On This Page – Quick Medical Summary
Measles Outbreak 2025: 1,958 Cases, 3 Deaths—Symptoms, Vaccine & Prevention Guide
The measles outbreak in 2025 has reached 1,958 confirmed cases across 44 U.S. states with 3 deaths reported, marking the highest measles cases since 1992. This highly contagious viral infection spreads through airborne droplets and causes fever, cough, distinctive rash, and potentially fatal complications—especially among unvaccinated children and immunocompromised individuals.
A Mother’s Fear: The Reality of Measles in 2025
Sarah Mitchell rushed her 4-year-old daughter Emma to the emergency room in Austin, Texas, when her fever spiked to 104°F. Three days earlier, Emma had developed what seemed like a common cold—runny nose, watery eyes, persistent cough. But when the telltale red rash spread from her face down to her chest, doctors confirmed measles. Emma, unvaccinated due to delayed appointments, spent five days hospitalized with measles pneumonia requiring oxygen support. “I never imagined measles could be this serious,” Sarah recalls, her voice breaking. “We came so close to losing her.”
Emma’s story mirrors thousands of families caught in the largest measles outbreak the United States has experienced in three decades. As of December 17, 2025, the Centers for Disease Control and Prevention reports 1,958 confirmed measles cases nationwide, with 222 hospitalizations and 3 tragic deaths—all among unvaccinated individuals. Public health experts confirm that 93% of hospitalized patients had no measles vaccination history, underscoring the vaccine’s critical protective role.
Measles Outbreak 2025: State-by-State Breakdown
The measles outbreak has hit several states particularly hard. Texas leads with 803 confirmed cases, followed by South Carolina (142 cases), Arizona (182 cases), Utah (122 cases), and Kansas (91 cases). Health departments across these regions have issued urgent vaccination advisories, especially for parents with children under 5—the demographic facing the highest complication rates.
Beyond U.S. borders, the measles spread presents a global crisis. The Pan American Health Organization documented 10,139 measles cases across ten countries in the Americas during 2025, including 18 deaths. Europe reported over 127,000 cases in 2024, demonstrating how quickly measles outbreaks escalate in populations with declining vaccination coverage.
Why This Outbreak Matters Now
- Vaccine hesitancy has dropped measles immunity below the 96% threshold needed for herd protection
- International travel increases exposure risk, with infected individuals unknowingly spreading measles in airports and public transit
- Rapid transmission: One infected person can spread measles to 9-18 others in confined spaces
- Preventable deaths: The 3 deaths reported in 2025 could have been avoided with timely MMR vaccination
If you or your child develops fever, cough, and rash after potential exposure, use our symptom checker tool immediately to assess symptom severity. Understanding the measles death rate (approximately 1-2 per 1,000 cases in developed countries) highlights why prevention through routine vaccination schedules remains the most effective strategy. The unvaccinated measles risk extends beyond individual health—every unprotected person weakens community immunity and enables measles outbreak 2025 numbers to climb further.
Disclaimer: This article is for educational purposes, not medical advice. Consult healthcare providers for diagnosis and treatment.
Early Signs and Measles Symptoms You Must Know
Recognizing measles symptoms early can save lives, especially during the current outbreak where delayed diagnosis has contributed to severe complications. The measles rash may be the most recognizable sign, but critical warning symptoms appear days before, giving families a narrow window to seek medical care and prevent transmission.
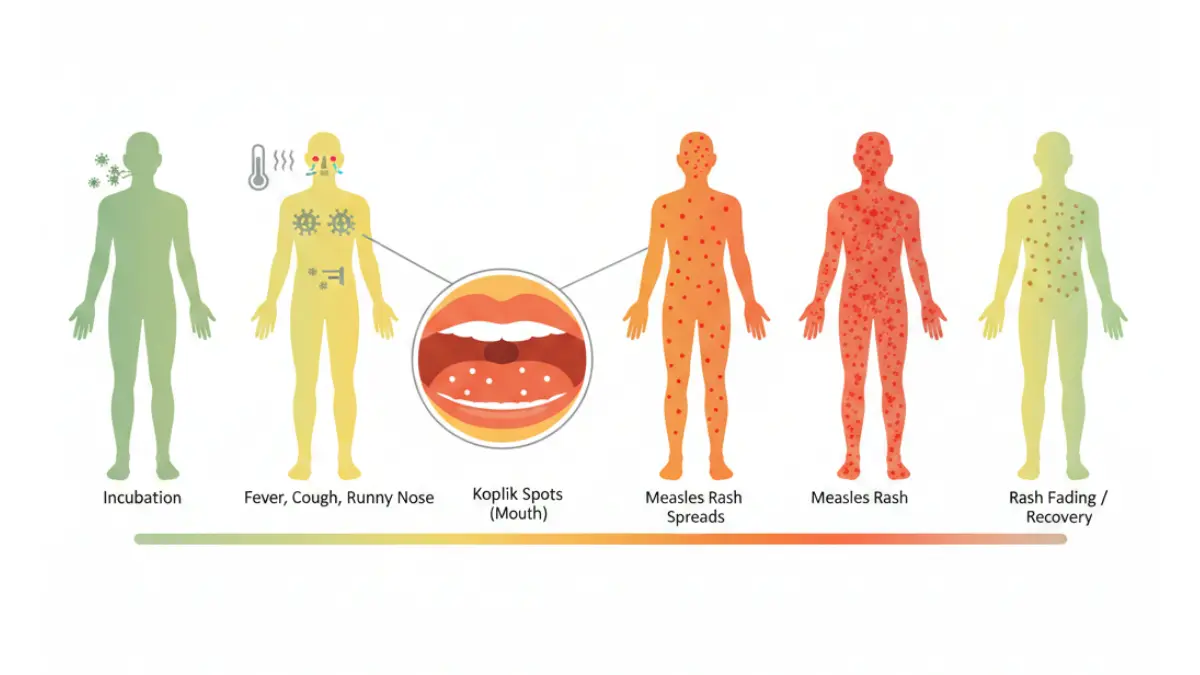
Timeline of Measles Symptoms (Days 1-14)
Days 1-4 (Incubation Period): After exposure to the measles virus, infected individuals show no symptoms but can already spread the disease to others. This silent transmission phase makes measles outbreak control particularly challenging.
