On This Page – Quick Medical Summary
Melanoma is the deadliest form of skin cancer, originating in melanocytes — the pigment-producing cells of the skin. It accounts for only about 1% of all skin cancers but causes the overwhelming majority of skin cancer deaths. When detected early, the five-year survival rate reaches 99%. When it spreads to distant organs, that rate drops to approximately 35%. This guide covers everything — from the first warning signs to 2026’s most advanced treatment breakthroughs.
What Is Melanoma? The Cancer That Kills One American Every Hour
A Diagnosis Nobody Expects
In 2021, Marcus, a 34-year-old high school football coach from Nashville, Tennessee, noticed a small dark spot on his upper back during a routine shower. It had always been there — or so he thought. Over eight weeks, it changed from a flat, uniform brown spot into something irregular, asymmetric, and darker at the edges.
His wife noticed it first. She photographed it. Compared it to photos from three months earlier.
It was different.
Marcus saw a dermatologist the next week. A punch biopsy followed. Three days later, the call came: Stage IB melanoma. He was 34 years old, athletic, and had no family history of cancer.
Within six weeks of that phone call, Marcus had surgery. A wide local excision removed the tumor with clean margins. A sentinel lymph node biopsy came back negative.
Today, Marcus is cancer-free. He speaks at schools across Tennessee about skin self-exams.
His story is not unique — but his outcome depended entirely on one decision: not waiting.
What Is Melanoma? The Direct Answer
Melanoma is a type of skin cancer that develops when melanocytes — the cells responsible for producing the pigment melanin — undergo DNA mutations that cause uncontrolled, invasive growth.
Melanin gives skin, hair, and eyes their color. When UV radiation from the sun or tanning beds damages melanocyte DNA, these mutations can trigger a cascade that turns normal pigment cells into life-threatening cancer.
What makes melanoma uniquely dangerous is its metastatic potential — the speed and frequency with which it spreads to distant organs, including the lungs, liver, brain, and bone, long before it causes visible symptoms in those areas.
You can also use our Symptom Checker tool to evaluate any unusual skin changes you’re concerned about.
Melanoma vs. Other Skin Cancers: Why It Stands Apart
Most skin cancers are curable and slow-growing. Melanoma is the exception.
| Feature | Melanoma | Basal Cell Carcinoma | Squamous Cell Carcinoma |
|---|---|---|---|
| Share of skin cancers | ~1% | ~75–80% | ~15–20% |
| Metastatic risk | Very High | Very Rare | Rare |
| 5-year survival (early) | 99% | 99%+ | ~95% |
| 5-year survival (metastatic) | ~35–50% | Very rare | ~25% |
| Annual US deaths (2026) | ~8,510 | Very Rare | ~2,000+ |
| Growth speed | Fast | Slow | Moderate |
| Primary cause | UV radiation + genetics | UV radiation | UV radiation |
Basal cell and squamous cell carcinomas, while more common, rarely spread beyond the skin. Melanoma, by contrast, can invade the lymphatic system and bloodstream within weeks of becoming invasive, making early detection an absolute medical necessity — not a preference.
2026 Melanoma Statistics: The Numbers That Demand Your Attention
According to American Cancer Society Facts & Figures 2026:
- ~112,000 new melanoma diagnoses will occur in the United States in 2026
- ~65,400 will be in men and ~46,600 in women
- ~8,510 people will die from melanoma in 2026
- Melanoma death rates dropped rapidly from 2013 to 2022 — largely due to immunotherapy advances
- Melanoma incidence has tripled in the past 30 years
- It is one of the most common cancers in adults under 30, particularly young women
Global burden: Worldwide, approximately 325,000 new melanoma cases are diagnosed annually. Australia and New Zealand carry the highest per-capita rates globally, followed by Scandinavia, the United States, and parts of Western Europe.
Racial disparities in outcomes: Data from the Skin Cancer Foundation shows a stark survival gap — the estimated five-year melanoma survival rate for Black patients is approximately 70%, compared to 95% for White patients. This gap is driven primarily by later-stage diagnosis, not by biological differences, making awareness in all communities a life-or-death issue.
Why Melanoma Incidence Is Rising — Especially in Young Adults
Several converging factors explain why melanoma rates, while declining in some groups, continue rising in others:
- Indoor tanning bed use — classified as a Group 1 carcinogen by the World Health Organization (WHO)
- Cumulative UV damage starting in childhood and adolescence
- Increased outdoor recreation without adequate protection
- Ozone layer changes affecting UV radiation levels
- Greater awareness + screening revealing previously undetected cases
Tanning bed use before age 35 increases melanoma risk by approximately 75%, according to research reviewed by international oncology bodies. For young women aged 20–39, this correlation is particularly strong.
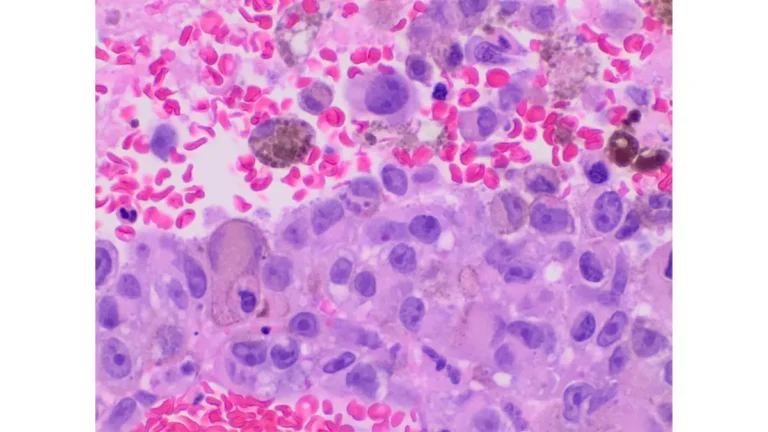
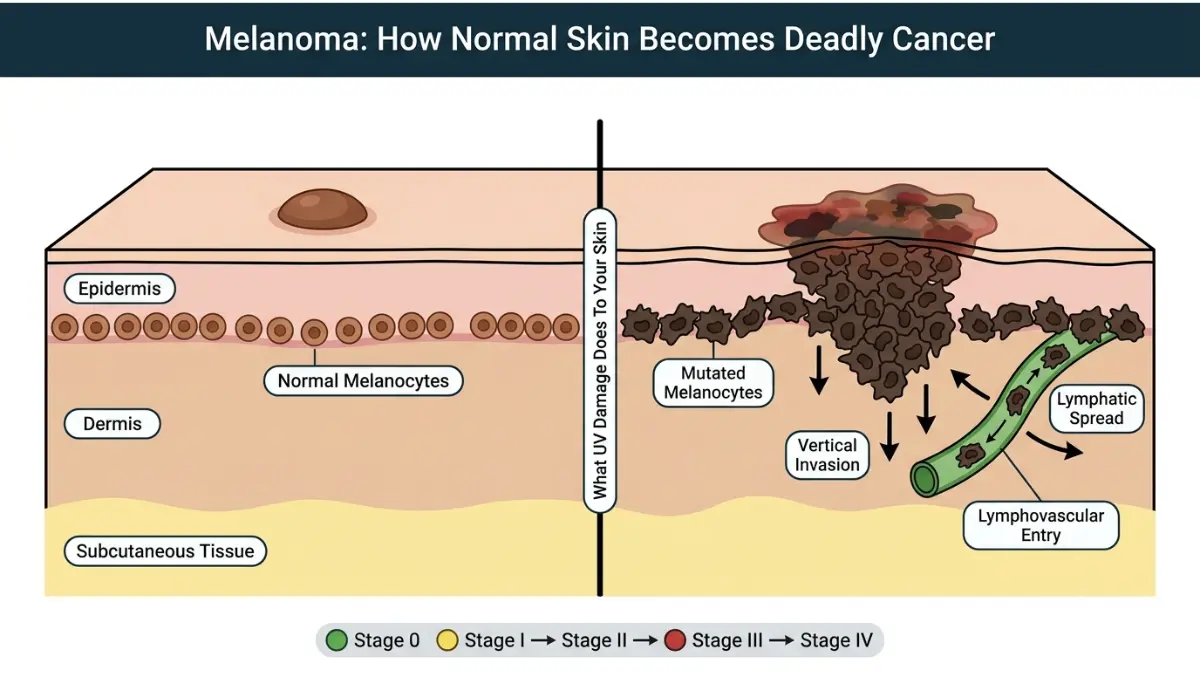
How Melanoma Forms: The Biology Made Simple
Every melanoma begins at the cellular level.
Step 1 — UV damage: Ultraviolet radiation (UVA and UVB) penetrates skin cells and damages the DNA within melanocytes.
Step 2 — Mutation accumulation: Critical tumor-suppressor genes are inactivated. Oncogenes — particularly the BRAF gene (mutated in ~50% of melanomas) — become overactive, driving uncontrolled cell division.
Step 3 — Radial growth: The abnormal melanocytes begin spreading outward along the skin’s surface (epidermis) — this is often the “flat, slowly spreading” phase visible as a changing mole.
Step 4 — Vertical invasion: The tumor breaks through the basement membrane and invades deeper skin layers (dermis), blood vessels, and lymphatics. This is when metastatic risk becomes real.
Step 5 — Distant spread: Via the lymphatic system and bloodstream, melanoma cells travel to regional lymph nodes, and then potentially to the lungs, liver, brain, and bone.
The window between Steps 1–2 and Steps 4–5 is your opportunity for cure. At Step 4, treatment becomes dramatically more complex. At Step 5, it becomes a fight for survival.
Three Reading Modes (Choose Your Level)
We’ve structured this guide for three audiences:
📗 Simple Summary — Plain language for patients and families. Look for the “What This Means For You” callout boxes.
📘 Standard — The main article text, written for the general public with clear explanations of medical terms.
📕 Clinical Deep-Dive — Advanced tables, guideline references, mutation classifications, and treatment algorithms — embedded throughout for healthcare providers.
Deadly Symptoms — How to Spot Melanoma Before It Kills You
The First Rule: Any Change Demands Attention
The single most important thing to understand about early melanoma symptoms is this: it’s change, not appearance, that saves lives.
A mole that has looked unusual your entire life is far less dangerous than a normal-looking mole that is changing. The evolving nature of a lesion — new growth, color shift, shape change, or new symptoms like itching or bleeding — is the most critical warning signal.
Every year, thousands of melanoma cases are missed because patients and even clinicians assume that because a spot “has always been there,” it is safe. That assumption kills people.
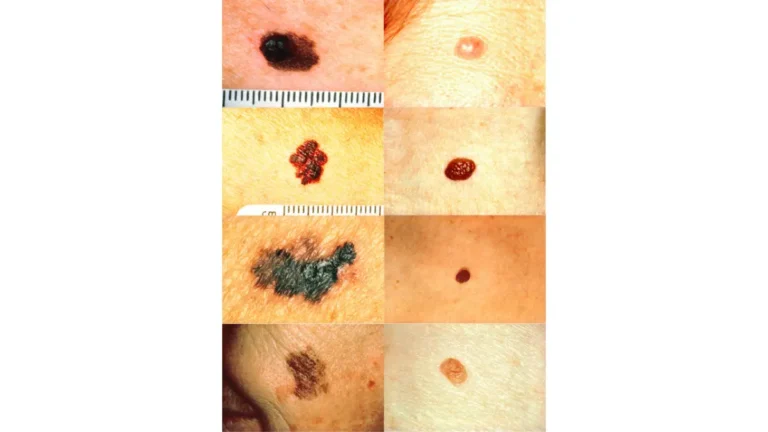
The ABCDE Rule: Your Complete 2026 Guide
The ABCDE rule, endorsed by the American Academy of Dermatology (AAD), remains the gold-standard visual guide for identifying suspicious lesions.
But what competitors don’t tell you — and what dermatologists know — is that E (Evolving) is the most important letter of all.
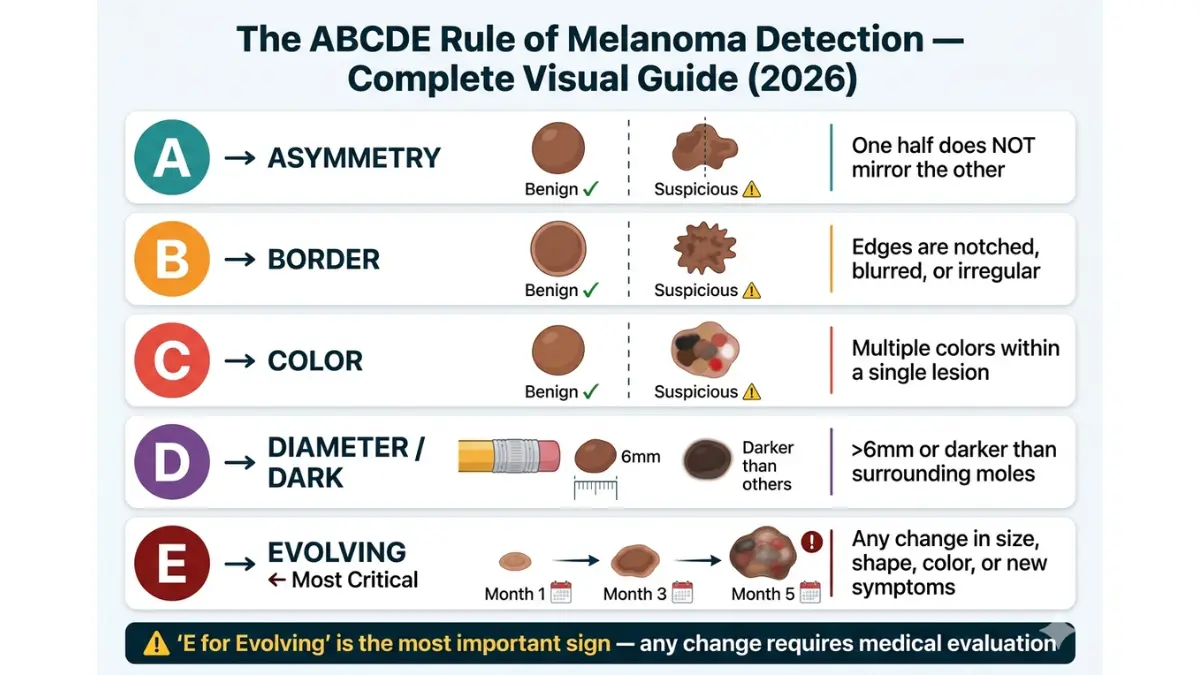
A — Asymmetry
Draw an imaginary line through the center of a mole. In a benign mole, both halves should roughly mirror each other.
In melanoma, the two halves are mismatched — one side may be darker, raised, or irregularly shaped compared to the other.
Clinical note: Asymmetry alone is not diagnostic — but asymmetry combined with any other ABCDE feature warrants urgent dermatological evaluation.
B — Border Irregularity
Normal moles have smooth, clearly defined borders.
Melanoma borders are often:
- Notched or scalloped
- Blurred or indistinct, fading into surrounding skin
- Jagged or irregular in outline
- Uneven on one side
What to check: Use a magnifying glass if needed. The edges of a concerning lesion may look like they’re “bleeding” pigment into the surrounding skin.
C — Color Variation
A uniform brown mole is generally less concerning. Melanoma often displays multiple colors within a single lesion.
