On This Page – Quick Medical Summary
Marcus noticed a thin brown line on his thumbnail in early 2023. He assumed it was from closing a car door too hard. By the time he saw a dermatologist — 16 months later — his subungual melanoma had progressed to Stage II.
Subungual melanoma — also called nail melanoma — is a rare but potentially lethal skin cancer that grows beneath the fingernail or toenail. It is frequently mistaken for a bruise, fungal infection, or minor nail trauma. This guide covers every warning sign, the critical red flags that demand urgent care, and what the latest 2025–2026 evidence says about survival and treatment.
What Is Subungual Melanoma?
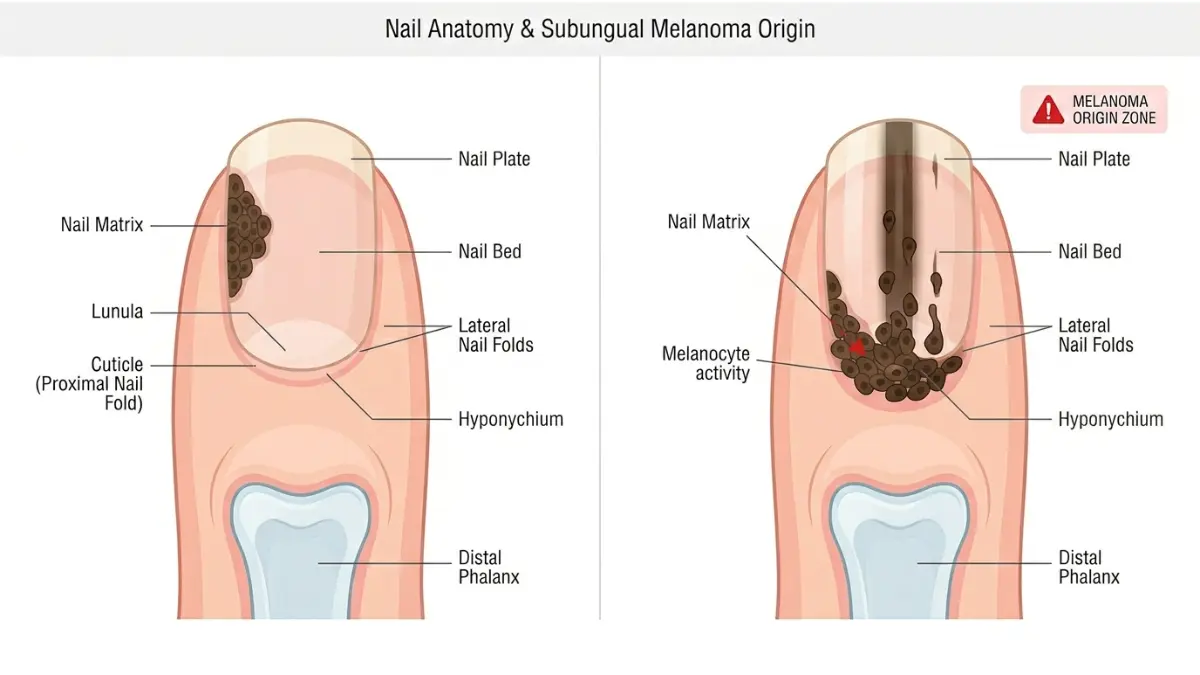
How It Develops Under the Nail
Subungual melanoma is a subtype of acral lentiginous melanoma — a form of skin cancer that originates in the nail matrix, the tissue beneath the nail plate where new cells are formed.
Unlike most skin cancers, nail melanoma is not caused by UV radiation or sun exposure. This makes it harder to predict and easier to dismiss. According to the NIH StatPearls updated August 2025, it accounts for 0.7–3.5% of all melanomas in lighter-skinned populations — but up to 30% of melanomas diagnosed in dark-skinned individuals.
- Most commonly affects the thumb (fingernail) and big toe (toenail) — 75–90% of cases
- Begins in melanocytes, the pigment-producing cells within the nail unit
- Can spread aggressively to lymph nodes and distant organs if not caught early
Understanding your personal risk is a smart first step — use our Genetic Risk Assessment Tool to evaluate your hereditary cancer risk profile.