Days 5-9 (Prodromal Stage): The first measles symptoms appear suddenly—high measles fever (often 103-105°F), persistent dry cough, runny nose, and watery red eyes (conjunctivitis). Many parents mistake these early measles signs for common cold or flu, delaying critical diagnosis. Monitoring elevated body temperature through tools like our heart rate zone calculator can help track fever patterns associated with viral infections.
Days 10-12 (Koplik Spots Emerge): Before the measles rash appears, tiny white spots with red halos develop inside the mouth, particularly on the inner cheeks. These Koplik spots are pathognomonic—meaning their presence definitively indicates measles infection. Unfortunately, they disappear within 1-2 days, often going unnoticed by families.
Days 13-17 (Rash Phase): The characteristic measles rash erupts as flat red spots that merge into larger patches. The rash progression follows a predictable head-to-toe pattern: starting at the hairline and face, spreading to the neck and trunk, then extending to arms and legs over 3-4 days. As the rash spreads downward, the measles fever typically peaks, sometimes reaching dangerous levels requiring hospitalization.
Days 18-21 (Recovery Phase): The measles rash begins fading in the same order it appeared, leaving a temporary brownish discoloration. However, patients remain contagious until 4 days after the rash emerges, requiring strict isolation.
Koplik Spots: The Tell-Tale Sign Before Rash
What are Koplik spots? These small white lesions appear 2-3 days before the measles rash and serve as the earliest definitive diagnostic marker. Healthcare providers trained to identify Koplik spots can diagnose measles during this critical window, potentially preventing severe complications through early intervention.
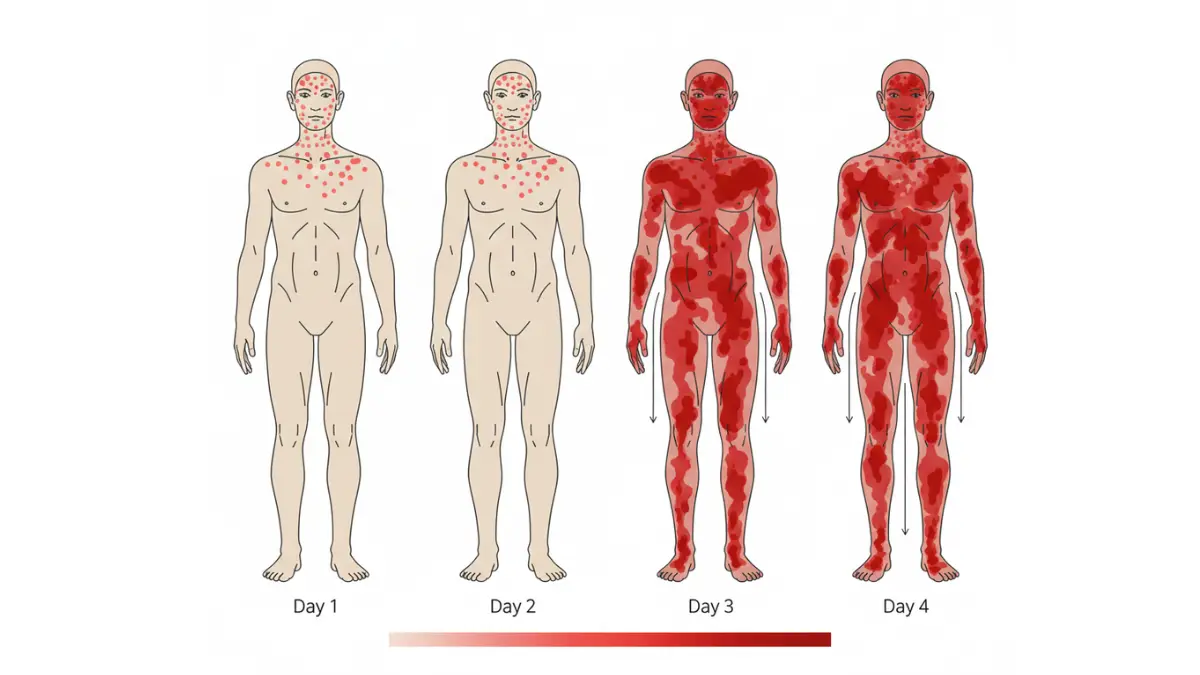
Measles Rash Progression: What to Expect
| Rash Timeline | Location | Appearance | Duration |
|---|---|---|---|
| Day 1-2 | Face, hairline, behind ears | Flat red spots (maculopapular) | Peaks at 2-3 days |
| Day 2-3 | Neck, upper trunk, arms | Spots merge into blotches | Begins fading on face |
| Day 3-4 | Lower trunk, legs, feet | Widespread coverage | Total body involvement |
| Day 5-7 | Fading (head to toe) | Brownish discoloration | Resolves completely by day 14 |
Measles in Children vs Adults: Key Differences
Measles in children under age 5 presents with more severe symptoms and higher complication rates. Infants too young for vaccination face the greatest risk—30% of measles cases in children result in complications like ear infections, diarrhea, or life-threatening pneumonia.
