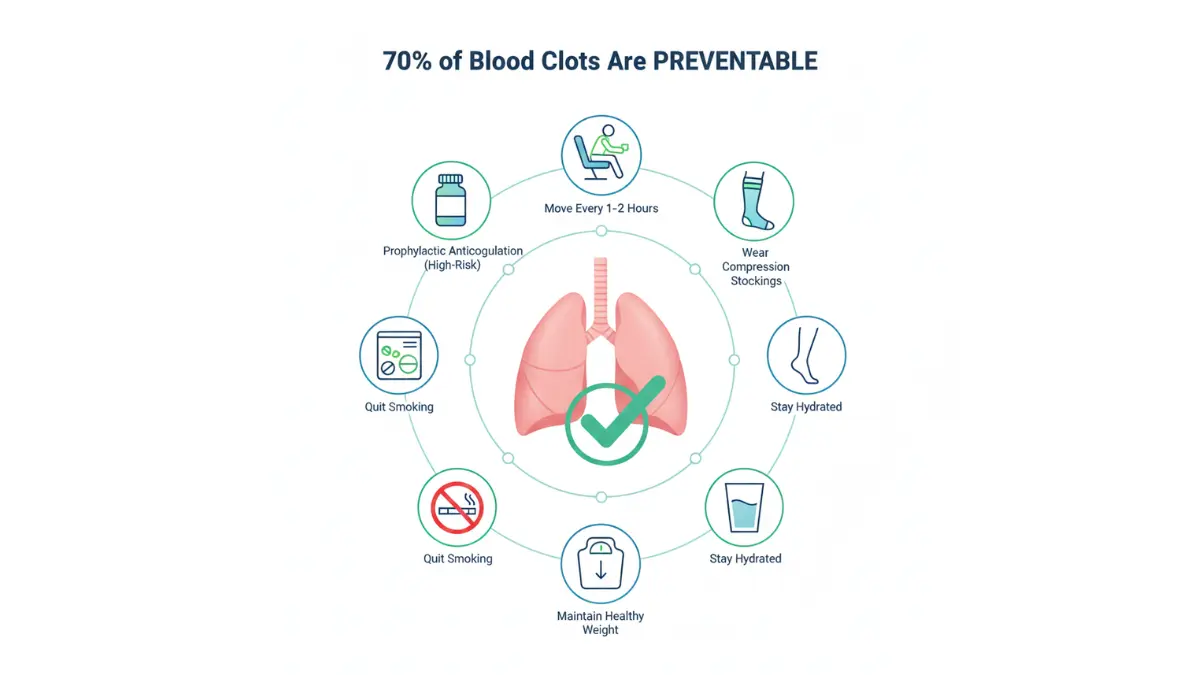
Travel Protection
The Centers for Disease Control and Prevention travel guidelines emphasize that air travel exceeding four hours significantly elevates deep vein thrombosis risk, with the longest flights (over 12 hours) tripling the odds of developing blood clots. Implement these protective measures during extended travel:
- Move legs and ankles every 1-2 hours to activate the calf muscle pump mechanism that promotes venous return and prevents blood stasis
- Graduated compression stockings (15-20 mmHg) reduce asymptomatic DVT in travelers by 90% according to Cochrane systematic reviews
- Stay adequately hydrated while avoiding alcohol and excessive caffeine, which promote dehydration and blood hyperviscosity
- Consider prophylactic anticoagulation for very high-risk travelers—discuss aspirin or low-molecular-weight heparin with your physician before departure
- Choose aisle seats to facilitate frequent movement without disturbing fellow passengers
Surgical Prevention
The CDC reports that healthcare-associated venous thromboembolism remains a leading preventable cause of hospital deaths, with up to 60% of VTE events occurring during or within 90 days of hospitalization. Essential surgical prophylaxis includes:
- Prophylactic anticoagulation starting pre-operatively and continuing post-discharge for high-risk surgeries
- Early mobilization protocols with physical therapy beginning within 24 hours post-surgery
- Sequential compression devices that mechanically compress leg veins during immobility periods
Lifestyle Modifications
- Weight management: Maintaining a healthy BMI below 30 reduces thrombosis risk—use our BMI Calculator to assess your current status and our Weight Loss Calculator for realistic goal-setting
- Smoking cessation: Tobacco damages vascular endothelium and increases coagulation factor levels
- Regular physical activity: Exercise improves venous circulation; track safe training zones with our Heart Rate Zone Calculator
- Medication review: Discuss alternatives to estrogen-containing contraceptives and hormone replacement therapy with your doctor if you have multiple risk factors
Life After Lung Embolism: Your New Normal
Long-Term Anticoagulation Management
Research from the National Institutes of Health demonstrates that extended anticoagulation therapy beyond the standard 3-month primary phase significantly reduces recurrence rates, with studies showing continued benefit for 2-4 years in selected patients. Critical management considerations include:
- Daily medication adherence is paramount—missing even a few doses increases recurrence risk
- Regular monitoring: INR checks for warfarin users, annual kidney function tests for DOAC users
- Bleeding risk management: Avoid NSAIDs (ibuprofen, naproxen), use soft toothbrushes, wear protective equipment during activities
- Dietary considerations: Maintain consistent Vitamin K intake if taking warfarin (found in leafy greens)
Our Pill Identifier tool helps verify correct anticoagulant dosing and prevent medication errors.