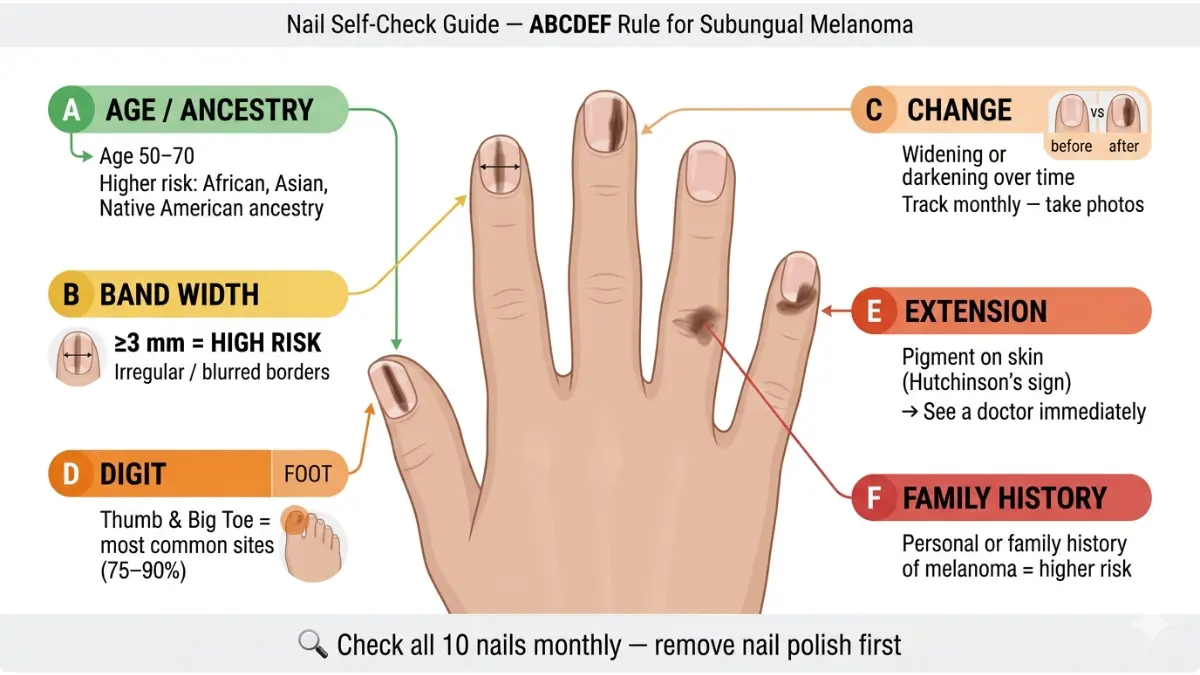
The ABCDEF Risk Factor Guide for Nail Melanoma
Dermatologists use the ABCDEF mnemonic to assess pigmented nail lesions. Learn it — it could save your life.
| Letter | What It Stands For |
|---|---|
| A | Age 50–70 years; African, Asian, or Native American heritage |
| B | Brown-black pigmented nail band ≥3mm with blurred or irregular borders |
| C | Change in nail band width, color, or texture — or no change despite treatment |
| D | Digit — thumb, big toe, or index finger most commonly affected |
| E | Extension of pigment onto the surrounding skin (Hutchinson’s sign) |
| F | Family or personal history of melanoma or atypical moles (dysplastic nevi) |
If 3 or more of these apply to you, see a board-certified dermatologist — not just your GP.
