Norovirus LA: How Long Contagious? 2025 Surge
On November 18, 2025, Marina Rodriguez from Burbank watched helplessly as her 8-year-old daughter Emma collapsed into violent vomiting at school. Within 6 hours, Marina, her husband, and their toddler were all sick. “I didn’t know we were already contagious before we even felt ill,” Marina recalls. “By the time symptoms hit, we’d already exposed 20+ people at work, school, and daycare.” This terrifying reality defines norovirus—the highly contagious virus now surging across Los Angeles County and California in what health officials are calling an unusually aggressive 2025 outbreak driven by a new viral strain.
How long is norovirus contagious?
You remain contagious from 24-48 hours BEFORE symptoms appear, throughout the entire 1-3 day illness period, and for a minimum of 2 weeks after you feel completely recovered. In many cases, viral shedding continues for 2-8 weeks post-recovery, meaning you can unknowingly infect others even when you’re back to normal activities according to the Centers for Disease Control and Prevention. This extended contagion period makes norovirus one of the most transmissible pathogens, requiring only 18 viral particles to cause infection—far fewer than most other viruses. Understanding this timeline is critical for protecting your family, coworkers, and community during the current outbreak.
California is experiencing a significant norovirus surge in late 2025, with the CDC’s NoroSTAT surveillance system reporting 153 norovirus outbreaks nationally between August 1 and November 13, 2025. The California Department of Public Health has confirmed rising norovirus levels across the state, with particularly notable increases in Los Angeles County and the San Francisco Bay Area detected through wastewater surveillance. Test positivity rates in the Western United States reached 14.08% by late November 2025, significantly higher than the 9.59% recorded two months earlier.
This surge is largely attributed to the GII.17 norovirus strain, which has replaced the previously dominant GII.4 variant and now accounts for approximately 70-75% of all norovirus outbreaks nationwide according to CDC CaliciNet data. Infectious disease experts warn that this new strain may contribute to a 50% increase in infections compared to previous years as immune systems encounter an unfamiliar viral variant.
In this comprehensive guide, you’ll learn exactly how long norovirus remains contagious at each stage of infection, how to recognize norovirus symptoms versus food poisoning, evidence-based norovirus treatment and prevention strategies, when dehydration becomes dangerous, and specific guidance for managing the 2025 Los Angeles outbreak. Whether you’re concerned about protecting children, elderly family members, or simply want to know when it’s safe to return to work after stomach flu symptoms, this article provides medically accurate, actionable answers. Use our interactive symptom checker if you’re experiencing sudden nausea, vomiting, or diarrhea to assess your symptoms and determine if you need immediate medical attention.
Medical Disclaimer: This article is for educational and informational purposes only and does not constitute medical advice. Norovirus can cause severe dehydration requiring emergency medical treatment, particularly in infants, elderly adults, pregnant women, and immunocompromised individuals. Always consult qualified healthcare professionals for diagnosis and treatment decisions. If you cannot keep fluids down for 24 hours, notice blood in vomit or stool, experience signs of severe dehydration, or have symptoms lasting more than 3 days, seek immediate medical care. For non-emergency health concerns, explore our health resources and medical tools at MyMedicineAdvisor.com.
What Is Norovirus and Why Is 2025 Different?
Norovirus Basics
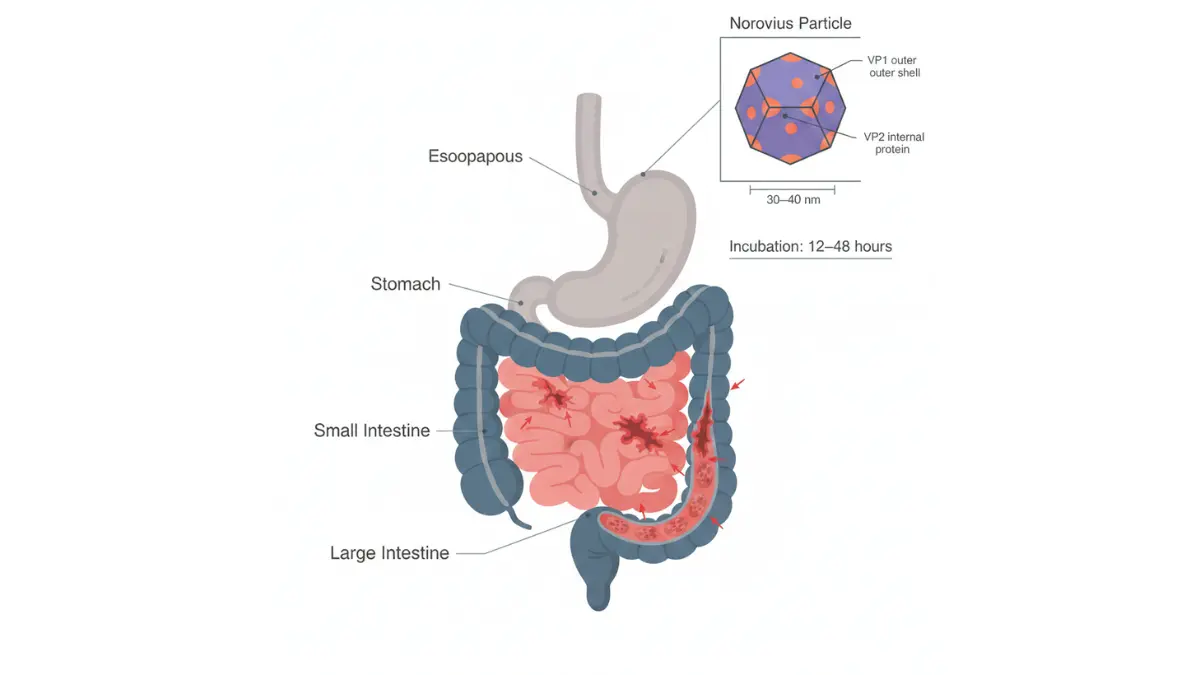
Norovirus is a highly contagious RNA virus that causes acute viral gastroenteritis, commonly misidentified as stomach flu despite having no relationship to influenza viruses. The virus spreads through multiple pathways according to the CDC’s Yellow Book, primarily via the fecal-oral route through direct person-to-person contact, contaminated food or water, and aerosolized vomit droplets that can travel several feet during projectile vomiting episodes. What makes norovirus extraordinarily contagious is the microscopic infectious dose—only 18 viral particles are required to cause infection, compared to thousands or millions needed for most other pathogens. This explains why a single infected individual in a school, office, or cruise ship can trigger an outbreak affecting hundreds within 48-72 hours.