Colors that may appear within a melanoma include:
- Shades of brown, tan, and black
- Red (inflammatory reaction or vascular involvement)
- White (areas of regression or fibrosis)
- Blue or dark blue (deeply pigmented cells or hemorrhage)
- Pink (particularly in amelanotic variants)
The more colors present within a single spot, the more urgently it needs evaluation.
D — Diameter or Dark
The traditional “D” stands for diameter — lesions larger than 6mm (the size of a pencil eraser) are considered a warning sign.
However, many dermatologists now emphasize “D for Dark” as equally important. A lesion that is dramatically darker than all your other moles — regardless of size — deserves scrutiny.
Important: Many melanomas are found when smaller than 6mm. Size alone is not reassuring. A growing lesion of any size requires evaluation.
E — Evolving (The Most Critical Factor)
This is the single most important ABCDE criterion, and the one most commonly overlooked.
Any spot on your skin that is new, changing, or behaving differently from your other moles represents an urgent call to action.
Evolving changes include:
- Growing larger over weeks or months
- Changing color, shape, or texture
- Developing a raised area within a previously flat lesion
- Beginning to itch, tingle, or feel tender
- Starting to bleed or crust without trauma
- Becoming elevated or firm
The key timeframe: Changes occurring over 4–8 weeks are particularly concerning. Slow changes over years are less urgent but still warrant annual monitoring.
The Ugly Duckling Sign: What the ABCDE Rule Misses
The Ugly Duckling sign is a complementary detection strategy that catches what ABCDE sometimes misses.
The concept: Most moles on a person’s body tend to resemble one another — they form a “pattern.” The Ugly Duckling is any mole that looks distinctly different from the rest. It might be larger, smaller, darker, lighter, or shaped differently than your other moles.
The strategy is especially important for:
- People with many moles (more than 50)
- Patients with dysplastic (atypical) moles
- Cases where a lesion doesn’t fit the classic ABCDE criteria but still “stands out”
How to apply it: During your monthly skin exam, mentally compare each lesion to your “average” mole. Anything that looks like an outsider — a lesion that doesn’t belong — should be evaluated.
An isolated lesion with no neighboring moles for comparison is automatically considered an Ugly Duckling.
7 Additional Warning Signs Doctors Check For (Beyond ABCDE)
The ABCDE rule doesn’t capture every melanoma presentation. Here are seven additional symptoms that warrant prompt medical evaluation:
- A lesion that persistently itches, bleeds, or crusts without any trauma or obvious cause
- A rapidly growing raised bump — particularly one that appears within days to weeks (classic nodular melanoma presentation)
- Pigment spreading beyond the border of an existing mole into the surrounding skin
- A sore that refuses to heal within three to four weeks
- Satellite lesions — small dark spots appearing near an existing mole
- A dark streak running beneath a nail (subungual melanoma) — often mistaken for a bruise
- A pink, red, or skin-colored growth with no dark pigmentation — this is amelanotic melanoma, and it is the most commonly missed presentation in all of clinical dermatology
Amelanotic Melanoma: The Invisible Killer
Amelanotic melanoma lacks the dark brown or black pigment that most people associate with skin cancer. Instead, it appears as:
- A pink or reddish bump
- A flesh-colored raised nodule
- A sore that looks like a cyst or pimple that won’t heal
- A pale, colorless growth that looks completely benign
This is why amelanotic melanoma carries a worse average prognosis than pigmented melanoma — by the time it’s recognized, it is typically at a more advanced stage.
Who gets it: Amelanotic melanoma can affect anyone but is more commonly seen in nodular melanoma subtypes and in patients with very fair skin.
What to do: If you have a pink or red growth that is growing or not healing within three to four weeks — regardless of whether it looks dark — it needs a dermatologist’s evaluation.
You can also review our comprehensive guide on skin cancer warning signs and symptoms to understand the full spectrum of skin cancer presentations.
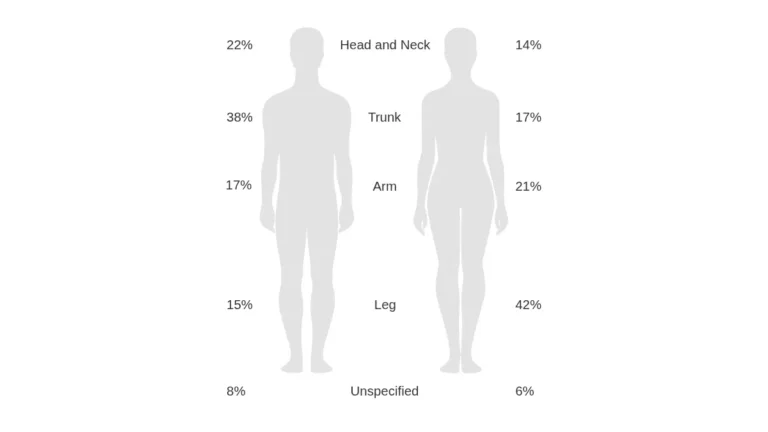
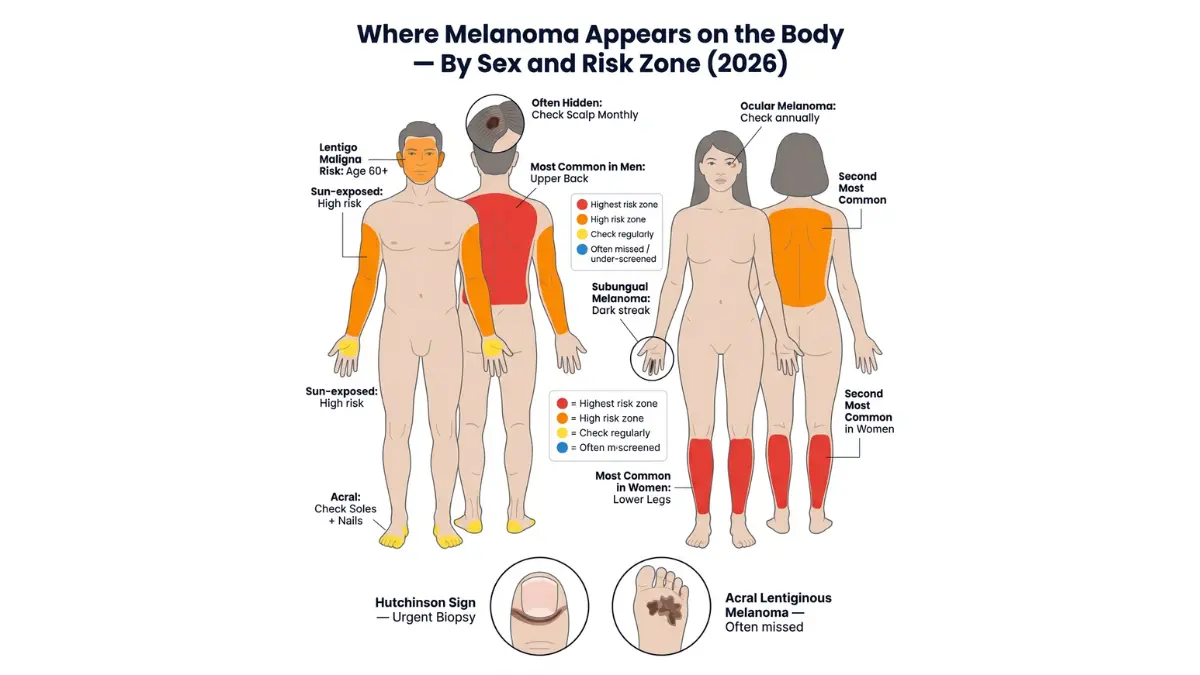
Melanoma Symptoms by Body Location
Where melanoma appears varies significantly by sex, age, and skin type.
| Body Location | Most Common In | What to Look For |
|---|---|---|
| Upper back / trunk | Men | Large, irregular dark patch changing over weeks |
| Legs (below knee) | Women | Flat, spreading lesion; often fair-skinned women |
| Palms and soles | People of color | Dark irregular streak; often late-detected |
| Under fingernails/toenails | All | Dark longitudinal band (hutchinson sign at nail fold) |
| Face, ears, scalp | Older adults 60+ | Flat tan/brown slowly expanding spot (lentigo maligna) |
| Scalp | All — especially men with thinning hair | Part hair regularly; use a partner or mirror |
| Eyes | All | Blurred vision, visual field loss, dark spot in eye |
| Mouth, genitals, rectum | All | Persistent dark or irregular mucous membrane lesion |
Melanoma Symptoms by Skin Type: The Fitzpatrick Scale
One of the largest gaps in competitor content is the failure to describe how melanoma presents differently across skin tones. This matters enormously for the ~40% of the US population with skin of color.
Fitzpatrick Types I–III (Fair to Medium Skin)
- Classical ABCDE presentation more visible
- Pigmented lesions generally contrast well with skin
- Sun-exposed areas (face, shoulders, back, arms) are highest risk
Fitzpatrick Types IV–VI (Olive to Dark Brown to Black Skin)
- Acral lentiginous melanoma is the most common subtype — occurs on palms, soles, and nail beds
- Mucosal melanoma (mouth, genitals, anal canal) occurs at higher rates
- Lesions are often amelanotic (no dark color), making visual detection harder
- Diagnosis comes on average 1.5–2 stages later in patients with darker skin — driven by lower awareness, less dermatological access, and different clinical presentation
- Subungual melanoma (under nails) represents a disproportionate share of melanomas in Asian and Black patients
What this means for all patients: Do not assume you are “low risk” based on skin tone. Melanoma in darker skin is often found later, which is precisely why self-awareness and regular skin checks are equally critical regardless of Fitzpatrick type.
Advanced Symptoms: What Metastatic Melanoma Feels Like
When melanoma reaches Stage III or IV and begins spreading beyond the skin, symptoms may include:
Lymph node involvement (Stage III):
- Swollen, firm, painless lymph node — commonly in the groin, armpit, or neck
- Hard lump beneath the skin near the primary tumor site
Lung metastases:
- Persistent dry cough
- Shortness of breath with minimal exertion
- Chest pain or discomfort
Liver metastases:
- Right-sided abdominal discomfort or fullness
- Jaundice (yellowing of skin/eyes) — often late sign
- Unexplained weight loss, fatigue
Brain metastases (melanoma has one of the highest rates of brain spread of any cancer):
- Persistent headaches, especially upon waking
- Seizures with no prior history
- Sudden confusion, memory changes
- Visual disturbances, speech difficulty
Bone metastases:
- Deep bone pain — often in spine, pelvis, or long bones
- Pathological fracture (fracture from minimal trauma)
Systemic symptoms (any advanced stage):
- Significant unintentional weight loss
- Severe fatigue unrelieved by rest
- Loss of appetite
- Brown or black urine (rare — melanin released into blood)
How to Perform a Monthly Self-Skin Examination
The Skin Cancer Foundation recommends performing a thorough skin self-examination monthly.
What you need:
- Full-length mirror
- Handheld mirror (for hard-to-see areas)
- Bright, consistent lighting
- A partner or family member for back and scalp checks
Step-by-step protocol (10 minutes):
- Face and scalp first — examine the face, ears, and neck under good light. Use a comb to part hair in sections to check the scalp.
- Arms and hands — examine both sides of arms, elbows, and between fingers and fingernails.
- Torso — examine chest, abdomen, breasts/nipples (in all genders). Use the handheld mirror for the lower back and sides.
- Back — use the full-length mirror and handheld mirror in combination, or have a partner check.
- Lower body — examine buttocks, genitals, and perineal area.
- Legs and feet — examine all surfaces, including between toes and beneath toenails.
- Photograph suspicious spots — use your smartphone to document any lesion you’re monitoring. Compare photos monthly.
When to see a dermatologist immediately (within 1–2 weeks):
- Any new mole or spot appearing after age 25
- Any mole that has visibly changed within 4–8 weeks
- Any lesion showing ABCDE criteria
- Any non-healing sore after 3–4 weeks
- Any dark streak under a nail that wasn’t caused by trauma
Annual professional skin check: Regardless of self-exam findings, anyone with a history of significant UV exposure, tanning bed use, 50+ moles, or a family history of melanoma should have a full-body skin check by a dermatologist annually.
✅ What This Means For You
If you’ve found a changing mole, don’t wait for your next routine appointment. Call a dermatologist and describe what you’re seeing. Most dermatologists prioritize suspected melanoma cases for rapid evaluation. Waiting even 30 extra days increases your risk. Early action costs you 20 minutes at a dermatologist’s office. Delay can cost your life.
Types of Melanoma — The 4 Deadly Variants and Their Hidden Differences
Why Type Matters as Much as Stage
Most patients learn their melanoma stage but never fully understand their melanoma type. This is a clinical gap that matters.
Different melanoma subtypes have different growth patterns, different locations, different risk populations, and critically — different early warning presentations. Understanding your type helps you understand your risk, your biopsy approach, and even your treatment options.
There are four major types of cutaneous melanoma and several rare variants.
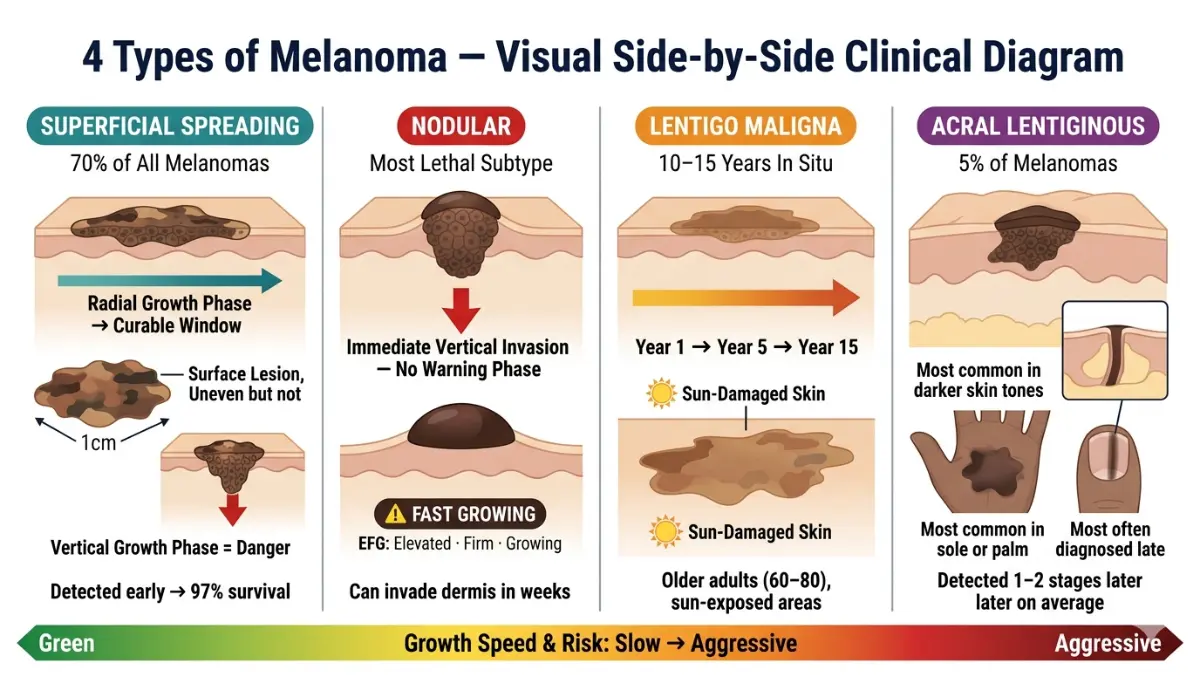
The 4 Major Types: Head-to-Head Comparison
| Subtype | Frequency | Most Common In | Where It Appears | Growth Pattern | Detection Difficulty |
|---|---|---|---|---|---|
| Superficial Spreading | ~70% | All adults | Anywhere on body | Slow horizontal → rapid vertical | Moderate |
| Nodular | ~15–20% | Men 50+; also younger | Trunk, head, neck | Immediately vertical — no warning phase | Very High |
| Lentigo Maligna | ~5–10% | Adults 60–80 | Sun-damaged face, ears, arms | Very slow horizontal (years) | Low-Moderate |
| Acral Lentiginous | ~2–5% | People of color; all ethnicities | Palms, soles, nail beds | Moderate horizontal → vertical | Very High |
Superficial Spreading Melanoma: The Most Common Type
Superficial spreading melanoma (SSM) accounts for approximately 70% of all melanoma diagnoses. It is the most recognizable subtype and, when caught in its early phases, carries an excellent prognosis.
