On This Page – Quick Medical Summary
You’ve been told you need a prostate biopsy — here’s what that means
If your doctor has recommended a prostate biopsy, you’re likely here for one of three reasons. You may be facing the procedure and want to know what actually happens. You may have your results in hand and need help reading the unfamiliar numbers, or you may be deciding whether to go ahead at all.
This guide follows each path: what a biopsy is and why it was suggested, what to expect on the day, how to recover safely, and what a Gleason score or Grade Group means once results arrive. Our overview of prostate cancer signs and stages covers the wider picture.
First, some grounding. Prostate cancer is common — about 1 in 8 men are diagnosed in their lifetime — and a biopsy is a step toward an answer, not a diagnosis in itself and not a confirmation that you have cancer.
📊 Clinical Data Point: About 1 in 8 men will receive a prostate cancer diagnosis in their lifetime; an estimated 333,830 new U.S. cases and 36,320 deaths are projected for 2026. — Source: American Cancer Society, Key Statistics for Prostate Cancer (Cancer Statistics 2026)
ℹ️ Medical Disclaimer: This article explains the prostate biopsy procedure, recovery, and how results such as the Gleason score and Grade Group are reported. It is general health education — not a diagnosis, treatment plan, medication guidance, or substitute for personalized care. Decisions about whether to have a biopsy, how to interpret your specific results, and what monitoring or treatment is right for you should be made with a board-certified urologist who knows your full medical history.
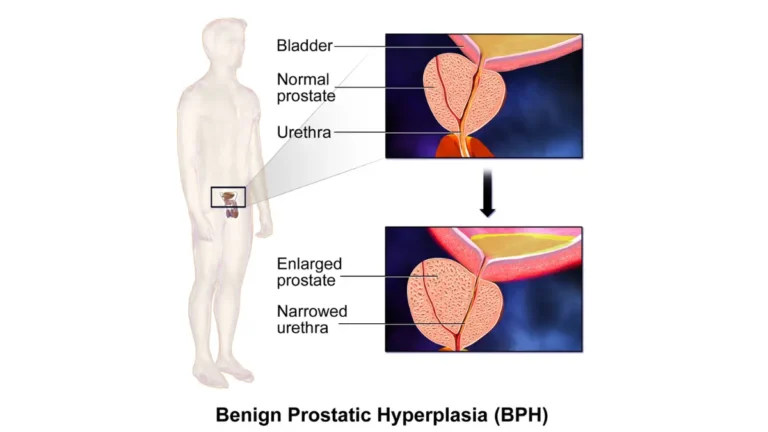
Why a biopsy was recommended — and the MRI step that often comes first
A biopsy is usually suggested after an elevated PSA result, an abnormal finding on a digital rectal exam, or a suspicious area on prostate imaging. None of these confirms cancer on its own; they are signals that the prostate needs a closer look.
What an elevated PSA actually tells you (and what it doesn’t)
PSA, or prostate-specific antigen, is a protein measured in a simple blood test. A raised level can come from cancer, but it is also commonly raised by benign causes such as an enlarged prostate or inflammation (prostatitis). Seeing how PSA levels are interpreted by age helps put one result in context.
🔬 How It Works: A PSA test measures a protein your prostate releases into the blood. It cannot show why the level is high — only a tissue sample taken at biopsy can tell cancer apart from a benign cause.
Do I need an MRI before the biopsy?
Current guidelines support an MRI of the prostate before a first biopsy, because it improves detection of clinically significant cancer and helps target where to sample. Suspicious areas are scored on a standard scale called PI-RADS, from 1 to 5. You can read the current AUA biopsy guidance for the full recommendations.
📊 Clinical Data Point: In the PRECISION trial, MRI-targeted biopsy detected clinically significant prostate cancer in 38% of men, versus 26% with systematic biopsy alone. — Source: AUA/SUO Early Detection of Prostate Cancer Guideline, citing PRECISION (New England Journal of Medicine, 2018)
A family history of prostate cancer, or a known inherited mutation, can raise your risk and may shape screening decisions. You can assess your inherited risk factors and bring the result to your appointment.