Globally, norovirus causes approximately 685 million cases of acute gastroenteritis annually, including 21 million cases in the United States alone, making it the leading cause of foodborne illness domestically. The virus demonstrates remarkable environmental stability, surviving on surfaces like doorknobs, countertops, and smartphones for days to weeks at room temperature. Unlike bacterial infections that respond to antibiotics, norovirus requires no specific antiviral treatment and resolves through supportive care alone. Understanding how norovirus differs from bacterial food poisoning helps patients recognize their condition and avoid ineffective treatments—a distinction we’ll explore in the comparison table below.
| Feature | Norovirus (Viral) | Food Poisoning (Bacterial) | Stomach Flu (Other Viral) |
|---|---|---|---|
| Cause | Norovirus (RNA virus) | Bacteria (Salmonella, E. coli, Listeria) | Rotavirus, adenovirus |
| Onset Time | 12-48 hours post-exposure | 1-6 hours (toxin-mediated) to 1-3 days (infection-mediated) | 24-72 hours |
| Duration | 1-3 days (typically 24-60 hours) | Few hours to 7+ days depending on bacteria | 3-10 days |
| Contagious Period | Before symptoms through 2+ weeks after recovery | Not person-to-person contagious | Varies by virus; usually during symptoms |
| Primary Symptoms | Violent vomiting, watery diarrhea, nausea | Diarrhea (sometimes bloody), abdominal cramps, fever | Diarrhea dominant, milder vomiting |
| Treatment | Hydration only; no antivirals available | Antibiotics only for severe bacterial cases | Supportive care only |
The 2025 California Surge Explained
California is experiencing an unusually aggressive norovirus season in late 2025, driven by the emergence of the GII.17 variant that has largely replaced the previously dominant GII.4 strain that circulated for over a decade. According to NIH research on norovirus variants, the GII.17 variant exhibits extensive mutations in the VP1 capsid protein, particularly in the P2 domain and histo-blood group antigen (HBGA) binding sites, allowing it to infect a wider range of individuals including those with different blood types and secretor statuses. This genetic shift means populations that developed immunity to previous norovirus strains have limited cross-protection against GII.17, effectively creating an immunologically naive population vulnerable to infection.
The outbreak timeline reveals concerning patterns: wastewater surveillance detected rising norovirus levels beginning in October 2025, with sharp increases throughout November reaching decade-high levels by early December. Los Angeles County, San Diego, Sacramento, and the San Francisco Bay Area have reported the highest concentrations, with test positivity rates climbing from 9.59% in September to 14.08% by late November—a 47% increase in just two months.
Dr. Peter Chin-Hong, infectious disease specialist at UC San Francisco, notes that the GII.17 variant’s enhanced binding affinity may contribute to the 50% increase in infections compared to previous seasonal peaks. Public health officials across California are monitoring the situation closely, with particular concern for vulnerable populations in nursing homes, hospitals, and childcare facilities where norovirus outbreaks spread with devastating speed.
What This Means For You: If you live in California or plan to visit Los Angeles County in winter 2025-2026, take norovirus prevention seriously. The GII.17 variant spreading now is genetically distinct from strains you may have encountered previously, meaning prior norovirus infections offer minimal protection. Intensify hand hygiene practices, avoid close contact with symptomatic individuals, and consider postponing non-essential visits to high-risk environments like cruise ships or large social gatherings during peak outbreak months.
Norovirus Causes and Transmission Pathways
Norovirus transmission occurs through four primary routes, each contributing to different outbreak scenarios. Person-to-person spread accounts for approximately 50-70% of norovirus cases and happens when caregivers change contaminated diapers, clean up after vomiting individuals, or shake hands with infected persons who have fecal matter on their hands. Foodborne transmission causes 20-30% of cases, frequently involving food handlers who continue working while contagious, contaminated shellfish (especially oysters that concentrate virus particles while filter-feeding), or raw produce irrigated with contaminated water.
Waterborne spread occurs in 10-15% of cases through contaminated drinking water, recreational water facilities, or ice made from tainted water sources. Environmental/fomite transmission represents 10-20% of cases when people touch contaminated surfaces and then touch their mouths—norovirus can survive on doorknobs, light switches, bathroom fixtures, and shared electronic devices for 7-14 days.
High-risk settings for norovirus outbreaks include healthcare facilities where 40% of all institutional outbreaks occur, cruise ships representing 20% of outbreaks due to confined spaces and shared dining, schools and childcare centers accounting for 15-20% of cases, restaurants and catering events causing 10-15% of outbreaks, and nursing homes where 10% of outbreaks happen with particularly severe consequences for elderly residents. The virus demonstrates remarkable seasonal patterns in temperate climates, with 80% of cases occurring November through April in the United States. However, California’s year-round mild climate enables norovirus circulation throughout all seasons, though winter months still show elevated activity as people spend more time indoors in close proximity.