Growth behavior:
SSM characteristically grows outward along the skin’s surface for a period of months to years — the radial growth phase. During this phase, it is most amenable to simple surgical cure.
At some point, often without warning, it transitions to a vertical growth phase, invading deeper skin layers and dramatically increasing metastatic risk.
What it looks like:
- Flat or slightly raised lesion
- Irregular, asymmetric outline
- Multiple colors — often brown, black, pink, white, or gray within the same lesion
- Often 1–3cm in diameter at presentation
- Typically located on the back (men) or legs (women)
The critical window: SSM gives you a relatively generous detection window during its horizontal growth phase. This is why regular skin exams and the ABCDE framework are so effective for this type. The patients who die from SSM are predominantly those who ignore the changing mole for 12–24 months.
Nodular Melanoma: The Silent, Fast Killer
Nodular melanoma (NM) is responsible for approximately 15–20% of diagnoses but a disproportionately high percentage of melanoma deaths.
This subtype is lethal because it breaks every rule.
What makes it uniquely dangerous:
Unlike SSM, nodular melanoma skips the horizontal growth phase entirely. From its very first cell division, it grows downward — invasively and aggressively.
By the time it is large enough to be noticed, it may already be >2mm thick with early lymphatic spread.
The EFG Rule — your emergency guide for nodular melanoma:
Dermatologists use a supplementary rule for nodular melanoma identification:
- E — Elevated (always raised above skin level, often dome-shaped)
- F — Firm (hard to the touch, unlike a soft lipoma or cyst)
- G — Growing (visibly increasing over weeks, not months)
What it looks like:
- A dark brown, black, or blue dome-shaped nodule
- Often amelanotic — pink or red with no pigmentation
- May appear as a large, rapidly growing pimple or cyst
- Often bleeds with minimal contact
- Size: typically 1–2cm at diagnosis, but already invasive
- Location: most common on the trunk, head, and neck in men
Who gets it: More common in men over 50, but can occur at any age. The risk of misdiagnosis as a cyst, keloid, or pyogenic granuloma is extremely high, which is why many nodular melanoma cases are found at advanced stages.
What this means for you: Any rapidly growing skin bump — regardless of color, regardless of whether it looks “like melanoma” — that is elevated, firm, and growing over 4–6 weeks requires biopsy. Do not wait. Do not accept reassurance without a biopsy when this pattern is present.
Lentigo Maligna Melanoma: The Slow Burn
Lentigo maligna melanoma (LMM) is one of the most forgiving melanoma subtypes in terms of natural history — but also one of the most frequently undertreated.
It begins as lentigo maligna — a flat, tan-to-brown in situ lesion confined to the epidermis. Lentigo maligna can remain non-invasive for 10–15+ years. When it finally invades the dermis, it becomes lentigo maligna melanoma.
What it looks like:
- Large, flat, irregularly shaped patch
- Tan, brown, or multiple shades of brown
- Slow, gradual expansion over years
- Often located on the face (nose, cheeks), ears, or dorsal forearms
- Borders blend somewhat into surrounding sun-damaged skin, making them difficult to define
- Average size at diagnosis: 3–5cm — considerably larger than other subtypes
Who gets it: LMM is most common in adults aged 60–80, predominantly in those with extensive lifetime sun damage and Fitzpatrick skin types I–III.
Treatment nuance: Standard wide local excision can be challenging for LMM because margins on the face are cosmetically sensitive. Mohs micrographic surgery is often preferred. Radiation therapy is an effective alternative for elderly patients who are not ideal surgical candidates.
Acral Lentiginous Melanoma: The Hidden Killer in Skin of Color
Acral lentiginous melanoma (ALM) is the most important melanoma subtype for American patients of color to understand — yet it receives the least attention in mainstream health content.
What “acral” means: “Acral” refers to the extremities — specifically the palms, soles, and digits. ALM occurs almost exclusively in these locations, which:
- Receive minimal UV exposure
- Are rarely inspected during routine skin checks
- Have no natural tanning response to warn of UV damage
Where it hides:
- The sole of the foot (most common location, especially the arch and heel)
- The palm of the hand
- Beneath fingernails or toenails (subungual ALM)
- Around nail folds
What it looks like:
- A dark, irregularly shaped patch on the palm or sole
- Often begins as a tan or brown streak, gradually darkening
- Subungual: a dark longitudinal band running the length of the nail — the Hutchinson sign (when pigment extends onto the nail fold) is highly suspicious
- May mimic a fungal infection, bruise, or callus — the three most common misdiagnoses
The racial disparity crisis:
ALM accounts for about 2–5% of melanomas in White patients — but it is the most common subtype in Black, Asian, and Hispanic populations. However, its incidence is not higher in these populations — it simply makes up a larger proportion of their total melanoma burden.
The critical problem is not incidence but stage at diagnosis. Multiple studies confirm that Black and Asian patients with ALM are diagnosed, on average, 1.5–2 stages later than White patients with any melanoma type. This is driven by:
- Lower awareness that melanoma can occur on sun-protected skin
- Less frequent dermatological care due to healthcare access barriers
- Physician bias — less clinical suspicion in darker-skinned patients
- Later presentation of ALM (it grows more slowly than nodular melanoma)
This disparity explains the significant survival gap described earlier.
What this means for all patients: Check your palms, soles, and nails monthly. Any dark streak under a nail that was not caused by a verified injury — especially one that is growing, widening, or extending onto the skin around the nail — requires biopsy.
Rare Melanoma Subtypes
Beyond the four primary types, several less common but clinically significant subtypes exist:
Desmoplastic melanoma:
- Neurotropic (grows along nerves), associated with perineural invasion
- Often amelanotic (non-pigmented), making visual identification very difficult
- Most common on sun-damaged face and neck
- High local recurrence risk; wider margins required
- Often requires adjuvant radiation therapy
Mucosal melanoma:
- Arises on mucous membranes — oral cavity, nasal passages, GI tract, vulva, vagina, penis, anal canal
- Accounts for ~1% of all melanomas but carries a significantly worse prognosis (5-year survival ~25%)
- Extremely rare UV contribution; likely driven by chronic inflammation and genetic factors
- First symptoms: pigmented lesion in the mouth or nose; vaginal bleeding; rectal bleeding
Ocular (uveal) melanoma:
- Arises within the eye — specifically the uvea (iris, ciliary body, choroid)
- The most common primary intraocular tumor in adults
- Often presents with visual changes, floaters, or loss of peripheral vision
- Unlike skin melanoma, uveal melanoma has different genetic drivers (GNAQ/GNA11 mutations) and responds poorly to immunotherapy
Spitzoid melanoma:
- Primarily affects children and young adults
- Pathologically resembles Spitz nevi (benign lesions), making diagnosis extremely challenging
- Management involves specialized pediatric dermatopathology
Our article on basal cell carcinoma cure rates and treatment provides useful context on how melanoma compares to other skin cancers in terms of treatability.
Causes, Risk Factors & Who Is Most Vulnerable
The Root Cause: UV Radiation and DNA Damage
The primary driver of melanoma is ultraviolet (UV) radiation — from both the sun and artificial sources (primarily tanning beds).
When UV rays penetrate skin cells, they directly damage DNA by creating abnormal bonds between adjacent nucleotides — particularly thymine-thymine dimers. In most cases, the body’s DNA repair mechanisms correct these errors. In melanocytes with impaired repair capacity, these mutations accumulate.
The two UV wavelengths matter differently:
| UV Type | Wavelength | Penetration | Primary Role in Melanoma |
|---|---|---|---|
| UVA | 320–400nm | Deeper — dermis | DNA mutation, immunosuppression |
| UVB | 280–320nm | Epidermis | Direct DNA strand breaks; primary driver of sunburn |
Both UVA and UVB contribute to melanoma risk. Tanning beds emit primarily UVA radiation at intensities 10–15 times higher than natural sunlight — which is why the WHO classifies them as Group 1 carcinogens (definitively cancer-causing in humans).
Complete Risk Factor Matrix
Understanding your personal risk profile is one of the most powerful tools in melanoma prevention. Use our Genetic Risk Assessment Tool to evaluate your individual risk profile.
Non-Modifiable Risk Factors
Skin, Hair, and Eye Characteristics:
- Fair skin (Fitzpatrick Type I–II) — lowest natural UV protection
- Red or blonde hair — associated with MC1R gene variants and reduced melanin protection
- Blue, green, or gray eyes
- Tendency to burn rather than tan
- Presence of freckles
Mole-Related Factors:
- More than 50 common moles (melanocytic nevi)
- One or more dysplastic (atypical) nevi — irregular, large moles with color variation
- Giant congenital nevi (large moles present at birth)
- Personal history of any previous melanoma
Family History:
- First-degree relative with melanoma: 2–8x increased risk
- Two or more first-degree relatives: significantly elevated risk
- Familial atypical mole-melanoma (FAMM) syndrome
Genetic Mutations:
- CDKN2A mutations — the most common hereditary melanoma gene, found in 20–40% of familial melanoma kindreds
- CDK4 mutations — rarer, high penetrance
- BAP1 mutations — associated with uveal melanoma and other cancers
Immunosuppression:
- Organ transplant recipients: 2–4x increased melanoma risk
- HIV/AIDS with advanced immunosuppression
- Long-term immunosuppressive therapy for autoimmune conditions
Previous Radiation Therapy:
- Prior radiation to skin increases localized melanoma risk (rare but documented)
Xeroderma Pigmentosum:
- Rare genetic disorder with severely impaired UV DNA repair; lifetime melanoma risk extremely high
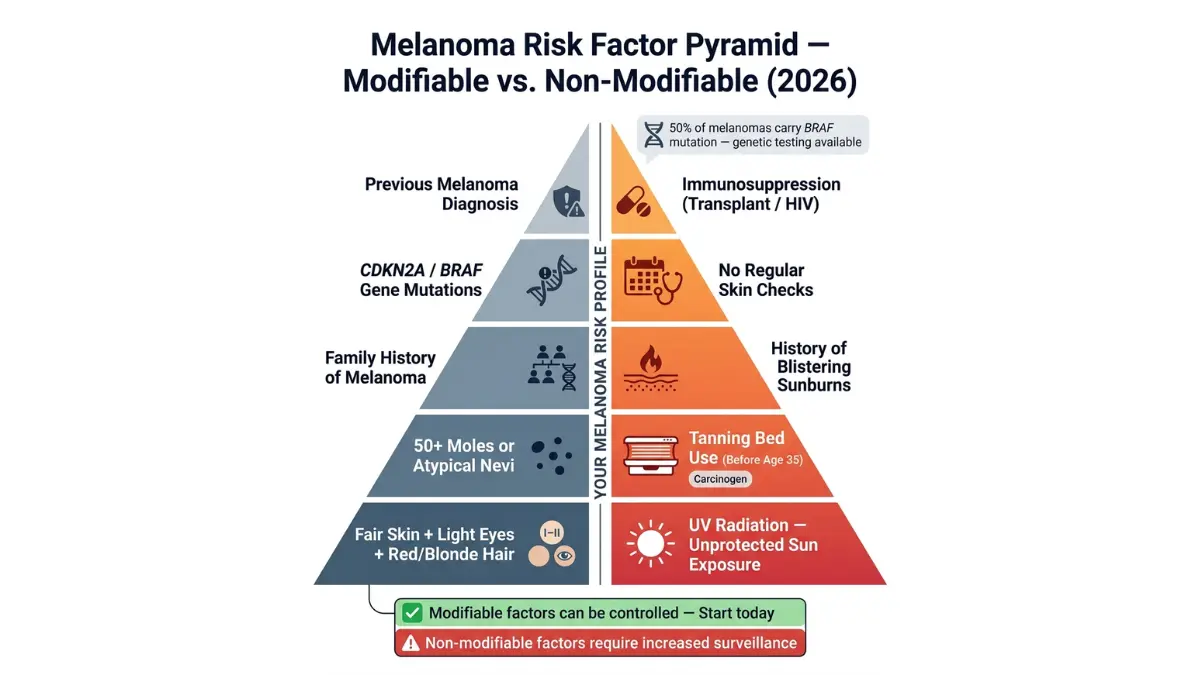
Modifiable Risk Factors
Sun Exposure:
- Cumulative lifetime UV exposure — particularly to the head, neck, and extremities
- History of blistering sunburns, especially in childhood and adolescence — strongly correlated with melanoma risk decades later
- Living at high altitude or near the equator (higher UV intensity)
- Outdoor occupation without adequate sun protection
Tanning Bed Use:
- Any use before age 35: ~75% increased melanoma risk
- Regular use over years: dose-dependent increase
- Particularly dangerous for adolescents and young adults
Geographic Factors:
- Residing in high-altitude locations (UV intensity increases ~4% per 300 meters)
- High-UV-index regions: Southern US states, Colorado, Hawaii, coastal areas
BRAF, NRAS, and the Genetics of Melanoma
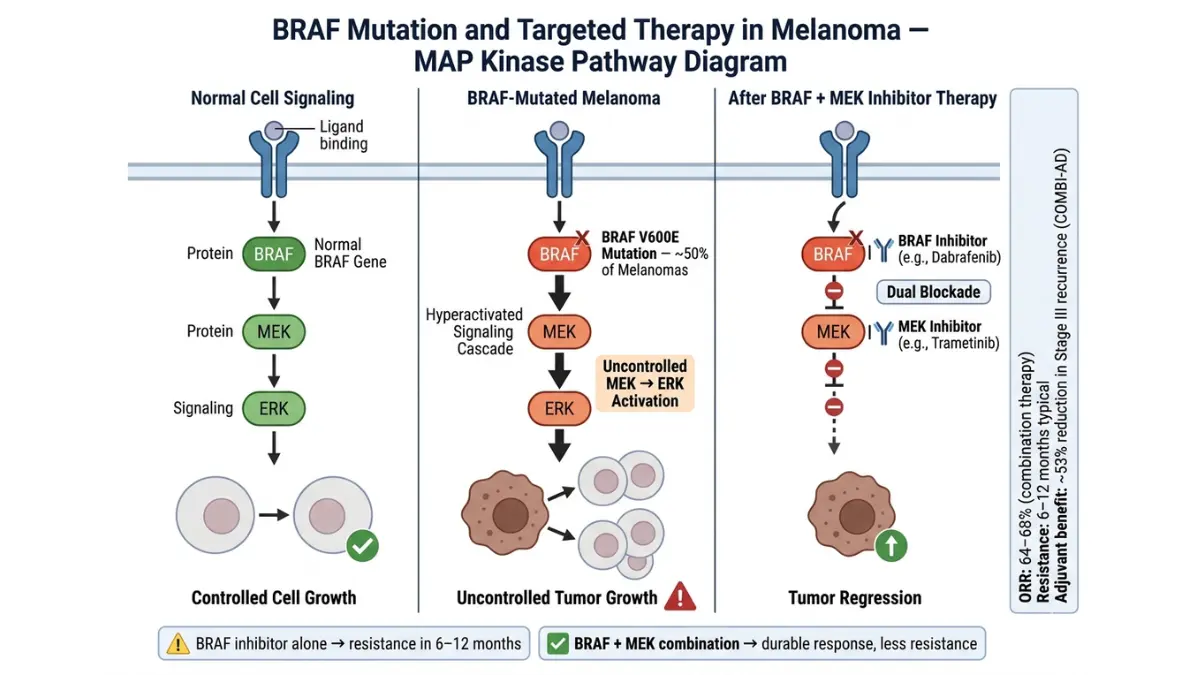
Approximately 50% of cutaneous melanomas carry a mutation in the BRAF gene — most commonly the BRAF V600E variant. This mutation drives rapid, uncontrolled activation of the MAP kinase signaling pathway, promoting tumor growth and survival.
