On This Page – Quick Medical Summary
If you’ve just learned that your prostate cancer carries a BRCA or other inherited DNA-repair mutation, a new option may have entered the conversation: a PARP inhibitor. PARP inhibitors are a form of targeted therapy — pills that exploit a specific weakness in cancer cells that cannot properly repair their own DNA.
This guide is written for three readers. If you’ve been newly told you carry a BRCA mutation with advanced prostate cancer, Sections 2 through 4 explain why the mutation matters and which drugs apply. If you’re comparing treatments, Sections 4 and 5 cover the approved options and how well they work. If you’re a caregiver, or deciding whether to get genetic testing at all, Sections 3 and 7 are for you.
A mutation that sounds alarming can, in this one respect, open a door. Understanding that door — who qualifies, what to expect, and what to ask — is what the rest of this page is for, alongside our broader overview of how prostate cancer is staged and treated.
ℹ️ Medical Disclaimer: This article is general health education — not a diagnosis, treatment recommendation, or substitute for personalized care. PARP inhibitors, genetic testing, and prostate cancer treatment involve regulated medications and procedures that must be guided by a board-certified medical oncologist or urologist who knows your case. Consult your care team, and a certified genetic counselor where relevant, before acting on anything here.
How PARP inhibitors work against prostate cancer