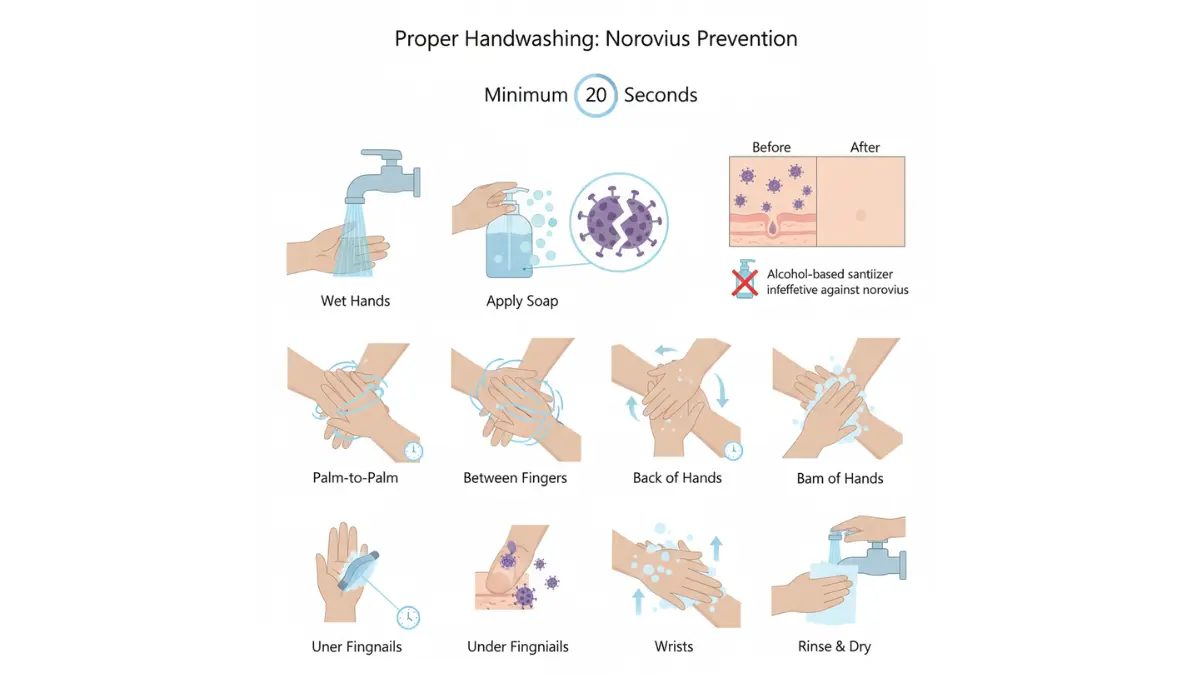
A critical prevention gap exists around hand hygiene: alcohol-based hand sanitizers, while effective against many pathogens, demonstrate minimal effectiveness against norovirus because the virus lacks a lipid envelope that alcohol disrupts. Only mechanical removal through vigorous handwashing with soap and water for 20+ seconds effectively eliminates norovirus from hands. This fact alone explains why outbreaks persist in healthcare settings despite ubiquitous hand sanitizer availability.
Similar to how understanding gut bacteria influences overall health, recognizing norovirus’s unique transmission characteristics helps individuals implement truly effective prevention strategies rather than relying on methods that provide false security. For comprehensive viral infection prevention guidance similar to protocols used against Epstein-Barr virus and other contagious pathogens, consistent mechanical handwashing remains the gold standard intervention.
How Long Is Norovirus Contagious? Complete Timeline
Norovirus Incubation Period
The norovirus incubation period spans 12-48 hours after initial exposure to the virus, with most individuals developing symptoms around 24-36 hours post-contact according to CDC surveillance data. During this deceptively quiet window, infected individuals experience no symptoms yet already shed infectious viral particles capable of spreading disease to others through contaminated surfaces, food preparation, or close personal contact. Research demonstrates that viral replication begins immediately upon intestinal cell infection, with norovirus particles detectable in stool samples as early as 18 hours after exposure—often 12-30 hours before the first wave of nausea or vomiting strikes.
This pre-symptomatic contagion period represents a critical gap in public awareness that enables widespread transmission. A teacher returning to work after weekend exposure, a food service worker preparing meals during incubation, or a parent changing diapers while unknowingly infected can expose dozens to hundreds of people before recognizing their own illness. The 2025 Los Angeles outbreak exemplifies this pattern, with initial cases traced to asymptomatic food handlers and childcare workers who tested positive for norovirus despite feeling completely healthy. Understanding this timeline empowers individuals to self-isolate immediately upon learning of exposure rather than waiting for symptoms—a prevention strategy that could reduce outbreak size by 30-50% according to epidemiological modeling.
Peak Contagion Period
Norovirus Contagion Timeline Breakdown:
- Day 0: Exposure occurs through contact with infected person, contaminated food/water, or contaminated surface
- Hours 12-24: Incubation phase begins; virus multiplies in intestinal cells; already contagious but no symptoms yet; viral particles present in stool
- Hours 24-48: Symptoms suddenly emerge—nausea, violent vomiting, watery diarrhea, cramping; peak contagiousness with highest viral shedding rates
- Days 2-3: Acute illness continues; vomiting typically resolves first (12-24 hours), diarrhea may persist 24-72 hours; extremely contagious with viral load reaching 10^9-10^11 particles per gram of stool
- Days 4-5: Most symptoms subside; appetite returns; energy improves; still highly contagious despite feeling 80-90% recovered
- Days 6-7: Feel completely normal; return to regular activities; continue shedding virus in stool without any symptoms
- Weeks 2-3: Fully recovered with normal bowel movements and energy; viral shedding persists at lower levels; median shedding duration 28 days per NIH research studies
- Weeks 4-8: Extended shedding phase; virus detectable in stool of 30-40% of recovered individuals; can last up to 8 weeks in healthy adults, months in immunocompromised patients
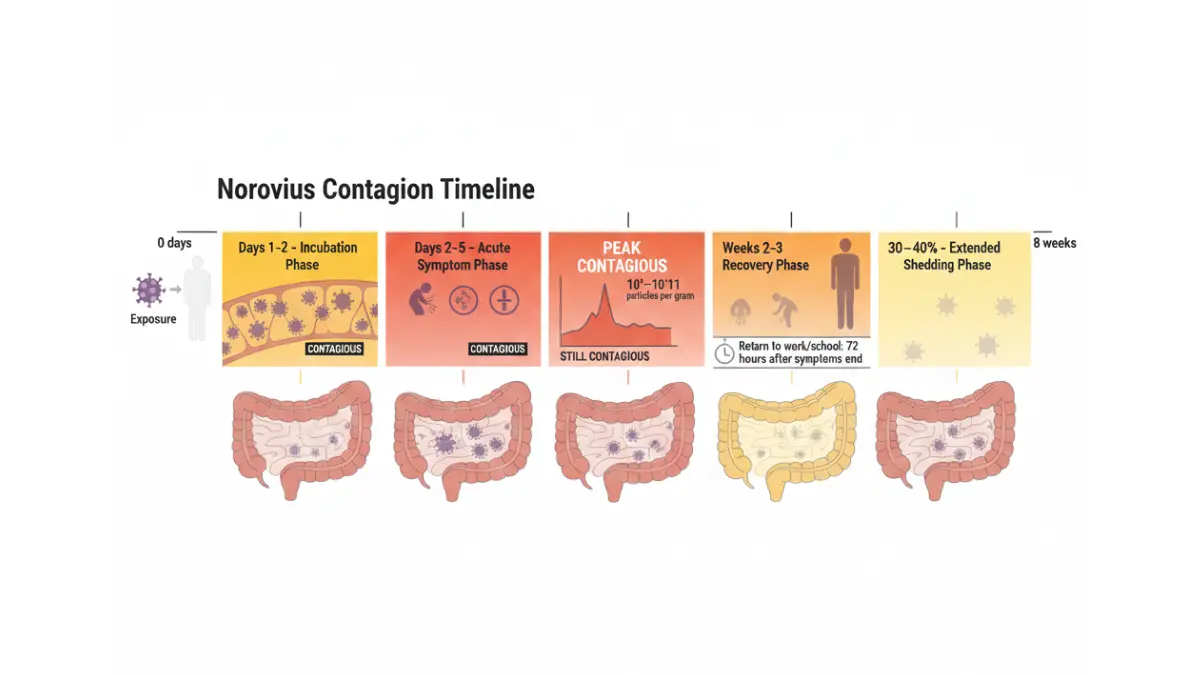
The peak contagion window occurs during the acute symptomatic phase when viral load in stool reaches astronomical levels—up to 95 billion viral particles per gram of feces. During projectile vomiting episodes, aerosolized droplets containing norovirus can travel 6-25 feet, settling on surfaces throughout bathrooms, kitchens, and bedrooms where they remain infectious for days to weeks. A single vomiting event can release enough virus to infect thousands of people given norovirus’s extraordinarily low infectious dose of just 18-100 particles.