Another 15–20% of melanomas carry NRAS mutations, which activate overlapping growth pathways.
These mutations are not inherited in the traditional sense — they arise in melanocyte DNA due to UV damage. However, they are critically important because:
- They are targetable — BRAF and MEK inhibitor drugs can specifically block the abnormal proteins produced
- BRAF status determines whether targeted therapy is an option for Stage III–IV disease
- BRAF/NRAS testing is now standard of care for all Stage III and IV melanoma patients
For families with multiple members affected by melanoma, genetic counseling and testing for inherited mutations (CDKN2A) is recommended and should be discussed with a board-certified genetic counselor.
Melanoma by Age, Sex, and Race: The Demographics That Define Your Risk
By Age:
- Average age at diagnosis: 66 years
- However, melanoma is one of the most common cancers in adults aged 20–30
- In women under 40, rates are rising rapidly — largely attributed to tanning bed use
- Pediatric melanoma: rare but increasing; often presents as a changing pigmented lesion or pink/red nodule
By Sex:
- Overall more common in men than women
- Men most commonly develop melanoma on the trunk (back)
- Women most commonly develop melanoma on the legs
- In adults under 50, incidence rates in women are slightly higher than in men due to tanning behavior
By Race/Ethnicity (US Lifetime Risk):
| Population | Lifetime Risk | Primary Subtype | Stage at Diagnosis |
|---|---|---|---|
| White | 1 in 33 (~3%) | Superficial spreading | Earlier (more awareness, screening access) |
| Hispanic | 1 in 200 (~0.5%) | Mixed | Later on average |
| Black | 1 in 1,000 (~0.1%) | Acral lentiginous | Significantly later |
| Asian/Pacific Islander | 1 in 200–400 | Acral lentiginous | Later on average |
These risk numbers reflect incidence — but the mortality gap is stark. A Black patient diagnosed with melanoma has approximately a 30% higher risk of death than a White patient with the same disease, entirely explained by later stage at diagnosis and treatment disparities, not tumor biology.
Melanoma in Young Adults (Under 30): A Growing Crisis
Melanoma’s rising incidence in young adults — particularly women aged 20–39 — is one of the most alarming trends in oncology.
Key facts for young adults:
- Melanoma is in the top 5 most common cancers in adults aged 20–29
- Young women with a tanning bed history face a particularly elevated risk
- Young adults often do not see a dermatologist regularly (or ever) — creating a silent epidemic of undetected early-stage disease
- Melanoma in young patients tends to have better prognosis if detected early — because their immune systems are stronger and treatment tolerance is greater
Warning signs specific to young adults:
- Any mole that changes within weeks in someone with a tanning history
- New dark moles appearing after age 20, especially on the back or legs
- Pink or red non-healing bumps in a heavy tanning bed user
Melanoma Prevention: Your Evidence-Based Action Plan
Prevention of melanoma — particularly for modifiable risk factors — is highly effective.
Daily SPF Application:
- Apply SPF 30+ broad-spectrum sunscreen every morning, regardless of cloud cover or season
- Reapply every two hours during outdoor activity
- SPF 50+ for high-UV environments (beach, high altitude, snow reflection)
- Don’t forget: ears, back of neck, hands, and tops of feet
Protective Clothing:
- UPF 50+ rated clothing blocks >98% of UV radiation
- Wide-brim hats (minimum 3-inch brim) for face, ears, and neck protection
- UV-protective sunglasses (wrap-around style)
Behavioral Modifications:
- Avoid peak UV hours: 10am–4pm whenever possible
- Never use tanning beds — there is no “safe” tanning bed exposure
- Seek shade, especially during peak UV hours
Regular Skin Checks:
- Monthly self-examination (see protocol above)
- Annual full-body professional skin check by a dermatologist
- More frequent checks (every 3–6 months) for high-risk individuals
Vitamin D: Sun avoidance does not mean vitamin D deficiency. Supplement with 1,000–2,000 IU vitamin D3 daily (or as recommended by your physician). Do not expose skin to UV radiation for vitamin D purposes — supplementation is safer and equally effective. You can also track your overall nutritional health with our Water Intake Calculator and Protein Intake Calculator to support your immune and skin health.
The 4 Deadly Stages of Melanoma — Complete Survival Rate Breakdown (2026)
Why Staging Is the Most Important Number in Your Diagnosis
When you receive a melanoma diagnosis, the first question your oncologist asks is: what stage?
Staging determines:
- How far the cancer has spread
- What treatment you need
- What your prognosis looks like
- Whether you need adjuvant (preventive) therapy after surgery
- How often you need follow-up imaging and exams
Melanoma staging uses the AJCC (American Joint Committee on Cancer) 8th Edition TNM System, which classifies melanoma based on three parameters:
| Parameter | What It Measures | Key Factors |
|---|---|---|
| T (Tumor) | Primary tumor characteristics | Breslow thickness + ulceration |
| N (Nodes) | Lymph node involvement | Number of nodes, micro vs macro, in-transit lesions |
| M (Metastasis) | Distant spread | Location + LDH level |
Breslow thickness — the measurement of tumor depth from the skin surface to the deepest point of invasion — is the single most powerful predictor of survival. Every additional millimeter of depth increases metastatic risk.
Ulceration — breakdown of the overlying skin surface — is an independent adverse prognostic factor at every stage.
For more context on how cancer staging works generally, see the National Cancer Institute’s staging overview.
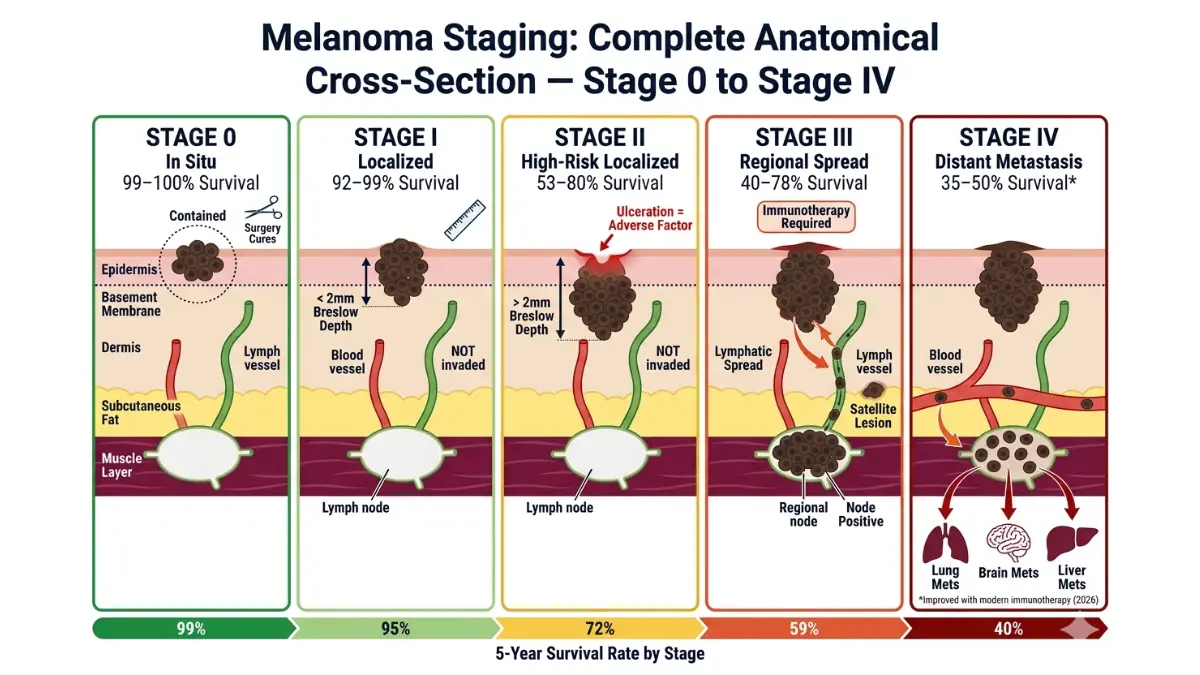
Stage 0 (Melanoma In Situ): Completely Curable
Definition: Melanoma cells are confined entirely to the epidermis — the outermost layer of skin. No invasion of the dermis has occurred. No lymph node or distant spread is possible at this stage.
Breslow thickness: By definition, Stage 0 has no measurable Breslow depth — the tumor has not yet breached the basement membrane.
Treatment: Simple surgical excision with 0.5–1cm margins. No lymph node biopsy required. No systemic therapy.
Prognosis:
- 5-year survival: 99–100%
- 10-year survival: 98–99%
- Local recurrence risk: Very low
What This Means For You: Stage 0 melanoma is essentially cured by surgery. The goal is to achieve clean surgical margins — meaning the pathologist confirms no melanoma cells at the edge of the removed tissue. Once confirmed, you enter a surveillance protocol and return to near-normal life risk.
Stage I Melanoma: Highly Curable With Surgery
Stage I melanoma remains localized to the primary skin site with no lymph node or distant spread.
Stage IA
- Breslow thickness: ≤0.8mm
- Ulceration: Absent
- 5-year survival: ~97–99%
Stage IB
- Breslow thickness: ≤0.8mm with ulceration, OR
- Breslow thickness: 0.8–2mm without ulceration
- 5-year survival: ~92–95%
Treatment: Wide local excision with:
- 1cm margins for lesions ≤1mm thick
- Sentinel lymph node biopsy (SLNB) considered for lesions >0.8mm or any lesion with ulceration
What SLNB tells you: A negative sentinel node means the cancer has not spread to lymph nodes — confirming Stage I. A positive sentinel node upstages to Stage III.
Post-treatment: Stage I patients enter surveillance monitoring. No adjuvant therapy required for IA. IB patients may be monitored closely for 2 years with consideration of adjuvant therapy if higher-risk features are present.
Stage II Melanoma: Intermediate to High Risk — and Often Undertreated
Stage II is one of the most nuanced — and most clinically important — melanoma stages. Many patients and even physicians underestimate the recurrence risk of advanced Stage II disease.
Stage IIA
- Breslow: 1–2mm with ulceration, OR 2–4mm without ulceration
- 5-year survival: ~80%
Stage IIB
- Breslow: 2–4mm with ulceration, OR >4mm without ulceration
- 5-year survival: ~72%
- Adjuvant pembrolizumab (Keytruda) now FDA-approved for IIB patients (2021 approval)
Stage IIC
- Breslow: >4mm with ulceration
- 5-year survival: ~53% — worse than some Stage IIIA patients
- High-risk for distant recurrence
- Adjuvant pembrolizumab strongly recommended
The Stage IIC problem: Stage IIC carries a worse prognosis than Stage IIIA — yet many patients are told “it hasn’t spread to the lymph nodes, so you’re Stage II, which is good.” This is clinically misleading. Stage IIC patients need aggressive adjuvant treatment and intensive surveillance.
What This Means For You: If you are diagnosed with Stage IIB or IIC, ask your oncologist explicitly: “Am I a candidate for adjuvant pembrolizumab?” The 2021 FDA approval for this indication has changed outcomes significantly.
Stage III Melanoma: Regional Spread — The Critical Crossroads
Stage III melanoma has spread beyond the primary skin site to nearby lymph nodes, in-transit skin lesions, or satellite metastases.
Stage III is divided into subcategories (IIIA through IIID) based on:
- Number and size of lymph node metastases
- Whether nodes are micro (found only by biopsy) or macro (palpable)
- Presence of in-transit metastases (tumors within lymphatic channels, between primary tumor and regional nodes)
- Presence of satellite lesions (small tumor deposits near primary)
| Substage | Key Features | 5-Year Survival |
|---|---|---|
| IIIA | Micrometastases in 1–3 nodes; thin primary | ~78% |
| IIIB | Micrometastases in 4+ nodes; OR macrometastases in 1–3 | ~59% |
| IIIC | Macrometastases in 4+ nodes; OR in-transit lesions | ~40–50% |
| IIID | Bulky nodes; extensive in-transit disease | ~32% |
Standard Treatment for Stage III (2026):
- Wide local excision of primary tumor
- Lymph node dissection (if positive sentinel or palpable nodes)
- Adjuvant systemic therapy — the treatment revolution for Stage III:
- Pembrolizumab (anti-PD-1) for 1 year — ~40% reduction in recurrence
- Nivolumab (anti-PD-1) — similar efficacy
- Dabrafenib + Trametinib (BRAF/MEK inhibitors) for BRAF V600E-mutated Stage III — ~53% reduction in recurrence
What This Means For You: Stage III is serious but increasingly manageable. The adjuvant immunotherapy approvals of 2017–2021 have dramatically reduced recurrence rates. The key is receiving treatment at a melanoma-specialized center where oncologists are familiar with current combination approaches.
Stage IV Melanoma: The Survival Revolution
Stage IV melanoma — cancer that has spread to distant organs — was once considered almost universally fatal. That era is over.
What changed: The development of checkpoint inhibitors and targeted therapies beginning in 2010–2011 fundamentally altered the natural history of metastatic melanoma. Before 2010, median survival for Stage IV melanoma was approximately 8–9 months. Today, substantial proportions of patients achieve multi-year remission.