Cancer cells survive by constantly repairing damage to their DNA, and PARP inhibitors interfere with one repair system they depend on. The benefit is largest in cancers that have already lost a second repair system — which is exactly what a BRCA mutation causes.
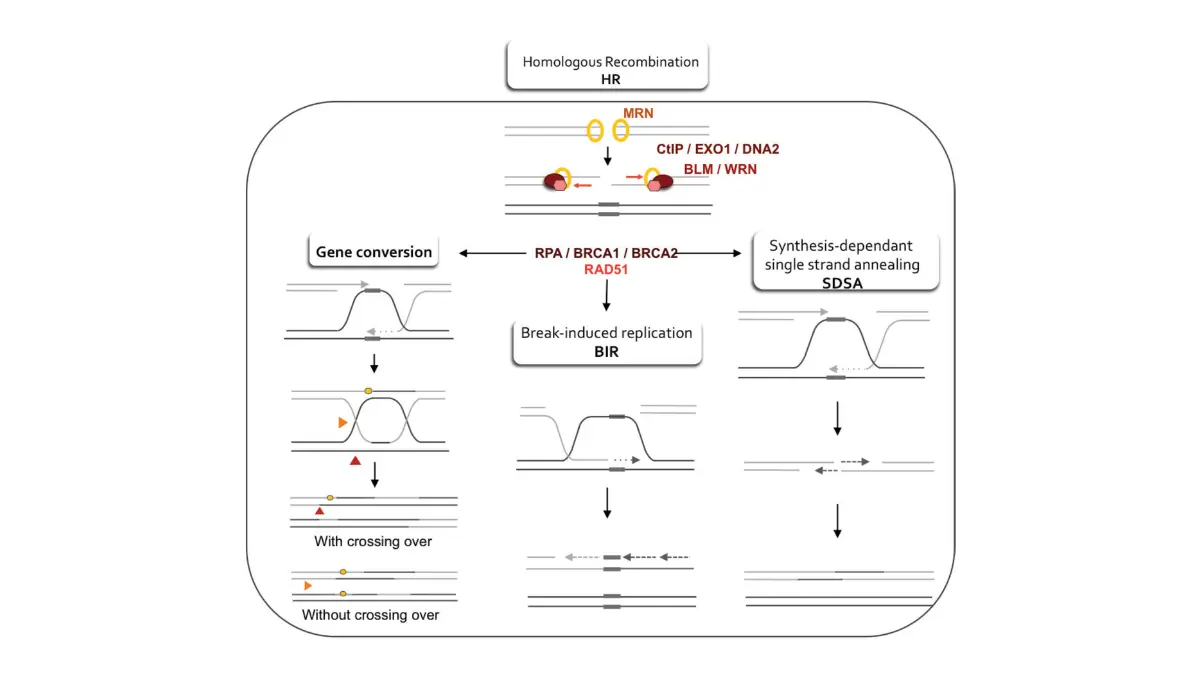
What PARP and BRCA genes normally do
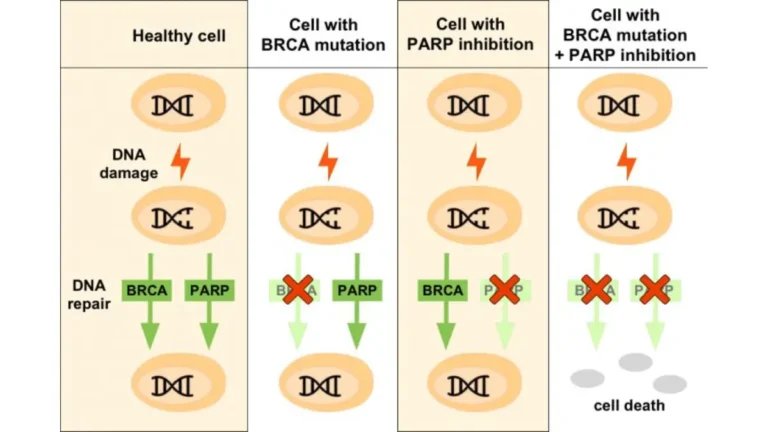
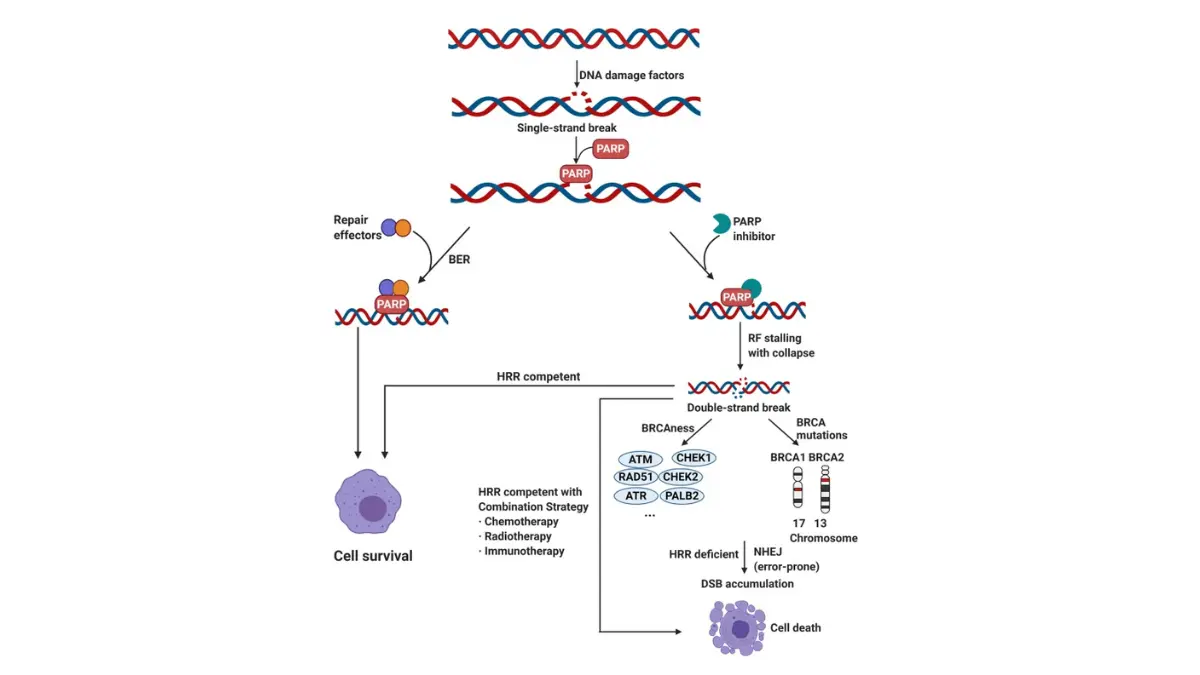
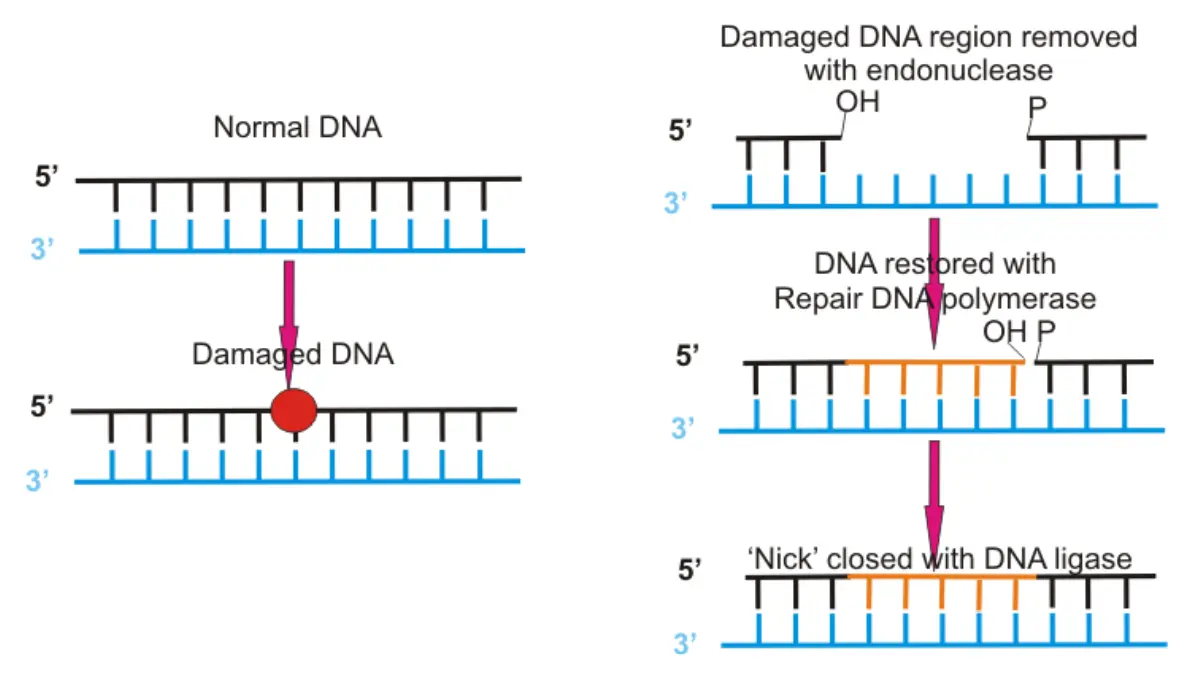
Cells use several tools to fix DNA damage. The PARP enzyme repairs single-strand breaks, while BRCA1, BRCA2, and other homologous recombination repair (HRR) genes fix more serious double-strand breaks. Most healthy cells can fall back on whichever system stays intact.
Why a “second hit” kills the cancer cell
🔬 How It Works: When a cancer cell already carries a faulty BRCA or HRR gene, it leans heavily on PARP to survive. Blocking PARP removes that backup, so DNA damage accumulates unrepaired and the cancer cell dies — while cells with working repair are relatively spared. Scientists call this “synthetic lethality”: neither defect alone is fatal, but together they are.
This is why testing comes first — the drug’s logic depends on which repair genes your cancer has lost.
Genetic testing: who qualifies and which mutations matter
Genetic testing is the gateway to PARP inhibitor treatment, because the drugs are approved only for cancers with specific mutations. Genetic testing here comes in two forms, and many men need both.