Subungual Melanoma Symptoms — The Complete Warning Sign Checklist
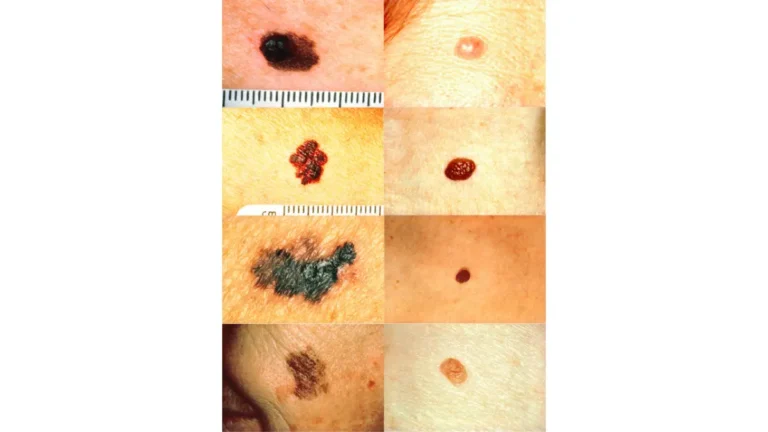
Classic Symptoms: What Nail Melanoma Actually Looks Like
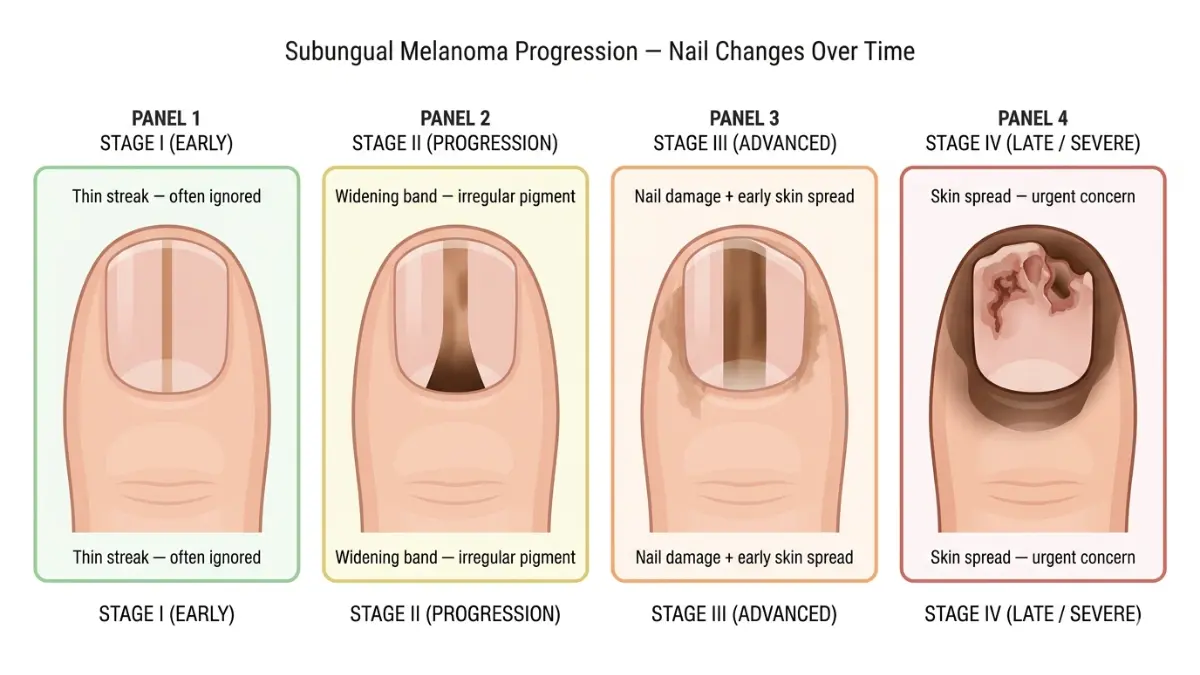
The most recognizable symptom of subungual melanoma is a longitudinal melanonychia — a vertical, dark-colored streak running from the nail base (cuticle) to the tip. Review the full melanoma warning signs guide for broader skin cancer context.