✅ Patient Action: Ask your urologist: “Given my PSA and MRI findings, do you recommend a targeted, systematic, or combined biopsy — and why?”
What to expect during a prostate biopsy
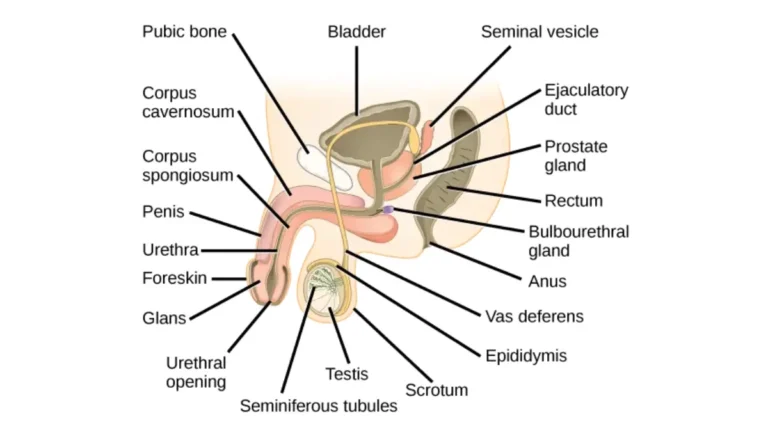
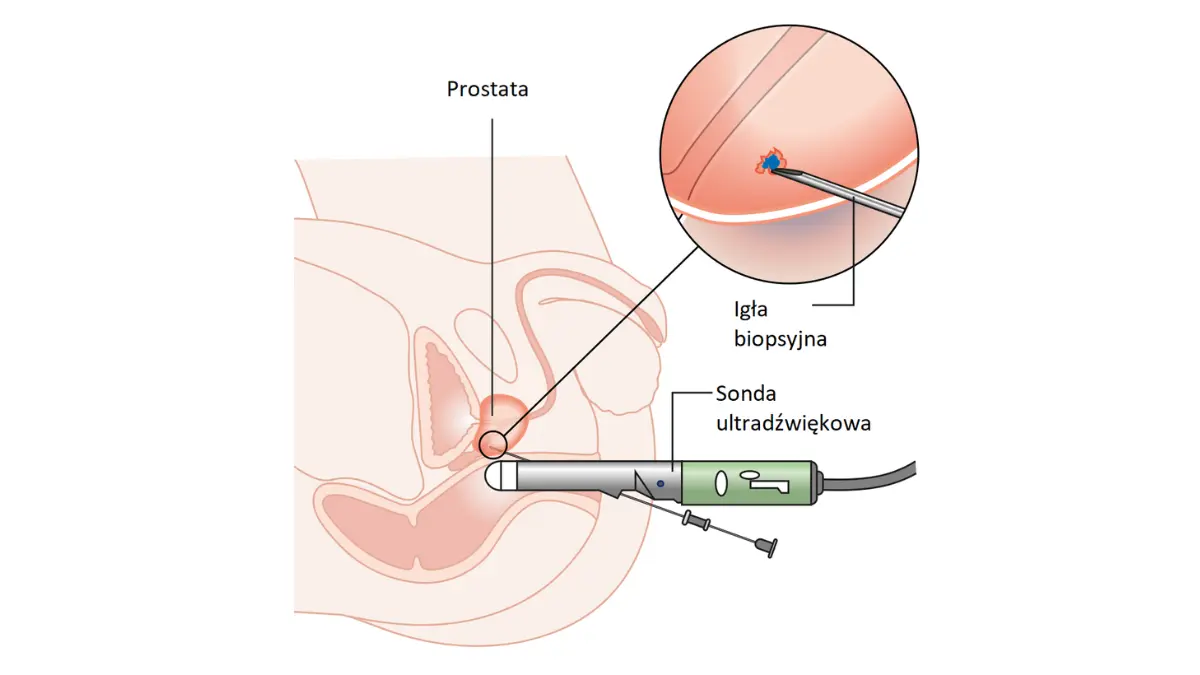
A prostate biopsy uses a thin needle, guided by ultrasound or MRI fusion, to take small tissue samples — called cores — from the prostate. It is usually done as an outpatient procedure under local anesthetic.