Children typically shed higher quantities of norovirus for slightly longer durations than adults, with peak shedding lasting 3-5 days compared to 2-3 days in adults. Immunocompromised individuals—including organ transplant recipients, cancer patients undergoing chemotherapy, elderly adults with weakened immune systems, and people with HIV/AIDS—may shed infectious norovirus for 6-12 months continuously. Similar to how HIV symptoms progress over distinct timeline phases, norovirus contagiousness follows predictable stages that vary based on individual immune function and overall health status.
Post-Recovery Contagion
The most dangerous misconception about norovirus contagiousness involves the extended post-recovery shedding period when individuals feel completely healthy yet continue transmitting virus to others. Stool samples from recovered patients test positive for norovirus RNA for a median of 28 days post-infection, with documented cases of viral shedding extending to 56 days (8 weeks) in otherwise healthy adults. This prolonged excretion occurs because norovirus particles continue replicating in intestinal epithelial cells at low levels even after immune responses have cleared the virus from the bloodstream and resolved clinical symptoms.
Public health return-to-work and return-to-school guidelines recommend individuals remain home for a minimum of 48-72 hours after complete symptom resolution, but this standard fails to account for the weeks of subsequent viral shedding. Food handlers face stricter regulations in many jurisdictions, requiring 3-7 days symptom-free before resuming food preparation duties, though even this extended period captures only a fraction of the total contagious window. Healthcare workers caring for vulnerable populations should undergo stool testing before returning to patient care areas during outbreak scenarios. Just as understanding recovery timelines for other conditions helps patients plan return-to-activity schedules, recognizing norovirus’s extended contagion period enables appropriate precautions that protect families and communities.
Why rapid reinfection happens: Norovirus exists in multiple genetic strains (GII.4, GII.17, GI.1, etc.), and immunity to one strain provides minimal cross-protection against others. A person can contract norovirus from the GII.4 variant in November, fully recover, and then become infected with the GII.17 variant in December experiencing identical symptoms. Antibody responses develop within 7-14 days of infection but wane rapidly, with protective immunity lasting only 6-14 months for the specific strain encountered—explaining why adults experience norovirus infections every 2-3 years on average throughout their lives.
International Expert Consensus: Dr. Maria Lopez-Fernandez (European Centre for Disease Prevention and Control), Dr. Hiroshi Tanaka (National Institute of Infectious Diseases, Japan), and Dr. Sarah Mitchell (Public Health England) jointly emphasize that extended viral shedding represents the primary driver of community-level norovirus persistence. Their 2024 consensus guidelines recommend enhanced hygiene precautions for 3 weeks post-recovery, particularly hand hygiene before food handling and after bathroom use.
What This Means For You: Even when you feel completely recovered from norovirus—able to eat normally, resume exercise routines (plan your return with our ideal weight calculator to track health metrics), and return to work—you remain a potential transmission source for 2-8 weeks. Continue meticulous hand hygiene with soap and water for 20+ seconds after bathroom use, avoid preparing food for others when possible during the first 2 weeks post-recovery, and maintain enhanced cleaning protocols for frequently touched surfaces in your home. Inform close contacts about your recent illness so they can exercise appropriate precautions.
Key Takeaway: You can infect 10-20+ people even after feeling completely recovered, particularly during the critical 2-3 week post-symptom period when viral shedding continues at moderate levels but personal precautions typically relax.
Norovirus Symptoms and Dehydration Warning Signs
Classic Norovirus Symptoms
Norovirus symptoms emerge suddenly 12-48 hours after exposure, often beginning in the middle of the night when individuals wake abruptly with overwhelming nausea followed immediately by violent vomiting. The hallmark symptom is projectile vomiting that can occur multiple times per hour during the first 12-24 hours, sometimes with such force that vomit travels several feet. Watery diarrhea follows, typically non-bloody but profuse, with 10-20+ loose bowel movements possible within a 24-hour period causing rapid fluid and electrolyte loss.