Measles in adults, particularly those who never received the MMR vaccine, experience more intense symptoms including prolonged high measles fever, severe body aches, and increased risk of measles pneumonia and measles encephalitis. Pregnant women infected with measles face additional dangers: pregnancy loss, preterm labor, and low birth weight babies. Women in their first trimester should use our pregnancy due date calculator to track gestational age if measles exposure occurs, as timing affects complication severity.
How Doctors Diagnose Measles (Blood Tests & Clinical Exam)
Healthcare providers diagnose measles through clinical assessment and laboratory confirmation. The diagnostic process includes:
- Physical examination: Identifying characteristic measles symptoms (fever, cough, conjunctivitis), Koplik spots, and distinctive measles rash pattern
- Blood tests: IgM antibody detection confirms acute measles infection within 3-28 days of rash onset
- Throat or nasopharyngeal swab: PCR testing detects measles virus RNA, providing rapid confirmation
- Differential diagnosis: Ruling out measles vs rubella, roseola, scarlet fever, and other viral infections with similar presentations
Measles vs Rubella: Spotting the Differences
| Feature | Measles | Rubella |
|---|---|---|
| Fever severity | High (103-105°F) | Mild (99-100°F) |
| Rash appearance | Large blotchy patches | Fine pink spots |
| Rash progression | Head-to-toe over 3-4 days | Rapid spread (1 day) |
| Koplik spots | Present (diagnostic) | Absent |
| Contagiousness | Extremely high (R0: 12-18) | Moderate (R0: 6-7) |
| Complications | 30% of cases | Rare except in pregnancy |
What This Means For You
Seek immediate medical care if you or your child develops measles symptoms after potential exposure, especially:
- Fever above 104°F that doesn’t respond to medication
- Difficulty breathing or rapid breathing (sign of measles pneumonia)
- Severe headache with stiff neck (possible measles encephalitis)
- Confusion or altered consciousness (neurological involvement)
- Pregnancy with any measles signs—contact your obstetrician immediately
Early measles diagnosis allows for post-exposure prophylaxis options and prevents community spread during the current measles outbreak 2025.
Understanding Measles Transmission & Contagious Period
Measles ranks as one of the most contagious diseases known to medicine, with a basic reproduction number (R0) between 12-18—meaning one infected person can transmit measles to up to 18 unvaccinated individuals in a susceptible population. This extraordinary transmission efficiency explains why the measles outbreak has spread so rapidly across 44 states despite decades of vaccination efforts.
How Contagious Is Measles? (R0 Value: 12-18 People)
The measles contagious period extends far longer than most realize, creating hidden transmission chains that fuel outbreaks. Infected individuals become measles contagious approximately 4 days before the rash appears and remain infectious until 4 days after rash onset. This 8-day window means people unknowingly spread measles during the prodromal phase when symptoms mimic common cold, making early detection through symptom monitoring critical for outbreak control.
To understand just how measles contagious this virus is, consider these comparisons:
| Disease | R0 Value | Transmission Efficiency |
|---|---|---|
| Measles | 12-18 | 90% of unvaccinated exposed contacts infected |
| COVID-19 (Original) | 2-3 | Significantly lower than measles |
| Influenza | 1-2 | Requires close prolonged contact |
| Ebola | 1.5-2.5 | Requires direct fluid contact |
The measles spread rate demonstrates why vaccination coverage must exceed 96% to prevent outbreaks—any gap in immunity allows rapid viral transmission.