Germline vs. tumor (somatic) testing
A germline test uses blood or saliva to find inherited mutations you were born with — results that also matter for blood relatives. A somatic (tumor) test reads mutations inside the cancer itself. In advanced prostate cancer, roughly 30% of HRR alterations are inherited, so the two tests answer different questions. A positive inherited result is covered in our guide to what a positive BRCA test means.
Who guidelines recommend for testing
National Comprehensive Cancer Network (NCCN) guidance recommends genetic testing for prostate cancer patients including:
- All men with metastatic, regional, high-risk, or very-high-risk disease, regardless of family history
- Men with a family history of prostate, breast, ovarian, or pancreatic cancer
- Men with Ashkenazi Jewish ancestry
- Men with intraductal or ductal tumor features
Eligibility often turns on your stage and risk category, which your oncologist will confirm.
Which mutations make a PARP inhibitor likely to help
Not every mutation carries equal weight. The strongest evidence supports BRCA2, with weaker evidence for BRCA1 and limited evidence for other HRR genes like ATM, CHEK2, and PALB2, per the NCI’s overview of inherited prostate cancer risk.
✅ Patient Action: Ask your oncologist: “Have I had both germline and tumor genomic testing, and which specific mutations were found?” Bring the actual report. You can also review your inherited-cancer risk factors before the visit.