Early and progressive warning signs include:
- A dark brown or black vertical stripe on one nail that does not move toward the fingertip as the nail grows
- A widening band — especially when the base (cuticle end) is wider than the tip (triangular shape = high-risk)
- Irregular pigmentation within the stripe — uneven color, patchy dark and light areas
- Nail splitting, cracking, thinning, or crumbling without obvious cause
- Nail lifting away from the nail bed (onycholysis)
- Unexplained swelling or redness around the nail without injury
- Bleeding under the nail that doesn’t resolve within 2–3 weeks
- Pigment spreading onto the surrounding skin (Hutchinson’s sign — see below)
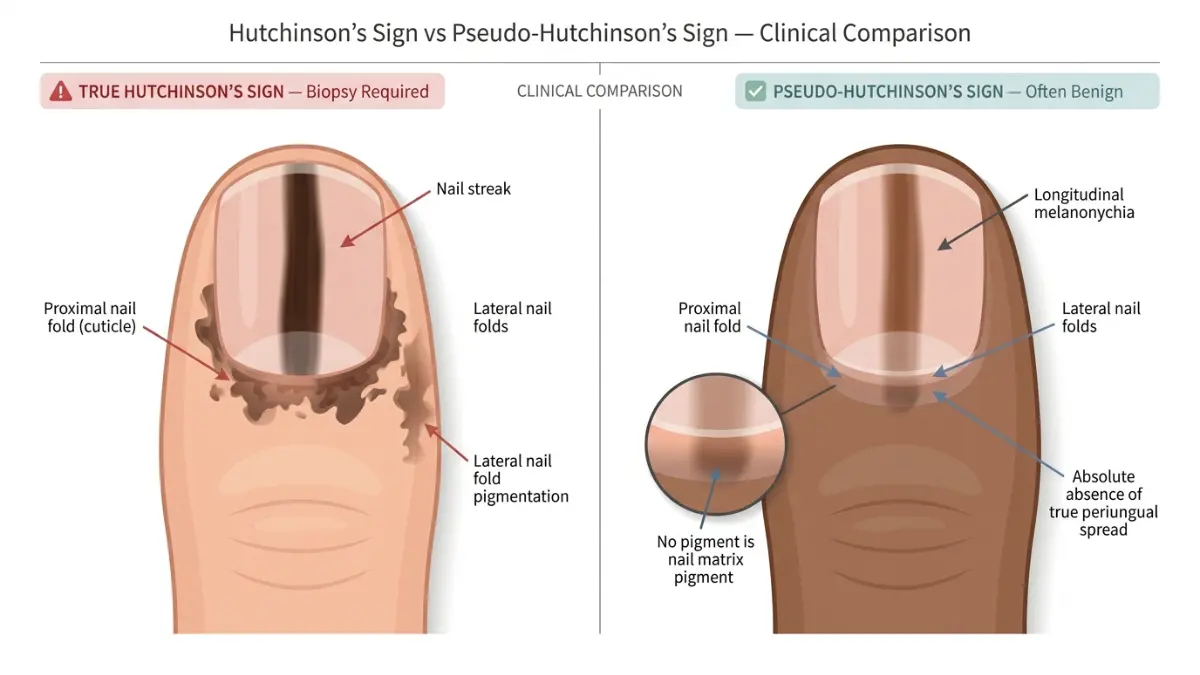
Hutchinson’s Sign: The Most Critical Red Flag in Nail Cancer
Hutchinson’s sign occurs when dark pigmentation spreads from beneath the nail onto the skin of the proximal or lateral nail folds — the skin surrounding the nail.
According to DermNet NZ’s updated nail melanoma resource, this sign is historically considered near-diagnostic of subungual melanoma and warrants immediate biopsy referral.
⚠️ Critical Note — Pseudo-Hutchinson’s Sign: Not every pigment extension means cancer. A “Pseudo-Hutchinson’s sign” occurs when deep nail pigmentation shows through the transparent nail fold skin, mimicking true periungual spread. This is more common in darker-skinned individuals and can lead to over-diagnosis if assessed without dermoscopy. Only a qualified dermatologist using dermoscopy can distinguish the two reliably.
Amelanotic Nail Melanoma: The Invisible Killer (Missed by Most Competitors)
This is the most under-discussed subtype — and the most dangerous for missed diagnosis.
Approximately 25% of subungual melanomas are amelanotic — meaning they produce no dark pigmentation at all. Per data from the Cancer Therapy Advisor clinical resource, amelanotic cases may present as:
- A red, pink, or flesh-colored band in the nail bed
- Unexplained nail bleeding or ulceration
- Nail notching at the distal edge
- A verrucous (wart-like) mass lifting the nail plate
Bold Takeaway: A nail melanoma with no dark color is among the most missed diagnoses in dermatology. If your nail changes feel abnormal but look “normal,” still see a doctor. Use our Symptom Checker for an initial assessment.