Sites of Stage IV spread and their implications:
| Metastasis Site | Clinical Features | Relative Prognosis |
|---|---|---|
| Distant skin/soft tissue | Often multiple nodules | Relatively better |
| Lung | Cough, dyspnea, chest pain | Intermediate |
| Liver | Abdominal fullness, elevated LFTs | Less favorable |
| Brain | Headache, seizure, confusion | Requires brain-specific treatment |
| Bone | Bone pain, fractures | Requires bone-specific approaches |
| Adrenal gland | Often asymptomatic | Moderately favorable |
2026 Survival Data for Stage IV:
| Era | Median Overall Survival | 5-Year Survival |
|---|---|---|
| Pre-2010 (chemotherapy only) | 8–9 months | ~5–10% |
| 2011–2015 (first-gen immunotherapy) | 18–24 months | ~20–25% |
| 2016–2020 (combination approaches) | 36–48 months | ~30–40% |
| 2021–2026 (Opdualag, TIL therapy, combos) | 48–60+ months in responders | ~40–50% in responders |
These numbers represent some of the most dramatic improvements in oncology outcome data in the past 25 years.
According to ACS survival statistics, the historically cited 35% five-year survival for Stage IV reflects data from patients diagnosed 5–10 years ago, before many current treatments were available. Real-world 2026 outcomes are meaningfully better for patients who respond to immunotherapy.
The Treatment Delay Data: Why Every Day Matters
This data point belongs in every melanoma article — and almost none of them include it.
Research cited by the Skin Cancer Foundation demonstrates the devastating impact of treatment delay after a suspicious biopsy:
- Treated within 30 days: Baseline survival
- Treated 30–59 days after biopsy: ~5% higher risk of melanoma death
- Treated 60–119 days after biopsy: ~20% higher risk
- Treated >119 days after biopsy: ~41% higher risk of melanoma death
Every single day of delay increases risk. If your biopsy comes back as melanoma, do not wait for a “convenient” surgical date. Push for treatment within 2–3 weeks.
Complete Survival Rate Master Table (2026)
| Stage | 5-Year Relative Survival | 10-Year Survival | Primary Determinant |
|---|---|---|---|
| Stage 0 | 99–100% | 98–100% | Complete excision with clean margins |
| Stage IA | 97–99% | 95% | Breslow <0.8mm, no ulceration |
| Stage IB | 92–95% | 88% | Breslow 0.8–2mm; ulceration status |
| Stage IIA | 80% | 74% | Breslow 1–4mm |
| Stage IIB | 72% | 63% | Breslow >2mm; ulceration |
| Stage IIC | 53% | 45% | Breslow >4mm with ulceration |
| Stage IIIA | 78% | 68% | Micrometastases in nodes |
| Stage IIIB | 59% | 47% | Macrometastases; in-transit lesions |
| Stage IIIC–D | 40–50% | 32–40% | Extensive nodal and in-transit disease |
| Stage IV | 35–50%* | 20–30%* | Response to immunotherapy |
*Significantly improving with modern checkpoint inhibitor combinations and TIL therapy.
Data sources: American Cancer Society, SEER Database, AIM at Melanoma Foundation
Diagnosis — From Suspicious Mole to Confirmed Melanoma
The Patient Diagnosis Journey: A Step-by-Step Roadmap
Understanding the diagnostic journey reduces anxiety and helps you advocate for yourself at every step.
Step 1 — Self-detection or incidental finding Most melanomas are found either by the patient or a partner during skin self-examination, or incidentally during a general physical examination.
Step 2 — Dermatologist evaluation A suspicious lesion should be seen by a board-certified dermatologist. General practitioners can perform initial evaluation, but any lesion with suspicious features should be referred promptly.
Step 3 — Dermoscopy Non-invasive magnified examination using a dermoscope. Significantly improves diagnostic accuracy compared to naked-eye examination alone.
Step 4 — Biopsy Tissue is removed for pathological analysis. This is the only definitive way to diagnose melanoma.
Step 5 — Pathology report A specialized dermatopathologist examines the tissue and provides a report detailing tumor characteristics. Learn how to decode your biopsy results in our guide on understanding pathology report results.
Step 6 — Staging scans (if warranted) Depending on Breslow thickness and biopsy findings, CT, PET, and/or MRI scans are ordered to determine spread. For help understanding scan results, see our guides on CT scan findings and PET scan SUV results.
Step 7 — Treatment planning A multidisciplinary team including a surgical oncologist, medical oncologist, and dermatologist develops your treatment plan.
Dermoscopy: The Dermatologist’s Most Powerful Tool
Dermoscopy (also called dermatoscopy) uses a handheld device that combines polarized light and 10x magnification to examine subsurface skin structures invisible to the naked eye.
What dermoscopy reveals:
- Atypical pigment networks
- Regression structures (white scar-like areas)
- Blue-white veil (sign of deeper melanin or neovascularization)
- Atypical vascular patterns
- Irregular globules and streaks
Why it matters: Dermoscopy improves melanoma detection sensitivity by approximately 35% compared to naked-eye examination alone. It also reduces unnecessary biopsies of clearly benign lesions — a meaningful quality-of-life benefit.
Digital dermoscopy: Many specialized dermatology practices now use digital dermoscopy systems that photograph and store lesion images, allowing direct comparison over time. AI-assisted dermoscopy platforms are increasingly being used in 2026 to flag suspicious patterns automatically.
Types of Skin Biopsy: Which Method and When
| Biopsy Type | Description | Best For | Melanoma Suitability |
|---|---|---|---|
| Excisional biopsy | Complete removal of lesion with 1–2mm margins | Suspected melanoma — gold standard | ★★★★★ |
| Punch biopsy | Circular blade removes a cylindrical core | Smaller lesions, accessible locations | ★★★★☆ |
| Shave biopsy | Superficial horizontal shave of lesion | Superficial lesions — risks incomplete sampling | ★★☆☆☆ |
| Incisional biopsy | Partial removal of a large lesion | Very large lesions, especially LMM | ★★★☆☆ |
| Fine needle aspiration (FNA) | Needle sampling of enlarged lymph node | Lymph node staging | ★★★☆☆ |
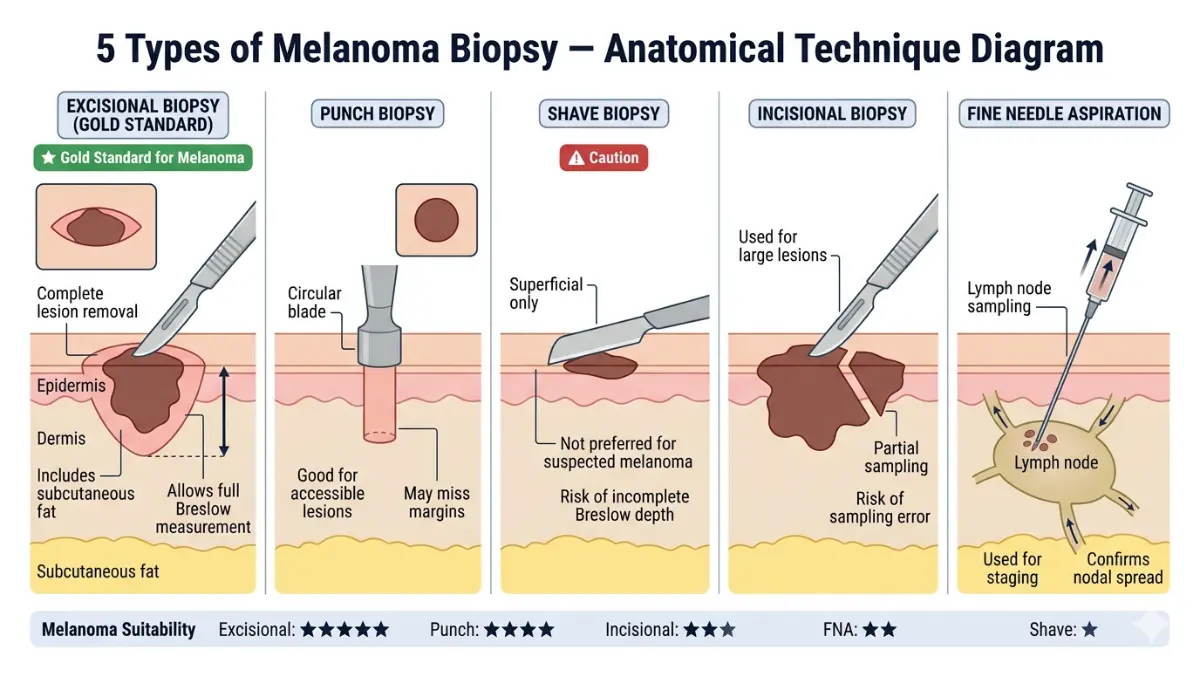
Critical rule: For suspected melanoma, excisional biopsy with narrow margins is the preferred approach. Deep enough to include the subcutaneous fat to allow accurate Breslow depth measurement. Shave biopsies that transect the tumor base can render Breslow depth unmeasurable — a significant clinical problem.
Reading Your Pathology Report: What Every Number Means
Your melanoma pathology report contains several critical data points. Understanding them helps you make informed decisions. For full guidance, see our biopsy results timeline and report guide.
| Finding | What It Means | Why It Matters |
|---|---|---|
| Breslow thickness | Depth of tumor in millimeters | Most important prognostic factor; determines margin width and SLNB need |
| Clark’s level | Anatomical depth (I–V) | Supplementary to Breslow; still used in very thin tumors |
| Ulceration | Breakdown of overlying epidermis | Adverse factor; upstages many tumors (e.g., T1b if present) |
| Mitotic rate | Number of dividing cells per mm² | Higher rate = more aggressive; ≥1/mm² is significant |
| Surgical margin status | Whether cancer cells reach excision edge | “Positive margins” = further surgery needed |
| Microsatellites | Small tumor nests in dermis near primary | Adverse — associated with in-transit risk |
| Tumor-infiltrating lymphocytes (TILs) | Immune cells within tumor | Higher TIL density associated with better prognosis |
| Lymphovascular invasion | Cancer cells in blood/lymph vessels | Adverse prognostic factor |
| Regression | Partial immune destruction of tumor | May underestimate true Breslow depth |
Sentinel Lymph Node Biopsy (SLNB): The Surgical Staging Procedure
SLNB is a procedure that samples the first lymph nodes to which a melanoma would drain — providing accurate information about lymph node status without the morbidity of full node dissection.
Who needs SLNB:
- Breslow thickness >0.8mm (regardless of ulceration)
- Any thickness with ulceration present
- Any thickness with mitotic rate ≥1/mm² (in some guidelines)
- At physician discretion for tumors 0.6–0.8mm with adverse features
How SLNB works:
- A radioactive tracer and/or blue dye is injected around the primary melanoma site
- The tracer travels through lymphatic channels to the first-draining (sentinel) node
- A gamma probe and/or visual identification locates the node
- The node is surgically removed and sent for pathological examination
- Finding melanoma cells in the sentinel node = positive result = Stage III
What a positive SLNB means: Your melanoma has reached the regional lymph nodes. You are now Stage III. You need discussion of lymph node dissection and adjuvant systemic therapy.
Completion lymph node dissection (CLND): Based on the MSLT-II trial, CLND after a positive sentinel node does not improve survival in most patients. However, it provides staging information and is still performed in select high-risk cases.
Imaging and Blood Tests by Stage
| Test | When Ordered | What It Detects | Notes |
|---|---|---|---|
| CT scan (chest/abdomen/pelvis) | Stage IIB+ or if symptoms present | Lung, liver, abdominal metastases | Most common staging scan |
| PET scan | Stage III–IV | Full-body metabolic activity; detects even small metastases | More sensitive than CT for soft tissue/nodal disease |
| MRI (brain) | Stage III–IV; brain symptoms present | Brain metastases | Superior to CT for brain lesions |
| Ultrasound (lymph nodes) | Stage IB–IIA in some guidelines | Regional lymph node assessment | Non-invasive; less sensitive than PET |
| LDH (blood test) | Stage III–IV | Prognostic marker; elevated = worse prognosis | Part of M-staging classification |
| BRAF/NRAS mutation testing | All Stage III–IV | Determines targeted therapy eligibility | Tissue-based or liquid biopsy |
See our complete guide on MRI report interpretation for understanding imaging findings.
What Gets Confused With Melanoma? Common Misdiagnoses
| Masquerading Condition | Actual Presentation | How to Differentiate |
|---|---|---|
| Seborrheic keratosis | Waxy, “stuck on” tan/brown lesion | Dermoscopy; characteristic “milia-like cysts” |
| Blue nevus | Blue-gray dome-shaped papule | Dermoscopy; stable long-term |
| Pyogenic granuloma | Red, rapidly growing friable nodule | Vascular pattern on dermoscopy; young patients |
| Subungual hematoma | Dark streak under nail after injury | History of trauma; grows out with nail |
| Atypical mole (dysplastic nevus) | Irregular mole with color variation | Biopsy is only definitive differentiation |
| Tattoo ink | Pigment in skin from tattoo | Location and history |
The key takeaway: When in doubt, biopsy. A biopsy is a minor outpatient procedure. Missing a melanoma is not minor.
2026 Technology: AI-Assisted Melanoma Detection
Artificial intelligence is transforming early melanoma detection. Several platforms are now FDA-cleared or in advanced clinical validation for AI-assisted dermoscopy.
Current 2026 AI tools:
- AI-enhanced dermatoscopes that provide real-time lesion scoring during clinical examination
- Smartphone-based apps with AI analysis (for preliminary screening — not diagnostic)
- Whole-body photography systems with AI change-detection over time
Our dedicated article on 2026 AI screening and melanoma survival explores how artificial intelligence is being integrated into early detection programs.
Melanoma Treatment in 2026 — From Surgery to Revolutionary Immunotherapy
The Treatment Decision Framework: By Stage
Before discussing individual treatments, understand this foundational principle:
Melanoma treatment is never one-size-fits-all. Every treatment decision is driven by:
- Stage — how far has it spread?
- Breslow thickness and ulceration — how aggressive is the primary tumor?
- BRAF mutation status — is targeted therapy an option?
- Performance status — can the patient tolerate systemic therapy?
- Patient preferences and goals — quality of life vs. maximum treatment intensity
| Stage | Primary Treatment | Adjuvant (Preventive) Therapy | Systemic (Metastatic) Therapy |
|---|---|---|---|
| 0 | Excision 0.5–1cm margins | None | None |
| IA | WLE 1cm margin | None | None |
| IB | WLE 1cm ± SLNB | Observation or consider pembro | None |
| IIA | WLE 1–2cm + SLNB | Consider pembrolizumab | None |
| IIB–IIC | WLE 2cm + SLNB | Pembrolizumab 1 year (FDA-approved) | None |
| III | WLE + LND ± CLND | Pembrolizumab OR nivolumab OR dabrafenib+trametinib | Escalate if recurs |
| IV | Palliative surgery if needed | N/A | Systemic therapy — see below |
Surgery: The Foundation of Melanoma Treatment
Surgery remains the cornerstone of melanoma care at all stages where it is technically feasible.
Wide Local Excision (WLE)
WLE removes the primary melanoma with a surrounding margin of normal skin to reduce local recurrence risk.
Margin guidelines (NCCN 2025–2026):
| Breslow Thickness | Recommended Margin |
|---|---|
| In situ (Stage 0) | 0.5–1cm |
| ≤1mm | 1cm |
| 1.01–2mm | 1–2cm |
| >2mm | 2cm |
Key principle: Wider margins do not improve survival for thick tumors if they have already spread to nodes or beyond. Margin width primarily reduces local recurrence risk.