The four FDA-approved PARP inhibitors — and who each is for
Four PARP inhibitors are FDA-approved for prostate cancer, used alone or with hormone therapy and matched to your mutation and stage. Olaparib (Lynparza) and rucaparib (Rubraca) are approved as single agents; talazoparib (Talzenna) and niraparib are approved in combinations.
| Drug (brand) | Partner therapy | Eligible mutation | Best for (setting) |
|---|---|---|---|
| Olaparib (Lynparza) | Used alone | Several HRR genes, incl. BRCA | mCRPC after enzalutamide or abiraterone |
| Olaparib (Lynparza) | Abiraterone + prednisone | BRCA | First-line mCRPC |
| Rucaparib (Rubraca) | Used alone | BRCA | mCRPC after a hormone agent and chemotherapy |
| Talazoparib (Talzenna) | Enzalutamide | HRR genes | First-line mCRPC |
| Niraparib (Akeega) | Abiraterone + prednisone | BRCA (mCRPC); BRCA2 (hormone-sensitive) | First-line mCRPC; 2025 option for BRCA2 hormone-sensitive disease |
Source: FDA approvals, 2020–2025. mCRPC = metastatic castration-resistant prostate cancer.
Single-agent vs. combination — what determines which
Whether you take a PARP inhibitor alone or with hormone therapy depends on your mutation, your stage, and prior treatments. Single-agent olaparib and rucaparib are generally used after earlier therapy, while combinations are first-line. Rucaparib’s approval follows prior chemotherapy, whereas combinations pair a PARP inhibitor with hormone therapy such as abiraterone or enzalutamide.
The newest expansion (2025)
📊 Clinical Data Point: On December 12, 2025, the FDA approved niraparib plus abiraterone and prednisone for men with BRCA2-mutated metastatic castration-sensitive (hormone-sensitive) prostate cancer — the first PARP-inhibitor combination cleared for the hormone-sensitive setting. — Source: the FDA’s December 2025 approval announcement.
If you don’t carry a qualifying mutation, other precision treatments such as Pluvicto (lutetium-177) may be options to discuss instead.
How well do PARP inhibitors work for BRCA+ prostate cancer?
For men with BRCA-altered advanced prostate cancer, PARP inhibitors can meaningfully delay cancer growth and extend survival versus standard hormone agents — though these are trial averages, not personal guarantees. The clearest evidence comes from the PROfound trial of olaparib.
What PROfound showed for BRCA-altered disease
📊 Clinical Data Point: In PROfound’s BRCA subgroup, men on olaparib had median radiographic progression-free survival of 9.8 months versus 3.0 months with enzalutamide or abiraterone, and median overall survival of 20.1 versus 14.4 months. — Source: de Bono et al., New England Journal of Medicine, 2020; PROfound BRCA subgroup analysis, Journal of Clinical Oncology, 2023.
These numbers describe men whose cancer had already progressed on hormone therapy, so they aren’t a forecast for any one person.
How to read “progression-free” and “survival”
Radiographic progression-free survival is the time before scans show growth; overall survival is time from treatment start. One caveat: 69% of the comparison group later crossed over to olaparib, which likely narrowed the measured survival gap. You can see the study itself in the PROfound trial record, and our guide to the outlook for advanced prostate cancer adds context.
✅ Patient Action: Ask your medical oncologist: “Based on my specific mutation and how my cancer has behaved, what benefit is realistic, and how will we know if the drug is working?”
Side effects and what monitoring to expect
Most men tolerate PARP inhibitors, but the drugs carry a predictable set of side effects and a few uncommon risks. Anemia and fatigue are the most common, and routine blood tests track them throughout treatment.
Common side effects
Across prostate cancer trials, the most frequent side effects of olaparib were anemia (low red blood cells, roughly 36–50% of men), fatigue or weakness (roughly 42–55%), nausea (roughly 43–60%), and decreased appetite (roughly 22–31%), per the FDA prescribing information for olaparib.
📊 Clinical Data Point: In the PROfound safety analysis, these effects were mostly mild to moderate, typically peaked within the first two months, and were usually managed with dose interruptions or reductions rather than stopping treatment. — Source: PROfound safety and tolerability analysis, European Journal of Cancer, 2022.