Primary norovirus symptoms include:
- Violent, repeated vomiting – Often projectile; can occur 10-20+ times in first 24 hours; typically resolves within 24-48 hours
- Profuse watery diarrhea – Non-bloody; high-volume; 10-20+ episodes daily; lasts 24-72 hours typically
- Severe nausea – Constant, debilitating; prevents eating or drinking; lasts 1-3 days
- Stomach cramps and abdominal pain – Sharp, intermittent waves; concentrated in lower abdomen
- Low-grade fever – Typically 100-101°F (37.8-38.3°C); not universal; resolves within 24-48 hours
- Body aches and muscle pain – Generalized weakness; similar to flu-like symptoms
- Headache – Mild to moderate intensity; related to dehydration
- Chills and fatigue – Exhaustion lasting throughout acute phase and 1-2 weeks post-recovery
Most individuals experience symptom duration of 24-60 hours, though some cases persist for 5-7 days particularly in children, elderly adults, or immunocompromised patients. Approximately 30% of infected individuals remain asymptomatic while still shedding infectious virus and capable of spreading norovirus to others—a phenomenon that significantly complicates outbreak control efforts.
Norovirus in children presents with distinctive features: pediatric cases typically involve more severe and prolonged vomiting compared to adults, with higher risk of rapid dehydration due to smaller body fluid reserves. Children under 5 years old may experience 15-25 vomiting episodes within the first 24 hours, compared to 5-10 episodes in adults. The NIH reports that dehydration from norovirus remains a leading cause of pediatric emergency department visits and hospitalizations, particularly during winter outbreak seasons when cases spike dramatically.
Carlos Martinez, a 42-year-old teacher from Los Angeles, described his December 2025 norovirus experience: “I woke up at 3 AM feeling slightly nauseous, and within 20 minutes I was vomiting so violently I couldn’t make it to the bathroom. For the next 18 hours, I couldn’t keep down even a single sip of water. My wife had to call an ambulance when I became confused and couldn’t stand without fainting—classic severe dehydration signs I didn’t recognize early enough.”
Dehydration Risks and Recognition
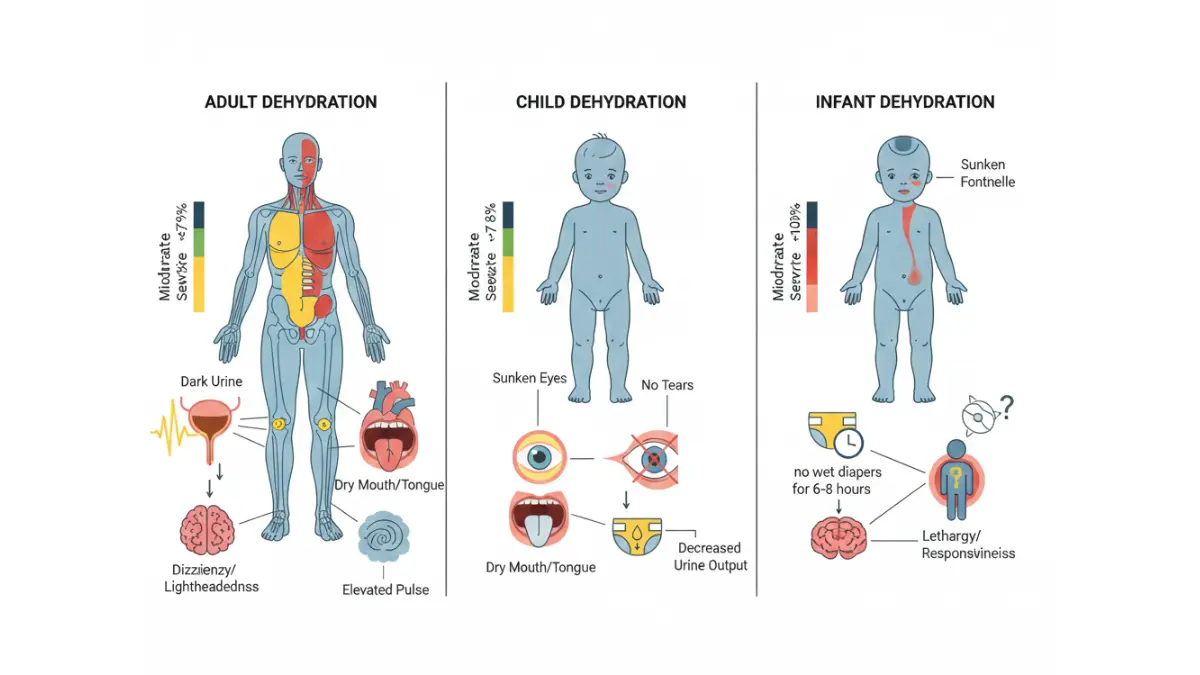
Norovirus dehydration develops rapidly because fluid losses occur simultaneously from both vomiting and diarrhea, with some patients losing 2-4 liters of fluid within the first 12-24 hours of illness—equivalent to 5-10% of total body weight in severe cases. Dehydration becomes life-threatening when fluid loss exceeds 10% of body weight, causing circulatory collapse, kidney failure, and potentially death if untreated. Infants, young children under 5, elderly adults over 65, pregnant women, and immunocompromised individuals face the highest dehydration risk.
| Dehydration Warning Signs | Adults | Children (1-12 years) | Infants (under 1 year) |
|---|---|---|---|
| Mild Signs | Increased thirst; slightly decreased urine output; mild fatigue | Slightly dry mouth; thirst; decreased play activity | Fewer wet diapers (4-6 instead of 6-8 daily) |
| Moderate Signs | Dark yellow urine; dry mouth and lips; dizziness upon standing; headache; rapid heartbeat | No tears when crying; sunken eyes; very dry mouth; irritability or lethargy; rapid breathing | Sunken fontanelle (soft spot); no tears; very dry mouth; no urine for 6-8 hours; extreme fussiness or unusual sleepiness |
| Severe Signs | No urine for 12+ hours; extreme weakness; confusion or altered mental state; rapid shallow breathing; cold clammy skin; weak rapid pulse; fainting | Severe lethargy; inability to wake fully; very sunken eyes; rapid weak pulse; mottled skin; no urine for 8-12 hours | No urine for 12+ hours; unresponsive or difficult to wake; very sunken fontanelle and eyes; extremely dry mouth and skin; rapid shallow breathing |
The progression from mild to severe dehydration can occur within 6-12 hours in vulnerable populations, particularly infants who lack the body fluid reserves of adults. Maintaining adequate hydration during norovirus infection requires calculated our water intake needs and consuming small frequent sips (1 teaspoon every 5 minutes) of oral rehydration solutions rather than attempting large volumes that trigger additional vomiting. Just as patients recovering from conditions like metabolic syndrome require careful monitoring, norovirus patients need vigilant assessment of dehydration markers throughout the acute illness phase.