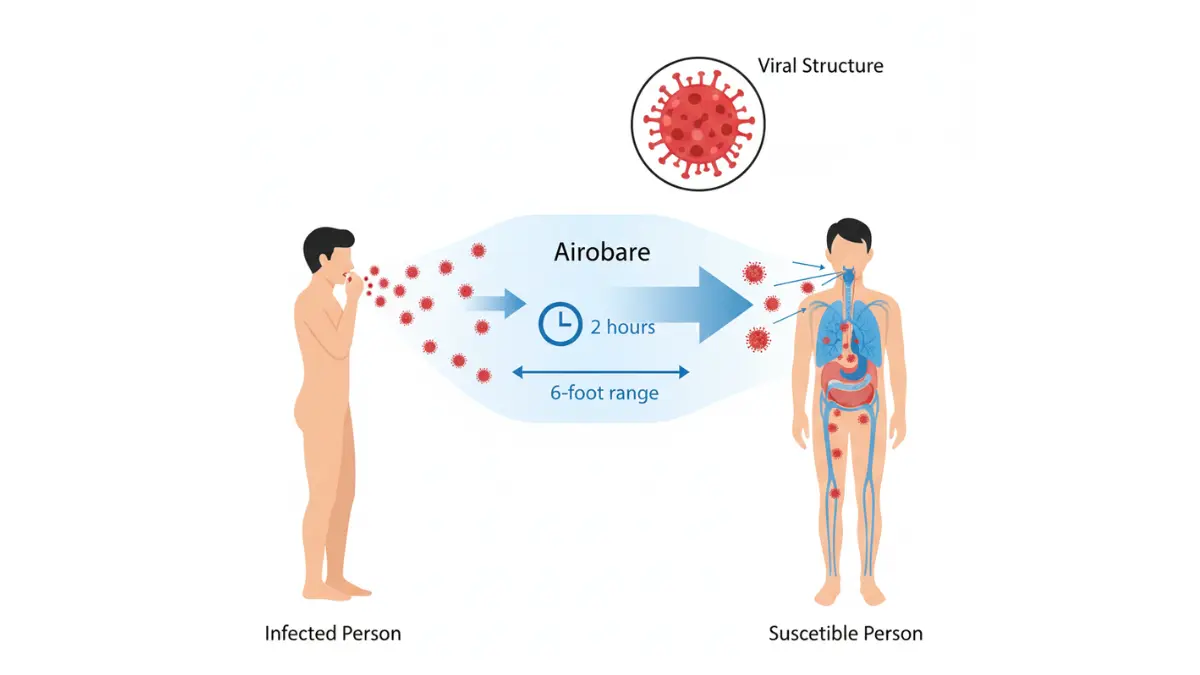
Airborne Transmission: 2-Hour Virus Survival
Unlike diseases requiring direct contact, measles spreads through airborne droplets that remain suspended in the air for up to 2 hours after an infected person leaves a room. This extraordinary survival capacity means measles contagious transmission occurs even without face-to-face contact. A child with measles who coughs in a doctor’s waiting room can infect every susceptible person entering that space for the next two hours.
The airborne nature of measles transmission contrasts sharply with other viral infections like norovirus that primarily spread through contaminated surfaces. Respiratory droplets containing measles virus enter the air when infected individuals:
- Cough or sneeze
- Talk or breathe heavily
- Share enclosed spaces like classrooms, airplanes, or healthcare facilities
When Are You Contagious? (4 Days Before to 4 Days After Rash)
Pre-rash contagious phase (Days -4 to 0): The most dangerous transmission period occurs before the measles rash appears, when infected individuals feel mildly ill but don’t yet realize they have measles. During these 4 days, people continue normal activities—attending school, traveling, visiting public places—unknowingly exposing dozens of contacts.
Rash contagious phase (Days 0 to +4): Once the characteristic rash emerges, patients remain measles contagious for an additional 4 days. Public health authorities require strict isolation during this period to prevent measles spread to vulnerable populations including infants, pregnant women, and immunocompromised individuals.
Pregnant women exposed to measles face heightened risks requiring immediate medical evaluation and potential post-exposure prophylaxis. Women in early pregnancy should track their gestational timeline using our pregnancy weight gain calculator to help healthcare providers assess complication risks if measles exposure occurs.
High-Risk Exposure Settings During Measles Outbreak
The 2025 measles outbreak has demonstrated how quickly measles spreads in high-density environments:
- Airports and airplanes: Recirculated air and prolonged contact with travelers from outbreak regions
- Schools and daycares: Close proximity among unvaccinated children enables rapid transmission
- Healthcare facilities: Emergency rooms treating measles cases expose immunocompromised patients
- Mass transit: Buses, trains, and subways with poor ventilation concentrate airborne virus particles
- Shopping centers and entertainment venues: Brief exposure in crowded spaces sufficient for infection
Understanding these transmission dynamics helps families assess their measles outbreak risk and take appropriate precautions, especially for vulnerable populations with compromised immunity.