How to prepare
Your team will give you specific instructions, which usually include taking prescribed antibiotics to lower infection risk and reviewing any blood-thinning medications beforehand. Tell your doctor about every medicine and supplement you take.
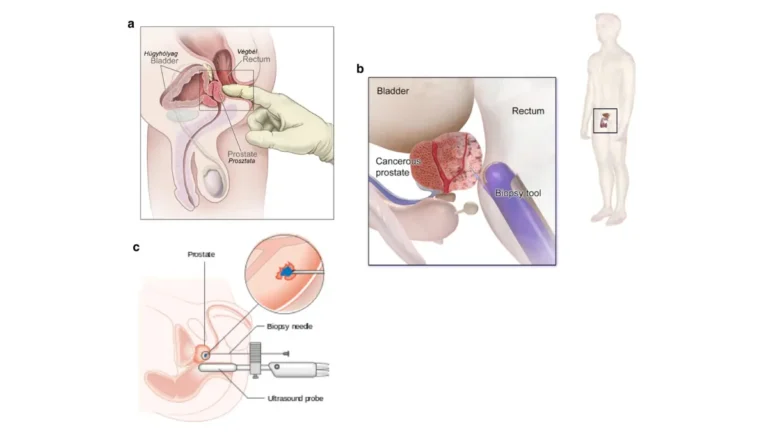
Transrectal vs transperineal: the two routes
There are two main routes for the needle: transrectal (through the rectal wall) and transperineal (through the skin behind the scrotum). Current AUA guidance allows either route and does not declare one superior for cancer detection; where the technology is available, an MRI-ultrasound fusion biopsy is recommended.
How many cores are taken and how long it takes
A standard systematic biopsy takes about 12 cores; when an MRI has flagged a target, guidelines advise at least two cores from that target. A step-by-step overview of the procedure can help you picture the day. The biopsy itself is brief, usually finished in well under half an hour.
📊 Clinical Data Point: A standard systematic prostate biopsy samples about 12 cores; for an MRI-suspicious target, at least 2 cores per target are advised, with limited added value beyond roughly 3 cores per target. — Source: AUA/SUO Early Detection of Prostate Cancer Guideline, Part II (2023)
Recovery and side effects: what’s normal and when to call
Most men tolerate a prostate biopsy well, and the common after-effects are minor and pass on their own. Serious complications are uncommon, but knowing the warning signs lets you act quickly if one appears.
Common, usually harmless side effects
In the days after a biopsy, it is normal to see some blood in the urine, blood in the semen (which can last for several weeks), and minor bleeding from the biopsy site. A short-lived dip in erectile function has also been reported and is generally temporary.
Transrectal vs transperineal and infection risk
Infection is the complication doctors watch most closely. Reported urinary infection and sepsis rates after biopsy are low, and the transperineal route has been linked to a lower infection risk than the transrectal route in pooled studies.
📊 Clinical Data Point: Across studies, post-biopsy urinary tract infection is reported in roughly 0.1%–7% of cases, and sepsis in roughly 0.3%–0.8% after transrectal biopsy (wider ranges are reported by region and antibiotic regimen). — Sources: Acosta et al., International Journal of Urology (2022); Journal of Urology
🔬 How It Works: Antibiotics given before the procedure reduce the chance that bacteria introduced during sampling cause a urinary infection — one reason prophylaxis is standard practice.