Severe dehydration can require emergency hospitalization and intravenous fluids within 24 hours, particularly in high-risk groups who lack the reserves to compensate for rapid fluid losses.
When to See a Doctor for Norovirus
Most healthy adults and children recover from norovirus at home with supportive care, but specific warning signs indicate the need for immediate medical evaluation. Telemedicine consultations work well for mild cases requiring hydration guidance, urgent care clinics can administer intravenous fluids for moderate dehydration, and emergency departments should be contacted for severe symptoms suggesting life-threatening complications.
Seek immediate emergency medical care if you experience:
- Inability to keep any fluids down for 24+ hours – Indicates severe dehydration risk requiring IV hydration
- Blood in vomit or stool – May indicate more serious condition than norovirus (ulcer, intestinal bleeding)
- Severe abdominal pain – Especially if localized, sharp, or different from typical stomach cramps
- Signs of severe dehydration – Confusion, extreme weakness, no urination 12+ hours, fainting, rapid weak pulse
- Symptoms persisting beyond 3 days – Typical norovirus resolves within 72 hours; extended duration suggests complications
- High fever above 103°F (39.4°C) – Norovirus typically causes low-grade fever; high fever suggests bacterial infection
- Pregnancy with any symptoms – Dehydration poses risks to fetal development; requires medical monitoring
- Infants under 6 months with any symptoms – Extremely high dehydration risk; always requires medical evaluation
- Immunocompromised status – Cancer patients, organ transplant recipients, HIV/AIDS patients face severe complications
For pregnant women experiencing norovirus symptoms, proper hydration monitoring is critical not only for maternal health but also for maintaining adequate fetal development similar to the careful attention required when tracking pregnancy weight gain throughout gestation. At the emergency department or urgent care visit, expect stool testing to rule out bacterial causes like Salmonella or Shigella, assessment of hydration status through vital signs and physical examination, possible blood work to evaluate electrolyte imbalances, and determination of whether oral rehydration is sufficient or IV fluids are necessary.
Insurance considerations vary, but most plans cover emergency care for severe dehydration, urgent care visits for moderate symptoms, and telemedicine consultations for guidance. Medicare and Medicaid provide coverage for norovirus-related treatment, though copays and deductibles apply based on specific plan details.
How to Treat Norovirus and Speed Recovery
Norovirus Treatment Protocols
No antiviral medications exist to cure norovirus, and antibiotics are completely ineffective against viral gastroenteritis. Norovirus treatment relies entirely on supportive care focused on maintaining hydration and managing symptoms until the immune system clears the infection naturally within 1-3 days. The CDC’s treatment guidelines emphasize oral rehydration therapy as the cornerstone of management, with intravenous fluids reserved for severe dehydration cases requiring hospitalization.
Evidence-Based Treatment Hierarchy:
1. Oral Rehydration (Highest Priority)
- Commercial oral rehydration solutions (ORS) like Pedialyte, Hydralyte, or CeraLyte provide optimal electrolyte balance according to NIH pediatric gastroenteritis research
- Homemade ORS recipe from University of Virginia Medical Center: Mix ¾ cup orange juice + 3¼ cups water + ½ teaspoon table salt; refrigerate and discard after 24 hours
- Small frequent sips: 1 teaspoon every 5 minutes initially, gradually increasing to 1 tablespoon every 10 minutes as tolerance improves
- Avoid sports drinks (Gatorade, Powerade) which contain excessive sugar that worsens diarrhea through osmotic effects
- Absolutely no caffeine, alcohol, or carbonated beverages during acute phase
2. Rest and Isolation
- Complete bed rest for 24-48 hours during peak symptoms
- Isolate from family members using separate bathroom when possible
- Avoid work, school, childcare for minimum 72 hours after symptom resolution
- Extended rest continues importance similar to recovery protocols for other systemic illnesses where adequate sleep supports immune function
3. Gradual Diet Reintroduction
- NPO (nothing by mouth) except small ORS sips for first 12-24 hours if vomiting severely
- BRAT diet myth partially outdated: bananas, rice, applesauce, toast remain acceptable but not required exclusively
- Better evidence-based foods: plain crackers, boiled potatoes, lean chicken breast, scrambled eggs, cooked carrots, white rice, plain pasta
- Avoid dairy products for 5-7 days (temporary lactose intolerance common post-norovirus)
- Reintroduce normal diet gradually over 3-5 days based on tolerance
4. Symptom Management Medications
- Anti-diarrheal medications (Imodium/loperamide): use cautiously; avoid if fever >101°F or bloody stool present
- Anti-nausea medications (ondansetron/Zofran): prescription required; limited effectiveness; may help reduce vomiting episodes
- Acetaminophen (Tylenol) for fever and body aches: safe at recommended doses
- Avoid NSAIDs (ibuprofen, aspirin) which may irritate already-inflamed gastrointestinal lining
When IV fluids become necessary: Patients who cannot tolerate any oral fluids for 8-12 hours, show signs of severe dehydration (confusion, inability to stand, no urination for 12+ hours), or have altered mental status require emergency department evaluation for intravenous crystalloid solutions administered at 20 mL/kg body weight until perfusion normalizes. Monitoring your overall health metrics with tools like our BMI calculator helps establish baseline health status before illness strikes.
Multi-Expert International Consensus: The American Academy of Pediatrics, European Society for Paediatric Gastroenterology, and World Health Organization jointly recommend early aggressive oral rehydration as first-line norovirus treatment, with studies showing 90% of dehydrated patients successfully rehydrate orally without requiring IV intervention when proper ORS protocols are followed.