Mohs micrographic surgery: For lentigo maligna melanoma on cosmetically sensitive areas (face, ears), Mohs surgery offers superior margin control and tissue conservation compared to WLE.
Skin reconstruction: Large excisions on the back, leg, or face may require:
- Primary closure (for smaller defects)
- Split-thickness skin grafts
- Full-thickness skin grafts
- Local or regional flap closure
Immunotherapy: The Revolution That Saved Thousands of Lives
What Are Checkpoint Inhibitors?
Your immune system has natural “brakes” — molecular checkpoints that prevent it from attacking normal cells. Melanoma cells have learned to exploit these brakes, essentially hiding from immune surveillance.
Checkpoint inhibitors are drugs that remove these brakes, allowing your T-cells to recognize and destroy melanoma cells.
This approach — developed between 2010–2014 — transformed Stage IV melanoma from near-universally fatal to potentially long-term survivable for substantial proportions of patients. Our detailed immunotherapy guide at how immunotherapy works provides a broader overview of this class of treatments.
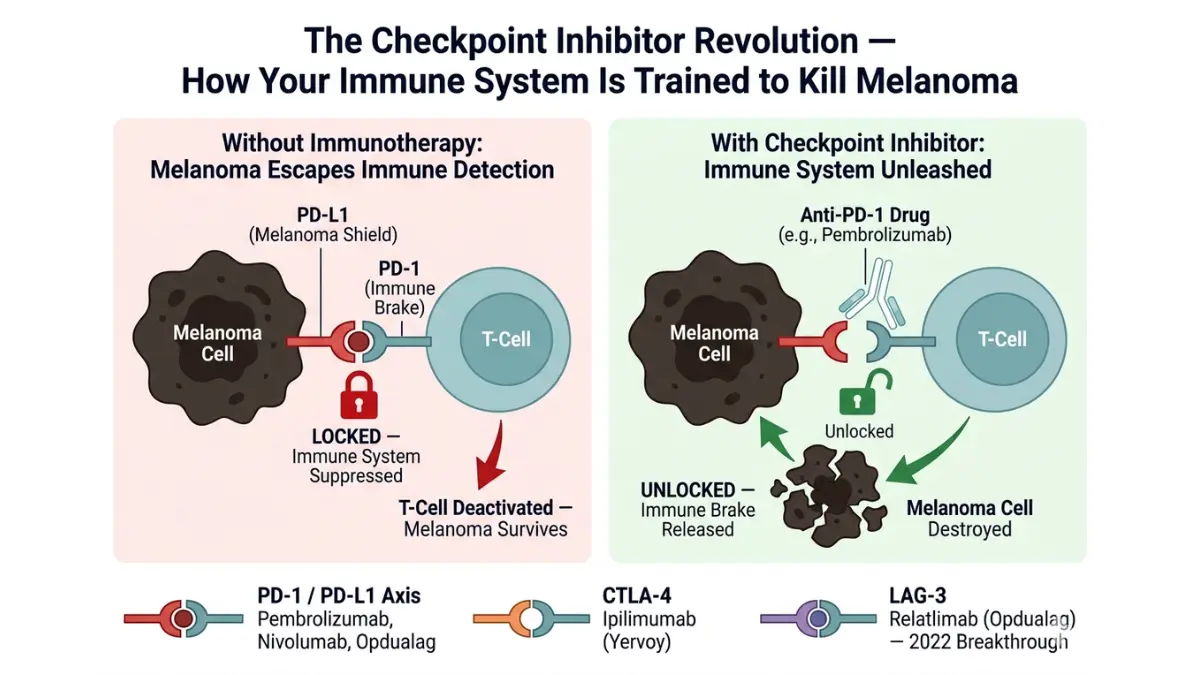
Pembrolizumab (Keytruda) — Anti-PD-1
Mechanism: Blocks the PD-1 receptor on T-cells, preventing melanoma cells from using the PD-L1 “do not attack me” signal.
FDA approvals for melanoma:
- First-line metastatic melanoma (2014)
- Adjuvant therapy for Stage III melanoma after surgery (2019)
- Adjuvant therapy for Stage IIB/IIC melanoma after surgery (2021)
Efficacy data:
- Stage III adjuvant: ~38% reduction in recurrence vs. placebo (KEYNOTE-716)
- Stage IIB/IIC adjuvant: ~35% reduction in distant metastasis (KEYNOTE-716)
- Metastatic: ~34% objective response rate as monotherapy; higher with combination
Dosing: 200mg IV every 3 weeks, OR 400mg every 6 weeks. Duration: up to 1 year adjuvant; continued until progression or toxicity in metastatic setting.
Nivolumab (Opdivo) — Anti-PD-1
Mechanism: Similar to pembrolizumab — PD-1 blockade.
FDA approvals for melanoma:
- Adjuvant Stage III (2017)
- Metastatic melanoma, first-line and after ipilimumab
- In combination with ipilimumab (nivo + ipi) for advanced melanoma
Key data point: The CheckMate 238 trial showed nivolumab adjuvant reduced recurrence in Stage III melanoma by ~35% vs. ipilimumab, with significantly better tolerability.
Ipilimumab (Yervoy) — Anti-CTLA-4
Mechanism: Blocks CTLA-4, a different immune checkpoint, allowing a broader and earlier T-cell activation against tumors.
Use in 2026: Primarily used in combination with nivolumab (“nivo + ipi”), not as monotherapy, due to its significant toxicity profile as a single agent.
Nivo + Ipi combination:
- ~57% objective response rate in metastatic melanoma
- Complete response rate ~22% — meaning roughly 1 in 5 advanced patients achieves complete tumor disappearance
- However: ~60% of patients experience significant immune-related adverse events (irAEs)
- Best for patients with good performance status who can tolerate combination toxicity
Opdualag (Nivolumab + Relatlimab) — The 2022 Breakthrough
Opdualag — a fixed-dose combination of nivolumab and relatlimab — received FDA approval in March 2022 and represents a significant advance in metastatic melanoma treatment.
What is LAG-3? LAG-3 is a third immune checkpoint molecule (alongside PD-1 and CTLA-4) that suppresses T-cell activity. Relatlimab blocks LAG-3, providing a complementary immunostimulatory effect to nivolumab’s PD-1 blockade.
Key RELATIVITY-047 trial data:
- Opdualag vs. nivolumab alone: median progression-free survival 10.1 months vs. 4.6 months — more than doubling the time before disease progression
- Particularly strong benefit in patients with PD-L1+ tumors
- Significantly better tolerability than nivo + ipi combination — ~20% severe irAEs vs. ~60% with nivo + ipi
2026 real-world data: Opdualag is now one of the most commonly used first-line regimens for metastatic melanoma in the United States, offering a favorable balance of efficacy and tolerability.
Targeted Therapy: BRAF and MEK Inhibitors
Approximately 50% of melanomas carry the BRAF V600E mutation. For these patients, targeted therapies that specifically block the abnormal BRAF protein offer rapid, impressive responses.
Why BRAF inhibitors alone are not enough:
Initially, BRAF inhibitors (vemurafenib, dabrafenib) were used as single agents. While they produced dramatic tumor responses in 60–80% of patients, resistance developed in most cases within 6–12 months.
The key insight: blocking BRAF alone activates an alternative pathway (MEK). Combining a BRAF inhibitor with a MEK inhibitor blocks both steps, dramatically improving durability.
2026 Standard Combinations:
| Drug Combination | BRAF Inhibitor | MEK Inhibitor | Key Data |
|---|---|---|---|
| Dabrafenib + Trametinib (Tafinlar + Mekinist) | Dabrafenib | Trametinib | ~64% ORR; adjuvant Stage III: 53% reduction in recurrence |
| Vemurafenib + Cobimetinib (Zelboraf + Cotellic) | Vemurafenib | Cobimetinib | ~68% ORR metastatic |
| Encorafenib + Binimetinib (Braftovi + Mektovi) | Encorafenib | Binimetinib | Longest PFS of three combinations; preferred in many centers |
BRAF/MEK vs. Immunotherapy — Which First for Stage IV?
This is one of the most debated questions in melanoma oncology:
- BRAF/MEK advantage: Rapid responses (within 2–4 weeks), very high response rates, better for patients with high disease burden needing quick tumor control
- Immunotherapy advantage: Potential for durable, long-term remission; responses that last years even after treatment stops
- 2026 practice: Sequencing depends on tumor burden, patient performance status, and LDH level. Most centers prefer immunotherapy first in fit patients with moderate tumor burden; BRAF/MEK first if rapid tumor control is needed.
For patients with both BRAF mutation and good performance status, combination immunotherapy followed by BRAF/MEK on progression, or vice versa, may be optimal. Clinical trials evaluating simultaneous combinations continue.
Radiation Therapy
Melanoma is traditionally considered relatively radioresistant, but radiation has specific, effective roles:
When radiation is used:
- Adjuvant radiation after lymph node dissection in Stage III with high-risk nodal features (reduces regional recurrence)
- Stereotactic radiosurgery (SRS) for limited brain metastases — highly effective, can achieve local control in 80–90% of lesions
- Palliative radiation for bone pain, spinal cord compression, or symptomatic soft tissue deposits
- Mohs surgery alternative for lentigo maligna on the face (radiation achieves excellent local control with cosmetic preservation)
See our comprehensive guide on radiation therapy approaches and side effects for additional detail.
T-VEC (Talimogene Laherparepvec): The Oncolytic Virus
T-VEC is a genetically engineered herpes simplex virus modified to replicate selectively within tumor cells, killing them directly while simultaneously activating a systemic immune response.
FDA approval: 2015 for unresectable melanoma lesions in the skin and lymph nodes.
How it works:
- T-VEC is injected directly into accessible melanoma lesions
- The virus infects and replicates within tumor cells, causing tumor lysis (cell death)
- The dying tumor cells release tumor antigens and stimulate a GM-CSF-driven immune response
- The immune system may then target melanoma cells elsewhere in the body
2026 use: T-VEC is increasingly used in combination with pembrolizumab for patients with injectable lesions, where synergistic responses have been observed.
2026’s Cutting-Edge Treatments: The Pipeline Changing Everything
Lifileucel (Amtagvi): TIL Therapy — FDA Approved February 2024
Tumor-infiltrating lymphocyte (TIL) therapy is one of the most significant melanoma approvals in years. Lifileucel (branded Amtagvi, developed by Iovance Biotherapeutics) became the first TIL therapy approved for any cancer by the FDA in February 2024.
How it works:
- A biopsy removes T-cells that have infiltrated the patient’s tumor
- These T-cells are expanded massively in a specialized laboratory (billions of cells)
- The patient undergoes lymphodepleting chemotherapy to “make room” for the new cells
- The expanded TIL cells are infused back, where they potently attack the melanoma
Key data: In patients with advanced melanoma who had progressed on prior immunotherapy, lifileucel achieved a ~36% objective response rate — remarkable in a population that had exhausted standard options.
Availability: Currently available at specialized cancer centers in the United States. Requires significant logistical coordination but offers hope for patients who have progressed on standard immunotherapy.
mRNA Melanoma Vaccine (mRNA-4157/V940)
Moderna and Merck are collaborating on a personalized mRNA cancer vaccine that teaches the immune system to target specific mutations unique to each patient’s tumor (neoantigens).
Current status (2026): Phase III trial ongoing (KEYNOTE-942/MRNA-4157-P201). Phase IIb data showed that mRNA-4157 combined with pembrolizumab reduced recurrence risk by ~44% compared to pembrolizumab alone in high-risk Stage III/IV patients after surgery — one of the most impressive adjuvant data sets in melanoma history.
What to watch: Full Phase III results are expected in 2027–2028. If confirmed, personalized mRNA vaccines could become a standard adjuvant option for high-risk melanoma.
The Financial Reality of Melanoma Treatment
This section covers what virtually no competitor addresses: the devastating financial cost of modern melanoma therapy.
| Treatment | Annual Cost (US, 2026) | Insurance Coverage |
|---|---|---|
| Pembrolizumab | ~$150,000–$200,000/year | Generally covered with prior authorization |
| Nivolumab + Ipilimumab | ~$250,000–$300,000/year | Coverage varies; high cost-sharing common |
| Opdualag | ~$200,000/year | Covered by most commercial/Medicare plans |
| Dabrafenib + Trametinib | ~$180,000/year | Covered for BRAF+ Stage III–IV |
| Lifileucel (Amtagvi) | ~$400,000+ (one-time) | Limited coverage; evolving |
| Wide local excision | ~$5,000–$20,000 | Typically covered |
Patient assistance programs:
- Merck Access Program — pembrolizumab for qualifying uninsured or underinsured patients
- Bristol Myers Squibb Patient Assistance Foundation — nivolumab and ipilimumab access programs
- Regeneron Oncology Patient Access Program — other melanoma-related therapies
- Clinical trials — provide access to cutting-edge treatments at no drug cost to the patient; find open trials at ClinicalTrials.gov
Practical advice:
- Request a dedicated oncology financial navigator at your cancer center
- Contact your state’s insurance commissioner if prior authorization is denied
- Ask your oncologist about clinical trial eligibility before starting any commercial therapy
Questions to Ask Your Oncologist (Checklist)
Before beginning any melanoma treatment, ask:
- What is my exact stage — and which substage?
- What is my Breslow thickness and ulceration status?
- Has my tumor been tested for BRAF mutations?
- Am I a candidate for adjuvant therapy?
- What are my options — and the evidence behind each?
- What side effects should I prepare for?
- Am I eligible for any clinical trials?
- Where is the nearest melanoma center of excellence?
- What does this treatment cost, and how do we navigate insurance?
Life After Melanoma — Recovery, Recurrence, Mental Health & Nutrition
Follow-Up Surveillance: Your Stage-Based Protocol
Melanoma doesn’t simply “go away” after treatment. Active surveillance is essential for detecting recurrence — which is most common in the first 2–3 years — as well as second primary melanomas (which affect 5–8% of survivors).
Surveillance Schedule by Stage (NCCN 2026 Guidelines):
| Stage | Year 1 | Year 2–3 | Year 4–5 | Beyond Year 5 |
|---|---|---|---|---|
| 0–IA | Every 6 months | Annually | Annually | Annual skin exam |
| IB–IIA | Every 3–6 months | Every 6 months | Annually | Annual |
| IIB–IIC | Every 3 months | Every 3–4 months | Every 6 months | Annually |
| III | Every 3 months | Every 3 months | Every 4–6 months | Annually |
| IV (remission) | Every 3 months | Every 3 months | Every 4–6 months | Individualized |
What surveillance involves:
- Complete skin examination by a dermatologist (look for new primary melanomas)
- Physical examination — lymph node palpation
- Review of new symptoms
- Imaging (CT, PET, MRI) for Stages IIB+ — frequency varies by stage and symptoms
Melanoma Recurrence: The Facts You Need to Know
Types of recurrence:
- Local recurrence: Melanoma returns at or near the original surgical site
- In-transit recurrence: Melanoma reappears in lymphatic channels between the primary site and regional nodes — appears as clusters of subcutaneous nodules
- Regional recurrence: Cancer returns in regional lymph nodes
- Distant recurrence: Cancer appears in new organ sites (lung, liver, brain, bone)
Recurrence rates by stage:
| Stage | 5-Year Recurrence Risk |
|---|---|
| Stage I | <5% |
| Stage IIA | ~20% |
| Stage IIB–IIC | 28–47% |
| Stage III | 35–60% depending on substage |
| Stage IV (complete response) | Ongoing risk; ~30–40% durable remission with immunotherapy |
Warning signs of recurrence:
- A new lump or nodule near the surgical scar
- New swelling in lymph node regions (armpit, groin, neck)
- New or worsening symptoms at known metastatic sites
- Unexplained weight loss, fatigue, or night sweats
- Any new changing skin lesion
The most important message: Early detection of recurrence matters just as much as early detection of primary melanoma. Recurrences found early — when small and localized — are far more treatable than those found late.