Warning signs: when to call the doctor
Some symptoms need prompt attention. Contact your urologist or seek urgent care if you notice any of the following:
- A fever with chills (a possible sign of a bloodstream infection)
- Inability to pass urine
- Heavy or persistent bleeding that does not settle
- Worsening pain instead of gradual improvement
⚠️ Clinical Warning: A fever with shaking chills after a prostate biopsy can signal a serious bloodstream infection (sepsis) and is a medical emergency. Do not wait — seek emergency care the same day.
Understanding your results: Gleason score and Grade Group
When your results arrive, the pathology report describes whether cancer was found and, if so, how aggressive the cells look. Two linked systems carry this information: the Gleason score and the Grade Group. A general walkthrough of how to decode a pathology report can make the page less daunting.
What the Gleason score measures
A pathologist examines the two most common cell patterns in your samples and grades each from 3 to 5 (lower-numbered patterns are essentially no longer assigned). The two grades are added together, with the most common pattern listed first — for example, 3 + 4 = 7. What a Gleason score means for prognosis is covered separately in more depth.
The Grade Group system (1–5) and how it maps to Gleason
The Grade Group system, used alongside Gleason, simplifies the report into five groups.
| Grade Group | Gleason score | What it generally indicates |
|---|---|---|
| Grade Group 1 | 6 or less (3+3) | Least aggressive; often slow-growing |
| Grade Group 2 | 3+4 = 7 | Favorable intermediate |
| Grade Group 3 | 4+3 = 7 | Less favorable intermediate |
| Grade Group 4 | 8 (4+4) | High grade |
| Grade Group 5 | 9–10 | Most aggressive |
Sources: National Cancer Institute (Grade Group); American Cancer Society, Understanding Your Pathology Report: Prostate Cancer.
Why Gleason 3+4 and 4+3 are not the same
Both add up to 7, but they are not equivalent. In 3+4 (Grade Group 2) the less-aggressive pattern dominates, while in 4+3 (Grade Group 3) the more-aggressive pattern leads — which is why the order of the numbers matters.
🩺 Physician Note: A common point of confusion is treating every Gleason 7 result as the same. Current grading deliberately separates 3+4 from 4+3 because the dominant pattern changes the outlook.
What your result means for next steps
Once results are back, what happens next depends on what the biopsy found. Knowing what the results timeline and report typically look like can ease the wait. There are three common scenarios, and each has a recognized path.
If your biopsy is negative (but your PSA is still high)
A negative biopsy is a real and common outcome, and it is reassuring. It does not always rule cancer out completely, though, because a systematic biopsy can miss disease that targeted sampling might catch — so your doctor may suggest continued PSA monitoring, repeat imaging, or a repeat biopsy if suspicion remains. Tracking any new or changing prostate symptoms is part of that follow-up.
Grade Group 1: what active surveillance means
If low-grade cancer (Grade Group 1) is found, many men are offered active surveillance rather than immediate treatment. This means active monitoring — repeat PSA tests, imaging, and biopsies over time — not “doing nothing,” and it is designed to avoid over-treating cancers unlikely to cause harm. Seeing how grade relates to overall stage can help the bigger picture make sense.
Higher Grade Groups: moving to a treatment conversation
Higher Grade Groups generally prompt a discussion about treatment, such as surgery or radiation, chosen according to your overall risk and health. If surgery is on the table, here is what prostate surgery involves, including cost and outcomes.
✅ Patient Action: Ask your urologist: “Based on my Grade Group and how much cancer was found, is monitoring, further testing, or treatment the right next step for me?”
Before your appointment: a quick prep and red-flag checklist
Use this as a quick reference — for the procedure, for your results visit, and for recovery. A partner or caregiver can use it too.
Quick prep checklist
- Confirm the route (transrectal or transperineal) and whether you’ll have an MRI-fusion biopsy
- Review all medications and supplements, especially blood thinners, with your doctor
- Take prescribed antibiotics exactly as directed
- Arrange a ride home if you’ll be sedated
- Write down your questions before the results appointment
Call-the-doctor-now signs
- Fever with chills
- Inability to urinate
- Heavy or persistent bleeding
- Worsening rather than improving pain
✅ Patient Action: Save this checklist or screenshot it, and bring your written questions to the results appointment.