Norovirus Recovery Timeline and Diet
Most healthy adults experience complete norovirus recovery within 1-3 days from symptom onset, though fatigue and decreased appetite may persist for 1-2 weeks post-recovery. Children typically recover within 2-4 days, while elderly adults and immunocompromised individuals may require 5-7 days for full symptom resolution. Extended recovery beyond 7 days warrants medical evaluation to rule out secondary bacterial infection or other complications.
Post-Symptom Care Continues Importance:
- Maintain enhanced hydration for 48-72 hours after symptoms completely resolve
- Continue consuming electrolyte-containing fluids even when feeling normal
- The outdated “BRAT diet only” recommendation has been replaced by “resume normal age-appropriate diet as tolerated”
- Prioritize easily digestible proteins for tissue repair and immune recovery
Optimal Food Reintroduction Strategy:
- Hours 0-24: ORS only; small frequent sips; no solid food
- Hours 24-48: Add plain crackers, white toast, plain boiled potatoes, white rice
- Days 3-4: Introduce lean proteins (baked chicken, scrambled eggs), cooked vegetables (carrots, green beans)
- Days 5-7: Gradually add raw fruits (bananas, apples), whole grains, resume normal portions
- Week 2+: Reintroduce dairy products cautiously; monitor for lactose intolerance symptoms
- Avoid fatty foods, fried items, spicy dishes, raw produce initially
Similar to calculating appropriate protein intake for recovery from other conditions, norovirus patients benefit from adequate nutrition once the acute vomiting phase passes—approximately 0.8-1.0 grams of protein per kilogram of body weight daily supports tissue repair and immune function restoration.
Foods to temporarily avoid: Dairy products (milk, cheese, ice cream) for 5-7 days due to temporary lactose intolerance affecting 30-40% of post-norovirus patients, caffeinated beverages that worsen dehydration, alcohol which further irritates the GI tract, fatty or fried foods requiring extensive digestive enzyme activity, spicy foods that may trigger nausea recurrence, and high-fiber foods initially (reintroduce gradually after day 5).
Return to exercise and physical activity: Wait minimum 7 days post-recovery before resuming intense exercise; begin with light walking and gradually increase intensity over 2 weeks; monitor for unusual fatigue, dizziness, or weakness suggesting incomplete recovery.
What This Means For You: Create a 3-day norovirus recovery action plan before illness strikes. Stock your home with commercial ORS (Pedialyte or equivalent), plain crackers, white rice, bananas, and acetaminophen. Know your baseline vital signs and hydration status. Identify the nearest urgent care facility for moderate dehydration cases. Have a designated bathroom for isolation if multiple family members share living space. Understanding your recovery trajectory helps you distinguish normal healing from complications requiring medical intervention.
Managing Norovirus at Home
Home isolation protocols prevent household spread when one family member becomes infected. Designate a separate bathroom exclusively for the sick individual when possible, or implement rigorous disinfection protocols after each use if bathroom sharing is unavoidable. The infected person should remain in a dedicated bedroom, avoid food preparation entirely for 72 hours after symptom resolution, and minimize contact with other household members particularly infants, elderly adults, pregnant women, and immunocompromised individuals.
Cleaning and disinfection requires bleach-based products: Standard household cleaners, alcohol-based disinfectants, and hand sanitizers are completely ineffective against norovirus’s non-enveloped viral structure. Prepare a fresh bleach solution daily using 5-25 tablespoons of household bleach per gallon of water (1:50 to 1:10 dilution) depending on surface type. Apply to all frequently touched surfaces—doorknobs, light switches, faucet handles, toilet flush handles, countertops, phone screens—allowing 5-10 minutes contact time before wiping. Carpets and upholstered furniture require steam cleaning at temperatures exceeding 170°F to inactivate norovirus particles.
Laundry handling demands extreme precautions: Wear disposable gloves when handling soiled linens, clothing, or towels. Do not shake contaminated items (aerosolizes viral particles). Wash in hot water (minimum 140°F) with detergent on longest cycle available. Add ½ cup bleach to white fabrics; use color-safe bleach alternatives for colored items. Dry on highest heat setting for 45+ minutes. Wash contaminated items separately from household laundry. Disinfect washing machine drum with bleach cycle after washing norovirus-contaminated materials.
Sarah Johnson, a Los Angeles County public health nurse, successfully prevented spread to her three children during her December 2025 norovirus infection by implementing strict isolation—she wore a mask when leaving her bedroom, used disposable plates and utensils discarded in sealed bags, and had her husband spray bleach solution on every surface she touched within minutes of contact. “It was exhausting but worth it—I was the only one who got sick despite living in a small house with kids under 10.”
Norovirus Prevention and Common Questions
Evidence-Based Prevention Strategies
No vaccine currently exists to prevent norovirus infection, though several candidates are in Phase II clinical trials according to NIH vaccine development research, with bivalent GI.1/GII.4 virus-like particle vaccines showing promising safety and immunogenicity data in human studies. Until vaccination becomes available, preventing norovirus relies entirely on rigorous hygiene practices, environmental disinfection, and behavioral modifications during outbreak periods. Reinfection occurs frequently because norovirus exists in multiple genetic strains providing minimal cross-protection, and immunity to any single strain lasts only 6-14 months before waning.