What This Means For You
If exposed to someone with confirmed measles:
- Contact your healthcare provider immediately (within 72 hours for potential post-exposure vaccination)
- Quarantine until 21 days after exposure if unvaccinated or immunocompromised
- Monitor for symptoms daily: fever, cough, runny nose, red eyes
- Avoid contact with high-risk individuals: infants, pregnant women, immunocompromised people
The measles contagious nature demands swift action to prevent further measles spread during this unprecedented measles outbreak.
Serious Measles Complications & Who’s Most at Risk
Measles complications occur in approximately 30% of all cases, transforming what some dismiss as a “childhood illness” into a potentially life-threatening medical emergency. The 2025 measles outbreak has resulted in 222 hospitalizations and 3 deaths, with measles hospitalization rates highest among unvaccinated children under 5 and adults over 20.
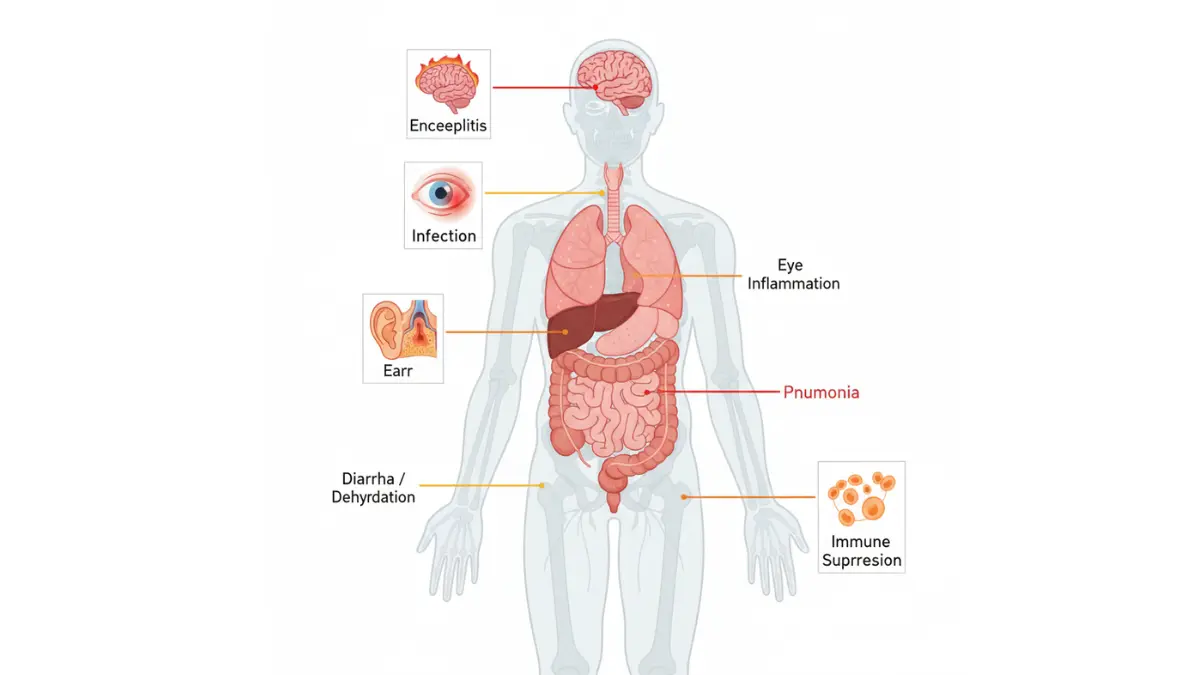
Common Complications: Ear Infections & Diarrhea
Even “mild” measles cases frequently produce complications that require medical intervention. Approximately 1 in 10 children with measles develops otitis media (middle ear infection), which can lead to permanent hearing loss if untreated. Severe diarrhea occurs in about 8% of measles cases, causing dangerous dehydration particularly in young children and infants.
These common measles complications underscore why maintaining proper hydration during infection is critical—families can use our water intake calculator to ensure adequate fluid replacement during the illness recovery period.
Life-Threatening Risks: Pneumonia & Encephalitis
Measles pneumonia represents the most common cause of measles death, occurring in approximately 1 in 20 children who contract the virus. This severe lung inflammation develops when the measles virus damages respiratory tissue, creating secondary bacterial infection opportunities. Symptoms of measles pneumonia include:
- Rapid or labored breathing
- Chest pain or tightness
- Severe persistent cough with mucus production
- Blue-tinged lips or fingernails (cyanosis indicating oxygen deprivation)
- Confusion or decreased alertness
Measles encephalitis (brain inflammation) strikes approximately 1 in 1,000 measles cases, with a mortality rate of 10-15% among those affected. Survivors often face permanent neurological damage including seizure disorders, intellectual disability, and motor function impairment. Warning signs of measles encephalitis include:
- Severe headache unresponsive to pain medication
- Stiff neck or sensitivity to light
- Seizures or convulsions
- Altered consciousness or difficulty waking
- Personality changes or confusion
Long-Term Effects: Immune Memory Erasure
Recent research reveals a disturbing measles complication called “immune amnesia”—the virus erases the immune system’s memory of previous infections, leaving recovered patients vulnerable to diseases they had previously fought off. This immune system reset can persist for 2-3 years after measles infection, increasing susceptibility to bacterial and viral infections that the body once recognized.