Subungual Melanoma vs. Bruise vs. Fungal Infection: Quick Comparison
| Feature | Subungual Melanoma | Subungual Hematoma (Bruise) | Fungal Nail Infection |
|---|---|---|---|
| Color | Brown/black/red streak | Dark purple-black | Yellow, white, or green |
| Moves with nail growth? | ❌ No — stays fixed at base | ✅ Yes — moves toward tip | N/A |
| Hutchinson’s sign | ✅ Possible | ❌ No | ❌ No |
| Preceded by injury? | ❌ Usually no | ✅ Yes | ❌ No |
| Resolves in weeks? | ❌ No | ✅ Yes (2–6 weeks) | Slow (months) |
| Multiple nails affected? | ❌ Usually single nail | Sometimes | ✅ Often multiple |
When Should You Worry? The “See a Doctor NOW” Decision Framework
Red Flags That Require Urgent Dermatologist Appointment
According to Cleveland Clinic’s subungual melanoma clinical guide, early detection is the single most important factor in survival outcomes. Do not wait if you notice:
- A dark nail band that has been present for more than 4–6 weeks with no injury history
- A band wider than 3mm, or one that appears wider at the cuticle end
- Irregular coloration (patchy, multi-toned pigmentation within the stripe)
- Any Hutchinson’s sign — pigment on the skin surrounding the nail
- Nail dystrophy (cracking, splitting, lifting) alongside any dark discoloration
- A non-healing wound, nodule, or ulcer beneath or around the nail
- New or unexplained nail changes in anyone over age 50, especially with African, Asian, or Native American heritage
“If your nail shows 3 or more of these warning signs, do not wait — contact a board-certified dermatologist this week, not this month.”
Signs That Are Likely Harmless (But Monitor Closely)
Some nail pigmentation is benign — but still worth tracking:
- A single thin line that appeared immediately after a direct nail injury
- A line that visibly moves distally (toward the fingertip) over 4–6 weeks
- Multiple nails showing faint pigmentation simultaneously (more likely melanonychia from systemic cause, medication, or ethnic variation)
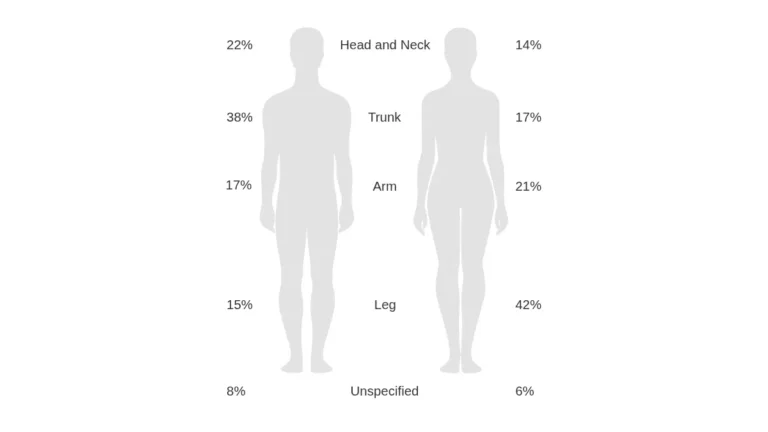
What This Means For You: If you’re in a lower-risk group and the line appeared after clear trauma and is moving — take a photo, monitor it monthly, and see your doctor at the 6-week mark if it hasn’t moved. For broader context on where melanoma appears on the body, read our guide on melanoma body locations and early spots.
How Is Subungual Melanoma Diagnosed?
Step 1: Clinical Examination and Dermoscopy
When you visit a dermatologist about a suspicious nail change, the initial assessment typically includes:
- Full ABCDEF history review — when did the change appear, how has it evolved
- Dermoscopy — a non-invasive magnification tool that reveals pigment patterns invisible to the naked eye
- Complete skin examination — checking for other melanocytic lesions
The American Academy of Dermatology recommends annual full-body skin checks for anyone with melanoma risk factors — which include nail inspection as standard.
Step 2: Nail Matrix Biopsy — The Gold Standard
If dermoscopy findings are suspicious, a nail matrix biopsy is required for definitive diagnosis. No blood test or imaging alone can confirm nail melanoma.