Prostate biopsy: frequently asked questions
1. Is a prostate biopsy painful?
A prostate biopsy is usually done under local anesthetic, so most men feel pressure and brief discomfort rather than sharp pain. Some soreness afterward is normal and settles within a few days. If you’re anxious about it, ask your urologist about anesthesia or sedation options.
2. How many cores are taken in a prostate biopsy?
A standard systematic prostate biopsy takes about 12 cores, which are small tissue samples. When an MRI has identified a suspicious target, guidelines advise at least two cores from that target, with little added benefit beyond about three.
3. Transrectal or transperineal — which is safer?
Current AUA guidance allows either route and finds similar cancer-detection rates. The transperineal route has been linked to a lower infection risk in pooled studies, though high-quality randomized data are still limited. Which route suits you depends on your history and your urologist’s experience.
4. Do I need an MRI before a prostate biopsy?
Guidelines support an MRI of the prostate before a first biopsy because it improves detection of clinically significant cancer and can guide where to sample. Suspicious areas are scored on the PI-RADS scale from 1 to 5. Ask your urologist whether your plan includes targeted, systematic, or combined sampling.
5. How long does it take to get prostate biopsy results?
Pathology results are typically available within about a week, though timing varies by lab and whether extra testing is ordered. Your urologist’s office will usually arrange a follow-up to walk through the report, so ask up front when and how you’ll receive it.
6. What does Gleason 3+4 mean compared with 4+3?
Both add up to 7, but they differ. In 3+4 (Grade Group 2) the less-aggressive pattern dominates; in 4+3 (Grade Group 3) the more-aggressive pattern leads, which generally carries a less favorable outlook. The order of the numbers matters, so discuss what your specific score means with your urologist.
7. Can a prostate biopsy miss cancer?
Yes. A systematic biopsy samples parts of the prostate and can miss cancer that MRI-targeted sampling might detect. That’s why a negative result doesn’t always rule cancer out, and why ongoing PSA monitoring or repeat testing may be advised if suspicion remains. Discuss the right follow-up timing with your urologist.
8. What if my prostate biopsy is negative but my PSA is still high?
A negative biopsy with a persistently high PSA usually means continued follow-up rather than treatment — repeat PSA tests, imaging, or a repeat biopsy depending on your level of risk. An elevated PSA has many causes besides cancer. Your urologist will decide which monitoring plan fits your situation.
9. What is active surveillance for Grade Group 1?
Active surveillance is structured monitoring of low-grade (Grade Group 1) prostate cancer rather than immediate treatment. It typically includes regular PSA tests, imaging, and repeat biopsies, with treatment offered if the cancer shows signs of progressing. It avoids over-treating cancers unlikely to cause harm, so discuss eligibility with your urologist.
10. When should I call the doctor after a prostate biopsy?
Contact your urologist or seek urgent care for a fever with chills, inability to pass urine, heavy or persistent bleeding, or worsening pain. A fever with shaking chills can signal a bloodstream infection and is a same-day emergency. Minor blood in the urine or semen is common and usually settles on its own.
11. How do I prepare for a prostate biopsy?
Confirm the biopsy route, take any prescribed antibiotics exactly as directed, and review all medications — especially blood thinners — with your doctor beforehand. Arrange a ride home if you’ll be sedated, and write down your questions in advance. Your urologist’s office will give you specific instructions.
The bottom line on your prostate biopsy
A prostate biopsy is a step toward clarity, and much of what it finds is manageable — including negative results and low-grade cancers that are simply monitored. Whatever your report says, you now know how to read the Gleason score and Grade Group, what recovery should look like, and which symptoms mean “call now.”
For the full picture, see our complete guide to prostate cancer signs, stages, and treatment. And bring your specific questions — and your results — to a urologist who knows your history.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.