Measles Hospitalization Rates in 2025 Outbreak
Current outbreak data shows measles hospitalization occurring in 11.3% of confirmed cases—significantly higher than pre-pandemic rates. Of the 222 hospitalized patients during the 2025 measles outbreak:
- 89% were unvaccinated by choice or medical contraindication
- 7% had received only one MMR dose (incomplete protection)
- 4% were fully vaccinated breakthrough cases (primarily immunocompromised)
The measles death rate remains approximately 1-2 per 1,000 cases in developed countries with advanced medical care, but rises dramatically to 3-6% in developing regions with limited healthcare access.
High-Risk Groups: Children, Pregnant Women, Immunocompromised
| High-Risk Group | Complication Rate | Primary Risks | Evidence Strength |
|---|---|---|---|
| Infants under 12 months | 40-50% | Pneumonia, encephalitis, death | ⭐⭐⭐ Very High |
| Children under 5 years | 30-35% | Ear infections, diarrhea, pneumonia | ⭐⭐⭐ Very High |
| Adults over 20 | 25-30% | Pneumonia, liver inflammation | ⭐⭐⭐ High |
| Pregnant women | 20-25% | Pregnancy loss, preterm birth, maternal death | ⭐⭐⭐ High |
| Immunocompromised | 60-70% | Severe pneumonia, encephalitis, death | ⭐⭐⭐ Very High |
| Malnourished children | 35-45% | Vitamin A deficiency complications | ⭐⭐⭐ High |
Measles in children with underlying health conditions face exponentially higher complication risks. Children with vitamin A deficiency experience more severe measles complications including blindness and fatal respiratory infections. Malnourished children can benefit from nutritional assessment using tools like our BMI calculator to identify deficiencies requiring medical attention.
Pregnant women infected with measles face devastating consequences: spontaneous abortion, stillbirth, preterm labor, and low birth weight babies with increased mortality risk. Maternal measles death rate reaches 6-9% in some populations, particularly in resource-limited settings.
Immunocompromised individuals—including cancer patients, organ transplant recipients, and those with HIV—cannot fight off measles infection effectively. This population experiences atypical presentations with prolonged virus shedding, making measles hospitalization nearly inevitable and measles death rate significantly elevated.
What This Means For You
Monitor closely for these red-flag measles complications requiring emergency care:
- Breathing difficulty (respiratory rate >30 breaths/minute in adults, >40 in children)
- High fever persisting beyond 5 days after rash onset
- Severe dehydration (decreased urination, dry mouth, sunken eyes)
- Neurological symptoms (confusion, seizures, severe headache)
- Pregnancy complications (vaginal bleeding, decreased fetal movement)
Understanding individual risk factors helps families make informed decisions about measles prevention and recognize when measles complications demand immediate medical intervention.
Measles Vaccine: Your Best Protection Against Outbreak
The MMR vaccine (measles, mumps, rubella) remains the most effective measles prevention strategy, providing 97% protection against infection after two doses. During the current measles outbreak, unvaccinated individuals account for 93% of hospitalizations, starkly demonstrating the life-saving power of measles vaccination.
MMR Vaccine Effectiveness: 97% Protection with 2 Doses
A single MMR vaccine dose provides approximately 93% protection against measles, while two doses increase measles immunity to 97%—near-complete protection for most recipients. This two-dose vaccination schedule addresses the small percentage of individuals who don’t develop adequate antibodies after the first shot.
The measles vaccine works by introducing a weakened (attenuated) form of the virus, triggering the immune system to produce protective antibodies without causing disease. These antibodies typically persist for decades, though measles immunity can wane in some individuals—particularly those vaccinated before age 12 months or with only one dose.
Measles Vaccination Schedule for Children & Adults
| Age Group | Dose | Timing | Evidence Strength |
|---|---|---|---|
| Infants (6-11 months) | Early dose (outbreak settings) | Before international travel | ⭐⭐⭐ High |
| Children (12-15 months) | First MMR dose | Routine childhood vaccination | ⭐⭐⭐ Very High |
| Children (4-6 years) | Second MMR dose | Before kindergarten entry | ⭐⭐⭐ Very High |
| Adults (born after 1957) | 1-2 catch-up doses | If no vaccination proof | ⭐⭐⭐ High |
| Healthcare workers | 2-dose series | Occupational requirement | ⭐⭐⭐ Very High |
| International travelers | 2-dose series completion | 28 days between doses | ⭐⭐⭐ High |
The standard measles vaccination schedule recommends the first MMR vaccine at 12-15 months and the second dose at 4-6 years. Adults born after 1957 without vaccination records should receive at least one MMR vaccine dose, with high-risk groups requiring two doses spaced 28 days apart. Understanding personalized vaccination needs may involve genetic risk assessment for individuals with family histories of adverse vaccine reactions.