Physical Activity Guidelines
Months 1-3: Begin with light walking (10-15 minutes twice daily), avoiding straining or heavy lifting over 10 pounds
Months 4-6: Gradually increase aerobic activity to 30 minutes daily; introduce resistance training with medical clearance
Months 6+: Most activities become safe with physician approval—calculate appropriate exercise intensity using our Calorie Deficit Calculator for weight management goals
Return to Work and Travel
- Desk-based jobs: Most patients return within 2-4 weeks
- Physical labor positions: Expect 2-3 months recovery time for demanding work
- Air travel: Wait minimum 2 weeks post-diagnosis; always wear compression stockings and follow CDC travel precautions
Monitoring for Complications
Post-Thrombotic Syndrome (PTS): Affects 20-50% of DVT patients, causing chronic leg pain, swelling, and skin changes due to venous valve damage
Chronic Thromboembolic Pulmonary Hypertension (CTEPH): Rare but serious complication (0.5-4% of PE survivors) where residual clots cause persistent pulmonary artery obstruction and heart strain
Mental health impact: Up to 30% of survivors experience anxiety, PTSD, or depression—consider our Sleep Calculator to address rest disturbances common in recovery
Quality of Life Recovery Timeline
| Timeframe | % Returned to Normal Activities | Common Limitations |
|---|---|---|
| 3 Months | 60% | Fatigue, mild shortness of breath with exertion |
| 6 Months | 75% | Reduced stamina, occasional chest discomfort |
| 1 Year | 85-90% | Minimal impairment in most survivors |
⚡ What This Means For You: Most lung embolism survivors return to full, active lives within one year, but lifelong vigilance about clot prevention remains essential. Calculate your ongoing risk using our Health Tools and implement the prevention strategies above. If you’re traveling, undergoing surgery, or experiencing prolonged immobility, proactively discuss prophylactic anticoagulation with your healthcare provider. Remember: the best treatment for pulmonary embolism is preventing it from happening in the first place.
When to Seek Help + Expert Insights
Emergency Action Plan: When Every Second Counts
Call 911 Immediately If You Experience:
Recognizing life-threatening symptoms and acting within minutes separates survivors from fatalities when lung embolism strikes. The Centers for Disease Control and Prevention emphasizes that difficulty breathing combined with chest pain demands immediate emergency services.
- Sudden severe shortness of breath that prevents speaking in complete sentences
- Chest pain combined with difficulty breathing, especially if sharp and worse with inhalation
- Coughing up blood (hemoptysis) of any amount
- Loss of consciousness or severe lightheadedness indicating hemodynamic instability
- Blue-tinged lips or fingertips (cyanosis) showing critical oxygen deprivation
Emergency Room Strategy
When you arrive at the emergency department, immediately state “I’m concerned about pulmonary embolism” to prioritize triage. According to guidelines from the University of Alabama Birmingham’s medical program, prompt recognition enables initiation of therapeutic anticoagulation within the first hour. Provide complete information about:
- All risk factors (recent surgery, long flights, cancer, birth control pills)
- Current medications, particularly hormonal therapies
- Family history of blood clots or clotting disorders
- Recent immobilization or leg symptoms
Use our Symptom Checker to document timeline and severity before calling 911, but never delay emergency care.