Serious but uncommon risks
⚠️ Clinical Warning: Rarely, PARP inhibitors are linked to serious blood disorders (myelodysplastic syndrome or acute myeloid leukemia), lung inflammation (pneumonitis), and blood clots. In PROfound, MDS/AML occurred in under 1% and pneumonitis in about 2% of men on olaparib. Report new shortness of breath, a persistent cough, unusual bruising or bleeding, or leg swelling promptly.
Monitoring during treatment
Because low blood counts are common, your team checks blood work regularly, especially in the early months.
✅ Patient Action: Ask your oncology team: “Which side effects should I report the same day, and how often will my blood counts be checked?”
Your next steps — and what a BRCA result means for your family
Understanding your options is the first step; the next is confirming your testing and recognizing that an inherited result reaches beyond you. A BRCA mutation found on a germline test has implications for blood relatives.
Questions to bring to your oncologist
Walking in prepared changes the conversation. Useful questions include:
- Have I had both germline and tumor genomic testing?
- Do my mutations make me eligible for a PARP inhibitor, alone or combined?
- What benefits and side effects are realistic for my situation?
- Should other precision treatments be considered?
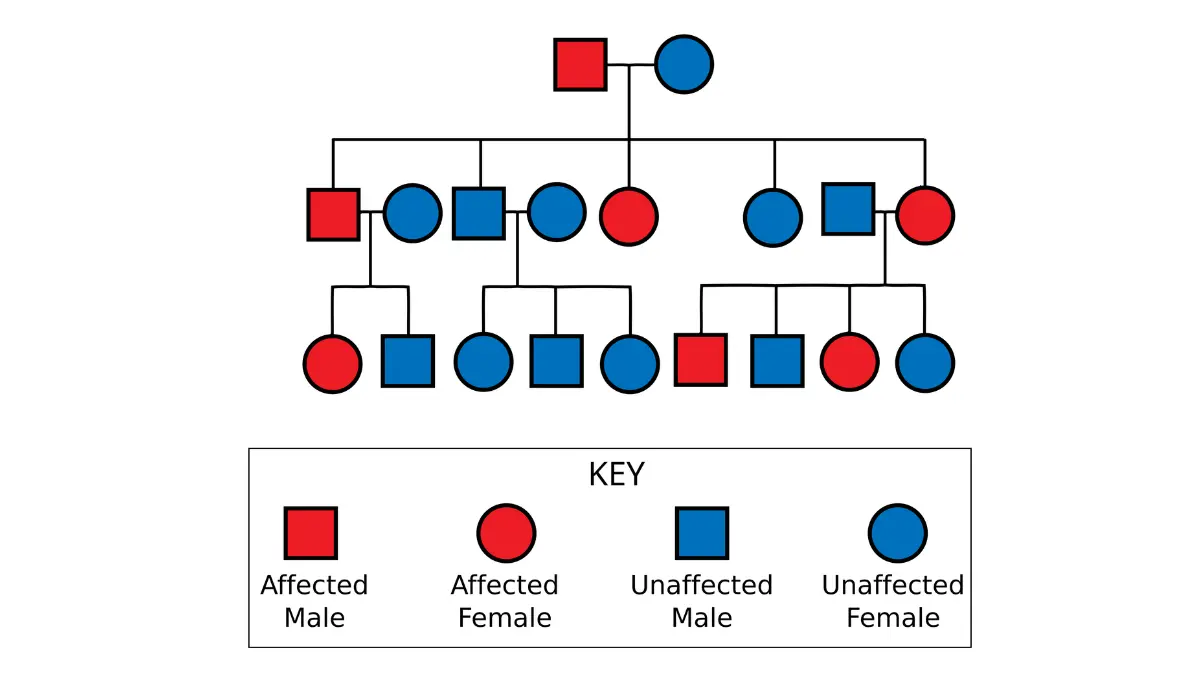
Why your relatives may need testing too
A germline BRCA mutation is inherited, so your children, siblings, and parents each have a chance of carrying it. Because these mutations also raise the risk of other cancers — including breast and pancreatic cancer, as noted in inherited prostate cancer risk factors — relatives can use the result for their own screening. A certified genetic counselor guides who should be tested, a process called cascade testing.
✅ Patient Action: Ask for a referral to a certified genetic counselor, and ask: “Is my mutation germline, and should my family members be tested?”