MMR Vaccine Side Effects: What’s Normal vs Concerning
Most MMR vaccine side effects are mild and temporary, resolving within days. Common reactions include:
- Injection site soreness (20% of recipients)
- Low-grade fever (5-15% within 7-12 days post-vaccination)
- Mild rash (5% of recipients, non-contagious)
- Temporary joint pain (up to 25% of adult women)
Serious MMR vaccine side effects occur extremely rarely—approximately 1 in 1 million doses. These include severe allergic reactions (anaphylaxis), temporary low platelet counts (thrombocytopenia), and febrile seizures in children predisposed to seizure disorders.
Vaccine safety research definitively disproves the discredited autism link, with multiple large-scale studies involving millions of children finding no connection between MMR vaccine and autism spectrum disorders. The original fraudulent study has been retracted, and its author lost medical licensure for ethical violations.
Can You Get Measles If Vaccinated? (Breakthrough Cases)
Breakthrough measles infections occur in approximately 3% of fully vaccinated individuals. These rare cases typically result from:
- Primary vaccine failure: Immune system doesn’t develop adequate antibodies (2-5% of vaccinated individuals)
- Waning immunity: Antibody levels decline over time, particularly decades after vaccination
- Immunocompromised status: Underlying conditions prevent robust immune response despite vaccination
Breakthrough cases generally present with milder symptoms, shorter duration, and significantly lower complication rates compared to infections in unvaccinated individuals. Even when measles vaccine doesn’t prevent infection entirely, it dramatically reduces measles hospitalization risk and prevents measles death.
How to Prevent Measles Without Vaccine (High-Risk Settings)
For individuals who cannot receive the measles vaccine due to medical contraindications, measles prevention strategies include:
- Avoid exposure: Stay away from outbreak areas and crowded public spaces during measles outbreaks
- Isolation protocols: Immediately quarantine if exposed to confirmed measles cases
- Hand hygiene: Frequent handwashing, though less effective than for other diseases due to airborne transmission
- Immune globulin: Post-exposure prophylaxis for eligible high-risk individuals
- Herd immunity reliance: Protection occurs when 96%+ of community receives MMR vaccine
Supporting overall immune function through adequate protein intake and nutrition helps the body mount effective vaccine responses and fight infections more successfully.
Post-Exposure Prophylaxis: 72-Hour Vaccine Window
Measles prevention remains possible even after exposure through timely intervention:
MMR vaccine within 72 hours of exposure: Can prevent or significantly reduce disease severity in previously unvaccinated individuals. This window represents a critical opportunity for measles prevention when exposure occurs.
Immune globulin (IG) within 6 days of exposure: Provides temporary passive immunity for pregnant women, infants, and immunocompromised individuals who cannot receive live vaccines. IG contains measles antibodies collected from blood donors, offering 2-3 weeks of protection.
| Prevention Method | Effectiveness | Best For | Timing |
|---|---|---|---|
| MMR vaccine (post-exposure) | 70-90% if given quickly | Unvaccinated healthy individuals | Within 72 hours |
| Immune globulin | 80-90% temporary protection | High-risk contraindications | Within 6 days |
| Standard MMR schedule | 97% with 2 doses | Routine prevention | Before exposure |
| Quarantine | 100% if compliance perfect | All unvaccinated exposed | 21 days post-exposure |
What This Means For You
If you’ve never been vaccinated or lack documentation:
- Schedule MMR vaccine immediately—the 2025 measles outbreak creates urgent need
- Consider checking your comprehensive vaccination status for other preventable diseases
- Two doses provide optimal measles immunity; one dose leaves 7% vulnerable
If recently exposed to measles:
- Contact healthcare provider within 24 hours for post-exposure options
- MMR vaccine within 72 hours can still prevent infection
- Immune globulin available for those who cannot receive vaccines
The measles vaccine represents the single most effective how to prevent measles strategy, with decades of safety data and proven community protection.
Measles Treatment Options & Home Care Guidelines
No specific antiviral medication cures measles—measles treatment focuses entirely on supportive care to manage symptoms and prevent complications while the immune system fights the virus. Recovery typically takes 2-3 weeks from initial symptom onset, though fatigue and cough may persist longer.
Why There’s No Measles Cure (Supportive Care Approach)
Unlike bacterial infections treatable with antibiotics, measles remains a viral infection requiring the body’s natural immune response for clearance. The supportive care approach emphasizes symptom relief, adequate nutrition, hydration maintenance, and close monitoring for complications that may require hospitalization.
Home Treatment: Managing Fever, Cough & Rash
Effective measles treatment at home includes several evidence-based strategies:
- Fever management: Acetaminophen or ibuprofen for measles fever reduction (never aspirin in children due to Reye’s syndrome risk)
- Hydration: Increased fluid intake to prevent dehydration from fever and diarrhea—calculate personalized needs using our water intake calculator
- Rest: Adequate sleep supports immune function; determine optimal rest periods with our sleep calculator for recovery phases
- Cough relief: Cool-mist humidifier to ease respiratory symptoms and soothe irritated airways
- Eye care: Dim lighting and cool compresses for light-sensitive, inflamed eyes
- Isolation: Stay home until 4 days after rash appears to prevent measles spread
Vitamin A Supplementation: Clinical Guidelines
Vitamin A measles supplementation reduces complication severity, particularly in children with deficiency or those hospitalized with severe disease. The World Health Organization recommends vitamin A for all children diagnosed with measles in communities where vitamin A deficiency is prevalent or measles death rate exceeds 1%.