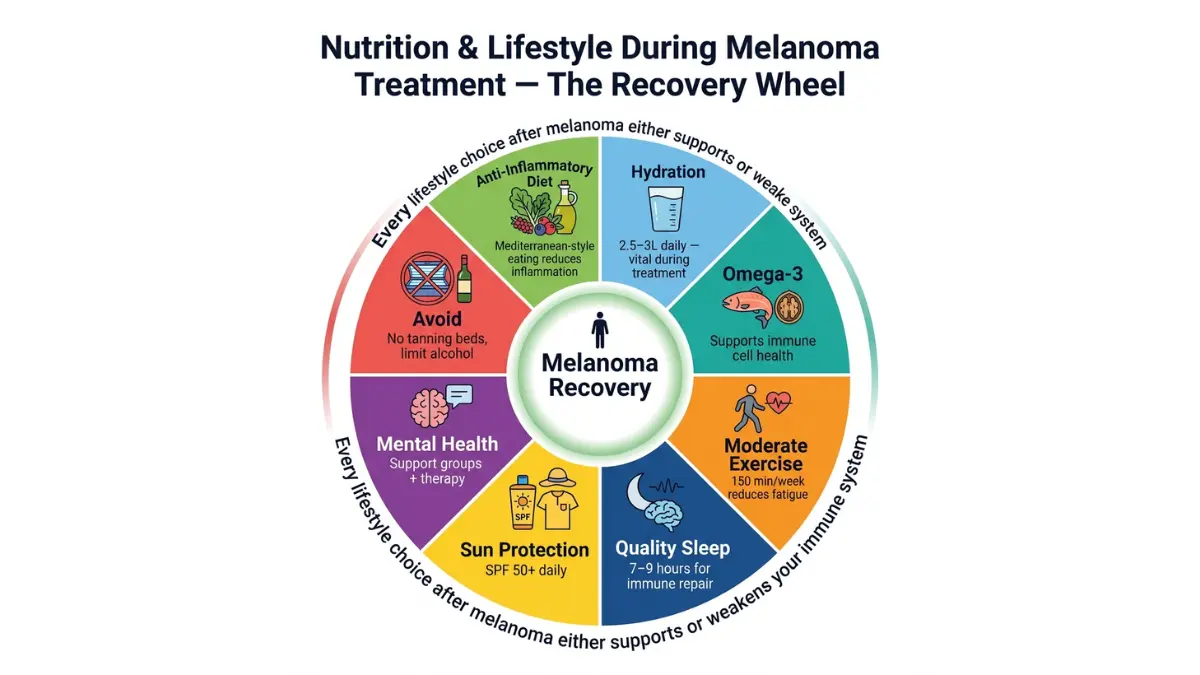
Nutrition During and After Melanoma Treatment
Nutrition during cancer treatment is one of the most-asked-about yet least-addressed topics by major health websites. Here is evidence-based guidance.
During immunotherapy (pembrolizumab, nivolumab, Opdualag):
- Foods to prioritize:
- Anti-inflammatory diet: abundant in colorful vegetables, berries, olive oil, fatty fish (omega-3 fatty acids)
- High-fiber diet: supports gut microbiome diversity — emerging evidence links gut microbiome to immunotherapy response rates
- Adequate protein: supports immune cell production and muscle preservation during treatment
- Use our Protein Intake Calculator to ensure you’re meeting daily protein targets
- Foods to limit:
- Processed meats and refined carbohydrates (pro-inflammatory)
- Excessive alcohol (impairs immune function and liver metabolism of drugs)
- Grapefruit and grapefruit juice if on BRAF/MEK inhibitors (inhibits CYP3A4 metabolism of some drugs)
- Supplements — proceed with caution:
- High-dose antioxidant supplements (Vitamin C, E, beta-carotene) may theoretically interfere with oxidative cell death mechanisms triggered by immunotherapy — discuss with your oncologist before supplementation
- Vitamin D (1,000–2,000 IU daily) appears generally safe and may support immune function
- Omega-3 fatty acids from food sources (salmon, sardines, walnuts) are generally favorable
Maintaining a healthy body weight: Obesity is associated with melanoma recurrence risk and worse immunotherapy outcomes in some studies. Maintaining a healthy BMI through evidence-based nutrition and appropriate exercise supports both treatment tolerability and long-term outcomes.
Hydration: Immunotherapy side effects (diarrhea, nausea) can significantly affect hydration status. Use our Water Intake Calculator to set daily hydration goals during treatment.
Exercise After Melanoma Diagnosis
Exercise during and after cancer treatment has robust evidence supporting:
- Reduced cancer-related fatigue (the most common complaint in immunotherapy patients)
- Improved immune function
- Better mental health outcomes
- Potentially improved survival in some cancer types
Safe guidelines for melanoma patients during immunotherapy:
- Moderate aerobic activity 150+ minutes per week (brisk walking, cycling, swimming) — adjust for fatigue
- Resistance training 2x per week to preserve muscle mass
- Avoid high-intensity exercise immediately after infusions (first 24–48 hours)
- Monitor for joint pain (potential immunotherapy adverse event — colitis and arthritis are common irAEs)
- Lymphedema precautions if lymph nodes have been removed (avoid repetitive heavy lifting in the affected arm/leg)
Optimizing your sleep is equally critical during treatment. Use our Sleep Calculator to establish optimal sleep schedules — immune function and drug metabolism are both profoundly impacted by sleep quality. Our dedicated article on sleep and its relationship to fatigue and daytime function may also be helpful for treatment-related fatigue management.
The Mental Health Crisis in Melanoma Survivors
This is the section that every other health website skips — and thousands of melanoma survivors desperately need.
Research consistently shows that 25–40% of melanoma survivors experience clinically significant anxiety or depression. For Stage III–IV patients, rates are even higher.
Common psychological challenges:
1. Scanxiety: The intense anxiety surrounding surveillance scans — particularly CT and PET scans. Many survivors describe the 2–3 weeks before a scan as the most psychologically difficult period of survivorship.
2. Fear of recurrence (FOR): A persistent, often intrusive fear that the cancer will return. FOR is normal and expected — but when it interferes with daily functioning, it meets criteria for clinical anxiety and deserves treatment.
3. Post-traumatic stress: Particularly in Stage III–IV patients, the trauma of a life-threatening diagnosis, complex treatment, and ongoing uncertainty can manifest as PTSD symptoms — intrusive thoughts, hypervigilance, avoidance.
4. Body image and surgical scars: Wide local excisions — particularly on the face, leg, or back — can leave significant scars. Lymph node dissections may cause lymphedema (chronic limb swelling). These physical changes profoundly affect self-image.
5. “Fear of the sun” anxiety: Many survivors develop excessive avoidance behaviors around sun exposure — refusing to go outdoors, social isolation, vitamin D deficiency. This is understandable but requires balanced guidance.
Evidence-based interventions that work:
| Intervention | Evidence Level | Notes |
|---|---|---|
| Cognitive Behavioral Therapy (CBT) | High (multiple RCTs) | Most effective for FOR and anxiety |
| Mindfulness-Based Stress Reduction (MBSR) | Moderate-High | Particularly effective for scanxiety |
| Support groups (in-person and online) | Moderate | Peer connection is powerfully therapeutic |
| Exercise (aerobic) | Moderate-High | Reduces depression and anxiety in survivors |
| Short-term medication (SSRI/SNRI) | High | For clinically significant depression/anxiety |
Where to find support:
- Melanoma Research Foundation: melanoma.org — patient support resources, community connections
- AIM at Melanoma Foundation: aimatmelanoma.org — survivorship resources
For a comprehensive guide to depression in medical contexts, see our depression guide.
Permanent Sun Protection: The Lifetime Protocol
After a melanoma diagnosis, sun protection is no longer optional — it is a medical necessity.
Non-negotiable lifetime rules for survivors:
- SPF 50+ every single day — including winter, cloudy days, and indoor days near windows (UVA penetrates glass)
- Reapply every 2 hours during outdoor activity; reapply after swimming or sweating
- UPF 50+ clothing for extended outdoor activity — long sleeves, wide-brim hat, UV-protective sunglasses
- Never use a tanning bed — not once, not ever, for any reason
- Avoid peak UV hours (10am–4pm) when possible
- Annual skin exam by a dermatologist — for life
- Monthly self-exam — for life
- Vitamin D via supplementation (1,000–2,000 IU daily) — never via intentional sun exposure
Returning to Work and Daily Life After Treatment
Immunotherapy and daily function: Many patients on pembrolizumab or nivolumab can maintain near-normal work and social function, particularly in the adjuvant setting. Infusions are administered every 3–6 weeks.
Common functional challenges:
- Fatigue (most common — present in 30–50% of patients on immunotherapy)
- Joint pain (immune-related arthritis)
- Skin rashes (common, usually manageable)
- GI upset (diarrhea — requires monitoring)
Work accommodations that can help:
- Flexible scheduling around infusion days (often the most fatiguing)
- Work-from-home options during acute irAE episodes
- Under the Americans with Disabilities Act (ADA), cancer patients are entitled to reasonable workplace accommodations
✅ What This Means For You
Finishing treatment is not the end of your melanoma journey — it’s the beginning of a new chapter that requires vigilance, self-care, and proactive mental health support. Build a surveillance plan with your oncologist, establish permanent sun protection habits, and don’t hesitate to seek psychological support. Survivorship is as much about living well as it is about staying cancer-free.
Global Perspectives, Expert Panel & Evidence Standards
Why Global Perspective Matters for Melanoma Patients
Melanoma is a global disease, but access to treatment varies dramatically by country. Understanding the international landscape helps American patients access the best available evidence — and recognize when their care may be lagging behind global standards.
International Treatment Access Comparison (2026)
| Country | Standard 1st-Line Stage IV | Opdualag Available | TIL Therapy Access | Clinical Trial Access |
|---|---|---|---|---|
| United States | Pembrolizumab / Opdualag / Nivo+Ipi | Yes (FDA 2022) | Yes (FDA 2024) | Highest globally |
| United Kingdom (NHS) | Pembrolizumab / Nivolumab | Yes (NICE-approved) | Limited (clinical trial only) | High |
| Australia | Pembrolizumab / Combination | Yes (TGA-approved) | Clinical trial | High — highest incidence drives research |
| Germany / EU | Pembrolizumab / Encorafenib+Binimetinib | Yes (EMA 2022) | Clinical trial | High |
| Canada | Pembrolizumab / Nivolumab | Yes | Clinical trial | Moderate |
| India | Pembrolizumab (limited affordability) | Very limited | Not available | Growing |
| Japan | Nivolumab / Pembrolizumab | Yes | Limited | Moderate |
Key insight for US patients: The United States currently offers the broadest access to approved melanoma treatments globally — including Opdualag and lifileucel (Amtagvi), both unavailable in many other countries. If you are receiving care at a specialized cancer center, you likely have access to the most advanced treatment options in the world.
European and International Guidelines (2026)
ESMO (European Society for Medical Oncology) — 2024 Update:
The 2024 ESMO Clinical Practice Guideline for cutaneous melanoma recommends:
- Pembrolizumab or nivolumab monotherapy as preferred first-line for Stage IV in PD-L1+ or unselected patients
- Combination nivo + ipi for high-burden disease where rapid response is needed
- BRAF/MEK inhibitors as alternative first-line for BRAF V600-mutated patients
- Testing for BRAF V600 mutation recommended from Stage IIB/C onwards
NCCN (National Comprehensive Cancer Network) — 2025–2026:
The NCCN Melanoma Guidelines (available in patient-friendly format at nccn.org) align with ESMO on systemic therapy but extend adjuvant treatment recommendations earlier — now including Stage IIB/IIC, whereas ESMO’s adjuvant recommendations historically started at Stage III.
Divergence point: European guidelines currently require a higher disease burden before recommending adjuvant immunotherapy. American (NCCN) guidelines extend this earlier. This divergence represents one of the key clinical debates in melanoma treatment entering 2026.
The Evidence Pyramid: How Confident Should You Be in Each Treatment?
| Treatment | Evidence Level | Supporting Studies | Confidence |
|---|---|---|---|
| Pembrolizumab adjuvant (III–IIC) | Level 1A | KEYNOTE-716, KEYNOTE-054 | ★★★★★ |
| Nivolumab adjuvant (Stage III) | Level 1A | CheckMate 238 | ★★★★★ |
| Nivo + Ipi Stage IV | Level 1A | CheckMate 067 | ★★★★★ |
| Dabrafenib + Trametinib adjuvant | Level 1A | COMBI-AD | ★★★★★ |
| Opdualag first-line Stage IV | Level 1B | RELATIVITY-047 | ★★★★☆ |
| Lifileucel (TIL therapy) | Level 1B | C-144-01 | ★★★★☆ |
| mRNA-4157 vaccine + pembro | Level 2B | KEYNOTE-942 (Phase IIb) | ★★★☆☆ |
| Nutrition interventions | Level 3 | Multiple observational | ★★★☆☆ |
| Exercise during treatment | Level 2A | Multiple RCTs | ★★★★☆ |
All major treatment recommendations referenced are based on peer-reviewed trials published in leading journals including NEJM, Lancet Oncology, JCO, and JAMA Oncology, and are consistent with guidelines from both the NCCN and ESMO.