- A small tissue sample is taken from the nail matrix and nail bed
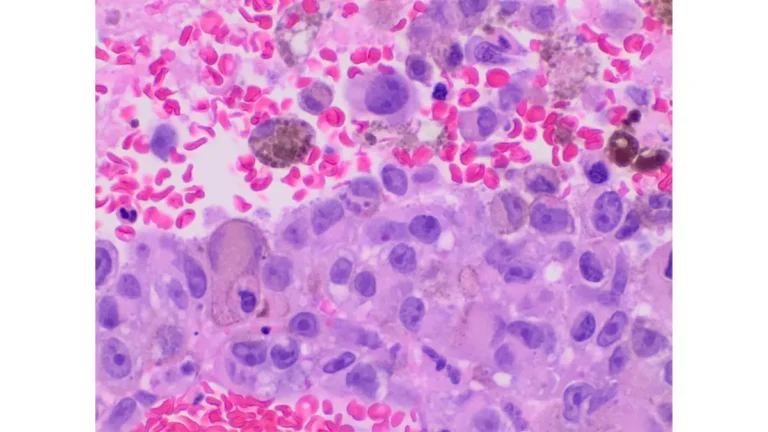
- A pathologist examines cells for melanocytic density, pagetoid spread, nuclear pleomorphism, and confluent cell patterns
- Incomplete biopsy is a known clinical risk — partial sampling can result in an in-situ (early) diagnosis when invasive melanoma is actually present
For more on how biopsy results work and what to expect from the timeline, see our biopsy results timeline and report guide.
If the biopsy confirms nail melanoma, your care team will order imaging (CT, PET scan, sentinel lymph node biopsy) to determine staging. According to the National Cancer Institute, staging determines prognosis and treatment pathway.
Subungual Melanoma Stages, Treatment, and Survival Rates
Staging and Survival Rate Table (2025–2026 Data)
| Stage | Description | 5-Year Survival Rate |
|---|---|---|
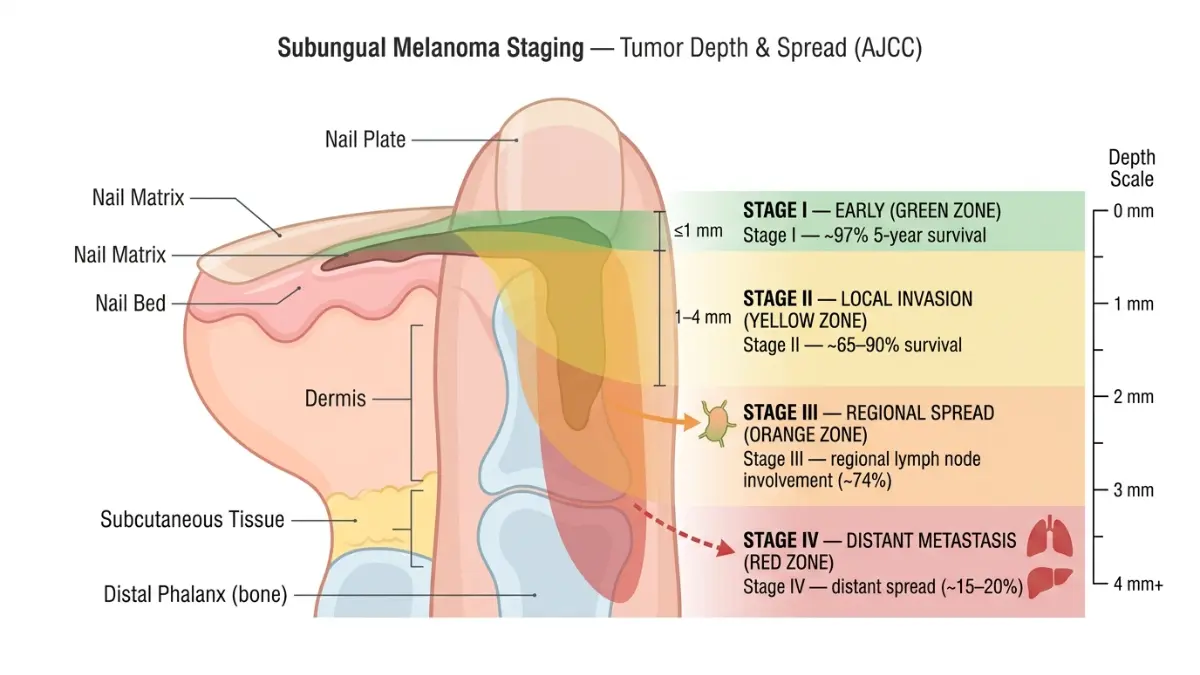
| Stage IA | Thin tumor (≤1mm), no ulceration, localized | ~97% |
| Stage IB/IIA | Thicker tumor or mild ulceration, localized | ~85–90% |
| Stage IIB/IIC | Thicker with ulceration, no lymph node spread | ~65–80% |
| Stage III | Regional lymph node involvement | ~74% (spread regionally) |
| Stage IV | Distant organ metastasis | 15–20% |
Sources: WebMD Subungual Melanoma Outlook | American Cancer Society | Medical News Today
Bold Takeaway: Stage IA subungual melanoma has a 97% five-year survival rate. Every month of delayed diagnosis moves the needle closer to Stage III or IV — where survival drops below 74%.