Frequently asked questions about PARP inhibitors for prostate cancer
1. What are PARP inhibitors and how do they treat prostate cancer?
PARP inhibitors are targeted pills that block a DNA-repair enzyme cancer cells rely on. In prostate cancers that have also lost a BRCA or other HRR repair gene, blocking PARP leaves DNA damage unrepaired, killing the cancer cell — an effect called synthetic lethality. They work best in cancers with these mutations.
2. Do all men with prostate cancer benefit from PARP inhibitors?
No. PARP inhibitors are approved only for cancers carrying specific DNA-repair mutations, and most prostate cancers lack them. BRCA1/2 mutations appear in roughly 11–13% of metastatic cases, with broader HRR mutations in a larger but still minority share. Genetic testing determines candidacy. Discuss testing with your oncologist.
3. Which prostate cancer patients qualify for genetic testing?
Guidelines recommend genetic testing for all men with metastatic, regional, high-risk, or very-high-risk prostate cancer regardless of family history, plus those with a relevant family history, Ashkenazi Jewish ancestry, or certain tumor features. Both germline and tumor testing are often used. Ask your oncologist which tests you need.
4. What’s the difference between germline and tumor (somatic) testing?
Germline testing uses blood or saliva to find inherited mutations you were born with, which also affect blood relatives. Somatic testing reads mutations inside the tumor, some arising only in the cancer. In advanced prostate cancer, about 30% of HRR mutations are germline, so the two tests answer different questions.
5. Which PARP inhibitors are FDA-approved for prostate cancer?
Four are approved: olaparib (Lynparza) and rucaparib (Rubraca) as single agents, and talazoparib (Talzenna, with enzalutamide) and niraparib (Akeega, with abiraterone) as combinations. They are matched to your mutation and stage. Your oncologist determines which, if any, fits your case.
6. Is a BRCA mutation required, or do other gene mutations count?
It depends on the drug. Some approvals require a BRCA mutation specifically, while others cover a broader set of HRR genes such as ATM, CHEK2, and PALB2. Evidence is strongest for BRCA2, weaker for BRCA1, and limited for other genes — which is why your exact mutation matters.
7. How well do PARP inhibitors work for BRCA+ prostate cancer?
In PROfound’s BRCA subgroup, olaparib roughly tripled the time before cancer growth on scans (9.8 vs 3.0 months) and extended median survival (20.1 vs 14.4 months) versus standard hormone agents. These are averages in men whose cancer had already progressed, not personal guarantees. Ask your oncologist what’s realistic.
8. What are the common side effects of PARP inhibitors?
The most common are anemia, fatigue, nausea, and decreased appetite — usually mild to moderate, often peaking in the first two months, and managed with dose adjustments. Rare but serious risks include blood disorders (MDS/AML), lung inflammation, and blood clots. Regular blood tests monitor counts. Report new symptoms to your team.
9. Are PARP inhibitors taken alone or combined with other drugs?
Both. Olaparib and rucaparib can be used alone, generally after prior therapy. Olaparib or niraparib with abiraterone, and talazoparib with enzalutamide, are first-line combinations. Which approach fits depends on your mutation, stage, and prior treatments. Your oncologist makes this determination.
10. If I carry a BRCA mutation, what does it mean for my family?
An inherited (germline) BRCA mutation can pass to children and be shared with siblings and parents, each with a chance of carrying it. Because BRCA mutations raise the risk of other cancers like breast and pancreatic cancer, relatives can use the result for their own screening. A genetic counselor guides cascade testing.
11. Can PARP inhibitors be used for early-stage prostate cancer?
Not currently. All FDA approvals are in metastatic disease — castration-resistant settings, and as of December 2025, BRCA2-mutated castration-sensitive (hormone-sensitive) disease. They aren’t approved for localized or early-stage prostate cancer outside clinical trials. Ask your oncologist whether a trial is appropriate for you.
The bottom line for BRCA+ men
For men with advanced prostate cancer and a BRCA or related DNA-repair mutation, PARP inhibitors are a genuine, targeted option — one that the right genetic testing unlocks. The evidence is strongest for BRCA2, the approved drugs are matched carefully to mutation and stage, and a 2025 approval extended this class into earlier, hormone-sensitive disease for BRCA2 carriers.
The most useful step is confirming your testing and bringing specific questions to your oncologist and a genetic counselor. They are your decision partners — for your treatment, and for what your result may mean for the people you love.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.