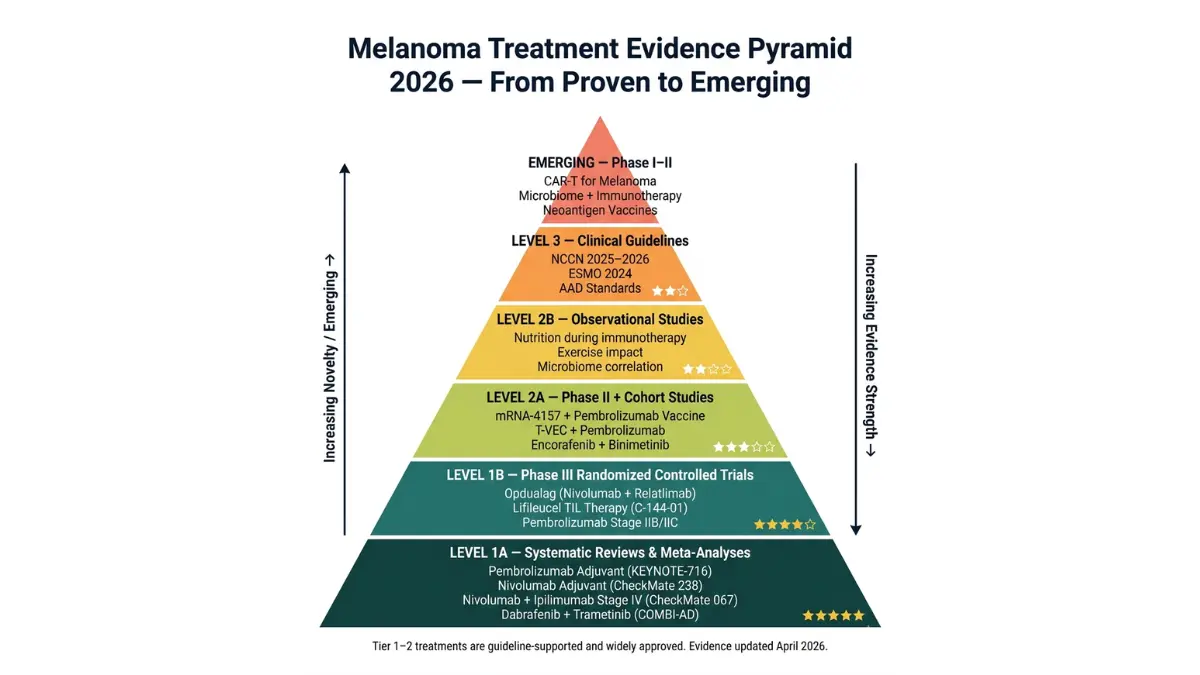
3 Real Patient Stories: Different Stages, Different Outcomes
Patient 1 — James, 41, Phoenix, Arizona: Stage IA Caught Early
James noticed a small changing mole on his forearm during a monthly self-exam he had started after a family friend was diagnosed with melanoma. The mole had been present for years but had recently developed a slight asymmetry and the color had deepened.
His dermatologist performed a dermoscopy examination and immediately recommended an excisional biopsy.
Result: Stage IA melanoma, Breslow depth 0.4mm, no ulceration, no lymph node involvement.
Treatment: Wide local excision with 1cm margins. Clean margins confirmed. No further treatment required.
Today: Eighteen months post-treatment, James remains cancer-free. He now volunteers with a melanoma awareness nonprofit in Phoenix and has convinced four friends and family members to get skin checks — two of whom were found to have atypical moles requiring removal.
Patient 2 — Denise, 54, Chicago, Illinois: Stage IIIB After Delayed Diagnosis
Denise had noticed a changing mole on her calf for approximately 14 months before seeing a dermatologist. Multiple visits to her primary care physician had reassured her the spot was “just a mole.”
When she finally saw a dermatologist, the biopsy returned Breslow depth 3.8mm with ulceration and a positive sentinel lymph node.
Stage: IIIB melanoma.
Treatment: Wide local excision with 2cm margins, completion lymph node dissection, followed by 1 year of adjuvant pembrolizumab.
Immunotherapy course: Denise completed 18 infusions of pembrolizumab. She experienced mild fatigue and a skin rash (Grade 1 immune-related dermatitis), both of which resolved without dose interruption.
Today: Three years post-surgery, Denise’s surveillance scans remain clear. She experiences ongoing “scanxiety” before her 6-monthly CT scans and has found a melanoma survivor support group to be transformative in managing the psychological burden.
Patient 3 — Roberto, 47, Miami, Florida: Stage IV — Clinical Trial Response
Roberto presented to his oncologist with two new skin nodules on his back and a PET scan showing bilateral lung lesions. Biopsy confirmed Stage IV melanoma with BRAF V600E mutation. His LDH was moderately elevated.
Treatment discussion: Roberto’s oncologist at a specialized cancer center offered two options — Opdualag (nivolumab + relatlimab) or enrollment in a clinical trial combining pembrolizumab with the mRNA-4157 neoantigen vaccine. Roberto chose the clinical trial.
Course: Roberto received lymphodepleting chemotherapy and was treated with mRNA-4157 + pembrolizumab. After four months, repeat PET scan showed a 62% reduction in tumor volume — a partial response. By month 9, complete radiological response was achieved.
Today: Roberto is 22 months post-treatment initiation, remains in complete radiological response on maintenance pembrolizumab, and has returned to full-time work as a restaurant owner. He credits his specialized cancer center, his clinical trial team, and his wife’s persistence in getting him to a melanoma specialist immediately after diagnosis.
The Research Horizon: What’s Coming in 2027–2030
Melanoma research is moving faster than in almost any other cancer field. Key developments to watch:
mRNA-4157 Phase III results (2027–2028): If the Phase III trial of Moderna/Merck’s personalized neoantigen vaccine confirms the Phase IIb data, this could become the first truly personalized cancer vaccine in routine clinical use for high-risk melanoma.
CAR-T cell therapy for melanoma: Early-phase trials are evaluating engineered CAR-T cells targeting melanoma-specific antigens. Results are preliminary but represent a potential fourth pillar of melanoma therapy alongside surgery, immunotherapy, and targeted therapy.
Gut microbiome and immunotherapy: Multiple studies have now demonstrated that the diversity and composition of the gut microbiome significantly predicts response to checkpoint inhibitor therapy. Microbiome modulation — through diet, probiotics, or fecal microbiota transplantation — is being studied as a strategy to improve immunotherapy response rates.
AI-powered early detection: Google DeepMind, IBM Watson, and multiple academic collaborators are developing AI systems capable of detecting melanoma from dermoscopy images with diagnostic accuracy approaching or exceeding expert dermatologists. These tools may democratize expert-level skin cancer screening globally.
Medical Expert Panel Reference
This guide is designed to reflect current guidelines and evidence from leading international institutions and medical bodies, including:
- National Cancer Institute (NCI) — treatment guidelines and epidemiological data
- American Cancer Society (ACS) — statistics, survivorship, and patient education
- National Comprehensive Cancer Network (NCCN) — evidence-based US clinical guidelines
- European Society for Medical Oncology (ESMO) — European clinical practice guidelines
- American Academy of Dermatology (AAD) — diagnostic standards and prevention recommendations
- Skin Cancer Foundation — ABCDE framework, early detection standards
- SEER (NCI Surveillance, Epidemiology, and End Results Program) — US epidemiological data
- MD Anderson Cancer Center — clinical trial leadership and surgical protocols
- Melanoma Research Foundation — patient advocacy and research funding priorities
📌 Disclaimer: This article is educational and informational only. It does not replace professional medical advice. Always consult a board-certified dermatologist or oncologist for diagnosis and treatment decisions. Statistics cited represent population averages and do not predict individual outcomes.
Frequently Asked Questions About Melanoma
1: Is melanoma always deadly?
No — melanoma is highly curable when detected early.
When found at Stage 0 or Stage I, melanoma is cured surgically in the vast majority of patients, with five-year survival rates of 97–100%. It is only when melanoma is allowed to advance to Stage III or IV — typically through delayed detection or delayed treatment — that mortality risk becomes significant. The critical message: melanoma kills people who wait. Melanoma caught early almost never kills.
2: How fast does melanoma spread if untreated?
Speed varies dramatically by subtype — from years to weeks.
Superficial spreading melanoma may grow slowly for 1–3 years before becoming invasive. Nodular melanoma, by contrast, can become deeply invasive within 6–12 weeks of first appearance. Acral lentiginous melanoma grows at an intermediate pace. Once any melanoma breaches the dermis and enters vertical growth phase, lymph node spread can occur within weeks to months. There is no “safe” window for delay.
3: Can melanoma be cured completely?
Yes — absolutely, when diagnosed at Stage 0–II.
Stage 0–I melanoma has cure rates approaching 99–100% with surgery alone. Even Stage II patients have excellent outcomes with surgical removal and surveillance. Stage III is increasingly curable with adjuvant immunotherapy. Stage IV can achieve complete, durable remission in 20–30% of patients treated with modern immunotherapy combinations — a number that was previously near zero. “Cured” is a term used cautiously in oncology, but functional long-term remission is absolutely achievable at all stages with today’s treatments.
4: What does Stage 1 melanoma look like?
Usually a flat, changing mole with irregular features — no raised bump required.
Stage I melanoma typically appears as a flat or slightly raised lesion with asymmetric shape, irregular or notched borders, multiple shades of brown or black, and possibly a faint reddish or white component. Breslow depth is ≤2mm — meaning it hasn’t grown deep into the skin yet. The lesion is most commonly located on the back in men and the legs in women. The key visual trigger: any mole that is changing in size, shape, or color over weeks to months.
5: Can you get melanoma without sun exposure?
Yes — acral lentiginous and mucosal melanomas occur on sun-protected skin.
Approximately 10–15% of melanomas develop on body areas that receive little or no UV exposure — including the palms, soles, under nails, and on mucous membranes. These subtypes are driven by genetic instability rather than UV damage. Ocular melanoma similarly occurs independently of sun exposure. While UV radiation is the dominant cause of cutaneous melanoma, the absence of sun exposure does not mean zero melanoma risk.
6: What is the ABCDE rule for melanoma?
A framework for visually identifying suspicious skin lesions — Asymmetry, Border, Color, Diameter, Evolving.
The ABCDE rule provides a structured checklist for evaluating moles. A = one half doesn’t match the other; B = irregular or jagged edges; C = multiple colors within the same lesion; D = diameter greater than 6mm (or any unusually dark lesion); E = evolving in size, shape, color, or new symptoms like itching or bleeding. The “E” criterion — evolution — is clinically considered the most important, as any change in a skin lesion demands professional evaluation.
7: How long can you live with Stage 4 melanoma?
Longer than ever before — the treatment revolution has transformed outcomes.
Before 2010, median Stage IV melanoma survival was approximately 8–9 months and very few patients survived five years. With modern immunotherapy combinations (checkpoint inhibitors, Opdualag, TIL therapy), approximately 35–50% of Stage IV patients in clinical trials achieve five-year survival, and a subset experiences durable complete remissions lasting a decade or longer. These numbers continue to improve with each new treatment generation. For more specific guidance on metastatic melanoma treatment options, see our detailed article on Stage 4 melanoma treatment and therapy.
8: Does melanoma itch or hurt?
It can — and new itching or tenderness in a mole is a warning sign.
Early melanoma is typically asymptomatic. However, as it grows and becomes more vascular or inflammatory, itching, tingling, tenderness, or burning within or around a mole can develop — all of which are listed as “E (evolving)” warning signs under the ABCDE framework. Bleeding or crusting without trauma is particularly concerning. Importantly, the absence of pain does not mean a lesion is benign. Most melanomas are painless until they have grown quite large or have metastasized.
9: What is the difference between a mole and melanoma?
Normal moles are symmetric, uniformly colored, have smooth borders, remain stable, and are typically smaller than 6mm. Melanoma shows the opposite pattern.
Normal benign moles (common nevi) develop during childhood and adolescence, are uniformly brown or tan, have smooth round or oval borders, and do not change over time. They are symmetric and smaller than 6mm. Melanoma typically develops later in life, shows color variation, asymmetry, irregular borders, and crucially — it changes. The most reliable differentiating feature is change over time. A mole that has been identical for 20 years is reassuring; a mole that has changed in the past 2 months is not.
10: Can melanoma appear on dark skin?
Yes — and it is frequently missed and diagnosed at a more advanced stage in people with darker skin tones.
Melanoma can develop in people of any skin color. In Black, Asian, and Hispanic individuals, the most common subtype is acral lentiginous melanoma — appearing on the palms, soles, and nail beds. Because these areas are sun-protected and often less scrutinized during skin checks, diagnosis is frequently delayed. The five-year survival rate for Black patients with melanoma is approximately 70% — compared to 95% for White patients — entirely explained by later stage at diagnosis and systemic healthcare disparities. Regular self-examination of palms, soles, and nails is essential for all patients, regardless of skin color.
11: What should I do if I think I have melanoma?
Act within 1–2 weeks — do not wait for a routine appointment.
If you have a mole or skin lesion showing ABCDE warning signs, or any lesion that is changing, bleeding, or not healing within 3–4 weeks: (1) call a board-certified dermatologist and describe what you’re seeing — most practices will prioritize suspected melanoma; (2) photograph the lesion today for comparison at your appointment; (3) do not attempt to remove, scratch, or treat the lesion yourself; (4) avoid excessive sun exposure to the area; (5) if you cannot reach a dermatologist within 1–2 weeks, visit an urgent care clinic with dermoscopy capability. Early action is the single most important variable in melanoma outcomes.
Summary: The 10 Most Important Things to Know About Melanoma in 2026
- Melanoma kills one American every hour — but 99% of Stage I cases are cured surgically.
- E (Evolving) is the most important ABCDE letter — any changing mole needs evaluation.
- Amelanotic and nodular melanoma don’t look like “classic” melanoma — they are the most missed.
- People of color get melanoma too — acral lentiginous melanoma on soles and nail beds is frequently detected late.
- Stage IIC has worse survival than Stage IIIA — do not minimize a Stage II diagnosis.
- Treatment delay kills — treated >119 days after biopsy carries a 41% higher death risk.
- 2026 immunotherapy has transformed Stage IV — 40–50% five-year survival in responders vs. 5–10% in 2009.
- BRAF testing is mandatory for Stage III–IV — determines whether targeted therapy is an option.
- Monthly skin self-exams save lives — establish this habit today.
- Melanoma in the sun-protected era is mostly preventable — SPF 50+, no tanning beds, annual dermatologist check.
References and External Resources
All statistics and clinical data referenced in this article are drawn from or consistent with:
- National Cancer Institute — Melanoma Treatment PDQ
- American Cancer Society — Melanoma Key Statistics 2026
- American Cancer Society — Melanoma Survival Rates by Stage
- Skin Cancer Foundation — ABCDE Warning Signs
- Skin Cancer Foundation — Skin Cancer Facts & Statistics
- SEER Database — Melanoma Statistics
- NCBI StatPearls — Cutaneous Malignant Melanoma
- American Cancer Society — Treatment by Stage
- NCCN Patient Guidelines — Melanoma 2026
- Cleveland Clinic — Melanoma
- AIM at Melanoma Foundation — Prognosis and Survival
- NCBI PMC — Melanoma Staging and Follow-Up
- ClinicalTrials.gov — Active Melanoma Trials
- Melanoma Research Foundation
- American Cancer Society — What Is Melanoma
- AAD — Melanoma Symptoms
- Skin Cancer Foundation — How Dangerous Is Melanoma: Timing
- Cure Melanoma — Melanoma 101
- NCI — Cancer Staging Overview
Related Articles on MyMedicineAdvisor:
- Melanoma 2026: AI Screening and Survival
- Stage 4 Melanoma: Survival and Therapy Options
- Skin Cancer Warning Signs: 12 Symptoms
- Basal Cell Carcinoma: Cure Rate and Treatment
- How Immunotherapy Works
- Radiation Therapy: Complete Guide
- Chemotherapy Guide 2026: Side Effects
- Understanding Your Biopsy Results
- CT Scan Findings: What Happens Next
- How to Reduce Anxiety Naturally
⚠️ Medical Disclaimer: This article is intended for educational and informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always seek the guidance of your physician, dermatologist, or oncologist with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay seeking it because of something you have read in this article. If you think you may have a medical emergency, call your doctor or emergency services immediately.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.