For deeper data on melanoma outcomes nationally, our melanoma statistics 2026 article provides the full landscape.
Treatment Options for Nail Melanoma in 2025–2026
1. Surgical Excision (Primary Treatment)
- Wide local excision is now the preferred approach for most cases — the historic standard of full digital amputation is no longer routine
- For thumb or big toe involvement, distal phalangeal amputation may still be recommended to achieve clear margins
- Sentinel lymph node biopsy is performed for tumors thicker than 0.8mm
2. Immunotherapy and Targeted Therapy (Advanced Cases)
This is the 2025–2026 breakthrough angle competitors miss. According to research published in Cancers (Basel), subungual melanoma frequently carries KIT gene mutations — distinct from the BRAF mutations common in other melanomas.
- Anti-PD-1 immunotherapy (nivolumab, pembrolizumab) — first-line for Stage III–IV
- KIT inhibitors (imatinib, sunitinib) — emerging targeted option for KIT-mutant cases
- Clinical trial enrollment is increasingly recommended for advanced nail melanoma
Our comprehensive guide to immunotherapy for melanoma and how it works explains these treatments in patient-friendly terms. For Stage IV nail melanoma specifically, see our Stage 4 melanoma survival and therapy guide.
3. Follow-Up and Monitoring
- Dermatology appointments every 3–6 months for the first 2 years
- Annual full-body skin exam for life
- Monthly nail self-checks at home (see Section 6)
Racial and Ethnic Disparities in Subungual Melanoma
This is a critical health equity point almost entirely absent from competitor articles.
Dark-skinned populations face significantly higher diagnostic delays because longitudinal melanonychia — the dark nail streak — is common and benign in people of African, Asian, and Hispanic descent. By age 50, nearly 100% of African Americans have some degree of nail pigmentation, per DermNet NZ.
This means the same symptom that triggers immediate concern in a lighter-skinned patient is routinely dismissed in darker-skinned patients — contributing to later-stage diagnosis and worse outcomes. Awareness in these communities is not optional; it is urgent.
Prevention, Self-Monitoring, and When to See a Specialist
Your Monthly 5-Step Nail Self-Check Routine
Subungual melanoma cannot be prevented — it is not caused by UV exposure, diet, or lifestyle. Your best defense is consistent self-monitoring and early action.
Do this once a month, in good lighting:
- Remove nail polish from all fingernails and toenails
- Inspect each nail under bright natural light — look at the nail plate, nail bed, and surrounding skin
- Check for any new dark lines, streaks, or spots — especially on thumbs, big toes, and index fingers
- Look at the skin around each nail — any pigment bleeding onto the surrounding skin?
- Photograph any suspicious nails with your phone — same angle each month — and compare
If you notice any change that meets the ABCDEF criteria, use our Symptom Checker and book a dermatologist appointment within 1–2 weeks.
When to See Which Doctor
| Symptom Severity | Who to See | How Fast |
|---|---|---|
| New dark line after clear injury, moving distally | GP or Primary Care | Within 4–6 weeks if not resolved |
| New line with no injury, ≥3mm, or widening | Dermatologist | Within 1–2 weeks |
| Hutchinson’s sign, nail destruction, or bleeding | Dermatologist (urgent referral) | Within days |
| Confirmed melanoma diagnosis | Dermatologic oncologist | Immediate |
The Skin Cancer Foundation recommends that any persistent, unexplained nail change be assessed by a board-certified dermatologist — not dismissed as cosmetic.