Dosing guidelines from the CDC’s measles clinical management protocols:
- Infants under 6 months: 50,000 IU orally once daily for 2 days
- Children 6-11 months: 100,000 IU orally once daily for 2 days
- Children 12 months and older: 200,000 IU orally once daily for 2 days
- Children with vitamin A deficiency signs: Third dose 4-8 weeks later
Important warning: Pregnant women should NOT take high-dose vitamin A measles supplementation due to birth defect risks. Doses exceeding 10,000 IU daily during pregnancy can cause fetal abnormalities.
When to Seek Emergency Medical Care
Certain red-flag symptoms indicate measles complications requiring immediate medical evaluation:
| Warning Sign | Possible Complication | Action Required |
|---|---|---|
| Difficulty breathing or rapid breathing | Measles pneumonia | Emergency room immediately |
| Severe headache with stiff neck | Measles encephalitis | Call 911 or emergency services |
| Confusion or altered consciousness | Brain inflammation | Emergency room immediately |
| High fever >5 days after rash | Secondary bacterial infection | Contact healthcare provider urgently |
| Severe dehydration (no urination 8+ hours) | Dehydration shock | Emergency room immediately |
| Seizures or convulsions | Febrile seizure or encephalitis | Call 911 or emergency services |
| Blue lips or fingernails | Severe oxygen deprivation | Emergency room immediately |
What This Means For You: Creating a Home Care Plan
Measles 2025 home management checklist:
✓ Stock fever reducers (acetaminophen/ibuprofen—check with our pill identifier for proper medication)
✓ Ensure adequate hydration (8-10 glasses daily for adults, adjusted for children)
✓ Create isolated recovery space (separate bedroom with minimal light)
✓ Monitor temperature 3-4 times daily (log patterns for healthcare provider)
✓ Watch for complication warning signs (breathing changes, neurological symptoms)
✓ Maintain isolation until 4 days after rash appears
✓ Notify close contacts immediately for post-exposure prophylaxis opportunities
Recovery from measles typically requires 10-14 days from rash onset, though immune system restoration takes 2-3 years due to immune amnesia effects. Families should monitor for increased susceptibility to other infections during this extended vulnerable period.
Final Disclaimer
This article is for educational purposes only and does not constitute medical advice. Measles diagnosis, treatment, and prevention decisions should be made in consultation with qualified healthcare providers. If you suspect measles exposure or infection, contact your doctor immediately for personalized guidance. The information presented reflects current CDC guidelines as of December 2025 but may be updated as new evidence emerges.
Frequently Asked Questions about Measles outbreak cases
1. How many measles cases are there in 2025?
As of December 17, 2025, there are 1,958 confirmed measles cases across 44 U.S. states, with 222 hospitalizations and 3 deaths reported—the highest number since 1992.
2. What are the first signs of measles?
The first measles symptoms include high fever (103-105°F), dry cough, runny nose, and watery red eyes appearing 7-14 days after exposure, followed by Koplik spots in the mouth 2-3 days before the rash.
3. How contagious is measles?
Measles is extremely contagious—one infected person can spread measles to 12-18 unvaccinated individuals. You’re contagious 4 days before until 4 days after the rash appears, and the virus survives in air for 2 hours.
4. Can you get measles if you’re vaccinated?
Yes, but rarely. Breakthrough infections occur in about 3% of fully vaccinated people due to waning immunity or primary vaccine failure, but these cases are typically much milder with fewer complications.
5. What does measles rash look like?
Measles rash appears as flat red spots that merge into larger blotches, starting at the hairline and face, then spreading downward to the neck, trunk, arms, and legs over 3-4 days.
6. Is there a cure for measles?
No, there’s no antiviral cure for measles. Treatment focuses on supportive care including fever reducers, hydration, rest, and monitoring for complications like pneumonia or encephalitis.
7. How effective is the MMR vaccine?
The MMR vaccine is 93% effective after one dose and 97% effective after two doses at preventing measles infection, making it the most reliable measles prevention method available.
8. What are the serious complications of measles?
Serious measles complications include pneumonia (1 in 20 cases), encephalitis or brain inflammation (1 in 1,000), permanent hearing loss, and death (1-2 per 1,000 cases in developed countries).
9. Can adults get measles?
10. Should I get the measles vaccine during an outbreak?
11. How long does measles last?
Measles symptoms typically last 7-10 days from initial fever to rash fading, with complete recovery taking 2-3 weeks. However, immune system vulnerability persists for 2-3 years due to immune memory erasure.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.