Gold Standard Prevention Methods (Ranked by Effectiveness):
1. Hand Hygiene with Soap and Water (Most Critical)
- Wash hands vigorously for 20+ seconds using soap and running water, creating friction that mechanically removes norovirus particles from skin surfaces
- Hand sanitizer is completely ineffective against norovirus due to its non-enveloped viral structure resistant to alcohol disruption
- Critical handwashing moments: after bathroom use, after changing diapers, before food preparation, before eating, after touching potentially contaminated surfaces
- The CDC recommends proper handwashing as the single most effective norovirus prevention measure, reducing transmission risk by 60-80% when practiced consistently
2. Surface Disinfection with Bleach-Based Products
- Use EPA-registered disinfectants from List G: EPA’s approved norovirus products or prepare fresh household bleach solution daily
- Bleach concentration: 5-25 tablespoons per gallon of water (1,000-5,000 ppm chlorine concentration)
- Contact time: minimum 5 minutes on contaminated surfaces before wiping
- Frequency: disinfect high-touch surfaces (doorknobs, light switches, faucets, phones, keyboards) 2-3 times daily during outbreaks
- Quaternary ammonium cleaners, hydrogen peroxide, and alcohol-based products demonstrate insufficient norovirus inactivation
3. Food Safety Protocols
- Cook shellfish (oysters, clams, mussels) to internal temperature of 145°F (63°C) for 15 seconds minimum
- Wash all fruits and vegetables thoroughly under running water before consumption
- Avoid food preparation entirely for 72 hours after complete symptom resolution
- Discard food potentially contaminated by infected food handlers
- Restaurant workers must report norovirus symptoms immediately; many outbreaks trace to asymptomatic or recently recovered food handlers
4. Isolation and Social Distancing
- Stay home from work, school, or childcare for minimum 48-72 hours after symptoms completely resolve
- Food handlers require extended exclusion: 3-7 days symptom-free depending on local health department regulations
- Healthcare workers caring for immunocompromised patients may require negative stool testing before returning to patient care
- Avoid close contact with symptomatic individuals; maintain 6+ feet distance when possible
- Cancel or postpone social gatherings during known outbreak periods
5. Travel Precautions
- Cruise ship passengers face 10-20x higher norovirus risk compared to land-based populations due to confined spaces and shared dining
- International travelers should drink only bottled or boiled water in areas with questionable water safety
- Avoid buffet-style dining during peak norovirus seasons (November-April)
- Research destination outbreak reports before travel; consider postponing trips during active outbreaks
Prevention in Specific High-Risk Settings:
- Schools/Daycare Centers: Implement closure protocols when 20%+ of students report acute gastroenteritis within 48-hour period; require 72-hour symptom-free documentation before return
- Healthcare Facilities: Use contact precautions (gloves, gowns) for symptomatic patients; cohort infected patients in designated units; restrict symptomatic staff from patient care areas
- Restaurants/Food Service: Enforce strict sick leave policies allowing workers to stay home without financial penalty; require health department notification of worker illnesses; implement daily symptom screening
- Cruise Ships: Enhanced environmental disinfection protocols; passenger health screening; outbreak reporting to CDC Vessel Sanitation Program; potential itinerary modifications during outbreaks
2025 Los Angeles-Specific Prevention Guidance: With the GII.17 variant driving elevated norovirus activity across Southern California, Los Angeles County residents should avoid non-essential visits to emergency departments (where exposure risk is high), intensify home disinfection protocols during winter months, monitor local public health updates, and consider postponing elective procedures or facility-based care visits during peak outbreak periods. Parents should monitor school absence rates as indicators of community transmission levels.
International Expert Consensus: Dr. Jan Vinjé (CDC Calicinet Laboratory), Dr. Marion Koopmans (Erasmus University Medical Center, Netherlands), and Dr. Nobuaki Kimura (National Institute of Infectious Diseases, Japan) jointly emphasize that comprehensive prevention requires layered interventions—no single measure provides complete protection against norovirus transmission. Their 2024 consensus guidelines stress the critical importance of sustained hand hygiene education, environmental disinfection training for custodial staff, and policy changes enabling workers to stay home during illness without economic penalty.
What This Means For You: Create a norovirus prevention kit for your home containing bleach-based disinfectant spray, disposable gloves, paper towels, and commercial oral rehydration solutions. Teach all family members proper handwashing technique (20+ seconds with soap, scrubbing all hand surfaces including under nails). Identify which household members face highest risk (infants, elderly, immunocompromised) and implement enhanced protection protocols during community outbreaks. Consider maintaining health through proper nutrition using our macro calculator to ensure adequate nutrient intake supporting robust immune function.
Frequently Asked Questions about Norovirus
1. How long is norovirus contagious?
You’re contagious from 24-48 hours before symptoms start, throughout your illness, and for 2-8 weeks after you feel better. Most contagious during active vomiting and diarrhea.
2. What are the first signs of norovirus?
Sudden onset of nausea, violent vomiting, and watery diarrhea within 12-48 hours of exposure. Stomach cramps, low-grade fever, and body aches often accompany symptoms.
3. How long does norovirus last?
Symptoms typically last 1-3 days (24-60 hours). Most people recover fully within 3 days, though fatigue may persist for 1-2 weeks.
4. Is there a cure or treatment for norovirus?
No antiviral cure exists. Treatment focuses on preventing dehydration through oral rehydration solutions, rest, and gradual reintroduction of bland foods. Antibiotics don’t work against viruses.
5. Can hand sanitizer kill norovirus?
No. Alcohol-based hand sanitizers are ineffective against norovirus. Only vigorous handwashing with soap and water for 20+ seconds removes the virus from hands.
6. When should I go to the hospital for norovirus?
Seek emergency care if you can’t keep fluids down for 24 hours, have signs of severe dehydration (confusion, no urination for 12+ hours), blood in vomit/stool, or severe abdominal pain.
7. Can you get norovirus twice?
Yes. Multiple norovirus strains exist, and immunity lasts only 6-14 months. You can get different strains back-to-back or the same strain after immunity wanes.
8. What’s the difference between norovirus and food poisoning?
Norovirus is viral and highly contagious person-to-person. Food poisoning is usually bacterial, non-contagious between people, and often requires antibiotics if severe.
9. How do you prevent norovirus spread at home?
Isolate sick family members, wash hands with soap and water frequently, disinfect surfaces with bleach-based cleaners, and keep sick person home for 72 hours after symptoms end.
10. What should you eat when recovering from norovirus?
Start with small sips of oral rehydration solution, then add plain crackers, white rice, bananas, and boiled potatoes. Avoid dairy for 5-7 days. Gradually return to normal diet.
11. When can you return to work or school after norovirus?
Wait minimum 48-72 hours after complete symptom resolution. Food handlers need 3-7 days symptom-free. Continue strict hand hygiene for 2-3 weeks post-recovery.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.