For a comprehensive overview of all melanoma subtypes, stages, and treatment pathways, our complete melanoma symptoms, stages, and treatment guide is the most thorough resource on our platform. You can also explore the full melanoma ABCDE warning signs guide for moles for a deeper look at how dermatologists assess pigmented lesions across the skin.
Finally, AI-assisted screening is emerging as a powerful early-detection tool — read our 2026 article on AI screening and melanoma survival rates to understand what’s available today.
Frequently Asked Questions About Subungual Melanoma
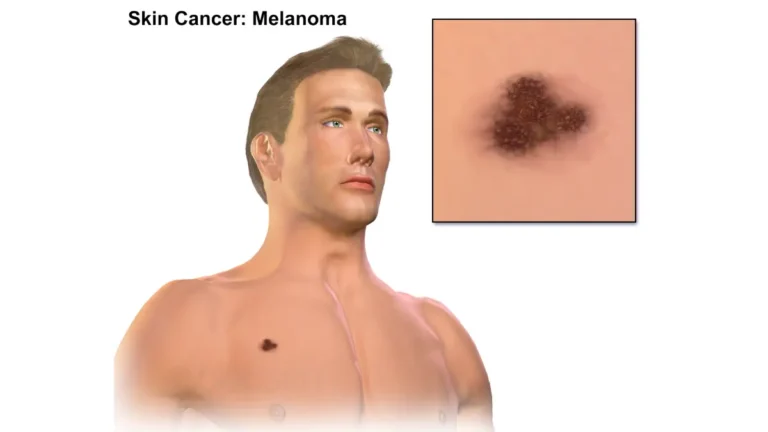
1. What does subungual melanoma look like?
It typically appears as a brown or black vertical streak on a single nail, often widening at the cuticle end. In ~25% of cases, no dark color is present — known as amelanotic nail melanoma.
2. Is a black line on my nail always cancer?
No. Benign longitudinal melanonychia is extremely common — especially in people with darker skin. However, any line wider than 3mm, irregular in color, or accompanied by nail changes should be evaluated by a dermatologist.
3. What is Hutchinson’s sign in nail melanoma?
It is the extension of dark pigmentation from beneath the nail onto the surrounding skin folds. It is a key red flag for subungual melanoma and warrants immediate biopsy referral.
4. Can subungual melanoma look like a bruise?
Yes — this is its most common mimicker. The key difference: a traumatic bruise (hematoma) gradually moves toward the fingertip as the nail grows. A melanoma stays fixed at the nail base.
5. Which nails does nail melanoma most commonly affect?
The thumb and big toenail in 75–90% of reported cases, according to City of Hope Cancer Center. The index finger is third most common.
6. What is the survival rate for subungual melanoma?
At Stage IA, the 5-year survival rate is approximately 97%. At Stage IV with distant organ metastasis, it drops to 15–20%. Early detection is the single most important factor.
7. Is nail melanoma caused by sun exposure?
No. Unlike other forms of melanoma, subungual melanoma has no established link to UV radiation or tanning bed use. Its exact cause remains unclear.
8. Who is at highest risk for subungual melanoma?
People over age 50, individuals of African, Asian, or Native American heritage, and those with a personal or family history of melanoma or dysplastic nevi.
9. How is subungual melanoma diagnosed?
Diagnosis requires a nail matrix biopsy — dermoscopy alone cannot confirm it. A pathologist examines the biopsy for specific cellular patterns consistent with melanoma.
10. What is amelanotic nail melanoma?
A subtype representing ~25% of nail melanomas that produces no dark pigment. It often presents as a red, pink, or flesh-colored nail abnormality, making it the most frequently missed form.
11. Can subungual melanoma be cured?
Yes — particularly when caught at Stage I or II. Surgical excision with clear margins offers excellent outcomes. Advanced stages require immunotherapy or targeted therapy, with ongoing clinical trials showing promising results in 2025–2026.
📚 Further Reading on MyMedicineAdvisor:
⚠️ Medical Disclaimer: This article is intended solely for educational and informational purposes. It does not replace professional medical advice, diagnosis, or treatment. If you notice any changes to your nails or skin, consult a board-certified dermatologist or licensed healthcare provider promptly. MyMedicineAdvisor.com does not provide medical diagnoses.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.