Global Expert Consensus
The American College of Chest Physicians (CHEST) guidelines, representing international expert consensus, recommend systemic thrombolytic therapy for pulmonary embolism patients with hypotension (Grade 2B recommendation), with direct oral anticoagulants preferred over traditional warfarin for long-term management. Research from the National Institutes of Health confirms that prompt recognition and interprofessional management significantly reduce the high mortality and morbidity rates associated with untreated lung embolism.
Key Takeaways
- Lung embolism kills 60,000-100,000 Americans yearly but achieves 95%+ survival with rapid treatment
- Eight warning signs—especially sudden breathlessness, pleuritic chest pain, or hemoptysis—demand immediate 911 calls
- Most cases originate from preventable leg clots (DVT) through prolonged immobility, surgery, or hormonal medications
- Anticoagulants for 3-12 months prevent recurrence; some patients require lifelong therapy based on risk stratification
- Prevention strategies—mobility during travel, compression stockings, weight management, smoking cessation—reduce risk by 70%
Medical Disclaimer
This article is for educational purposes only, not medical advice. Always consult qualified healthcare providers for diagnosis and treatment of lung embolism or any medical condition. If experiencing symptoms described above, seek emergency care immediately by calling 911. Information presented reflects current medical evidence but cannot substitute for personalized clinical evaluation. Visit our Health Tips section and Main Website for additional evidence-based resources.
Frequently Asked Questions (FAQs) About Lung Embolism
1. What is lung embolism?
Lung embolism (pulmonary embolism) is a life-threatening condition where a blood clot blocks one or more arteries in the lungs, cutting off oxygen supply to lung tissue. Most clots originate from deep veins in the legs.
2. How fatal is lung embolism?
Untreated lung embolism kills 60-100,000 Americans yearly with 60% mortality within a week. However, with immediate treatment, survival rates exceed 95%, making early recognition critical.
3. What are the main warning signs?
The most common symptoms include sudden shortness of breath (73% of cases), sharp chest pain that worsens with breathing, rapid heartbeat, coughing up blood, lightheadedness, leg swelling, and unexplained anxiety.
4. What causes blood clots to form?
Risk factors include prolonged immobility (long flights, bed rest), recent surgery, active cancer, pregnancy, birth control pills, obesity, smoking, age over 60, and inherited clotting disorders that increase blood coagulation.
5. How is lung embolism diagnosed?
Doctors use D-dimer blood tests (95% sensitivity), CT pulmonary angiography (gold standard imaging), Wells Score risk assessment, and sometimes V/Q scans or ultrasound to confirm diagnosis within 30-60 minutes.
6. What is the main treatment?
Anticoagulants (blood thinners) like rivaroxaban, apixaban, or heparin are first-line treatment for 3-12 months. Massive PE may require thrombolytic “clot-buster” medications or surgical removal.
7. How long does recovery take?
Most patients return to normal activities within 3-6 months, with 85-90% fully recovered by one year. Initial hospital stay lasts 1-2 weeks, followed by gradual activity increases under medical supervision.
8. Can lung embolism be prevented?
Yes—70% of cases are preventable through leg movement during travel, wearing compression stockings, maintaining healthy weight, staying hydrated, avoiding prolonged immobility, and prophylactic anticoagulation for high-risk situations.
9. Will I have another blood clot?
Recurrence risk depends on the cause—provoked PE (from surgery/injury) has 3-5% recurrence, while unprovoked PE has 10-30% risk within 5 years, often requiring extended anticoagulation therapy.
10. When should I call 911?
Immediately call emergency services for sudden severe breathlessness, chest pain with breathing difficulty, coughing blood, fainting, or blue-tinged lips—these indicate life-threatening PE requiring urgent intervention.
11. Can you survive without treatment?
No—untreated lung embolism is fatal in approximately 30% of cases within 30 days, with mortality exceeding 60% within the first week. Treatment reduces death risk to under 5%, making immediate medical care absolutely essential.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.